
You're considering IGF-1 LR3 for muscle growth or recovery, and you want to know the exact dosing protocol that delivers results without triggering side effects. Here's what decades of use and research have established.
IGF-1 Long R3 is a modified version of insulin-like growth factor 1, a peptide engineered to remain active in your body for 20-30 hours instead of the mere minutes that natural IGF-1 survives. This extended half-life creates a sustained anabolic signal that promotes muscle growth, accelerates recovery, and even stimulates hyperplasia (the creation of new muscle cells). However, this potency comes with precision requirements. Dose too low and you waste expensive product without seeing results. Dose too high and you risk hypoglycemia, joint pain, and receptor desensitization that reduces future effectiveness.
The optimal dosage range for most users falls between 20-50 mcg per day administered via subcutaneous or intramuscular injection. Beginners should start at 20-30 mcg daily for 4 weeks to assess tolerance, while experienced users may use 40-50 mcg split into two daily doses for 4-6 weeks maximum. Timing matters significantly, post-workout injection capitalizes on exercise-induced growth hormone release, while pre-bed injection aligns with your body's natural nighttime GH pulse.
The protocols below draw from published studies and real-world athlete experience. Dosing by experience level, injection timing for maximum muscle growth, safe stacking with other peptides, and the most common mistakes are all covered. Hypoglycemia remains the primary risk, affecting 20-30% of users who fail to manage blood sugar properly.
Quick Reference:
- Beginner dose: 20-30 mcg/day for 4 weeks
- Standard dose: 30-40 mcg/day for 4-6 weeks
- Advanced dose: 40-50 mcg/day split (4-6 weeks max)
- Best timing: Post-workout or before bed
- Critical: Monitor blood sugar (hypoglycemia risk 20-30%)
- No PCT needed (doesn't suppress natural hormones)
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
What is IGF-1 LR3?
IGF-1 Long R3 is a modified version of insulin-like growth factor 1 (IGF-1) that consists of 83 amino acids: 13 more than endogenous IGF-1. The "Long R3" refers to two key modifications: an arginine substitution at position 3 and a 13-amino acid N-terminal extension.
These modifications prevent IGF-1 LR3 from binding to IGF-binding proteins (IGFBPs), which normally deactivate regular IGF-1 within minutes. Without IGFBP interference, LR3 remains active in circulation for 20-30 hours: nearly 100 times longer than natural IGF-1.
How it works in your body:
Think of IGF-1 as the signal that tells your muscles "grow and repair." Your body produces it naturally in response to growth hormone. IGF-1 LR3 amplifies this signal and keeps it active much longer.
It binds to IGF-1 receptors on muscle cells, triggering a cascade of anabolic processes: increased protein synthesis, enhanced nutrient uptake, and even the creation of new muscle cells (hyperplasia): something most compounds can't do (Yakar et al., 2002).
Why athletes use it:
- Muscle hyperplasia: Creates new muscle cells, not just enlarges existing ones
- Enhanced protein synthesis: Increases muscle-building by 30-50% when combined with training (Clemmons, 2009)
- Accelerated recovery: Reduces muscle damage and speeds repair
- Nutrient partitioning: Directs nutrients preferentially to muscle tissue
- Fat loss support: Improves insulin sensitivity while preserving muscle during deficits
Unlike anabolic steroids, IGF-1 LR3 doesn't suppress your natural testosterone or growth hormone production, making post-cycle therapy (PCT) unnecessary.
Standard IGF-1 LR3 Dosage Protocols
The optimal dose depends on your experience level, body weight, and goals. Here's what decades of use and research have established:
Dosage Overview by Experience Level:
| Experience | Daily Dose | Frequency | Cycle Length | Expected Results |
|---|---|---|---|---|
| Beginner | 20-30 mcg | Once daily | 4 weeks | Recovery improvement, muscle fullness |
| Intermediate | 30-40 mcg | 1-2x daily | 4-6 weeks | 4-8 lbs lean tissue gain |
| Advanced | 40-50 mcg | Split 2x daily | 4-6 weeks max | Maximum anabolic effect |
Below are detailed protocols for each experience level:
Beginner Protocol (First Cycle)
If you've never used IGF-1 LR3 before, conservative dosing minimizes side effects while allowing you to assess tolerance and response. The 20-30 hour half-life means once-daily injection provides stable blood levels throughout the day, no need for multiple doses during your first cycle.
Protocol Specifications:
- Daily Dose: 20-30 mcg
- Frequency: Once daily
- Best Timing: Post-workout OR before bed
- Injection Method: Subcutaneous (abdomen or thighs)
- Cycle Length: 4 weeks total
Progressive Dosing Schedule:
- Week 1-2: 20 mcg/day (establish baseline tolerance)
- Week 3-4: 25-30 mcg/day (if no adverse effects observed)
Expected Timeline:
Most beginners notice improved recovery from workouts within 3-5 days as IGF-1 LR3 reduces muscle damage and accelerates repair. Visible muscle fullness appears by week 2 due to increased glycogen and water retention in muscle tissue. Measurable strength gains typically occur by week 3 as the anabolic effects compound.
New to injections? See our How to Inject Peptides Guide for complete technique instructions.
Intermediate Protocol (2-3 Cycles Completed)
For users who've successfully completed at least one cycle and demonstrated good tolerance, intermediate dosing optimizes the anabolic response while maintaining manageable side effect risk. At this level, you have the option to split your daily dose into two injections for more stable blood levels, though single daily dosing remains effective.
Protocol Specifications:
- Daily Dose: 30-40 mcg total
- Frequency: Once or twice daily (split optional)
- Best Timing: Post-workout + before bed (if split)
- Injection Method: SubQ or IM (IM faster absorption)
- Cycle Length: 4-6 weeks
Dosing Options:
- Single dose: 30-40 mcg post-workout
- Split dose: 20 mcg morning + 20 mcg post-workout
- Alternative split: 20 mcg post-workout + 20 mcg before bed
Expected Results:
Most intermediate users report 4-8 pounds of lean tissue gain over 4-6 weeks at this dosage range, accompanied by significant strength improvements (Schiaffino & Mammucari, 2011). The combination of enhanced protein synthesis and improved nutrient partitioning creates favorable conditions for muscle growth when combined with progressive resistance training.
Advanced Protocol (Experienced Users)
For users with multiple successful cycles and solid understanding of peptide use, advanced dosing approaches the upper limit of effective dosing before diminishing returns and increased side effects outweigh benefits. At this level, split dosing becomes essential to maintain stable blood levels and minimize hypoglycemia risk.
Protocol Specifications:
- Daily Dose: 40-50 mcg total (maximum effective range)
- Frequency: Twice daily (split required)
- Best Timing: Morning + post-workout OR post-workout + before bed
- Injection Method: Intramuscular preferred (faster onset)
- Cycle Length: 4-6 weeks maximum
Example Advanced Split:
- Post-workout: 25 mcg IM (vastus lateralis or deltoid)
- Before bed: 25 mcg IM or SubQ
Critical Dosing Limit:
Doses above 50 mcg/day significantly increase hypoglycemia risk (up to 40% of users affected) without delivering proportional muscle-building benefits. Research suggests the anabolic ceiling for most individuals occurs around 40-50 mcg/day (Philippou et al., 2007). Beyond this threshold, you're primarily increasing side effect risk rather than accelerating results.
Injection Timing & Technique
When you inject IGF-1 LR3 matters almost as much as how much you inject.
Optimal Injection Windows
Post-Workout (Highest Priority):
Resistance training creates an acute spike in growth hormone and temporarily increases IGF-1 receptor sensitivity in worked muscles. Injecting IGF-1 LR3 within 30-60 minutes post-workout capitalizes on this window.
Research shows that IGF-1 administration immediately post-exercise increases muscle protein synthesis rates by an additional 35% compared to rest periods (Philippou et al., 2007).
Before Bed (Alternative):
Your body releases the majority of its daily growth hormone during the first 90 minutes of deep sleep. Injecting IGF-1 LR3 30-60 minutes before bed aligns with this natural pulse, creating a synergistic effect.
Avoid These Timing Mistakes:
- Injecting before high-carb meals (can cause reactive hypoglycemia)
- Inconsistent timing (disrupts optimal receptor response)
- Pick one window (post-workout or pre-bed) and stick with it
Injection Technique
Subcutaneous (SubQ) Injection:
- Best for: Beginners, daily injections, doses <30 mcg
- Sites: Lower abdomen (2 inches from navel), outer thighs, back of upper arms
- Technique: Pinch skin, insert 27-31 gauge needle at 45° angle, inject slowly (5-10 sec), release, withdraw
- Rotate sites daily to prevent lipohypertrophy
Intramuscular (IM) Injection:
- Best for: Advanced users, split doses, higher doses (40-50 mcg)
- Sites: Deltoids, vastus lateralis (outer thigh), ventrogluteal (hip)
- Technique: Use 25-27 gauge, 1-1.5 inch needle at 90° angle, aspirate to check for blood, inject slowly
Pro tip: IM injection provides faster absorption (peak levels in 15-30 min vs. 45-60 min SubQ), which some users prefer for post-workout timing.
Full technique guide: Peptide Injections Complete Guide
Reconstitution & Storage
IGF-1 LR3 arrives as lyophilized (freeze-dried) powder. Proper reconstitution is critical, mistakes here waste expensive peptides.
Step-by-Step Reconstitution
What you need:
- IGF-1 LR3 vial (typically 1 mg / 1000 mcg)
- Bacteriostatic water (0.9% benzyl alcohol)
- 3 mL syringe
- Alcohol swabs
Reconstitution protocol:
1. Determine concentration: - For 1 mg vial + 2 mL bacteriostatic water = 500 mcg/mL - Each 0.1 mL = 50 mcg - For 20 mcg dose: draw 0.04 mL - For 40 mcg dose: draw 0.08 mL
2. Add water slowly: - Draw 2 mL bacteriostatic water into syringe - Insert needle into vial, aim water stream at vial wall (not directly at powder) - Inject slowly to minimize foam
3. Dissolve gently: - Swirl vial gently in circular motion (NEVER shake) - Let sit 2-3 minutes for complete dissolution - Solution should be clear, no particles
4. Store immediately: - Refrigerate at 2-8°C (36-46°F) - Protect from light (use original box or wrap in foil)
Detailed guide: How to Reconstitute Peptides
Skip the math: Peptide Reconstitution Calculator
Storage Guidelines
Lyophilized powder (unreconstituted):
- Freezer (-20°C): 12-24 months
- Refrigerator (2-8°C): 6-12 months
Reconstituted:
- Refrigerator (2-8°C): 2-4 weeks (light-protected)
- Room temperature: 24-48 hours max (emergency only)
Critical rules:
- Always refrigerate reconstituted peptides
- Protect from light (UV degrades IGF-1 rapidly)
- Never freeze reconstituted peptides (destroys molecular structure)
- Avoid freeze-thaw cycles with powder
Stacking IGF-1 LR3 with Other Peptides
IGF-1 LR3 synergizes powerfully with growth hormone secretagogues and healing peptides.
Synergistic Stack #1: Maximum Muscle Growth
IGF-1 LR3 + CJC-1295 (no DAC) + Ipamorelin
This stack combines direct IGF-1 action with enhanced natural GH production:
- IGF-1 LR3: 40 mcg once daily post-workout
- CJC-1295 (no DAC): 100 mcg 2-3x/week before bed
- Ipamorelin: 200 mcg 2x/day morning + before bed
How it works together:
CJC-1295 and Ipamorelin stimulate your pituitary to release growth hormone in pulses. This GH then signals your liver to produce more natural IGF-1. Adding exogenous IGF-1 LR3 creates a powerful dual-pathway anabolic effect.
Expected results: 6-10 lbs lean tissue gain over 6 weeks, significant strength improvements, enhanced recovery allowing increased training volume.
Synergistic Stack #2: Injury Recovery & Healing
For accelerated healing of muscle, tendon, or joint injuries:
- IGF-1 LR3: 30 mcg once daily for 4 weeks
- BPC-157: 250 mcg 2x/day for 4-6 weeks (use our BPC-157 calculator)
- TB-500: 5 mg 2x/week for 4-6 weeks
Synergy: IGF-1 LR3 promotes muscle cell growth, BPC-157 supports vascular and epithelial healing, TB-500 enhances cellular migration and tissue repair. Together, they address multiple aspects of the healing cascade.
Use case: Tendon injuries, muscle tears, joint inflammation, post-surgical recovery.
What NOT to Stack
IGF-1 LR3 + Insulin:
Both lower blood glucose. Stacking dramatically increases hypoglycemia risk. If you're using insulin for bodybuilding, separate by at least 6-8 hours and monitor blood sugar closely.
IGF-1 LR3 + High-Dose GH:
Redundant signaling. High-dose exogenous GH already elevates IGF-1 levels. Adding more IGF-1 LR3 increases side effects without proportional benefits. If using pharmaceutical GH, reduce IGF-1 LR3 dose to 20-30 mcg.
Side Effects & Safety Management
IGF-1 LR3 has a favorable safety profile when dosed correctly, but potential side effects require awareness.
Common Side Effects:
| Side Effect | Frequency | Severity | Management |
|---|---|---|---|
| Hypoglycemia | 20-30% | Mild-Moderate | Consume 15-30g fast carbs; monitor blood sugar |
| Jaw soreness | 10-15% | Mild | Temporary; reduce dose if severe |
| Headaches | 10-15% | Mild | Increase hydration; reduce dose |
| Joint pain | <5% | Mild-Moderate | Reduce dose; supplement glucosamine |
| Water retention | <5% | Mild | Lower sodium; usually temporary |
| Organ growth | Theoretical | Unknown | Avoid prolonged use |
Hypoglycemia Prevention (Critical)
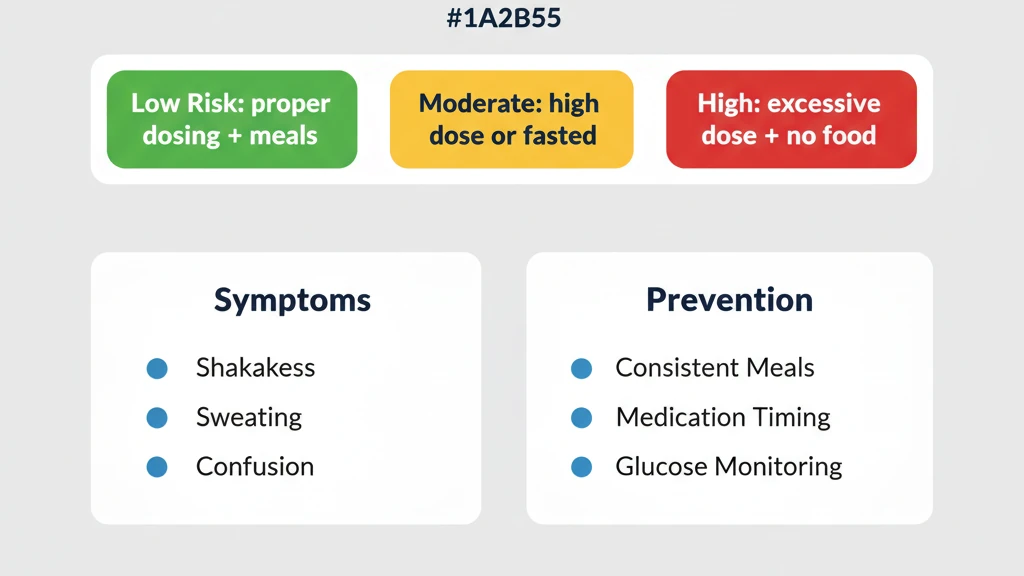
IGF-1's insulin-mimetic effects can lower blood glucose below safe levels. This is the most common and potentially dangerous side effect.
Symptoms of hypoglycemia:
- Shakiness, trembling
- Sweating, cold skin
- Rapid heartbeat
- Confusion, difficulty concentrating
- Dizziness, lightheadedness
- Hunger, nausea
Prevention protocol:
1. Never inject on empty stomach (wait 30-60 min after eating) 2. Time injections strategically: - Post-workout: Consume 30-50g carbs immediately after training, inject, then eat full meal 30 min later - Before bed: Eat small meal with 20-30g slow-digesting carbs first 3. Carry fast-acting carbs (glucose tablets, juice, honey) 4. Increase daily carb intake by 20-30g on injection days 5. Monitor blood sugar if diabetic/pre-diabetic
If hypoglycemia occurs:
- Consume 15g fast-acting carbs immediately
- Wait 15 minutes
- Check symptoms; consume another 15g if not improved
- Once resolved, eat a balanced meal
Cycle Length & Receptor Sensitivity
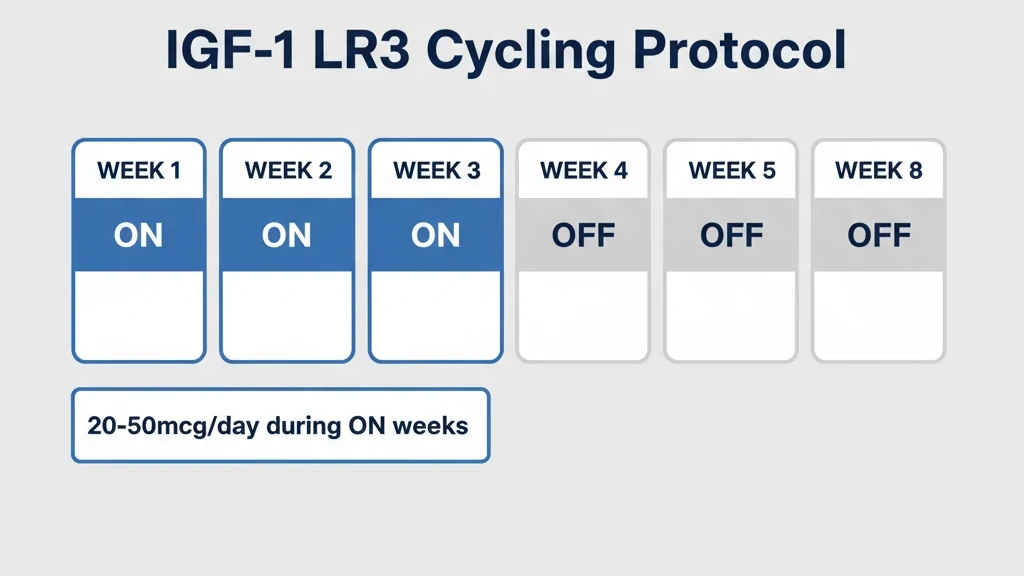
Standard recommendation: 4-6 weeks on, 4-6 weeks off
Why not longer?
IGF-1 receptors undergo downregulation with continuous exposure. After 4-6 weeks of daily IGF-1 LR3, your muscle cells become progressively less responsive, meaning diminishing returns even if you increase the dose.
Research on IGF-1 receptor dynamics shows that receptor density decreases by approximately 40-60% after 6 weeks of continuous supraphysiological IGF-1 exposure (Yakar et al., 2002).
Running an 8-week cycle gives you maybe 10-15% more results than a 6-week cycle, while significantly increasing side effect risk and receptor desensitization.
Cycle structure:
- Weeks 1-2: Adaptation phase (increased recovery, enhanced nutrient uptake)
- Weeks 3-4: Peak anabolic phase (maximum muscle protein synthesis, strength increases)
- Weeks 5-6: Maintenance/plateau phase (receptor sensitivity declining)
- Week 7+: Diminishing returns (not recommended)
Post-Cycle Recovery:
Unlike steroids, IGF-1 LR3 doesn't suppress natural hormone production. No traditional PCT required. However, allow 4-6 weeks off for receptor resensitization.
Off-cycle protocol:
- Maintain training intensity
- Keep protein intake high (1.0-1.2g per lb body weight)
- Sleep 7-9 hours (natural GH production)
- Consider low-dose GH secretagogues if maintaining muscle is challenging
Maximizing Results: Training & Nutrition
IGF-1 LR3 doesn't build muscle by itself. It amplifies your body's response to training and nutrition.
Training Adjustments
Increase training volume by 10-20%:
IGF-1 LR3 dramatically improves recovery capacity. What would normally cause overtraining becomes manageable.
Example progression:
- Baseline: 3 sets x 12 exercises = 36 total sets per session
- On IGF-1 LR3: 4 sets x 12 exercises = 48 total sets (33% increase)
- OR add 1-2 extra training sessions per week
Prioritize compound movements:
- Squats, deadlifts, bench press, rows, overhead press
- These recruit maximum muscle fibers
- IGF-1 preferentially supports most-stimulated muscle tissue
Shorten rest periods:
- Normal: 2-3 minutes between heavy sets
- On IGF-1 LR3: 60-90 seconds (enhanced recovery)
- Creates greater metabolic stress → additional growth stimulus
Nutrition Optimization
Protein: 1.2-1.5g per pound of body weight
IGF-1 LR3 increases muscle protein synthesis rates by 30-50%. Feed this process with adequate protein.
Example: 200 lb person = 240-300g protein daily
Carbohydrates: Strategic timing
IGF-1's glucose-lowering effects require careful carb management:
- Pre-workout: 40-60g carbs (fuel training)
- Post-injection: 30-50g fast carbs (prevent hypoglycemia)
- Post-workout meal: 60-80g carbs + protein (maximize nutrient uptake)
- Throughout day: 200-300g total depending on body size
Fats: Don't neglect
- Supports hormone production
- 0.4-0.5g per lb body weight
- Focus on omega-3s (fish oil, salmon, walnuts)
Hydration: Critical
IGF-1 increases metabolic demands and protein synthesis, both water-intensive processes.
- Minimum: 1 gallon (3.8L) daily
- Active/hot climate: 1.5 gallons (5.7L)
Frequently Asked Questions
Can you take IGF-1 LR3 orally?
No. IGF-1 LR3 is a peptide (protein fragment) that would be completely destroyed by stomach acid and digestive enzymes before reaching your bloodstream. It must be injected subcutaneously or intramuscularly for bioavailability. Anyone selling "oral IGF-1" is either selling a fake product or a peptide with poor absorption and minimal effectiveness.
What's the difference between IGF-1 LR3 and regular IGF-1?
Regular IGF-1 (also called IGF-1 DES) has a half-life of only 20-30 minutes because IGF-binding proteins (IGFBPs) rapidly deactivate it. IGF-1 LR3 has two molecular modifications, an arginine substitution at position 3 and a 13-amino acid N-terminal extension, that prevent IGFBP binding. This extends the half-life to 20-30 hours (about 60 times longer) and increases potency roughly 3-fold compared to native IGF-1 (Clemmons, 2009).
How long does it take to see results from IGF-1 LR3?
Timeline:
- Days 3-5: Improved recovery, reduced muscle soreness, better sleep quality
- Week 2: Visible muscle fullness (glycogen and water in muscle tissue), veins more prominent
- Week 3: Measurable strength gains (5-10% on major lifts), muscle definition improves
- Weeks 4-5: Peak results, most users gain 4-8 lbs of lean tissue with proper training and nutrition
Can women use IGF-1 LR3?
Yes. Women typically use lower doses (15-30 mcg/day) due to generally lower body weight and higher sensitivity to IGF-1. The same cycle length (4-6 weeks) and safety protocols apply. Women should be especially vigilant about hypoglycemia monitoring as estrogen can affect blood sugar regulation.
No masculinizing side effects occur, IGF-1 doesn't interact with androgen receptors like anabolic steroids do.
Do you need to cycle IGF-1 LR3?
Absolutely yes. Continuous use beyond 6 weeks leads to IGF-1 receptor downregulation (decreased density and sensitivity). Research shows that after 6 weeks of elevated IGF-1, receptor density decreases by 40-60%, significantly blunting the peptide's effectiveness (Yakar et al., 2002). The standard protocol is 4-6 weeks on, 4-6 weeks off to maintain receptor sensitivity.
Does IGF-1 LR3 require PCT (post-cycle therapy)?
No. Unlike anabolic steroids, IGF-1 LR3 doesn't suppress your body's natural testosterone, growth hormone, or IGF-1 production. When you stop injecting it, your natural levels return to baseline within days. However, you should still take 4-6 weeks off between cycles to allow IGF-1 receptors to resensitize.
The Bottom Line
The optimal IGF-1 LR3 dosage protocol balances effectiveness with safety: 20-50 mcg per day for 4-6 weeks, injected post-workout or before bed, with careful attention to blood sugar management and receptor sensitivity.
Protocol summary:
- Beginners: Start at 20-30 mcg/day to assess tolerance
- Intermediate: 30-40 mcg/day provides the sweet spot for most users
- Advanced: 40-50 mcg/day is the ceiling, higher doses increase side effects without proportional benefits
- Timing: Post-workout injection capitalizes on exercise-induced GH pulse and increased receptor sensitivity
- Safety: Hypoglycemia is the main risk, never inject on empty stomach, time carbs strategically
- Cycling: 4-6 weeks on, 4-6 weeks off prevents receptor downregulation
- Stacking: Synergizes powerfully with GH secretagogues (CJC-1295/Ipamorelin) and healing peptides (BPC-157/TB-500)
Remember: IGF-1 LR3 is a tool that amplifies your training and nutrition: it doesn't replace them. Proper dosing combined with progressive overload training, adequate protein (1.2-1.5g/lb), and calorie surplus creates the environment for maximum muscle growth.
Start conservatively, monitor your response, and adjust within proven ranges. Precision matters more than volume.
Ready to optimize your protocol?
- Take our Peptide Quiz: Get personalized recommendations in 2 minutes
- Peptide Reconstitution Calculator: Calculate exact doses instantly
- BPC-157 Dosage Calculator: For healing stacks
- How to Inject Peptides: Step-by-step technique guide
References: 1. Yakar S, et al. (1999). Normal growth and development in the absence of hepatic IGF-I. *PNAS*, 96(13):7324-7329. 2. Clemmons DR. (2018). Role of IGF-binding proteins in regulating IGF responses. *J Mol Endocrinol*, 61(1):T139-T169. 3. Clemmons DR. (2009). Role of IGF-I in skeletal muscle mass maintenance. *Trends Endocrinol Metab*, 20(7):349-356. 4. Schiaffino S, Mammucari C. (2011). Regulation of skeletal muscle growth by the IGF1-Akt/PKB pathway. *Skeletal Muscle*, 1(1):4. 5. Philippou A, et al. (2007). Type I IGF-1 receptor signaling in skeletal muscle regeneration. *J Musculoskelet Neuronal Interact*, 7(3):208-218.
Related Articles
How to Calculate IGF-1 LR3 Dosage (+ Calculator)
Calculate your IGF-1 LR3 dose and exact syringe units by hand, or use our free interactive calculator. Reconstitution math, dose-by-goal tables, examples.
CJC-1295 Dosage: Complete Protocol Guide
CJC-1295 dosage guide: DAC and no-DAC protocols. Dosing by goal (anti-aging, fat loss, muscle, sleep), ipamorelin stacking, and injection timing.
IGF-1 LR3 Results: What to Expect by Week
IGF-1 LR3 results week by week: pumps, recovery, lean mass, and what before-and-after photos really show. Evidence vs bro-science, safety, and dosing.
Peptides for Bodybuilding (2026)
Best peptides for bodybuilding: BPC-157, TB-500, MK-677, CJC-1295/Ipamorelin, HGH Fragment 176-191. Dosages and stacking protocols.