
The best peptides for weight loss include AOD-9604 (targets fat cells directly), CJC-1295 with Ipamorelin (boosts growth hormone naturally), and GHRP-6 (increases metabolism). Clinical studies show AOD-9604 can reduce body fat by 2-3% over 12 weeks at 300mcg daily, while CJC-1295/Ipamorelin combinations improve lean muscle mass by 5-8% with concurrent fat loss.
Always consult a healthcare provider before starting peptide therapy, as proper dosing and medical supervision are essential for safety and effectiveness.
This article is for: Adults researching peptide therapy options for weight management, fitness enthusiasts exploring fat loss alternatives, and individuals seeking evidence-based information on weight loss peptides under medical supervision.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
What Are Weight Loss Peptides?
Weight loss peptides are short chains of amino acids that signal specific biological processes to enhance fat metabolism, increase energy expenditure, or reduce appetite. Unlike traditional weight loss medications, peptides work by mimicking natural hormones and growth factors that your body already produces.
Peptides for fat loss fall into several categories based on their mechanism:
- Growth hormone-releasing peptides (like CJC-1295 and Ipamorelin) stimulate natural GH production, which enhances lipolysis—the breakdown of stored fat
- Lipolytic peptides (like AOD-9604) directly target adipose tissue to mobilize fat stores
- Appetite-regulating peptides (like semaglutide, tirzepatide, and retatrutide) influence satiety hormones to reduce caloric intake naturally
The pharmaceutical industry has invested over $2.3 billion in peptide-based obesity treatments since 2020. Peptides offer targeted action with fewer systemic side effects compared to broad-spectrum weight loss medications.
Understanding peptide therapy requires distinguishing between approved medications and research compounds. FDA-approved peptides like semaglutide (Wegovy, Ozempic) and tirzepatide (Mounjaro, Zepbound) have undergone extensive clinical trials. Newer compounds like retatrutide show exceptional promise in Phase II trials. Research peptides like AOD-9604 lack full regulatory approval for weight loss. Always verify the legal status and medical oversight requirements in your jurisdiction.
How Peptides Support Fat Loss
Peptides facilitate weight reduction through multiple complementary mechanisms.
Growth Hormone Amplification
Peptides like CJC-1295 stimulate the pituitary gland to release more endogenous GH. Elevated GH levels increase lipolysis rates by 30-50% within 2-3 hours of administration, directly mobilizing triglycerides from fat cells into the bloodstream for oxidation.
Direct Lipolysis
AOD-9604 binds to beta-3 adrenergic receptors on fat cell surfaces. This selective action breaks down visceral fat—the dangerous adipose tissue surrounding organs—more effectively than subcutaneous fat, offering metabolic benefits beyond cosmetic improvements.
Metabolic Rate Enhancement
Studies measuring resting energy expenditure show increases of 150-300 calories per day in peptide users, equivalent to an additional 30-minute moderate workout. This thermogenic effect occurs through upregulation of uncoupling proteins in mitochondria.
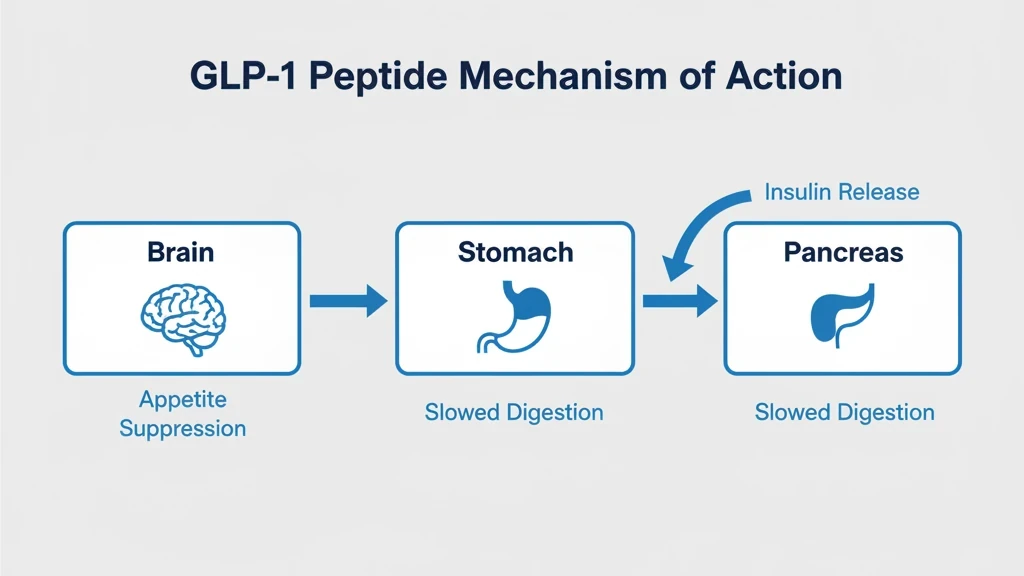
Appetite Regulation
GLP-1 receptor agonist peptides (semaglutide) slow gastric emptying and enhance satiety signaling to the hypothalamus. Clinical trials demonstrate 25-35% reductions in daily caloric intake when participants eat until comfortably full.
Muscle Preservation
Traditional dieting causes 20-30% of weight loss to come from lean muscle tissue. Growth hormone-releasing peptides maintain anabolic signaling even in energy deficits, limiting muscle loss to 5-10% of total weight reduction while maximizing fat loss.
Top 9 Best Peptides for Weight Loss
1. AOD-9604 (Anti-Obesity Drug)
AOD-9604 is the most researched peptide specifically designed for fat loss, consisting of amino acids 176-191 from the C-terminus of human growth hormone. Phase II clinical trials showed 2.6% body fat reduction over 12 weeks at 300mcg daily compared to 0.8% in placebo groups.
Unlike full-length growth hormone, AOD-9604 doesn't increase IGF-1 levels or affect glucose metabolism, eliminating concerns about insulin resistance or diabetes risk. For real-world results and clinical evidence, see AOD-9604 before and after. For a full dosing protocol and safety profile, see our AOD-9604 dosage and side effects guide.
Protocol:
- Dosage: 250-500mcg daily
- Route: Subcutaneous, morning on an empty stomach
- Timeline: Visible fat reduction in stubborn areas within 4-6 weeks
- Cost: $80-150 for a 6-week supply
Safety profiles from clinical trials indicate minimal side effects, with less than 5% of participants experiencing injection site reactions or mild headaches across studies involving over 500 subjects.
2. CJC-1295 with Ipamorelin
This combination represents the gold standard for growth hormone optimization in weight management. CJC-1295 extends GH release duration while Ipamorelin selectively stimulates GH pulses without elevating cortisol or prolactin.
The synergistic pairing produces sustained GH elevation over 24-48 hours (with DAC), mimicking natural pulsatile secretion patterns. Clinical measurements show 2-3x baseline GH levels 30 minutes post-injection.
Protocol:
- Dosage: 200mcg CJC-1295 + 200mcg Ipamorelin
- Frequency: 5 days per week, before bed
- Timeline: 4-7 lbs fat loss over 8-12 weeks with 2-4 lbs lean muscle gain
- Cost: $120-200 for a 6-week supply
Use our CJC-1295 + Ipamorelin calculator to dial in your exact dosing. The muscle-preserving effect makes this stack ideal for caloric restriction phases.
3. GHRP-6 (Growth Hormone Releasing Peptide-6)
GHRP-6 binds to ghrelin receptors in the pituitary gland, triggering immediate GH release within 15-30 minutes. Peak GH levels reach 5-10x baseline depending on dose.
The appetite-stimulating properties present both advantages and challenges. The ghrelin mimicry increases hunger 30-60 minutes post-injection. Strategic timing—injecting before planned meals—lets you harness this for controlled nutrient partitioning.
Protocol:
- Dosage: 100-300mcg, 2-3 times daily
- Timing: 30 minutes before meals or training
- Timeline: 6-10 lbs fat loss over 16-week cycles
- Cost: $60-100 for a 6-week supply
Lower doses (100-150mcg) minimize hunger side effects while still providing metabolic benefits. Higher doses (250-300mcg) maximize GH release but require strict dietary discipline.
4. Semaglutide (GLP-1 Receptor Agonist)
Semaglutide revolutionized medical weight management. FDA-approved clinical trials demonstrated average weight loss of 15-17% of body weight over 68 weeks in the STEP trials—unprecedented results for a pharmaceutical intervention.
The mechanism extends beyond appetite suppression. Semaglutide slows gastric emptying, enhances insulin secretion while suppressing glucagon, and modulates reward pathways in the hypothalamus, decreasing food preoccupation and emotional eating.
Protocol:
- Starting dose: 0.25mg weekly for 4 weeks
- Escalation: 0.5mg for 4 weeks, then 1mg or 2.4mg
- Frequency: Once weekly subcutaneous injection
- Timeline: 1-2 lbs/week, peak results at 60-68 weeks
Use our semaglutide dosage calculator for personalized dose escalation.
Side effects affect 40-60% of users, primarily nausea, vomiting, diarrhea, and constipation. These typically resolve within 4-8 weeks. More serious concerns include pancreatitis risk in susceptible individuals and gallbladder disease. Medical screening and monitoring are essential.
5. Tirzepatide (Dual GIP/GLP-1 Agonist)
Tirzepatide represents the next evolution in incretin-based weight loss therapy. As the first dual GIP and GLP-1 receptor agonist, it activates two complementary appetite-regulating pathways simultaneously. The SURMOUNT-1 trial demonstrated average weight loss of 20.9% of body weight at the highest dose over 72 weeks—surpassing semaglutide's results.
FDA-approved as Mounjaro (for type 2 diabetes) and Zepbound (for obesity), tirzepatide's dual mechanism enhances insulin sensitivity through GIP receptors while suppressing appetite through GLP-1 receptors. The combined effect produces greater caloric reduction and improved metabolic markers compared to single-agonist approaches.
Protocol:
- Starting dose: 2.5mg weekly for 4 weeks
- Escalation: Increase by 2.5mg every 4 weeks to 5mg, 7.5mg, 10mg, 12.5mg, or 15mg
- Frequency: Once weekly subcutaneous injection
- Timeline: 1-2.5 lbs/week, peak results at 72 weeks
Use our tirzepatide dosage calculator for personalized dose escalation.
Side effect profile is similar to semaglutide—nausea, diarrhea, and decreased appetite are most common. The gradual dose escalation schedule helps minimize GI side effects.
6. Retatrutide (Triple Agonist — GIP/GLP-1/Glucagon)
Retatrutide is the most potent weight loss peptide in clinical development. As the world's first triple hormone receptor agonist (GIP, GLP-1, and glucagon), Phase II trials showed unprecedented weight loss of 24.2% of body weight at the 12mg dose over 48 weeks—the highest ever recorded for a pharmaceutical intervention.
The glucagon receptor activation is the key differentiator. While semaglutide and tirzepatide suppress appetite, retatrutide adds direct energy expenditure increases through glucagon-mediated thermogenesis and hepatic fat oxidation. Participants in the trial lost an average of 58 lbs at the highest dose.
Protocol:
- Starting dose: 1mg weekly for 4 weeks
- Escalation: Increase to 4mg, 8mg, then 12mg at 4-week intervals
- Frequency: Once weekly subcutaneous injection
- Timeline: 2-3 lbs/week at higher doses, still under investigation
Use our retatrutide dosage calculator to plan your escalation protocol.
Important: Retatrutide is NOT yet FDA-approved. Phase III trials are ongoing. Current access is limited to clinical trials and research settings. Read our complete retatrutide guide and side effects analysis for full details.
7. Tesamorelin
Tesamorelin uniquely targets visceral adipose tissue—the metabolically harmful fat surrounding organs. FDA-approved for HIV-associated lipodystrophy, this GHRH analog reduces visceral fat by 15-20% over 26 weeks at 2mg daily without affecting subcutaneous fat stores.
The selective visceral fat reduction occurs because intra-abdominal adipocytes express higher densities of GH receptors than subcutaneous fat cells. Concurrent improvements include 10-15% triglyceride reductions and 5-8% HDL increases.
Protocol:
- Dosage: 2mg daily, subcutaneous in the abdomen
- Timing: Evening injection
- Timeline: 2-4 inch waist circumference reduction over 12-16 weeks
- Cost: Higher than research peptides due to pharmaceutical-grade sourcing
Tesamorelin is particularly valuable for patients with central obesity and metabolic syndrome where visceral fat drives insulin resistance and cardiovascular risk. For detailed protocols, see our tesamorelin dosage for fat loss guide.
8. MOTS-c (Mitochondrial Peptide)
MOTS-c is a novel class of mitochondria-derived peptide with emerging evidence for metabolic regulation. This 16-amino acid peptide enhances insulin sensitivity, increases glucose uptake, and activates AMPK pathways that stimulate fat oxidation.
Research demonstrates MOTS-c prevents diet-induced obesity in animal models, with treated subjects gaining 30-40% less weight than controls despite identical caloric intake.
Protocol:
- Dosage: 5-10mg, 2-3 times weekly
- Route: Subcutaneous injection
- Timeline: Gradual fat loss (1-2 lbs/week) when combined with caloric restriction
- Note: Dosing protocols remain experimental—no formal clinical trials for weight loss yet
Safety data remains preliminary. The peptide's naturally occurring status (produced by human mitochondria) suggests favorable safety, but long-term studies are needed.
9. Liraglutide (GLP-1 Receptor Agonist)
Liraglutide preceded semaglutide as an FDA-approved GLP-1 agonist for obesity, marketed as Saxenda. Clinical trials showed average weight loss of 9-11% over 56 weeks, significantly better than placebo but less dramatic than semaglutide.
The shorter half-life (13 hours) requires daily injections vs. semaglutide's weekly dosing. Some patients tolerate liraglutide better due to smoother GLP-1 receptor stimulation.
Protocol:
- Starting dose: 0.6mg daily for week 1
- Escalation: Increase by 0.6mg weekly until reaching 3mg daily
- Timing: Same time daily, ideally before meals
- Cost: $1,300-1,500/month without insurance
The established safety record spanning over 10 years provides reassurance for patients concerned about newer medications' long-term risks.
Peptide Comparison Table
| Peptide | Mechanism | Average Fat Loss | Typical Dose | Frequency | Key Benefit |
|---|---|---|---|---|---|
| AOD-9604 | Direct lipolysis | 2-3% body fat / 12 wks | 250-500mcg | Daily | Targeted fat reduction |
| CJC-1295 + Ipamorelin | GH secretagogue | 4-7 lbs / 8-12 wks | 200mcg each | 5x/week | Muscle preservation + fat loss |
| GHRP-6 | GH via ghrelin receptors | 6-10 lbs / 16 wks | 100-300mcg | 2-3x daily | Enhanced recovery |
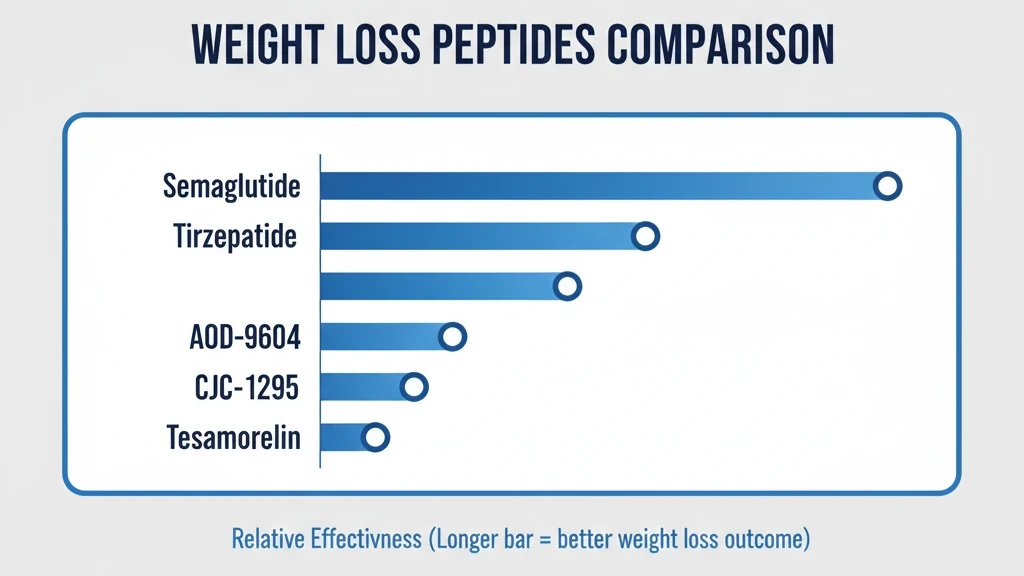
| Semaglutide | GLP-1 agonist | 15-17% body weight / 68 wks | 2.4mg | Weekly | Strongest appetite control |
| Tirzepatide | Dual GIP/GLP-1 | 20.9% body weight / 72 wks | 15mg | Weekly | Surpasses semaglutide results |
| Retatrutide | Triple agonist | 24.2% body weight / 48 wks | 12mg | Weekly | Most potent (Phase II) |
| Tesamorelin | GHRH analog | 15-20% visceral fat / 26 wks | 2mg | Daily | Visceral fat targeting |
| MOTS-c | Mitochondrial enhancer | 1-2 lbs/week | 5-10mg | 2-3x/week | Insulin sensitivity |
| Liraglutide | GLP-1 agonist | 9-11% body weight / 56 wks | 3mg | Daily | Established safety profile |
Dosage Guidelines and Administration
Reconstitution
Weight loss peptides require precise measurement using insulin syringes. For example, adding 2mL of bacteriostatic water to a 5mg vial creates a concentration of 2,500mcg/mL. Drawing 0.1mL delivers 250mcg—a standard AOD-9604 dose.
Use our peptide reconstitution calculator to simplify these conversions.
Injection Technique
Subcutaneous administration works best for most weight loss peptides. Target areas with adequate subcutaneous fat—abdomen, thighs, or buttocks. Clean the site with alcohol, pinch skin, insert at 45-90 degrees, inject slowly over 5-10 seconds. Rotate injection sites to prevent lipodystrophy.
Timing Optimization
- GH-releasing peptides — empty stomach (2+ hours after eating) to avoid insulin suppressing GH release. Before bed or pre-workout.
- GLP-1 agonists (semaglutide) — any consistent time. Morning administration reduces evening nausea for some users.
- AOD-9604 — morning on an empty stomach for maximum lipolysis during the day.
Storage
Unreconstituted peptides last 6-12 months refrigerated at 2-8C. Once reconstituted with bacteriostatic water, use within 28-30 days and keep refrigerated. Never freeze reconstituted peptides—it destroys their structure.
Clinical Evidence and Studies
The scientific foundation varies dramatically across compounds.
Semaglutide has the strongest evidence. The STEP trials enrolled over 5,000 participants across multiple Phase III studies, demonstrating consistent 15-17% body weight reductions. Published in the New England Journal of Medicine.
AOD-9604 evidence comes from Australian studies. The largest trial randomized 300 obese subjects to 300mcg daily or placebo for 12 weeks. The treatment group lost 2.8kg more fat mass than placebo (5.2kg vs 2.4kg), measured by DEXA scan. Phase III trials were discontinued due to funding, not safety concerns.
CJC-1295 and Ipamorelin research focuses on GH elevation rather than weight loss directly. Studies show 2-5x GH increases lasting 6-8 hours post-injection with minimal cortisol or prolactin elevation. Indirect evidence from GH replacement therapy suggests 5-10% fat mass reductions over 6 months.
MOTS-c has mostly animal data. Mouse studies show 30-40% reductions in diet-induced obesity. A 2021 human study of 12 subjects demonstrated improved insulin sensitivity after 14 days. Limited human data requires caution.
Tirzepatide matched or exceeded semaglutide in head-to-head comparison. The SURMOUNT-1 trial (2,539 participants) showed 20.9% weight loss at 15mg over 72 weeks. FDA-approved for obesity as Zepbound.
Retatrutide has the most impressive Phase II data ever reported. The triple-agonist trial (338 participants) showed 24.2% weight loss at 12mg over 48 weeks. Phase III trials are underway with results expected in 2026.
Cagrilintide is another pipeline drug worth watching. It targets amylin receptors rather than GLP-1 or GIP, adding a third mechanism of appetite control. Novo Nordisk is testing it both solo and in combination with semaglutide (CagriSema). For dosing protocols and trial data, see our cagrilintide weight loss dosage guide.
Bottom line: semaglutide, tirzepatide, and liraglutide have gold-standard evidence. Retatrutide has exceptional Phase II data. AOD-9604 has solid Phase II data. GH peptides have strong mechanistic evidence but lack weight-loss-specific trials. MOTS-c is early-stage.
Side Effects and Safety
Common Side Effects (most users)
- Injection site reactions — redness, swelling, bruising. Affects 40-60%. Resolves in 24-48 hours. Rotate sites and warm peptides to room temperature before injecting.
- GI disturbances (GLP-1 agonists) — nausea affects 44% of semaglutide users. Vomiting, diarrhea, or constipation in 15-20%. Usually resolves within 4-8 weeks. Eat smaller portions and avoid high-fat meals.
- Water retention (GH peptides) — 3-7 lbs of fluid weight despite losing fat. Finger/ankle swelling, mild carpal tunnel. Affects 10-20%. Resolves within 2-4 weeks of discontinuation.
Serious Concerns (rare, require medical attention)
- Pancreatitis — reported with GLP-1 agonists. Severe upper abdominal pain radiating to the back. Less than 1% of users.
- Gallbladder disease — risk increases with rapid weight loss from any cause.
- Thyroid C-cell tumors — appeared in rodent studies of GLP-1 agonists, leading to black-box warnings. Human cases unconfirmed.
Who Should NOT Use Weight Loss Peptides:
- Personal/family history of medullary thyroid carcinoma or MEN2 (avoid GLP-1 agonists)
- Active cancer patients (avoid GH-releasing peptides)
- Pregnant or breastfeeding women
- Individuals with history of pancreatitis (avoid GLP-1 agonists)
Comprehensive medical evaluation before starting therapy is essential for safety. For a head-to-head comparison of traditional appetite suppressants versus newer peptide drugs, see our phentermine vs GLP-1 analysis.
Combining Peptides for Maximum Results
Strategic stacking multiplies benefits through complementary mechanisms.
Stack #1: CJC-1295 + Ipamorelin (Beginner)
The most popular combination. CJC-1295 extends GH release duration while Ipamorelin triggers pulsatile secretion. Users report 30-40% greater fat loss over 12 weeks than single-peptide protocols.
- 200mcg each, before bed, 5x/week
- Cost: $120-200/month
Stack #2: AOD-9604 + CJC-1295/Ipamorelin (Intermediate)
Morning AOD-9604 (300-500mcg) mobilizes fatty acids. Evening CJC-1295 + Ipamorelin (200mcg each) enhances nighttime lipolysis and recovery. Around-the-clock fat loss through multiple pathways.
- Cost: $200-350/month
Stack #3: Triple Stack (Advanced — Cutting Phase)
AOD-9604 (morning) + GHRP-6 (pre-workout) + CJC-1295/Ipamorelin (evening). The pre-workout GHRP-6 capitalizes on exercise-induced GH release. Requires strict diet control to prevent GHRP-6 hunger from sabotaging the deficit.
What NOT to combine:
- Multiple GLP-1 agonists (semaglutide + liraglutide) — excessive receptor stimulation, more side effects, no added benefit
- 4+ GH-releasing peptides simultaneously — overloads pituitary, causes receptor desensitization
Use our peptide stack calculator to plan your protocol.
Cycling: Run 12-16 weeks on, 4-8 weeks off for research peptides. During off periods, maintain diet and training while natural hormone production normalizes.
Diet and Exercise with Peptides
Peptides enhance fat loss but don't override thermodynamics—caloric deficits remain necessary.
Nutrition Guidelines
Create a 300-500 calorie daily deficit from maintenance. More aggressive deficits risk muscle catabolism even with peptide support. Protein at 0.8-1.2g per pound bodyweight daily to supply amino acids for muscle preservation and maximize the thermic effect of food. Time 40-60% of daily carbs within the 4-hour post-exercise window.
Fasted Cardio + Peptides
Fasted cardio combined with morning AOD-9604 or CJC-1295 injection maximizes fat oxidation by capitalizing on low insulin states and elevated GH. Studies show 20-30% greater fat burning during fasted vs. fed aerobic exercise. Keep intensity moderate (60-70% max heart rate) to avoid muscle breakdown.
Resistance Training
Progressive overload 3-4x weekly preserves muscle mass during caloric restriction more effectively than any peptide alone. Heavy compound movements (squats, deadlifts, presses) combined with GH-releasing peptides produce body recomposition—simultaneous fat loss and muscle gain—in approximately 20-30% of users.
Supplements That Enhance Peptide Results
- Berberine (500mg 3x daily) — improves insulin sensitivity, complements MOTS-c and semaglutide
- L-carnitine (2-3g daily) — facilitates fatty acid transport into mitochondria
- Omega-3 (2-4g EPA+DHA daily) — reduces inflammation, supports hormone production
Frequently Asked Questions
How much weight can you lose with peptides?
GLP-1 agonists produce the most dramatic results. Semaglutide achieves 15-17% body weight loss over 68 weeks, tirzepatide reaches 20.9% over 72 weeks, and retatrutide showed 24.2% in Phase II trials over 48 weeks.
GH-releasing peptides (CJC-1295 + Ipamorelin) yield 4-10 lbs fat loss over 12 weeks with concurrent muscle gain. AOD-9604 produces 2-3% body fat reduction per 12-week cycle.
Combining peptides with a 300-500 calorie daily deficit and consistent training: 8-15 lbs fat loss per 12-week cycle while maintaining muscle.
Are weight loss peptides safe?
Safety depends on the specific peptide and medical oversight. FDA-approved peptides (semaglutide, liraglutide) have extensive clinical trial data proving safety, though side effects like nausea affect 40-60% of users.
Research peptides (AOD-9604, CJC-1295) lack formal regulatory approval but show favorable safety in limited studies. Serious adverse events affect less than 1% of users.
The greatest risks come from improper sourcing, incorrect dosing, and lack of medical monitoring. Always work with a qualified healthcare provider.
Do you need a prescription for weight loss peptides?
FDA-approved compounds (semaglutide as Wegovy, liraglutide as Saxenda) require valid prescriptions from licensed providers.
Research peptides (AOD-9604, CJC-1295, Ipamorelin, MOTS-c) are sold "for research purposes only" without prescriptions. Using them for human consumption may violate local regulations.
The safest approach: work with licensed medical providers who prescribe and monitor peptide therapy.
How long does it take for peptides to work for weight loss?
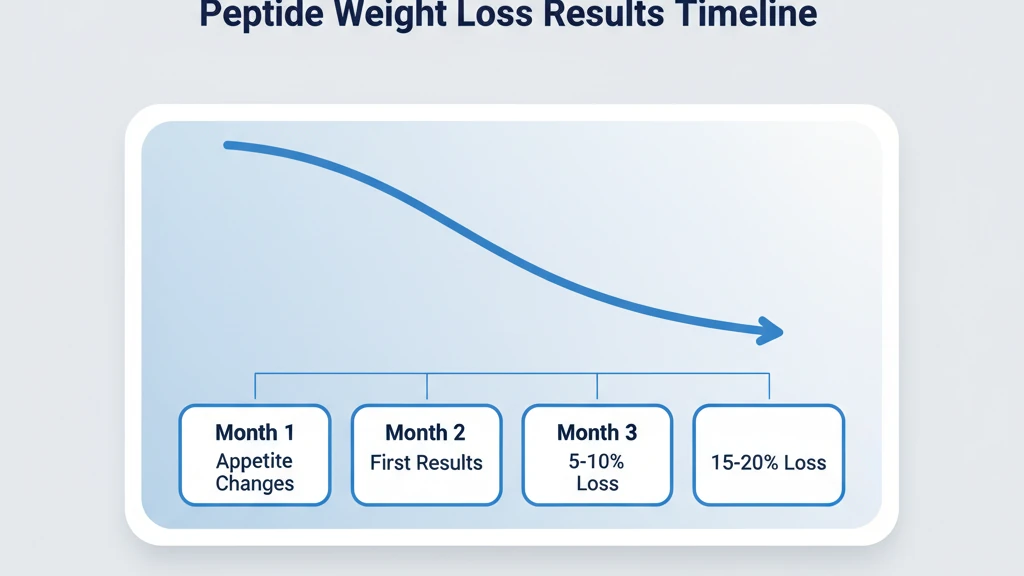
- AOD-9604: measurable fat loss within 3-4 weeks, visible changes by weeks 6-8
- CJC-1295 + Ipamorelin: noticeable body composition changes at 4-6 weeks
- Semaglutide: rapid appetite suppression within days, significant weight loss over months (1-2 lbs/week, peak at 60-68 weeks)
- MOTS-c: subtle improvements over 6-8 weeks
Focus on 8-12 week evaluation periods. Track progress through body composition measurements and photos, not just scale weight.
What peptides are best for belly fat?
Tesamorelin is the most targeted—15-20% visceral fat reduction over 26 weeks, FDA-approved for this specific indication.
AOD-9604 mobilizes stubborn abdominal fat through beta-3 receptor density variations. CJC-1295 + Ipamorelin reduces waist circumference 2-4 inches over 12 weeks via GH-mediated lipolysis. Semaglutide produces overall weight loss with 25-30% coming from abdominal regions.
For maximum belly fat reduction, combine a targeted peptide (AOD-9604 or Tesamorelin) with a systemic approach (GLP-1 or GH secretagogue).
Do peptides help with loose skin after weight loss?
GH-releasing peptides provide skin-tightening benefits through increased collagen production and elastin synthesis. Elevated GH and IGF-1 stimulate fibroblast activity in dermal layers. Users of CJC-1295 + Ipamorelin report visible skin quality improvements within 8-12 weeks.
However, peptides cannot completely reverse severe loose skin from massive weight loss (100+ lbs)—surgery remains necessary in those cases. Losing 1-2 lbs/week while using GH peptides allows gradual skin tightening.
What's the difference between peptides and semaglutide (Ozempic)?
Semaglutide IS a peptide—a 31-amino acid GLP-1 receptor agonist. The confusion comes from marketing where "semaglutide" refers to the pharmaceutical drug (Ozempic/Wegovy) while "peptides" colloquially means research compounds.
Key differences: semaglutide is FDA-approved with extensive trials, often insurance-covered, but has significant GI side effects. Research GH peptides (CJC-1295, Ipamorelin) are less regulated, out-of-pocket, but have minimal side effects and preserve muscle mass. Both are valid tools for different weight loss strategies.
How much do weight loss peptides cost?
Pharmaceutical: Semaglutide (Wegovy) $1,300-1,600/month without insurance. Compounded semaglutide $250-400/month.
Research peptides: - AOD-9604: $80-150 per 6 weeks - CJC-1295 + Ipamorelin: $120-200 per 6 weeks - GHRP-6: $60-100 per 6 weeks
Additional costs: bacteriostatic water ($20-30), syringes ($15-25/100ct), medical consultations ($150-300 initial), lab work ($200-400/panel).
Budget option: $150-250/month with research peptides and self-administration. Premium clinic programs: $800-1,500/month all-inclusive.
Can you take peptides without injections?
Most weight loss peptides currently require injectable administration. Oral consumption destroys peptide bonds through stomach acid and digestive enzymes before they reach circulation.
The exception is oral semaglutide (Rybelsus), which uses an absorption enhancer called SNAC. However, oral bioavailability is less than 1% vs 90%+ for injections, requiring much higher doses.
Nasal spray and transdermal systems are in development but not yet commercially available for weight loss peptides.
Can peptides be combined with other weight loss medications?
With medical supervision, yes. GLP-1 agonists can be safely combined with GH-releasing peptides since they work through different mechanisms—one suppresses appetite, the other enhances metabolism.
Avoid combining: peptides with stimulant-based fat burners (phentermine) without blood pressure monitoring. Don't stack multiple experimental compounds without understanding interactions.
Best practice: Start with a single peptide for 4-8 weeks, assess tolerance, then add complementary compounds under medical guidance with blood work every 8-12 weeks.
The Bottom Line
The best peptides for weight loss work through distinct mechanisms: AOD-9604 for targeted lipolysis, CJC-1295 + Ipamorelin for GH-driven body recomposition, and semaglutide for appetite regulation with the strongest clinical evidence (15-17% body weight reduction).
Successful peptide therapy requires more than injections alone—caloric deficits, resistance training, and medical oversight produce superior outcomes while minimizing risks. Realistic expectations: 8-12 week evaluation periods, 0.5-2 pounds weekly fat loss depending on protocol.
Three things to remember:
- Work with qualified healthcare providers for screening and monitoring
- Start with single peptides before stacking—assess tolerance first
- Combine with proper nutrition and training for maximum results
Related articles: - AOD-9604 Before and After — clinical results and real-world evidence for AOD-9604 - Tesamorelin Dosage for Fat Loss — dosing protocols for visceral fat reduction - Sermorelin for Fat Loss — GH-pathway fat loss with sermorelin
Helpful Tools
Related Articles
AOD-9604 Before and After: Results
AOD-9604 before and after results are modest: 2-3 kg fat loss over 12 weeks in clinical trials. Learn realistic timelines and dosing protocols.
Sermorelin for Fat Loss: Dosing & Data
Sermorelin stimulates natural GH release to enhance fat oxidation. Dosing protocols (100-300mcg/day), cycling, and CJC-1295 comparison.
Does Tirzepatide Burn Fat?
Tirzepatide produced 33.9% fat mass loss in SURMOUNT-1. Learn how GLP-1/GIP dual agonism drives fat loss, body composition data, and how to protect lean mass.
Compound Semaglutide with B12: Guide
Compounded semaglutide with B12 combines a GLP-1 agonist with cyanocobalamin to offset GI malabsorption. Learn about 503A/503B regulations, cost, and safety.