The best peptides for libido are PT-141 (bremelanotide), kisspeptin, and melanotan II. PT-141 is the only FDA-approved option, sold as Vyleesi for hypoactive sexual desire disorder (HSDD) in premenopausal women. It works by activating melanocortin-4 receptors in the brain to increase desire directly, a completely different mechanism from Viagra or Cialis. Kisspeptin is the rising star: 2022 and 2023 clinical trials showed it boosts sexual brain activity and increases penile tumescence by 56% versus placebo.
These peptides address desire at its source, the central nervous system, rather than just enabling physical response through blood flow. That distinction matters. An estimated 10% of premenopausal women and 8% of men experience HSDD, a persistent lack of sexual desire that causes distress (Goldstein et al., 2017).
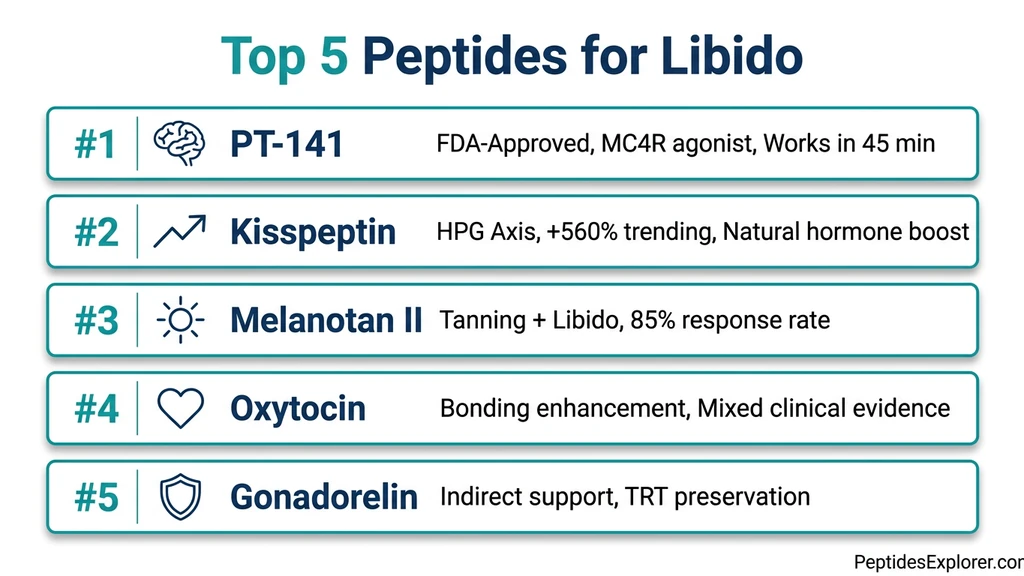
Below, we rank the top five peptides for libido based on clinical evidence, mechanism, and suitability for both men and women. No peptide covered here should replace professional medical advice.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
How Do Peptides Improve Libido?
Peptides for libido work through the brain's arousal circuitry, not through genital blood flow like PDE5 inhibitors (Viagra, Cialis). Two main pathways drive the effect.
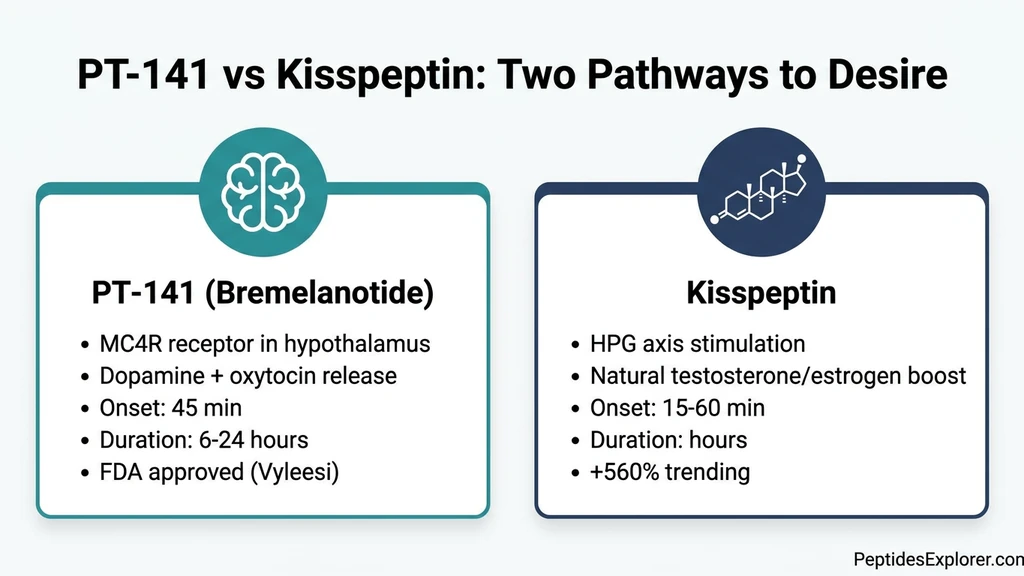
The melanocortin pathway. PT-141 and melanotan II activate melanocortin-4 receptors (MC4R) in the hypothalamus, specifically the paraventricular nucleus and medial preoptic area. This triggers dopamine release in the mesolimbic reward system and activates oxytocinergic neurons, producing both the psychological desire ("wanting") and the physical arousal response (Hadley, 2005).
The HPG axis pathway. Kisspeptin and gonadorelin stimulate the hypothalamic-pituitary-gonadal axis. Kisspeptin activates GnRH neurons, which release gonadotropin-releasing hormone, driving luteinizing hormone (LH) and follicle-stimulating hormone (FSH) secretion. The downstream result: increased testosterone in men and estrogen in women. Kisspeptin also acts directly on sexual brain regions, a dual mechanism unique to this peptide.
The clinical implication: these peptides can help people for whom Viagra does nothing. If the problem is desire rather than mechanics, brain-acting peptides are the appropriate tool.
1. PT-141 (Bremelanotide): The Gold Standard
PT-141 is the most proven peptide for libido. It holds FDA approval (as Vyleesi) and has the largest clinical dataset of any sexual desire peptide. It was derived from melanotan II by isolating the specific activity responsible for sexual arousal enhancement.
How PT-141 Works
PT-141 is a selective MC4R agonist. It activates melanocortin-4 receptors in the hypothalamus, triggering dopamine release in the mesolimbic pathway (the brain's reward and desire circuitry) and activating oxytocinergic neurons that drive genital arousal in both sexes.
The key distinction from Viagra: PT-141 acts on "wanting," not "plumbing." A man who cannot achieve desire will not benefit from blood flow enhancement. PT-141 addresses that upstream problem. It was developed by Palatin Technologies and approved by the FDA on June 21, 2019 as Vyleesi (AMAG Pharmaceuticals).
For the full molecular profile, see the PT-141 peptide page.
Clinical Evidence for PT-141
The RECONNECT Phase III trials, two identical randomized controlled studies, enrolled 1,247 premenopausal women with HSDD over 24 weeks. Results:
- Effect size for desire: 0.49 to 0.61
- Effect size for distress reduction: 0.60 to 0.62
- 25% of treated patients versus 17% placebo achieved clinically meaningful desire increase
- 35% versus 31% achieved clinically meaningful distress reduction
A 52-week open-label extension confirmed sustained efficacy and safety (PMC6819021, PMC6819023).
In men, PT-141 induced erections in patients who had failed PDE5 inhibitors, though this use remains off-label. The peptide works in men whose erectile dysfunction has a neurological or psychological basis rather than a purely vascular one (PMC8788464).
PT-141 Dosage
Beginner: 1 mg subcutaneous, 1 to 2 hours before sexual activity (to assess tolerance) Standard (FDA-approved for women): 1.75 mg subcutaneous, at least 45 minutes before activity Advanced (men, off-label): 2 mg subcutaneous
Maximum: one dose per 24 hours, no more than 8 doses per month. Onset occurs at 45 minutes to 2 hours. Effects on desire and arousal last 6 to 12 hours, with some users reporting residual effects up to 24 hours. The plasma half-life is approximately 2.5 hours, but the neurochemical effects persist longer.
Use the Peptide Reconstitution Calculator for precise dose preparation from lyophilized vials. For a step-by-step walkthrough, see How to Reconstitute Peptides.
PT-141 Side Effects
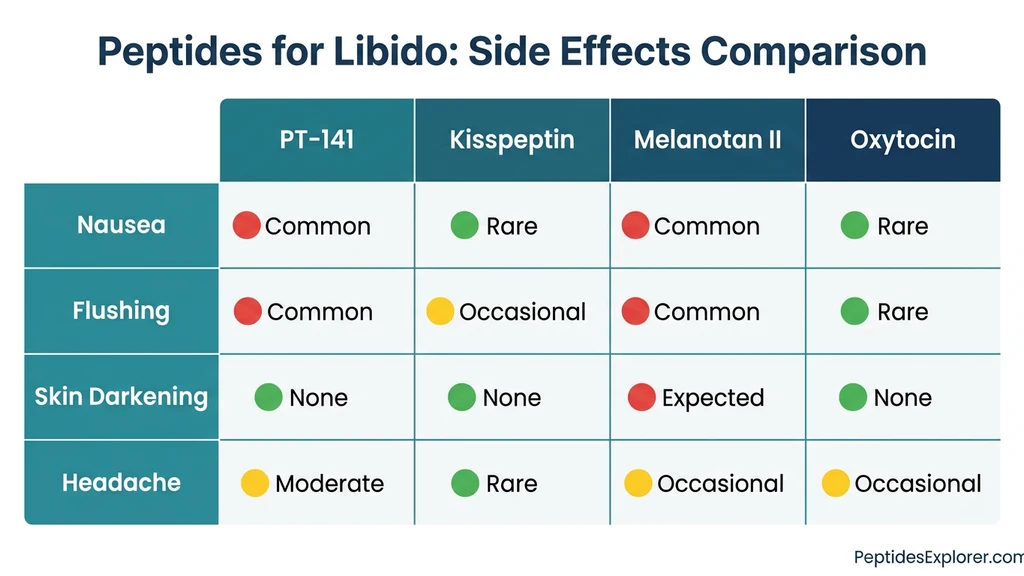
Nausea is the dominant side effect, affecting approximately 40% of users in clinical trials. It is worst with the first dose and diminishes with subsequent use. Flushing occurs in about 21% of users, headache in 12%.
Nausea management strategies: - Start at 1 mg rather than 1.75 mg for the first dose - Take ondansetron (Zofran) 30 minutes before injection - Eat a light meal 1 to 2 hours before dosing - BPC-157 at 250 to 500 mcg may reduce nausea (anecdotal, not clinically validated for this use)
Contraindications: uncontrolled hypertension, pregnancy, significant hepatic impairment. PT-141 causes a small, transient increase in blood pressure (FDA Label). For BPC-157 safety data, see the BPC-157 Side Effects Guide.
2. Kisspeptin: The Rising Star (+560% YoY Search Growth)
Kisspeptin search interest has surged 560% year-over-year, from 390 average monthly searches to 6,600 in December 2025. The reason: clinical trial results published in JAMA Network Open showed that a single kisspeptin injection measurably increased sexual desire and brain activity in both men and women.
How Kisspeptin Works
Kisspeptin is a neuropeptide encoded by the KISS1 gene, first discovered in 1996 in Hershey, Pennsylvania during melanoma research (hence the name, a nod to Hershey's Kisses). It sits at the top of the HPG axis: kisspeptin activates GnRH neurons, which drive LH and FSH release, which stimulate testosterone production in men and estrogen in women.
The libido effect operates through a dual mechanism. First, the indirect hormonal pathway: more kisspeptin means more testosterone or estrogen, which supports baseline desire. Second, a direct neural effect: kisspeptin activates brain regions involved in sexual processing. In men, it activates the amygdala. In women, it activates the hippocampus. These are distinct, sex-specific patterns of brain activation (PMC9898824).
The key distinction from PT-141: kisspeptin works WITH the body's natural hormone cascade rather than bypassing it. For the full peptide profile, see the kisspeptin page.
Clinical Evidence for Kisspeptin
Men (JAMA Network Open, 2023). A randomized, double-blind, placebo-controlled trial led by Professor Waljit Dhillo at Imperial College London enrolled 32 men with HSDD. A single kisspeptin-54 injection produced a 56% increase in penile tumescence versus placebo. Participants reported improved "happiness about sex" and enhanced sexual brain processing. No adverse effects were reported (PMC9898824).
Women (JAMA Network Open, 2022). A parallel trial of 32 women with low sexual desire found that kisspeptin deactivated brain regions associated with sexual self-judgement while increasing "feeling sexy" ratings and reducing sexual aversion. The neural effect was distinct from hormonal changes (JAMA 2797718).
2025 Review. A review in Trends in Endocrinology & Metabolism asked: "Can kisspeptin be a new treatment for sexual dysfunction?" The authors highlighted therapeutic potential but noted the short half-life (~28 minutes) as the primary delivery challenge (ScienceDirect, 2025).
Kisspeptin Dosage
Kisspeptin dosing is weight-based (nmol/kg), not a flat dose, and is not yet standardized outside clinical research.
Low exploratory: 1 nmol/kg subcutaneous (produces a measurable LH pulse within 30 minutes) Moderate support: 3 to 5 nmol/kg subcutaneous, daily or every other day, for 2 to 4 weeks
Two forms exist: kisspeptin-54 (full-length, longer-acting, better studied in clinical trials) and kisspeptin-10 (C-terminal fragment, shorter-acting). The half-life of kisspeptin-54 is approximately 28 minutes, which is the primary challenge for therapeutic development.
This is an advanced peptide. Blood work monitoring (LH, FSH, testosterone or estrogen) is essential before and during use. Use the Peptide Interaction Checker before combining with other compounds and the Peptide Unit Converter for weight-based dose calculations.
Why Kisspeptin Is Trending
Four factors drive the surge. First, the natural mechanism: kisspeptin works with the HPG axis rather than bypassing it, which appeals to users wary of synthetic interventions. Second, dual benefit: kisspeptin supports both libido and fertility, and is being tested in IVF protocols. Third, the safety profile in trials has been clean, with no reported adverse effects. Fourth, the audience is broader than "just a sex peptide." Kisspeptin is positioned as a reproductive health tool, which expands its appeal beyond the traditional peptide community.
3. Melanotan II: The Multi-Effect Peptide
Melanotan II is the parent compound from which PT-141 was derived. It is a non-selective melanocortin agonist, binding MC1R through MC5R. This gives it a dual effect: skin tanning (via MC1R) and libido enhancement (via MC4R).
In the Wessells et al. study, 17 of 20 men (85%) experienced erections with melanotan II versus placebo. Among treated men, 68% reported increased sexual desire compared to 19% in the placebo group (PubMed 11035391). Diamond et al. confirmed sexual function effects in both males and females (PubMed 15996790).
Dosage for libido: 0.25 to 0.5 mg subcutaneous during a loading phase (daily for 5 to 7 days), then 0.5 mg once or twice weekly for maintenance. For the full dosing protocol, see the melanotan 2 dosage guide.
Side effects reflect the non-selective binding: nausea, facial flushing, spontaneous erections, skin darkening, and new mole formation (nevi). The mole concern is clinically significant. Anyone with a history of melanoma or atypical moles should avoid melanotan II entirely.
Who it suits: users who want both tanning and libido enhancement from one peptide, and who accept the broader side effect profile. Who should avoid it: anyone with melanoma risk factors.
Melanotan II is not FDA-approved for any indication. PT-141 was developed specifically to isolate the sexual function activity of melanotan II while reducing the non-selective side effects.
4. Oxytocin: The Honest Assessment
Oxytocin is released naturally during skin contact, arousal, and orgasm. It modulates GABAergic interneurons in the amygdala and interacts with serotonergic systems. The mechanism for sexual enhancement is biologically sound.
The problem is clinical translation. A comprehensive review in Sexual Medicine Reviews found that "results of clinical studies mainly using intranasal oxytocin in men and women did not appear to confirm the facilitatory role found in animals" (PMC8509000). Animal data is strong. Human data is inconsistent.
One positive case study reported improved libido, erection quality, and orgasm intensity with intranasal oxytocin (PubMed 22458365). A preliminary survey of 26 men using oxytocin troches found that 56% responded positively.
Oxytocin's effects appear to be context-dependent. It enhances bonding and emotional closeness, which can indirectly support desire in relationship contexts. As a standalone libido treatment, the evidence does not yet support recommending it over PT-141 or kisspeptin.
Our assessment: mechanism is sound, preclinical support is strong, clinical translation has been disappointing. Best positioned as an adjunct to other therapies or for users specifically seeking emotional and bonding enhancement rather than raw desire amplification.
5. Gonadorelin: The Indirect Supporter
Gonadorelin is a synthetic GnRH analog that stimulates LH and FSH production. It does not directly enhance desire. Instead, it restores the hormonal foundation on which desire depends.
The primary use case: men on testosterone replacement therapy (TRT) who need to preserve testicular function and fertility. Exogenous testosterone suppresses the HPG axis. Gonadorelin keeps it active. The libido benefit is secondary to hormone normalization and typically takes 1 to 2 months to manifest.
Dosage: 100 to 200 mcg subcutaneous, two to three times per week.
Gonadorelin is not FDA-approved for libido enhancement or anti-aging purposes. It is approved as a diagnostic agent for evaluating pituitary function.
This is a supporting player. If your testosterone is low because of TRT-induced suppression, gonadorelin addresses the root cause. If your hormones are normal and desire is still low, gonadorelin will not help.
Peptides for Libido: Head-to-Head Comparison
No single resource in the current search landscape compares these peptides against each other. The table below covers mechanism, evidence, suitability, and practical considerations.
| Feature | PT-141 | Kisspeptin | Melanotan II | Oxytocin | Gonadorelin |
|---|---|---|---|---|---|
| Mechanism | MC4R: dopamine + oxytocin | HPG axis + direct neural | MC1R-MC5R (non-selective) | Amygdala GABA modulation | GnRH: LH/FSH: T/E2 |
| FDA approved | Yes (Vyleesi, women HSDD) | No | No | No | No (diagnostic only) |
| Evidence level | Phase III RCT (n=1,247) | Phase II RCT (n=32+32) | Phase II (small studies) | Mixed (inconclusive) | Indirect |
| Works for women | Yes (approved indication) | Yes (clinical data) | Yes (limited data) | Mixed | Indirect only |
| Works for men | Yes (off-label) | Yes (clinical data) | Yes (strong data) | Weak evidence | Indirect only |
| Onset | 45 min to 2 hours | 15 to 60 min (hormonal) | Hours (loading days) | Minutes (intranasal) | 1 to 2 months |
| Duration | 6 to 24 hours | Minutes to hours | Days to weeks (with loading) | Hours | Ongoing |
| Key side effect | Nausea (40%) | Minimal | Nausea + skin darkening | Nasal irritation | Minimal |
| Unique benefit | Only FDA-approved option | Natural HPG activation | Tanning + libido combo | Bonding enhancement | Preserves fertility on TRT |
| Difficulty | Beginner | Advanced | Intermediate | Beginner | Intermediate |
| Price | $$ | $$$ | $ | $$ | $$ |
Best Peptides for Female Libido
HSDD affects approximately 10% of premenopausal women, roughly 6 million in the United States. Before peptides, only two FDA-approved treatments existed: Vyleesi (PT-141, approved 2019) and Addyi (flibanserin, approved 2015).
PT-141 for women is the first choice. It is FDA-approved specifically for this indication. The RECONNECT trials enrolled premenopausal women. The dosage is 1.75 mg subcutaneous, as-needed, at least 45 minutes before sexual activity. Nausea management is the main practical challenge.
Kisspeptin for women showed that a single injection deactivated brain regions associated with sexual self-judgement while increasing "feeling sexy" ratings. The JAMA 2022 trial demonstrated reduced sexual aversion in women with low desire. Kisspeptin also supports fertility, which makes it appealing for women planning conception.
Oxytocin for women may enhance emotional and bonding aspects of desire. The evidence is mixed, but the mechanism aligns with relationship-based desire patterns that are more common in women than men.
Hormonal context matters. Menopause, hormonal contraception, and postpartum states all affect peptide response. Baseline hormone testing is recommended before starting any protocol. Our peptide safety guide covers recommended lab work.
Practical recommendation: PT-141 as the primary option (proven efficacy, FDA-approved). Kisspeptin for women interested in hormonal optimization and fertility preservation.
Best Peptides for Male Libido
The primary candidates are men for whom PDE5 inhibitors (Viagra, Cialis) are insufficient. When erectile dysfunction has a neurological or psychological basis, blood flow agents fail. Brain-acting peptides address the upstream problem.
PT-141 for men is used off-label at 1 to 2 mg subcutaneous. Clinical data shows it induces erections in men who failed PDE5 inhibitors. Some men combine PT-141 with Viagra for both desire enhancement and mechanical support.
Kisspeptin for men produced a 56% increase in penile tumescence versus placebo in the JAMA 2023 trial of 32 men with HSDD. It also boosts testosterone naturally through HPG axis stimulation, offering a dual benefit: desire enhancement and hormonal optimization.
Melanotan II for men has the strongest erection response data: 85% of men in the Wessells study experienced erections. The trade-off is a broader side effect profile including skin darkening and mole changes. Only appropriate for men who also want the tanning effect or who accept the cosmetic changes.
Gonadorelin for men on TRT preserves testicular function and endogenous hormone production. It does not directly boost desire but restores the hormonal environment that supports it.
Practical recommendation: PT-141 for acute, on-demand situations. Kisspeptin for ongoing hormonal optimization. Melanotan II only if tanning is also desired. Gonadorelin only if on TRT.
How to Choose the Right Peptide for Your Goals
The decision depends on what you need, how fast you need it, and your tolerance for side effects.
Want proven, FDA-approved, on-demand use? PT-141. The most evidence, the simplest protocol. Take it when needed.
Want natural hormone optimization alongside libido? Kisspeptin. Works with the body's own HPG axis. Best for users willing to commit to daily or every-other-day dosing and blood work monitoring.
Want tanning and libido from one peptide? Melanotan II. Accept the broader side effect profile.
Want emotional and bonding enhancement? Oxytocin. Understand the limited clinical evidence.
On TRT and need hormonal preservation? Gonadorelin. The libido effect is indirect and takes 1 to 2 months.
Stacking for maximum effect? Kisspeptin daily (hormonal base, HPG axis stimulation) plus PT-141 as-needed (acute MC4R-mediated desire boost). The two peptides work through completely different pathways and do not compete for receptors. Clinical data on this specific combination is limited, but the pharmacological rationale is sound. For stacking principles, see our peptide stacking guide and use the Peptide Stack Calculator for dosing logistics.
If you are new to peptides and want broader orientation, see our Getting Started with Peptides guide. For injection technique, see the Peptide Injection Guide. If performance anxiety contributes to your situation, see Peptides for Anxiety. Not sure which peptide fits your goals? Take the Peptide Quiz for a personalized recommendation.
Frequently Asked Questions
What is the best peptide for female libido?
PT-141 (bremelanotide) is the best-supported peptide for female libido. It is FDA-approved as Vyleesi for hypoactive sexual desire disorder (HSDD) in premenopausal women, based on Phase III trials involving 1,247 women. Kisspeptin is a promising alternative with clinical data showing it increases sexual desire ratings and reduces sexual aversion in women.
How does PT-141 work differently from Viagra?
PT-141 works in the brain by activating melanocortin-4 receptors (MC4R) to increase sexual desire through dopamine and oxytocin pathways. Viagra works in the genitals by inhibiting PDE5 to increase blood flow. PT-141 addresses desire (the wanting), while Viagra addresses erection mechanics. Some men use both together.
What are the side effects of PT-141?
The most common side effect is nausea, affecting about 40% of users in clinical trials. Flushing occurs in about 21% and headache in 12%. Nausea typically diminishes after the first few uses. Starting at 1 mg instead of the full 1.75 mg dose and taking anti-nausea medication beforehand can help.
Is kisspeptin better than PT-141 for libido?
They work through different mechanisms and serve different purposes. PT-141 provides acute, on-demand libido enhancement within 45 minutes. Kisspeptin stimulates the body's natural hormone production, supporting libido through testosterone or estrogen optimization over days to weeks. PT-141 has stronger clinical evidence (Phase III, FDA approval). Kisspeptin is earlier in development but shows significant promise.
Can women use peptides for libido?
Yes. PT-141 is specifically FDA-approved for women with HSDD. Kisspeptin has positive clinical trial data in women showing reduced sexual aversion and increased desire ratings. HSDD affects approximately 10% of premenopausal women, and these peptides offer alternatives to the limited treatments previously available.
What is the correct PT-141 dosage?
The FDA-approved dose is 1.75 mg subcutaneous injection, taken at least 45 minutes before sexual activity. Beginners should start at 1 mg to assess tolerance. Men sometimes use up to 2 mg off-label. Do not exceed one dose per 24 hours or eight doses per month.
How long does PT-141 take to work?
PT-141 typically begins working within 45 minutes to 2 hours after subcutaneous injection. Peak plasma concentration occurs at about 1 hour. Effects on desire and arousal last 6 to 12 hours, with some users reporting residual effects up to 24 hours.
What is the kisspeptin dosage for libido?
Kisspeptin dosing is weight-based (nmol/kg), not a flat dose, and is not standardized outside clinical research. Research protocols use 1 to 10 nmol/kg subcutaneously. Kisspeptin-54 (full-length) is better studied than kisspeptin-10 (fragment). The short half-life of approximately 28 minutes is a therapeutic challenge. Blood work monitoring is essential.
Can you stack kisspeptin and PT-141 together?
Yes. Kisspeptin and PT-141 work through completely different pathways (HPG axis versus melanocortin system) and do not compete for receptors. A rational protocol is kisspeptin daily for ongoing hormonal optimization, with PT-141 as-needed for acute libido enhancement. Clinical data on this specific combination is limited, but the pharmacological rationale is sound.
Is melanotan II safe for libido enhancement?
Melanotan II has clinical data supporting libido enhancement (85% erection response rate in one study), but it is not FDA-approved and carries more side effects than PT-141 due to non-selective receptor binding. Risks include skin darkening, new mole formation, and nausea. Anyone with a history of melanoma or atypical moles should avoid it. PT-141 was developed as the safer, more targeted alternative.
The Bottom Line
PT-141 remains the gold standard for peptide-based libido enhancement: FDA-approved, well-studied, effective in both sexes. For users seeking a more natural approach, kisspeptin offers a compelling alternative that works with the body's own hormonal architecture. Melanotan II suits a niche audience willing to accept broader side effects for a tanning bonus. Oxytocin's promise exceeds its clinical proof. Gonadorelin serves men on TRT who need hormonal axis preservation.
The field is moving fast. Kisspeptin's 560% search growth reflects genuine scientific momentum, not hype. The JAMA trials from 2022 and 2023 represent the first rigorous evidence that a peptide can enhance desire through the body's own reproductive signaling system. Longer-acting kisspeptin analogs are in development.
Choose the peptide that matches your specific situation. Use the comparison table above to narrow your options. Start conservatively with dosing. Monitor your response.
For peptide profiles, dosage calculators, and interaction checking, visit PeptidesExplorer.com. For all dosing references in one place, see the peptide dosage chart. For proper peptide handling, see how to store peptides and where to buy peptides in 2026.
Related Articles: - Melanotan 2 Dosage Protocol - Peptides for Anxiety - Peptide Safety Guide - Peptide Stacking Guide - Getting Started with Peptides
Helpful Tools
Related Articles
PT-141 Peptide: What It Is and How It Works
PT-141 peptide (bremelanotide) explained: MC4R mechanism in the brain, FDA approval as Vyleesi for HSDD, real benefits, RECONNECT trial data, and safety limits.
Peptides for Men: Best Options by Goal (2026 Guide)
Best peptides for men ranked by goal: muscle growth, fat loss, libido, testosterone, sleep, hair loss, and longevity. Protocols with doses.
PT-141 for Men: Dosage, Results & How It Works
PT-141 (bremelanotide) for men: 34% success in Viagra non-responders. Dosage, mechanism, clinical trial data, side effects, and comparison to PDE5 inhibitors.
Kisspeptin Peptide: What the Human Evidence Shows
Kisspeptin peptide sits upstream of GnRH and drives LH, FSH, and testosterone. Human trial doses, kisspeptin-10 vs 54, and the desensitization risk.