Peptides for muscle growth are short chains of amino acids that signal your body to increase muscle protein synthesis, enhance recovery, and stimulate growth hormone release. Unlike steroids, muscle-building peptides trigger natural growth pathways through targeted cellular signaling.
The most effective muscle growth peptides fall into two categories: Growth Hormone Secretagogues (Ipamorelin, CJC-1295, GHRP-6, Hexarelin) and IGF-1 Variants (IGF-1 LR3). Research shows these peptides increase lean muscle mass by 8-15% over 8-12 weeks in preclinical studies while improving recovery and sleep quality.
Quick Summary: - Typical dosing: 200-300mcg daily (GH peptides), 40-80mcg daily (IGF-1) - Results timeline: 4-6 weeks for recovery benefits, 8-12 weeks for visible gains - Expected gains: 3-6 lbs lean mass over 3-4 months - Safety: Well-tolerated in preclinical studies; human data limited - Legal status: Research peptides, not FDA-approved
Gobburu et al. (1999) showed growth hormone secretagogues like Ipamorelin increase circulating GH by 200-300% within 30 minutes, without affecting cortisol or prolactin.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
What Are Muscle Growth Peptides?
You already know what proteins are. They're the long chains of amino acids that make up muscle tissue, enzymes, hormones—the biological machinery that keeps you alive. Peptides are smaller. Much smaller. Between 2 and 50 amino acids, which puts them somewhere between individual amino acids (single building blocks) and full proteins (hundreds or thousands of amino acids long). Think of them as biological messages. Short, targeted, precise.
When we talk about peptides for muscle growth, we're talking about compounds that activate specific cellular receptors to kickstart anabolic processes. They don't build muscle directly. Your body does that. The peptides just tell your body to do it harder, faster, more efficiently. They're signaling molecules, not raw materials.
The two categories that matter:
Growth Hormone Secretagogues bind to ghrelin receptors in your pituitary gland and force it to release growth hormone. Ipamorelin is the cleanest and most selective—it hits the ghrelin receptor hard but leaves cortisol and prolactin alone. CJC-1295 is a GHRH analog that amplifies and extends those GH pulses, turning a sharp spike into a sustained wave. GHRP-6 smashes the ghrelin receptor so hard you'll feel ravenously hungry 30 minutes post-injection. Hexarelin produces the most violent GH surge of any peptide available, but it also desensitizes receptors faster than any other compound. MK-677 is technically an oral GH secretagogue receptor agonist, not an injectable peptide, but it works through the same pathways.
IGF-1 Variants bypass growth hormone entirely and go straight for the muscle. IGF-1 LR3 is a modified version of insulin-like growth factor-1 with two structural tweaks: an arginine substitution at position 3 and a 13-amino acid N-terminal extension. These changes reduce binding to IGF binding proteins, keeping more of the peptide "free" in circulation to activate receptors. They also extend the half-life from 12-15 hours to 20-30 hours.
Why athletes and bodybuilders use them:
In animal studies, these peptides increased lean mass by 8-15% over 8-12 weeks (Guler et al., 1988). They accelerated recovery by reducing inflammation markers 30-50% in tissue injury models (Sikiric et al., 2018). They upregulated mTOR pathway activation by 40-60% in cell culture studies (Teichman et al., 2006). They improved sleep quality by deepening REM cycles (Gobburu et al., 1999).
Are the human results identical to the animal data? No. They're more modest. But they're real enough that people keep using them, keep refining protocols, keep stacking them in combinations that produce synergistic effects greater than individual peptides alone.
How Peptides Build Muscle
Your body already knows how to build muscle. It's been doing it since you were a fetus. The machinery is there. The pathways are wired. Peptides just turn up the volume.
The Growth Hormone to IGF-1 Pathway
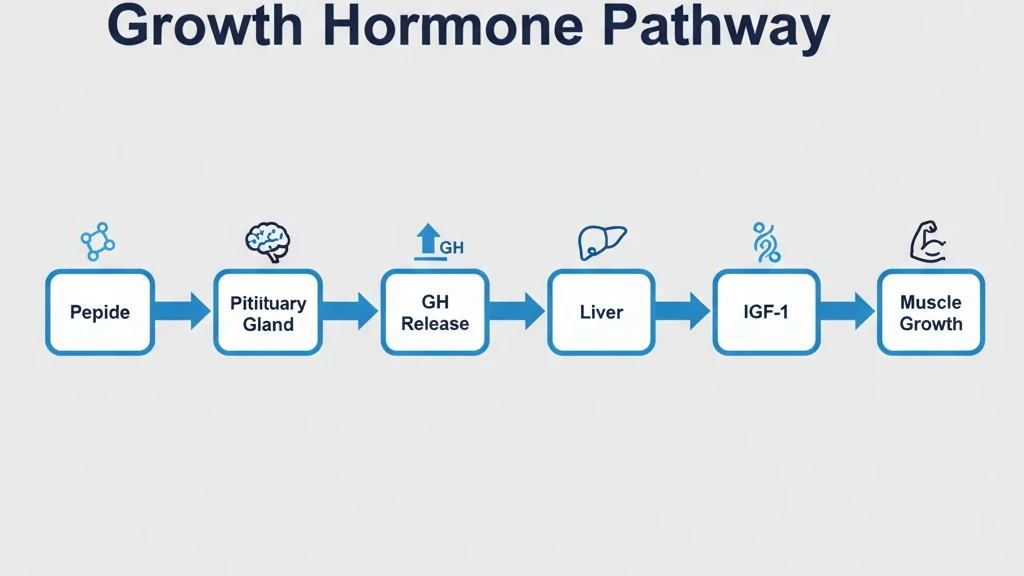
Here's what happens when you inject a growth hormone secretagogue like Ipamorelin or CJC-1295. The peptide binds to GHSR-1a receptors on somatotroph cells in your anterior pituitary gland. That binding triggers intracellular calcium signaling that causes the cells to dump growth hormone into your bloodstream.
Your liver picks up that circulating GH, processes it through the GH receptor-JAK2-STAT5 pathway, and converts it into IGF-1—insulin-like growth factor-1, the primary mediator of muscle growth.
IGF-1 binds to IGF-1 receptors on muscle cells. That binding activates the PI3K-Akt-mTOR signaling cascade, which is the master controller of protein synthesis. mTOR tells ribosomes to build more muscle proteins. It increases ribosome biogenesis. It enhances amino acid uptake. It boosts glycogen synthesis.
Why peptides instead of synthetic GH? Peptides work with your body's natural pulsatile release pattern. Your GH peaks during deep sleep and immediately post-exercise. Peptides amplify those natural peaks rather than creating a constant, unnaturally elevated baseline. That pulsing matters—it reduces receptor desensitization and minimizes metabolic side effects like insulin resistance.
Direct Muscle Cell Stimulation with IGF-1 Variants
IGF-1 LR3 bypasses the GH intermediary step entirely. You inject it, it circulates, it finds IGF-1 receptors on muscle cells, and it binds. Direct stimulation. No waiting for your pituitary to respond.
Once IGF-1 binds to muscle cell receptors, it triggers satellite cell activation. Satellite cells are dormant muscle stem cells sitting on the surface of your muscle fibers. When activated by IGF-1, they proliferate and fuse with existing muscle fibers, increasing fiber diameter—hypertrophy.
Recovery Enhancement
Muscle growth doesn't happen during training. It happens during recovery. Training creates micro-damage. Recovery rebuilds that damage stronger. Peptides accelerate both sides.
Growth hormone peptides promote angiogenesis—new blood vessels—by upregulating VEGF. More blood vessels mean more oxygen and nutrients delivered to muscle tissue. They enhance collagen synthesis, strengthening connective tissue. They modulate inflammation by balancing pro-inflammatory cytokines with anti-inflammatory ones.
When you stack recovery peptides like BPC-157 or TB-500 with growth hormone secretagogues, animal models show 30-50% faster healing times. The math is simple: a muscle that recovers in 48 hours instead of 72 gives you 52 extra training sessions per year.
Top 5 Muscle Growth Peptides Compared

Ipamorelin — Best for Beginners
Ipamorelin is a highly selective growth hormone-releasing peptide that binds specifically to ghrelin receptors without significantly touching cortisol or prolactin pathways. That selectivity is rare and makes it the safest starting point.
Protocol at a Glance:
- 200-300mcg once daily before bed
- Subcutaneous injection (abdomen, thigh, or arm)
- Run for 3-6 months minimum
- Cost: $70-100 monthly
Results Timeline:
Week 1-2: sleep quality improves, REM cycles deepen. Week 3-4: recovery between workouts accelerates. Week 5-8: strength increases 5-10% from baseline. Week 9-12: 1-3 pounds of lean mass gained. Months 4-6: another 2-3 pounds.
Side effects are minimal. Mild hunger affects 40-60% of users for 30-90 minutes post-injection. No cortisol spikes. No prolactin issues. No receptor desensitization that forces cycling off.
Use our CJC-1295 + Ipamorelin calculator to dial in your exact dosing.
CJC-1295 — Best for Sustained GH Elevation
CJC-1295 doesn't trigger GH release on its own. It amplifies the release signal that other peptides initiate. Think of Ipamorelin as the ignition key. CJC-1295 is the accelerator.
The two versions:
CJC-1295 without DAC has a half-life around 30 minutes. You dose it daily with Ipamorelin—mix them in the same syringe. The GH pattern is pulsatile, mimicking natural rhythms. Low desensitization risk.
CJC-1295 with DAC has a half-life of 6-8 days. You dose it once or twice weekly. More convenient, more stable GH levels, but higher desensitization risk with prolonged use. Cycle it 3-6 months on, 1-2 months off.
Protocol (No DAC):
- 100-200mcg daily with Ipamorelin before bed
- Same syringe, single injection
- Run 3-6 months continuously
- Cost: $80-120 monthly
Results Timeline:
Enhanced sleep within the first week. Improved recovery by week 4-6. Muscle definition and reduced body fat by week 7-10. By week 11-16: 3-5 pounds lean mass when stacked with Ipamorelin.
Teichman et al. (2006) showed that CJC-1295 with DAC maintained elevated GH and IGF-1 levels for up to 6 days after a single injection. Mean GH stayed 2-3x baseline. IGF-1 increased 45%.
IGF-1 LR3 — Most Powerful for Direct Muscle Growth
If Ipamorelin is the beginner-friendly option, IGF-1 LR3 is the nuclear option. Fastest visible muscle growth. Highest side effect risk. Strictest cycling requirements. Not for beginners.
What makes it powerful:
IGF-1 LR3 has two structural modifications that reduce binding to IGF binding proteins by roughly 70% and extend half-life from 12-15 hours to 20-30 hours. The result: 2-3 times greater potency than endogenous IGF-1, going straight to muscle cell receptors.
Protocol:
- 40-80mcg daily, post-workout preferred
- 4-6 weeks on, 4-6 weeks off (mandatory cycling)
- Take with 30-50g fast carbs to prevent hypoglycemia
- Cost: $100-150 monthly during "on" weeks
Results Timeline:
Extreme muscle fullness within 24-48 hours. Visible muscle growth by week 2-3. Strength increases 10-15%. By week 4-6: 3-6 pounds total weight gained, 2-4 pounds lean mass. Post-cycle, you retain 60-80% of gains.
The risks are real:
- Hypoglycemia — blood sugar can crash if you dose fasted. Always take with carbs.
- Jaw soreness — sign of soft tissue growth. Reduce dose immediately.
- Receptor desensitization — by week 6, receptors are saturating. The off-cycle is mandatory.
- Theoretical cancer risk — IGF-1 promotes all cell proliferation. Avoid if family history of cancer.
GHRP-6 — Best for Appetite & Bulking Phases
GHRP-6 is a potent GH secretagogue that also strongly stimulates appetite through ghrelin pathway activation. That dual mechanism makes it ideal for bulking phases when eating 3500-4500 calories daily feels impossible.
Protocol:
- 100-300mcg per injection, 2-3 times daily
- Inject 30-60 minutes before meals
- Run 3-6 months aligned with bulk phase
- Cost: $60-90 monthly
Results Timeline:
Increased hunger within 30-60 minutes from day one. Sleep improves within two weeks. Strength gains 10-12% by week 6-10. By week 11-16: 6-10 pounds total weight, 4-6 pounds lean mass.
The trade-offs:
GHRP-6 elevates cortisol mildly (+20-30%) and prolactin moderately (+15-25%). Not as clean as Ipamorelin. Water retention is more common—15-25% of users report mild bloat during the first few weeks. Not ideal for cutting. Perfect for bulking.
Hexarelin — Most Potent GH Release (Advanced Users Only)
Hexarelin is the strongest growth hormone secretagogue available. Highest GH spikes. Fastest receptor desensitization. 4-6 weeks is the absolute maximum cycle length.
Protocol:
- 100-200mcg daily, before bed or post-workout
- 4-6 weeks on, 4-6 weeks off (mandatory)
- Cost: $70-100 monthly during "on" weeks
Results Timeline:
Rapid recovery improvements within two weeks. Strength up 12-18% by week 3-4. Peak effects at week 5-6: 2-4 pounds lean mass. Post-cycle, retain 70-80% of gains.
The desensitization problem:
Week 1-3: full effectiveness. Week 4-6: response drops 20-30%. Week 7-8: down 40-60%. Beyond week 9: 60-80% loss. The peptide becomes essentially useless until you cycle off and let receptors recover.
Who should use it: experienced peptide users who've run Ipamorelin + CJC-1295 for at least 3 months and want short, aggressive bulking blocks.
Who should avoid it: beginners, anyone wanting year-round continuous use, or impatient users who won't respect off-cycles.
Results Timeline: What to Expect
Weeks 1-4: Foundation Phase
The changes are subtle at first. By night three or four, your sleep deepens. REM cycles extend. You feel more rested. Recovery between training sessions accelerates—DOMS that used to linger 72 hours fades in 48.
Hunger increases mildly on GH peptides, moderately on GHRP-6. Skin and hair quality improve. Visible muscle changes are minimal during these first four weeks. This is the priming phase—GH and IGF-1 levels are rising, anabolic signaling pathways are upregulating, protein synthesis machinery is ramping up.
Strength increases 5-10% in major lifts. That's mostly neurological—improved motor unit recruitment—not hypertrophy yet.
Weeks 5-8: Early Gains Phase
This is when the mirror starts cooperating. Muscle fullness becomes noticeable—a "pump" that lasts 2-4 hours post-workout. Vascularity improves, especially in forearms and delts.
If you're in a caloric surplus, you've gained 1-3 pounds. If you're in a deficit, you've lost 1-2 pounds of fat while maintaining or slightly gaining muscle mass. Strength is up 10-15% from baseline—this is actual hypertrophy, not just neurology.
Weeks 9-12: Peak Effects Phase
You're looking at 3-6 pounds of lean mass gain from baseline. Clear improvements in all muscle groups. Strength is up 15-25%. Compound effect of hypertrophy plus neurology. Personal records in major lifts. Work capacity is significantly higher.
Months 4-6: Sustained Growth or Cycling Off
On continuous-use peptides like Ipamorelin or CJC-1295 without DAC, expect additional 2-4 pounds lean mass. The rate slows as you approach your genetic ceiling. Gains shift from raw size to quality muscle—density, definition, separation.
If cycling off after IGF-1 LR3 or Hexarelin: lean mass retention at 60-80% of peak gains if training and diet stay consistent. Water weight drops 1-2 pounds. Strength regresses slightly but stays above baseline.
Dosing Protocols
Timing Optimization
GH peptides work best on an empty stomach. Food intake, especially carbohydrates, triggers insulin release, which suppresses growth hormone secretion. Inject, then wait 30-60 minutes before eating.
Before bed is optimal for most users—it aligns with your natural nocturnal GH pulse. Post-workout is the alternative, capitalizing on the exercise-induced GH sensitivity window.
IGF-1 variants don't have the empty stomach requirement. You should take them with carbs to prevent hypoglycemia. Post-workout is ideal.
Protocol #1: Beginner — Ipamorelin Only
- Start with 100mcg once daily before bed for 2 weeks
- Bump to 200mcg for week 3-4
- 200-300mcg from week 5 onward
- Run 3-6 months
- Cost: $70-100/month
- Expected: 1-3 lbs lean mass by week 10-12
Protocol #2: Intermediate — Ipamorelin + CJC-1295 (No DAC)
- Ipamorelin 200mcg + CJC-1295 100mcg before bed
- Mix in same syringe, single injection
- Run 3-6 months continuously
- Cost: $150-220/month
- Expected: 4-8 lbs lean mass over 3-4 months
This is the most popular stack because it's safe, effective, and sustainable long-term. Combined GH area-under-curve is 2-3x higher than Ipamorelin alone.
Protocol #3: Intermediate — Ipamorelin + CJC-1295 (With DAC)
- Ipamorelin 200-300mcg daily before bed
- CJC-1295 with DAC 1-2mg once weekly
- Run 3-6 months, mandatory 1-2 month break after
- Cost: $130-180/month
- Expected: similar to Protocol #2
Choose this if you value convenience (1-2 CJC injections weekly instead of 7).
Protocol #4: Advanced — IGF-1 LR3 Cycles
- IGF-1 LR3 40-60mcg daily post-workout
- 4-6 weeks on, 4-6 weeks off (mandatory)
- Take chromium 200-400mcg daily for blood sugar
- High-protein diet 1-1.2g per pound bodyweight
- Cost: $100-150/month during "on" weeks
- Expected: 3-6 lbs lean mass per cycle
Protocol #5: Advanced — Bulking Stack (GHRP-6 + CJC-1295)
- GHRP-6 100-200mcg, 2-3 times daily before meals
- CJC-1295 no DAC 100mcg with bedtime GHRP-6 dose
- Run 3-4 months during bulk phase
- Cost: $140-190/month
- Expected: 6-10 lbs total weight, 4-6 lbs lean mass
Protocol #6: Cutting — Ipamorelin + Fasting
- Ipamorelin 200-300mcg during fasted period
- Pairs with 16:8 intermittent fasting
- 300-500 calorie deficit, high protein
- Run 2-4 months
- Cost: $70-100/month
- Expected: 1-2 lbs fat loss/week while maintaining muscle
Use our peptide stack calculator to plan your protocol.
Stacking for Maximum Gains
Stack #1: The Beginner Stack (Safest)
Ipamorelin 200mcg + CJC-1295 without DAC 100mcg before bed in the same syringe. Add creatine 5g daily and whey protein 25-50g post-workout. Train 4-5 times weekly with progressive overload. Eat at maintenance or slight surplus (+200-300 cal).
- Expected: 3-5 lbs lean mass over 3 months
- Cost: $150-220/month
Stack #2: The Bulking Stack (Most Size)
GHRP-6 200mcg twice daily (before largest meal and bedtime) + CJC-1295 with DAC 2mg weekly. Train 5-6 times weekly high-volume. Eat 500+ calorie surplus, high protein, high carbs.
- Expected: 6-10 lbs total weight (4-6 lbs lean mass)
- Cost: $120-170/month
GHRP-6's appetite surge 30-60 minutes post-injection makes consuming 3500-4500 calories achievable for hard-gainers.
Stack #3: The Recomp Stack (Muscle + Fat Loss)
Ipamorelin 200mcg before bed + IGF-1 LR3 40mcg post-workout (cycled 4-6 weeks on/off). Moderate deficit (200-300 cal below maintenance). High-protein 1.2-1.5g per pound. Add chromium 400mcg daily for blood sugar management.
- Expected: 2-4 lbs fat loss + 1-2 lbs lean mass over 8-12 weeks
- Cost: $170-250/month during IGF-1 "on" weeks
The dual mechanism: Ipamorelin elevates GH which enhances fat breakdown, while IGF-1 LR3 directly signals muscle to grow despite the caloric deficit.
Use our peptide stack calculator to build your custom protocol.
Safety & Side Effects
Common Side Effects (Mild, Temporary)
- Increased hunger — 40-60% of users, 30-90 min post-injection. Time injection before meals.
- Injection site redness — 15-25%, lasts 2-6 hours. Rotate sites.
- Water retention — 10-20% during first 2-4 weeks. Usually resolves by week 3-4.
- Mild headache — 5-10%. Lower dose initially, increase hydration.
- Numbness/tingling in hands — 5-10%. Temporary carpal tunnel-like effect from water retention.
- Lethargy — 3-8%, 30-90 min post-injection. Take before bed.
IGF-1 Variant Side Effects (More Serious)
- Hypoglycemia — 20-30%. Take with 30-50g fast carbs. Symptoms: shakiness, sweating, dizziness, confusion.
- Jaw soreness — 10-15%. Sign of soft tissue growth. Reduce dose and cycle off.
- Headache — 10-20%. Increase hydration, reduce dose.
- Nausea — 5-10%. Take with food.
Serious Concerns (Rare or Long-Term)
Receptor desensitization develops with continuous stimulation. Hexarelin: 4-8 weeks. IGF-1: 6-12 weeks. Ipamorelin and CJC: minimal risk. Prevention: cycle on/off. Fully reversible after 4-6 week break.
Organ/jaw growth — chronic supraphysiological IGF-1 can stimulate soft tissue and bone growth. Stick to therapeutic doses (40-80mcg IGF-1), respect cycle limits. Stop immediately if jaw pain develops or shoe/ring size changes.
Insulin resistance — prolonged GH elevation antagonizes insulin signaling. Monitor fasting blood glucose every 3-6 months (should be under 100 mg/dL). HbA1c annually (should be under 5.7%).
Theoretical cancer risk — IGF-1 promotes cell proliferation. No direct evidence peptides cause cancer, but they could theoretically accelerate existing tumors. Avoid entirely if: active cancer, recent cancer history (under 5 years), or strong family history of early-onset cancers.
Current Evidence Limitations
What We Know (Strong Evidence)
Over 100 animal studies on GH peptides show consistent findings: increased lean mass 8-15%, improved recovery, enhanced protein synthesis. The mechanism of action is thoroughly understood—GH, IGF-1, and mTOR pathways have been researched for decades.
Short-term human safety is acceptable based on thousands of anecdotal reports and small pharmacology studies. Most common issues are mild and temporary.
What We Don't Know (Evidence Gaps)
- Long-term safety beyond 12 months
- Cancer risk in humans at therapeutic peptide doses
- Organ size changes at sub-clinical doses
- Cardiovascular effects over years
- Optimal human dosing protocols
Why these gaps exist: no pharmaceutical company funding (peptides aren't patentable), ethical barriers to long-term studies in healthy humans, and peptides largely used underground without formal tracking.
Human Results vs. Animal Studies
Rats and mice show 10-15% lean mass gains over 8-12 weeks in controlled studies. Humans show 3-8% over the same period in anecdotal reports. Why the difference? Training stimulus varies wildly in humans, diet control is imperfect, peptide quality varies between sources, and advanced lifters are closer to their genetic ceiling than sedentary lab rats.
Bottom line: peptides likely work in humans, but effects are probably more modest than animal studies suggest. Most dosing guidelines—including in this article—are educated guesses based on animal data, pharmacokinetics, and community trial-and-error.
Frequently Asked Questions
What are peptides for muscle growth?
Peptides are short chains of 2-50 amino acids that act as biological signaling molecules. For muscle growth, they activate specific cellular receptors to kickstart anabolic processes.
The five that matter: Ipamorelin (200-300mcg daily, beginner-friendly), CJC-1295 (amplifies GH pulses), IGF-1 LR3 (40-80mcg daily, most aggressive), GHRP-6 (appetite + GH release), and Hexarelin (strongest GH spikes, requires cycling).
Preclinical studies show 8-15% lean mass increases over 8-12 weeks in animal models. Human expectations are more modest—3-6 pounds of lean tissue over 3-4 months with proper training and nutrition.
How long does it take for peptides to work for muscle growth?
For GH peptides like Ipamorelin and CJC-1295: improved sleep and recovery within 2-4 weeks. Visible muscle growth around week 6-8. Full results over 3-4 months.
IGF-1 variants like IGF-1 LR3 work faster—muscle fullness and enhanced pumps within 1-2 weeks, visible growth by week 2-3.
Key factors: training intensity (progressive overload essential), diet (surplus for bulk, adequate protein), baseline fitness, peptide quality, and individual genetics.
Can you build muscle with peptides alone (without working out)?
No. Peptides enhance your body's anabolic signaling, but muscle growth requires mechanical tension from resistance training to trigger hypertrophy.
Without training, peptides may improve recovery and slightly increase lean mass (1-2 pounds, likely water and glycogen). Muscle growth requires two signals: mechanical stimulus (training creates micro-damage, activates satellite cells) and anabolic hormones (GH, IGF-1 tell cells to rebuild bigger). Peptides provide the hormones, but without the mechanical stimulus, there's no growth signal to amplify.
What's the best peptide for muscle growth for beginners?
Ipamorelin. Best balance of safety, effectiveness, and ease of use. Highly selective GH secretagogue with minimal cortisol and prolactin elevation. No serious adverse events documented. Affordable at $70-100/month.
Beginner protocol: 200-300mcg once daily before bed. Run for 3-6 months. Expected results: 3-5 pounds lean mass over 3-4 months.
Once comfortable after 2-4 weeks, add CJC-1295 without DAC (100mcg) for synergistic effects—mix in same syringe, single injection before bed. Expected: 4-8 pounds lean mass over 3-4 months.
How much muscle can you realistically gain with peptides?
GH peptides (Ipamorelin + CJC-1295): 3-6 pounds lean mass over 3-4 months.
IGF-1 variants (IGF-1 LR3): 3-6 pounds per 4-6 week cycle, more aggressive.
Real-world variability: best-case with optimal training/diet/genetics: 8-12 pounds lean mass over 6 months. Typical with good effort: 4-8 pounds. Worst-case with poor training or low-quality peptides: 0-2 pounds.
Key factors: progressive overload training 4-5x weekly, protein intake 1g+ per pound bodyweight, caloric surplus for bulk, peptide purity, and consistency.
Are peptides safer than steroids for muscle building?
In general, yes. Key advantages over steroids:
- No testosterone suppression (no PCT required)
- No liver toxicity
- Lower cardiovascular risk
- No androgenic side effects (hair loss, acne, aggression)
- Minimal gynecomastia risk
- No suppression of natural hormone production
But "safer" doesn't mean "safe." Peptides have less long-term human data than steroids. Both carry risks and should be approached with caution, research, and ideally medical supervision.
Do you need to cycle peptides, or can you use them continuously?
Depends on the peptide:
- Ipamorelin, CJC-1295 (no DAC), GHRP-6 — low desensitization risk. Use 3-6 months continuously. Optional 1-2 month break every 6-12 months.
- Hexarelin, IGF-1 LR3, IGF-1 DES — high desensitization risk. Must cycle 4-6 weeks on, 4-6 weeks off.
- CJC-1295 (with DAC) — middle ground. Use 3-6 months, then take 1-2 months off.
Why cycling matters: continuous stimulation causes cells to reduce receptor density (downregulation). The break allows receptors to recover full sensitivity.
Can women use muscle growth peptides?
Yes. Women may see better results in some cases because they naturally produce less GH—more room for improvement—and don't risk testosterone suppression.
No androgenic effects (no hair growth, voice deepening). Better body recomposition response—women respond well to GH's fat-burning + muscle-preserving effects.
Recommended doses for women: Ipamorelin 100-200mcg daily, CJC-1295 no DAC 50-100mcg daily, IGF-1 LR3 20-40mcg daily (half male dose). Expected results: 2-4 pounds lean mass over 3-4 months with GH peptides.
How much do muscle growth peptides cost?
Monthly costs per peptide:
- Ipamorelin: $70-100
- CJC-1295 (no DAC): $80-120
- CJC-1295 (with DAC): $60-80
- IGF-1 LR3: $100-150
- GHRP-6: $60-90
- Hexarelin: $70-100
Popular stacks: beginner (Ipamorelin + CJC-1295) $150-220/month. Bulking (GHRP-6 + CJC-1295) $120-170/month. Add $10-20/month for syringes, alcohol swabs, bacteriostatic water. Blood work every 3-6 months: $100-200.
What's the difference between peptides and HGH?
Peptides signal your body to produce more natural growth hormone. HGH directly introduces synthetic GH.
Peptides: pulsatile release (mimics natural peaks), maintains natural GH production, lower desensitization risk, $70-220/month, minimal side effects.
HGH: sustained elevation (bypasses natural rhythms), can suppress natural production, higher receptor stress, $500-1000+/month, higher side effect risk.
Peptides offer 70-80% of HGH's muscle-building benefits at 15-25% of the cost with lower side effect risk.
Can you stack multiple muscle growth peptides together?
Yes. The most effective stack is Ipamorelin + CJC-1295, which produces 2-3x higher GH release than either alone.
Protocol: Ipamorelin 200mcg + CJC-1295 no DAC 100mcg, mixed in same syringe, once daily before bed. Run 3-6 months. Expected: 4-8 pounds lean mass over 3-4 months. Cost: $150-220/month.
Start with one peptide, assess tolerance for 2-4 weeks, then add the second. Don't stack 3+ peptides as a beginner—too complex, can't isolate issues. Use our peptide stack calculator to plan your stack.
The Bottom Line
Peptides for muscle growth amplify your body's natural anabolic pathways. Growth hormone secretagogues like Ipamorelin and CJC-1295 offer a relatively safe entry point for enhanced recovery and lean muscle building.
Protocol summary: - Peptides work when combined with training and nutrition - Safer profile than steroids (no testosterone suppression) - Results take 6-12 weeks (not overnight) - Long-term human safety data limited - Not FDA-approved for muscle building
Ready to optimize your protocol?
- Take our Peptide Quiz: Personalized recommendations
- Peptide Reconstitution Calculator: Calculate exact doses
- CJC-1295 + Ipamorelin Calculator: Growth stacks
- Peptide Stack Calculator: Plan combinations
Related Articles
Peptides for Bodybuilding (2026)
Best peptides for bodybuilding: BPC-157, TB-500, MK-677, CJC-1295/Ipamorelin, HGH Fragment 176-191. Dosages and stacking protocols.
IGF-1 LR3 Results: What to Expect by Week
IGF-1 LR3 results week by week: pumps, recovery, lean mass, and what before-and-after photos really show. Evidence vs bro-science, safety, and dosing.
CJC-1295 Dosage: Complete Protocol Guide
CJC-1295 dosage guide: DAC and no-DAC protocols. Dosing by goal (anti-aging, fat loss, muscle, sleep), ipamorelin stacking, and injection timing.
Hexarelin Dosage Guide: Protocols
Hexarelin dosage by goal: 100-200 mcg protocols, dose-response data, desensitization timeline, GHRP comparison table, and cycling guide.