Three vials sit on your desk. You know what each one does alone. You have no idea what happens when you combine them. That uncertainty is the difference between a protocol that multiplies results and one that wastes $300 worth of peptides.
Peptide stacking works because individual compounds target different biological pathways. BPC-157 builds blood vessels at an injury site. TB-500 mobilizes repair cells to travel along those vessels. Running both covers two repair mechanisms that a single peptide cannot reach. The key is matching peptides to your specific goal, understanding timing, and knowing which combinations to avoid entirely.
Use the Peptide Stack Calculator to build a protocol tailored to your goal, or the Peptide Interaction Checker to verify safety before combining any compounds. To convert each dose into syringe units, see the peptide dosage calculator.
No peptide stack discussed here is FDA-approved for human use. All dosages reflect research literature and community protocols. Consult a healthcare provider before starting any peptide regimen.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
Best Peptide Stacks by Goal: Quick Reference
This table covers the five most popular stacks, ranked by community adoption and supporting evidence.
| Goal | Stack | Synergy Rating | Protocol Length | Monthly Cost (approx.) |
|---|---|---|---|---|
| Healing & Recovery | BPC-157 + TB-500 ("Wolverine Stack") | 6-8 weeks | $80-150 | |
| Muscle Growth | Ipamorelin + CJC-1295 DAC | 12 weeks | $120-200 | |
| Fat Loss | MOTS-c + Exercise Protocol | 8-12 weeks | $100-180 | |
| Anti-Aging | GHK-Cu + Thymosin Alpha-1 | 8-12 weeks | $90-160 | |
| Recovery + Growth | BPC-157 + TB-500 + Ipamorelin | 8-12 weeks | $150-280 |
The "Wolverine Stack" earns its top rating from decades of published research on both compounds plus the largest body of anecdotal healing reports in the peptide community. Each stack below includes exact dosages, timing protocols, and citations. For beginners, start with the getting started with peptides guide before building a stack.
What Is Peptide Stacking and Why It Works
Stacking peptides is like using both a hammer and a screwdriver on the same project. Each tool does something the other cannot. The hammer drives nails; the screwdriver sets screws. Using both completes the job faster than doubling down on either one alone.
In biological terms, peptide stacking combines compounds that activate different molecular pathways. BPC-157 upregulates vascular endothelial growth factor (VEGF), driving angiogenesis at the injury site (Sikiric et al., Curr Pharm Des, 2018). TB-500 regulates actin polymerization and recruits stem cells to damaged tissue (Goldstein et al., Expert Opin Biol Ther, 2012). One builds the roads; the other sends the repair trucks.
Multi-pathway synergy is the formal term. A single peptide saturates one receptor system. Adding a second peptide that targets a completely different receptor system produces compounding effects rather than diminishing returns. This is why the BPC-157 + TB-500 combination outperforms double-dosing either compound alone.
Three conditions must be met for a stack to work:
- 1.Different mechanisms. Each peptide should activate a distinct pathway. Two GH secretagogues in the same stack compete for the same receptor.
- 2.Compatible pharmacokinetics. Half-lives and dosing frequencies should be manageable together. A twice-daily peptide pairs well with a twice-weekly one.
- 3.No antagonistic interactions. Some peptides blunt each other's effects. The compatibility chart below maps every major combination.
Peptide Compatibility Chart
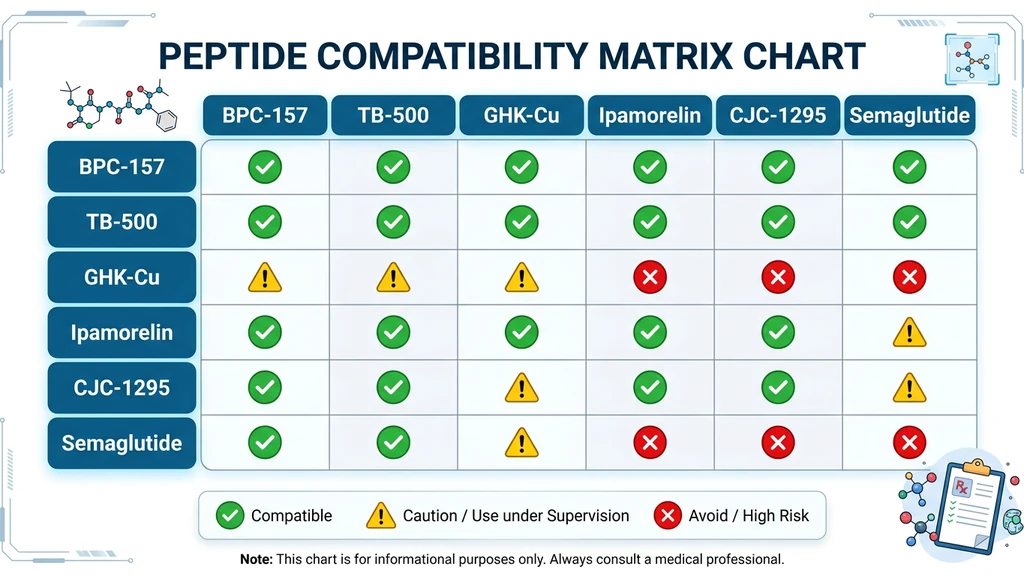
This chart covers the 11 most commonly stacked peptides. Check your planned combination before purchasing.
| BPC-157 | TB-500 | GHK-Cu | Ipamorelin | CJC-1295 | Semaglutide | Tirzepatide | MOTS-c | TA-1 | KPV | MT-2 |
|---|---|---|---|---|---|---|---|---|---|---|
| BPC-157 | ||||||||||
| TB-500 | ||||||||||
| GHK-Cu | ||||||||||
| Ipamorelin | ||||||||||
| CJC-1295 | ||||||||||
| Semaglutide | ||||||||||
| Tirzepatide | ||||||||||
| MOTS-c | ||||||||||
| TA-1 | ||||||||||
| KPV | ||||||||||
| MT-2 |
Key: - Compatible: Safe to run together. Complementary or non-overlapping mechanisms. - Use Caution: Can be combined under medical supervision. May share pathway overlap or increase specific side effects. - Avoid: Redundant mechanisms, antagonistic effects, or compounded cardiovascular/GI risk.
Important notes: - Semaglutide + Tirzepatide: Both are GLP-1 agonists. Combining them doubles GI side effects (nausea, gastroparesis risk) with no additional benefit. - Melanotan-2 + GLP-1 agonists: MT-2 raises blood pressure and heart rate. GLP-1 drugs alter cardiovascular parameters. The combined cardiovascular strain is unnecessary. - Ipamorelin/CJC-1295 + GLP-1 agonists: GH secretagogues can increase insulin resistance. GLP-1 agonists work by enhancing insulin sensitivity. The effects partially oppose each other. - BPC-157 + GLP-1 agonists: BPC-157 may provide GI protection against GLP-1 side effects, but monitor closely as both affect gastric motility.
Run your planned stack through the Peptide Interaction Checker for personalized safety notes.
How to Stack Peptides Safely
Safe stacking requires attention to three variables: timing, injection technique, and site rotation. Ignoring any one of them can reduce efficacy or increase side effects.
Timing: Same Time vs. Staggered Injections
Peptides that target different receptors can be injected at the same time. BPC-157 and TB-500 work through entirely separate mechanisms, so simultaneous injection is standard practice.
GH secretagogues (ipamorelin, CJC-1295) require an empty stomach. Injecting them within 60 minutes of a meal blunts growth hormone release by up to 80% (Nass et al., J Clin Endocrinol Metab, 2008). Schedule these before bed or at least 90 minutes after your last meal.
Sample daily timing for a three-peptide stack (BPC-157 + TB-500 + Ipamorelin):
| Time | Peptide | Dose | Notes |
|---|---|---|---|
| 7:00 AM | BPC-157 | 250 mcg | Morning dose, subcutaneous |
| 7:00 AM | TB-500 | 750 mcg (on injection days) | Same time as BPC-157, different site |
| 10:00 PM | Ipamorelin | 200 mcg | Empty stomach, 90+ min after dinner |
| 10:00 PM | BPC-157 | 250 mcg | Second daily dose (optional) |
Can You Mix Peptides in the Same Syringe?
The short answer: it depends on the peptides. BPC-157 and TB-500 are commonly drawn into the same syringe and injected together. Both are stable in bacteriostatic water and do not interact chemically.
Peptides from different classes should generally be kept in separate syringes. Mixing GH secretagogues with healing peptides in one syringe is not well-studied. The risk is not toxicity; it is degradation. Some peptides alter the pH of the solution, potentially denaturing the other compound before it reaches your tissue.
Safe to combine in one syringe: BPC-157 + TB-500, GHK-Cu + BPC-157 + TB-500 (the GLOW blend).
Use separate syringes: Ipamorelin + BPC-157, CJC-1295 + any healing peptide, semaglutide + anything else.
Injection Site Rotation
Rotate injection sites to prevent lipodystrophy (fat tissue changes at the injection site). Use at least four sites and cycle through them systematically.
Subcutaneous injection sites: left abdomen, right abdomen, left thigh, right thigh. Some users add the upper arm as a fifth site.
For localized healing (knee tendonitis, shoulder injury), inject BPC-157 subcutaneously near the injury site. TB-500 works systemically, so its injection location does not affect which tissue it reaches. For BPC-157 knee injection technique, see where to inject BPC-157 for knee pain.
Use the Peptide Reconstitution Calculator to determine your exact draw volume before injecting.
Best Stack for Healing and Recovery: The Wolverine Stack
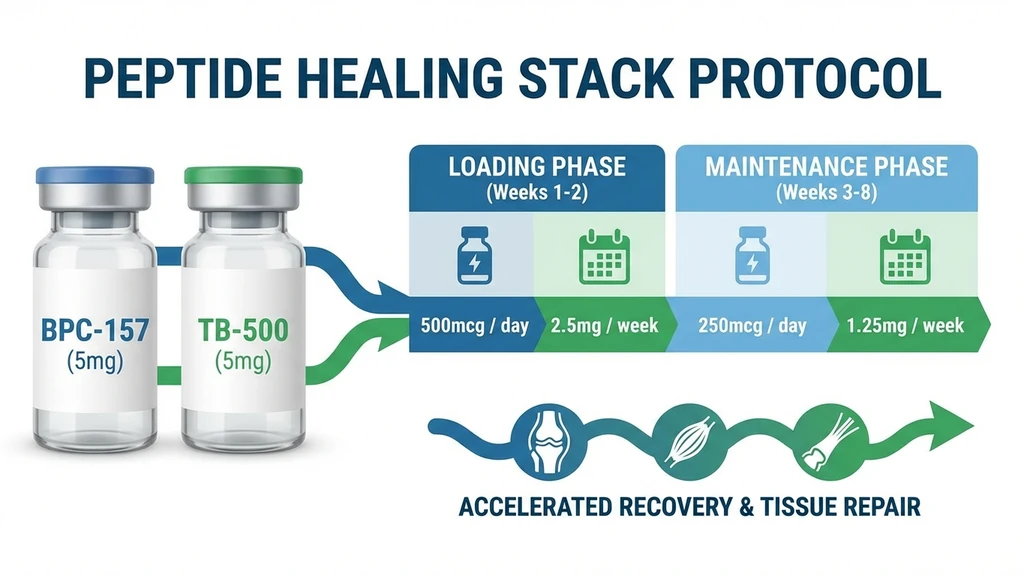
The BPC-157 + TB-500 combination is the most researched and widely used peptide stack. The nickname "Wolverine Stack" comes from the rapid tissue repair users report across tendon, muscle, ligament, and joint injuries.
BPC-157 drives local angiogenesis (new blood vessel formation) through VEGF upregulation (Sikiric et al., Curr Pharm Des, 2018). TB-500 activates global cellular migration through actin polymerization, sending repair cells to every damaged area in the body (Goldstein et al., Expert Opin Biol Ther, 2012). One peptide builds the infrastructure. The other delivers the workforce.
BPC-157 + TB-500 Protocol
Loading Phase (Weeks 1-4):
| Peptide | Dose | Frequency | Route |
|---|---|---|---|
| BPC-157 | 250-500 mcg | 1-2x daily | Subcutaneous (near injury) |
| TB-500 | 750 mcg - 2 mg | 2x per week | Subcutaneous (abdomen) |
Maintenance Phase (Weeks 5-8):
| Peptide | Dose | Frequency | Route |
|---|---|---|---|
| BPC-157 | 250 mcg | 1x daily | Subcutaneous |
| TB-500 | 750 mcg | 1x per week | Subcutaneous |
Protocol notes: - TB-500 requires 4-6 weeks to reach tissue saturation. Do not judge results before week 4. - BPC-157 provides faster initial relief (often within 7-14 days) because it acts locally. - For a 200 lb male, the BPC-157 dosage calculator recommends 500 mcg daily. See the full breakdown at BPC-157 dosage for a 200 lb male. - Total cycle cost: approximately $80-150 depending on source and vial size. Use the Peptide Cost Calculator to estimate your specific protocol. - Store reconstituted vials properly. Potency degrades after 28-30 days in the refrigerator. See how long reconstituted peptides last and how to store peptides.
Adding GHK-Cu: The Triple Healing Stack
GHK-Cu adds a third repair mechanism to the Wolverine Stack. While BPC-157 builds vessels and TB-500 mobilizes cells, GHK-Cu delivers the copper required for lysyl oxidase to cross-link collagen fibers into durable tissue (Pickart et al., BioMed Res Int, 2012). Without this cross-linking step, new collagen is fragile and prone to re-injury.
Triple Healing Stack Protocol:
| Peptide | Dose | Frequency |
|---|---|---|
| BPC-157 | 250-500 mcg | 1-2x daily |
| TB-500 | 750 mcg - 2 mg | 2x per week |
| GHK-Cu | 200 mcg | 1x daily |
GHK-Cu also modulates over 4,000 human genes, suppressing IL-6 and TNF-alpha while activating antioxidant defenses. Users report enhanced skin quality and faster scar resolution as additional benefits.
For the pre-mixed version of this stack, see the GHK-Cu + BPC-157 + TB-500 blend dosage guide. For GHK-Cu's additional benefits, including collagen stimulation and hair follicle support, see GHK-Cu for hair growth.
Best Stack for Muscle Growth
Muscle growth peptide stacks center on growth hormone (GH) optimization. The goal is not to replace GH directly but to amplify your body's natural GH pulses, particularly the large nocturnal pulse that drives recovery and protein synthesis.
Ipamorelin + CJC-1295 DAC Protocol
This is the gold standard GH secretagogue stack. Ipamorelin is a selective GH secretagogue that triggers pituitary GH release without raising cortisol or prolactin (Raun et al., Eur J Endocrinol, 1998). CJC-1295 DAC extends the GH release window from minutes to hours through its Drug Affinity Complex, which binds to albumin and prolongs half-life to 6-8 days (Teichman et al., J Clin Endocrinol Metab, 2006).
Ipamorelin fires the GH pulse. CJC-1295 DAC keeps the pulse elevated. Together, they produce sustained GH elevation that a single compound cannot achieve.
Protocol:
| Peptide | Dose | Frequency | Timing |
|---|---|---|---|
| Ipamorelin | 200-300 mcg | Daily | Before bed, empty stomach |
| CJC-1295 DAC | 2 mg | 1x per week | Any time (long half-life) |
Cycle length: 12 weeks on, 4 weeks off. Extended use beyond 16 weeks may desensitize GH receptors.
Expected outcomes: Improved sleep quality within 1-2 weeks. Visible body composition changes (reduced fat, increased lean mass) by weeks 6-8. Enhanced recovery between training sessions.
Critical rule: Inject ipamorelin on an empty stomach. Food intake, particularly carbohydrates and fats, suppresses ghrelin-mediated GH release by up to 80% (Nass et al., J Clin Endocrinol Metab, 2008). Wait at least 90 minutes after eating. Most users inject 15-30 minutes before sleep.
For complete dosage charts across all peptides, see the peptide dosage chart.
Adding Follistatin-344 for Myostatin Inhibition
Follistatin-344 binds myostatin, the protein that limits muscle growth. Blocking myostatin removes the genetic ceiling on muscle fiber hypertrophy. This is a more advanced addition to the ipamorelin + CJC-1295 stack.
Protocol:
| Peptide | Dose | Frequency |
|---|---|---|
| Follistatin-344 | 100-200 mcg | Daily for 10-30 days |
| Ipamorelin | 200-300 mcg | Daily (before bed) |
| CJC-1295 DAC | 2 mg | 1x per week |
Follistatin-344 cycles are kept short (10-30 days) due to the compound's potent effect on follicle-stimulating hormone (FSH), which can temporarily affect fertility in men. Full protocol details and safety considerations are covered in the follistatin-344 dosage guide.
For BPC-157's indirect role in supporting muscle recovery through tendon and tissue repair, see BPC-157 for muscle growth.
Best Stack for Fat Loss
Fat loss peptide stacks divide into two categories: GLP-1 receptor agonist stacks (semaglutide, tirzepatide) that suppress appetite through incretin signaling, and metabolic peptide stacks (MOTS-c, tesamorelin) that increase energy expenditure or target specific fat deposits.
GLP-1 Based Stacks: Semaglutide or Tirzepatide + Complementary Peptides
Semaglutide and tirzepatide produce dramatic weight loss (15-22% body weight over 72 weeks per the SURMOUNT trials) (Jastreboff et al., NEJM, 2022). The main limitations are GI side effects: nausea, constipation, and slowed gastric emptying.
BPC-157 is commonly added to GLP-1 stacks for gastroprotective effects. BPC-157 accelerates gastric mucosal healing and modulates nitric oxide pathways in the gut. Users report reduced nausea and fewer GI complications when running BPC-157 alongside semaglutide or tirzepatide.
Sample protocol:
| Peptide | Dose | Frequency |
|---|---|---|
| Tirzepatide | 2.5-15 mg (titrated) | 1x per week |
| BPC-157 | 250 mcg | 1-2x daily |
Caution: Do not combine semaglutide with tirzepatide. Both activate GLP-1 receptors. Running them together doubles GI side effects without additional fat loss benefit. Choose one. For a detailed comparison, see retatrutide vs. tirzepatide.
For semaglutide-specific dosing and reconstitution, see the semaglutide dosage chart in mL.
MOTS-c + Exercise Protocol
MOTS-c is a mitochondrial-derived peptide that mimics the metabolic effects of exercise at the cellular level. It activates AMPK, increases glucose uptake into skeletal muscle, and improves insulin sensitivity (Lee et al., Cell Metab, 2015). In mouse studies, MOTS-c prevented diet-induced obesity and reversed age-dependent insulin resistance.
MOTS-c does not replace exercise. It amplifies the metabolic adaptations that exercise produces. Users report enhanced endurance, faster recovery between cardio sessions, and measurable reductions in fasting glucose.
Protocol:
| Peptide | Dose | Frequency | Duration |
|---|---|---|---|
| MOTS-c | 5-10 mg | 3-5x per week | 8-12 weeks |
MOTS-c pairs well with virtually every other peptide on the compatibility chart. It targets mitochondrial metabolism, a pathway that no other peptide in this guide activates. For complete MOTS-c dosing protocols, see the MOTS-c dosage guide.
Tesamorelin for Visceral Fat
Tesamorelin is a growth hormone releasing hormone (GHRH) analog FDA-approved for HIV-associated lipodystrophy. It specifically reduces visceral adipose tissue (the deep abdominal fat surrounding organs) by an average of 15-18% over 26 weeks in clinical trials.
Unlike ipamorelin, tesamorelin directly stimulates the GHRH receptor rather than working through ghrelin pathways. This makes it a complementary addition to an ipamorelin stack for users targeting both subcutaneous and visceral fat.
Protocol:
| Peptide | Dose | Frequency |
|---|---|---|
| Tesamorelin | 1-2 mg | Daily (before bed, empty stomach) |
Tesamorelin can be stacked with MOTS-c for a dual-mechanism fat loss approach: tesamorelin mobilizes visceral fat through GH-mediated lipolysis, while MOTS-c increases mitochondrial fat oxidation. For complete dosing protocols, see tesamorelin dosage for fat loss. An alternative GH-pathway approach is sermorelin for fat loss, which works through a similar GHRH mechanism at lower cost.
Best Stack for Anti-Aging
Anti-aging peptide stacks target the two systems that deteriorate most with age: tissue quality (collagen density, skin elasticity, wound healing) and immune function (thymic involution, declining T-cell diversity).
GHK-Cu + Thymosin Alpha-1 Protocol
GHK-Cu reverses age-related decline in collagen and extracellular matrix integrity. It modulates over 4,000 genes involved in tissue remodeling, suppresses pro-inflammatory cytokines (IL-6, TNF-alpha), and activates proteasome and antioxidant pathways (Pickart et al., BioMed Res Int, 2012). Serum GHK-Cu levels drop from 200 ng/mL at age 20 to 80 ng/mL by age 60. Supplementation restores the signaling environment of younger tissue.
Thymosin Alpha-1 (TA-1) addresses the immune side of aging. The thymus gland shrinks with age, reducing naive T-cell production. TA-1 activates dendritic cells, enhances T-cell maturation, and modulates the Th1/Th2 immune balance. It has been approved in over 35 countries for hepatitis B and as an immune adjuvant. For a complete overview, see thymosin alpha-1 benefits.
Protocol:
| Peptide | Dose | Frequency | Duration |
|---|---|---|---|
| GHK-Cu | 200-400 mcg | Daily (subcutaneous) | 8-12 weeks on, 4 weeks off |
| Thymosin Alpha-1 | 1.6 mg | 2x per week | 8-12 weeks on, 4 weeks off |
This stack produces visible skin quality improvements within 3-4 weeks (fewer fine lines, faster wound healing) and measurable immune marker improvements within 6-8 weeks.
Adding Epitalon: The Pineal Peptide
Epitalon (epithalon) is a synthetic tetrapeptide based on epithalamin, a pineal gland extract. Its primary mechanism is telomerase activation. In cell culture studies, epitalon increased telomerase activity and extended the lifespan of human fetal fibroblasts by 44% compared to controls.
Epitalon also normalizes melatonin secretion patterns that degrade with age, improving sleep architecture. Better sleep drives higher nocturnal GH output, creating a positive feedback loop for tissue repair.
Protocol:
| Peptide | Dose | Frequency | Duration |
|---|---|---|---|
| Epitalon | 5-10 mg | Daily | 10-20 day cycles, 2-3x per year |
| GHK-Cu | 200-400 mcg | Daily | Continuous during cycle |
| Thymosin Alpha-1 | 1.6 mg | 2x per week | Continuous during cycle |
Epitalon cycles are short because telomerase activation does not require chronic stimulation. Two to three cycles per year maintain telomere length without the theoretical risks of sustained telomerase upregulation.
Stacking Peptides with TRT
Testosterone replacement therapy (TRT) pairs well with specific peptides. The synergy runs in both directions: TRT increases protein synthesis and training capacity, while peptides protect the connective tissue that higher training loads stress.
Best peptides to add to TRT:
| Peptide | Purpose | Why It Pairs with TRT |
|---|---|---|
| BPC-157 | Tendon and ligament protection | TRT increases muscle strength faster than tendons adapt. BPC-157 accelerates tendon remodeling to match. |
| Ipamorelin | GH pulse optimization | Testosterone and GH are synergistic for body composition. Ipamorelin fills the GH side of the equation. |
| GHK-Cu | Collagen and skin quality | TRT can accelerate hair thinning and skin changes. GHK-Cu supports collagen density and may slow androgen-related follicle miniaturization. |
Peptides to avoid with TRT:
Melanotan-2 (MT-2) raises blood pressure and heart rate through melanocortin receptor activation. TRT also increases hematocrit and blood viscosity. Combining both compounds creates unnecessary cardiovascular strain. If tanning is the goal, use MT-2 during TRT off-periods or explore lower-risk alternatives.
For women considering peptide stacks, many of these protocols apply at adjusted dosages. See BPC-157 benefits for women for female-specific guidance.
Stacking with GLP-1 Peptides
GLP-1 receptor agonists (semaglutide, tirzepatide, retatrutide) are the fastest-growing category in the peptide space. Stacking them requires specific caution because GLP-1 drugs alter gastric motility, insulin signaling, and appetite regulation.
Safe additions to a GLP-1 protocol:
| Peptide | Benefit | Notes |
|---|---|---|
| BPC-157 | GI protection | Reduces nausea, supports gastric mucosal healing |
| GHK-Cu | Skin elasticity during weight loss | Prevents loose skin by supporting collagen remodeling |
| MOTS-c | Metabolic amplification | Different pathway (AMPK vs. GLP-1), additive fat loss |
Combinations to avoid:
- Two GLP-1 agonists together. Semaglutide + tirzepatide, or semaglutide + retatrutide. Redundant mechanism, doubled GI side effects.
- GH secretagogues + GLP-1 agonists. Ipamorelin and CJC-1295 increase insulin resistance through GH elevation. GLP-1 agonists improve insulin sensitivity. The pharmacological opposition makes the combination less predictable.
BPC-157 paired with tirzepatide or retatrutide is the most popular GLP-1 support stack. BPC-157 addresses the main complaint (GI distress) while the GLP-1 drug handles appetite suppression and metabolic improvement. For a head-to-head comparison of the newest GLP-1 options, see retatrutide vs. tirzepatide.
Common Peptide Stacking Mistakes
Four errors account for the majority of failed peptide stacks. Each one is quantifiable.
Mistake 1: Running too many peptides simultaneously. More compounds does not mean more results. Running four or more peptides increases side effect frequency by 2-4x without proportional benefit. The body has a finite number of receptor sites. Once the key pathways are covered (usually with 2-3 peptides), additional compounds compete for the same receptors or introduce new side effect vectors. Keep stacks to three peptides maximum.
Mistake 2: Wrong timing with GH secretagogues. Injecting ipamorelin or CJC-1295 after a meal suppresses the GH pulse by up to 80%. A 300 mcg dose of ipamorelin taken on a full stomach delivers the equivalent GH output of 60 mcg on an empty stomach. That is $240 wasted per month on a protocol that could have worked by simply shifting injection time to bedtime (Nass et al., J Clin Endocrinol Metab, 2008).
Mistake 3: Ignoring peptide receptor competition. Two GH secretagogues that both work through the ghrelin receptor (GHSR) will compete for binding sites rather than producing additive effects. Ipamorelin + GHRP-6, for example, is less effective per milligram than ipamorelin + CJC-1295, because ipamorelin and CJC-1295 target different receptors (GHSR vs. GHRH-R). Always stack across pathways.
Mistake 4: Skipping the TB-500 loading phase. TB-500 has a 2-day half-life and requires 4-6 weeks of consistent dosing at 2-5 mg per week to reach tissue saturation. Users who start at maintenance dose (750 mcg/week) and quit after 3 weeks report "TB-500 doesn't work." It does. It needs the loading phase. See the full protocol in the peptide dosage chart.
Frequently Asked Questions
Can you mix peptides in the same syringe?
BPC-157 and TB-500 can be combined in one syringe safely. They are chemically stable together in bacteriostatic water. Peptides from different classes (GH secretagogues + healing peptides) should use separate syringes to prevent pH-related degradation. The GHK-Cu + BPC-157 + TB-500 GLOW blend is also designed for single-syringe delivery.
How many peptides can you stack at once?
Two to three peptides is the practical maximum. Running four or more increases side effect frequency by 2-4x without proportional benefit. The body has finite receptor capacity. A well-designed two-peptide stack covering different pathways outperforms a five-peptide stack where compounds compete for the same binding sites.
What is the Wolverine Stack?
The Wolverine Stack is BPC-157 (250-500 mcg daily) combined with TB-500 (750 mcg to 2 mg twice weekly). BPC-157 builds blood vessels at the injury site through VEGF upregulation. TB-500 mobilizes repair cells through actin polymerization. Together they compress 6-12 months of healing into 6-8 weeks for many tendon and muscle injuries.
Can you stack peptides with SARMs?
Technically yes, but the risk profile changes significantly. SARMs suppress natural testosterone production. Adding GH secretagogues (ipamorelin) to a SARMs cycle can amplify results, but you are managing two layers of hormonal manipulation. BPC-157 is the safest peptide to pair with SARMs because it has no hormonal effects and protects tendons from SARM-accelerated strength gains.
Do you need PCT after peptide stacks?
Pure peptide stacks (BPC-157, TB-500, GHK-Cu, ipamorelin) do not suppress natural hormone production and do not require post-cycle therapy. If your stack includes SARMs or prohormones, PCT is necessary for those compounds. GH secretagogues may benefit from a 4-week off period after 12 weeks to prevent receptor desensitization.
How long should you run a peptide stack?
Healing stacks (BPC-157 + TB-500): 6-8 weeks. GH secretagogue stacks (ipamorelin + CJC-1295): 12 weeks on, 4 weeks off. Anti-aging stacks (GHK-Cu + TA-1): 8-12 weeks on, 4 weeks off. GLP-1 protocols run continuously under medical supervision. TB-500 needs minimum 4-6 weeks to reach tissue saturation before results appear.
Can women use the same peptide stacks as men?
Most peptide stacks apply to women at the same or slightly lower dosages. BPC-157 (250 mcg daily) and TB-500 dosing is identical. Ipamorelin dosing is typically 100-200 mcg for women versus 200-300 mcg for men. GHK-Cu, MOTS-c, and TA-1 dosing does not change. Women should avoid melanotan-2 at high doses due to unpredictable melanocyte stimulation.
What is the cheapest effective peptide stack?
BPC-157 + TB-500 costs approximately $80-150 per month and is the highest-value stack available. A 5 mg BPC-157 vial ($30-50) lasts 10-20 days at 250-500 mcg daily. A 5 mg TB-500 vial ($25-40) lasts 2-3 weeks at loading doses. Use the Peptide Cost Calculator to estimate your exact protocol cost.
The Bottom Line
Peptide stacking multiplies results when you combine compounds that target different biological pathways. The core principle is simple: stack across mechanisms, not within them.
Start with one goal and two peptides. For healing, BPC-157 + TB-500 remains the most proven combination in the peptide space. For muscle growth, ipamorelin + CJC-1295 DAC is the standard. For fat loss, pair a GLP-1 agonist with BPC-157 for GI protection. For anti-aging, GHK-Cu + Thymosin Alpha-1 covers both tissue quality and immune function.
Build your protocol with the Peptide Stack Calculator, verify every combination with the Peptide Interaction Checker, and read the peptide safety guide before your first injection.
Related articles: - AOD-9604 Before and After — lipolytic peptide results for fat loss stacks - Tesamorelin Dosage for Fat Loss — GHRH protocol for visceral fat targeting - Sermorelin for Fat Loss — GH-pathway fat loss as a stacking component
Helpful Tools
Related Articles
Thymalin Peptide: Benefits, Research, and Dosage
Thymalin is a thymus-derived immune bioregulator from the Khavinson program. Review the mechanism, human research, dosage context, and an honest look at the limits.
HCG Peptide: What It Is, Uses & Is It a Peptide?
HCG is a glycoprotein hormone, not a true peptide. See its real FDA-approved uses for fertility and male hypogonadism, plus why the HCG diet fails.
HMG Peptide: Human Menopausal Gonadotropin Explained
HMG (menotropins) is an FDA-approved FSH+LH gonadotropin, not a true peptide. Learn its fertility uses in women and men, dosing context, and OHSS risk.
Bioregulator Peptides: The Complete Khavinson Guide
Bioregulator peptides (Khavinson short peptides) are studied for tissue-specific gene regulation. Review the families, honest evidence, and safety gaps.