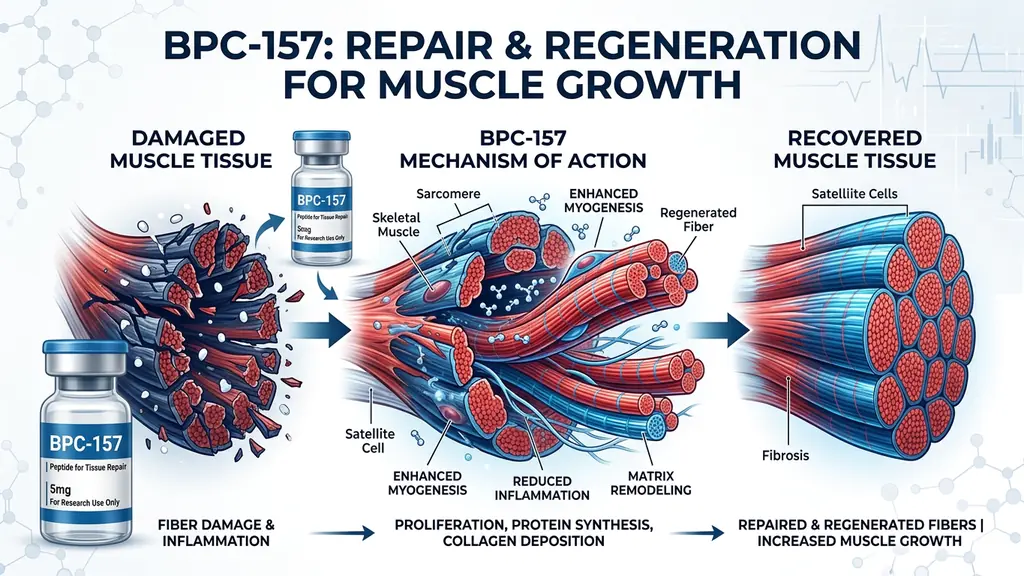
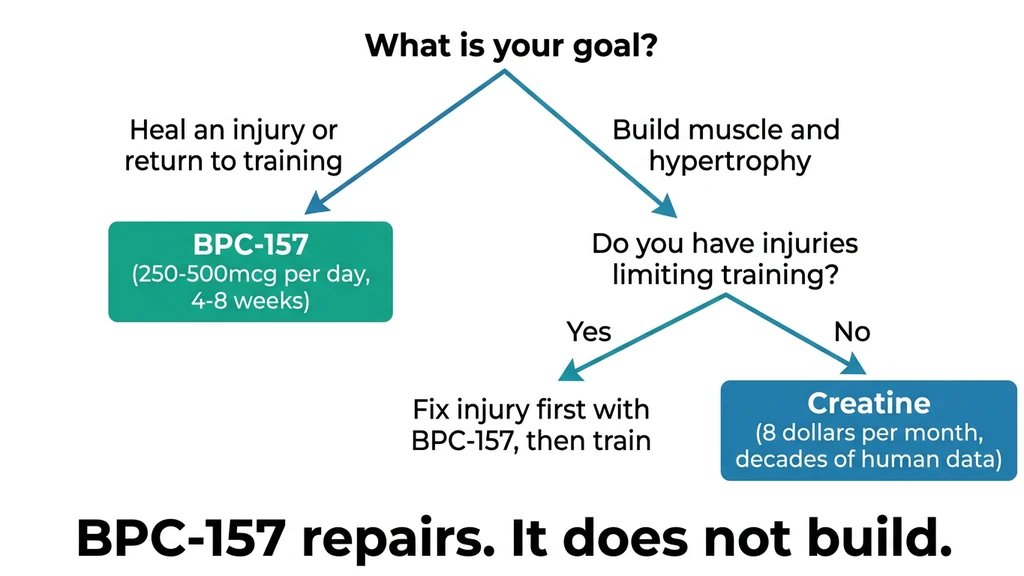
You tore a hamstring six weeks ago. Training is stalled. Someone in the gym mentioned BPC-157 and called it a "muscle growth peptide." Here is the honest answer: BPC-157 does not build muscle. It repairs damaged tissue faster, which lets you get back under the bar sooner.
A 2025 systematic review of 36 studies confirmed that BPC-157 improves structural, biomechanical, and functional outcomes across muscle, tendon, ligament, and bone injury models (Vasireddi et al., 2025). In rat models, it restored crushed muscles (Novinscak et al., 2008), reversed corticosteroid-impaired healing (Pevec et al., 2010), and repaired completely detached muscle-tendon junctions (Staresinic et al., 2021).
None of that equals "building muscle" the way testosterone or growth hormone does. BPC-157 does not increase protein synthesis. It accelerates repair of tissue that is already damaged. That distinction changes how you should use it. Use the BPC-157 Dosage Calculator to plan your protocol.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
Quick Reference: BPC-157 Muscle Claims vs. Evidence
Every claim you have read about BPC-157 and muscle growth falls somewhere on this table.
| Claim | Evidence Level | Reality |
|---|---|---|
| Repairs damaged muscle fibers | Strong (multiple rat models) | Confirmed in crush, transection, and myotendinous junction studies |
| Increases muscle protein synthesis | None | No study shows direct anabolic activity |
| Speeds recovery between workouts | Moderate (extrapolated from healing data) | Plausible based on anti-inflammatory and angiogenic mechanisms |
| Prevents muscle loss during injury | Moderate (rat data) | Counteracted progressive atrophy in myotendinous junction model |
| Replaces steroids for muscle gain | None | Completely different mechanism; no comparison |
If your goal is pure hypertrophy and you have no injuries, BPC-157 is the wrong compound. If chronic pain, tendonitis, or a nagging strain limits your training volume, BPC-157 targets that bottleneck directly.
How BPC-157 Supports Muscle Growth (Indirectly)
Think of BPC-157 like a road crew that fixes potholes on a highway. The crew does not make cars faster. But a smooth highway lets every car reach full speed. BPC-157 repairs the damaged infrastructure (tendons, muscle fibers, blood vessels) so your body's own growth systems operate without obstruction.
In literal terms: muscle growth requires progressive overload. You train, create micro-damage, recover, and return stronger. BPC-157 compresses the recovery window.
The Recovery Math
A muscle that heals in 48 hours instead of 72 gives you roughly 52 additional productive training sessions per year. Tendons that repair faster tolerate higher training volume without forced deloads. Reduced inflammation means fuller range of motion during compound lifts.
BPC-157 earns its gym reputation here. It removes the obstacles to consistent, progressive training. For someone dealing with patellar tendonitis or a recurring hamstring pull, that removal of obstacles often produces more real-world muscle gain than any direct anabolic compound would, because the training itself was the bottleneck.
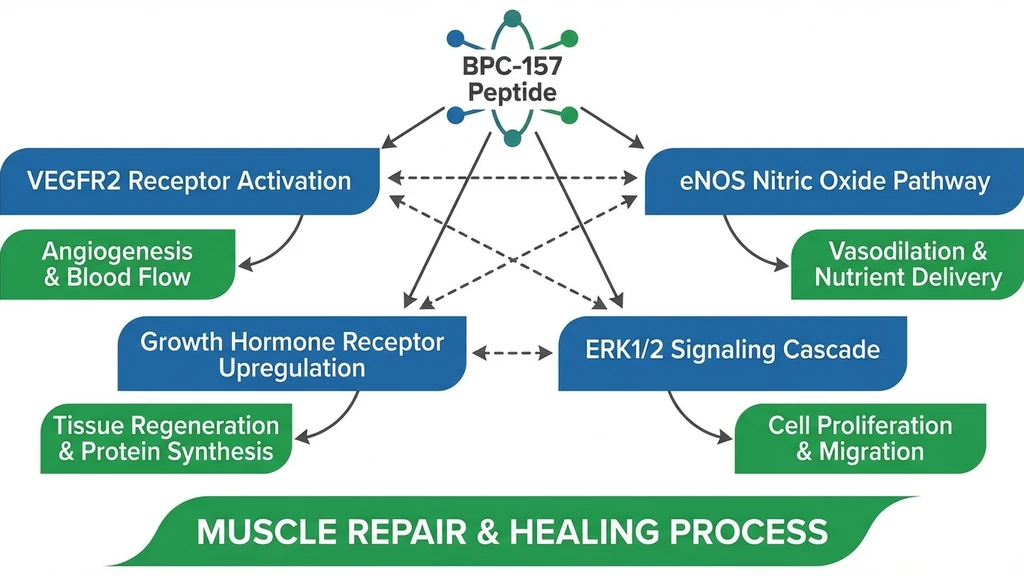
The Science: Four Repair Mechanisms
BPC-157 is a 15-amino-acid fragment derived from human gastric juice (Body Protection Compound). Its healing effects operate through four overlapping molecular pathways. Understanding them clarifies why the peptide works across so many tissue types and why its muscle effects differ from traditional anabolics.
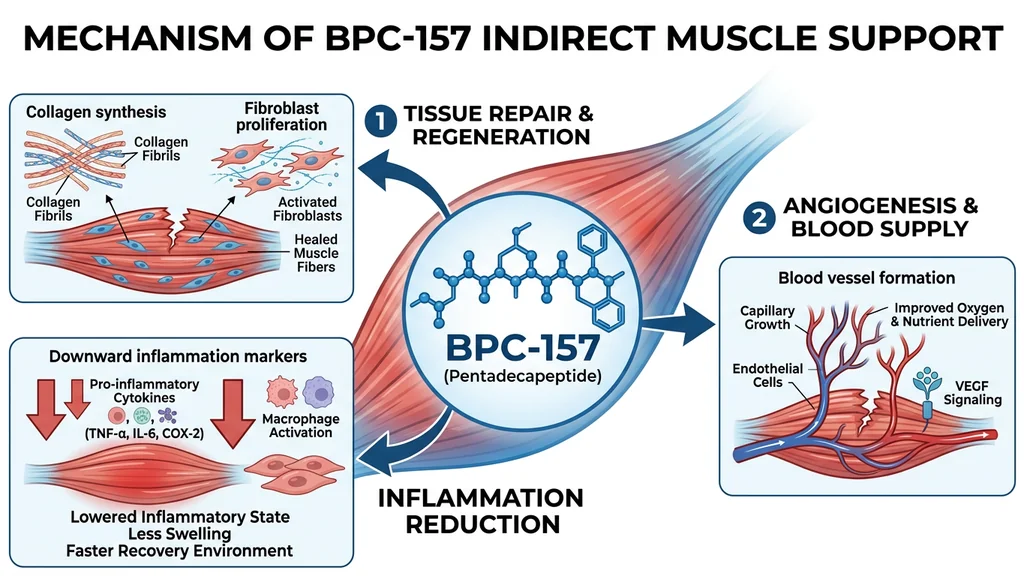
1. Angiogenesis: New Blood Vessels
Damaged muscle needs blood flow. Oxygen, nutrients, immune cells, and growth factors arrive through blood vessels. BPC-157 promotes new vessel formation by activating the VEGFR2-Akt-eNOS signaling pathway.
Hsieh et al. (2017) demonstrated that BPC-157 increases vessel density in vivo and in vitro. The peptide upregulated VEGFR2 mRNA and protein expression in human vascular endothelial cells, promoted VEGFR2 internalization, and activated downstream Akt-eNOS signaling (Hsieh et al., 2017).
In a rat ischemic hind limb model, BPC-157 accelerated blood flow recovery to the affected muscle. More vessels meant faster delivery of everything the muscle needed to rebuild.
2. Nitric Oxide System Modulation
Nitric oxide (NO) regulates blood flow, inflammation, and tissue repair. Trauma disrupts NO signaling. BPC-157 restores it.
The peptide activates both VEGF-dependent (VEGFR2-PI3K-Akt-eNOS) and VEGF-independent (Src-caveolin-1-eNOS) pathways to NO production (Hsieh et al., 2017; Vukojevic et al., 2020). This dual-pathway activation matters: even when one NO pathway is compromised by severe injury, the other remains active.
For muscle repair, NO modulation delivers improved perfusion to the injury site, reduced excessive inflammation, and better neuromuscular signaling during recovery.
3. Growth Hormone Receptor Upregulation
Chang et al. (2014) found that growth hormone receptor was one of the most abundantly upregulated genes in tendon fibroblasts treated with BPC-157. The peptide increased GH receptor expression at both mRNA and protein levels in a dose- and time-dependent manner (Chang et al., 2014).
BPC-157 does not raise GH levels. It amplifies tissue-level response to whatever GH your body already produces. BPC-157-treated fibroblasts showed enhanced JAK2 phosphorylation when exposed to growth hormone, activating the JAK2-STAT5 pathway that drives cell proliferation and tissue repair.
For someone with healthy GH output (or using secretagogues like Ipamorelin or CJC-1295), this creates a synergistic effect: more responsive receptors meeting the same amount of circulating hormone.
4. ERK1/2 Signaling and Cell Migration
BPC-157 activates extracellular signal-regulated kinase 1/2 (ERK1/2) in endothelial cells. This pathway governs cell proliferation, migration, and differentiation.
In a tendon explant model, BPC-157 accelerated outgrowth, increased cell survival under oxidative stress (H2O2), and enhanced fibroblast migration in a dose-dependent manner (Chang et al., 2011). These cellular processes also govern muscle connective tissue repair following strain or tear.
BPC-157 also reduces pro-inflammatory cytokines (TNF-alpha, IL-6) while preserving the constructive inflammatory signals needed for early-phase healing. This balanced approach avoids the problem with NSAIDs, which suppress inflammation broadly and can impair tissue remodeling (Sikiric et al., 2018).
Animal Study Evidence: What BPC-157 Does to Injured Muscle
All evidence for BPC-157 and muscle repair comes from preclinical animal studies. No human clinical trials on muscle healing exist. That limitation is real. The breadth and consistency of the animal data, however, is unusually strong for a peptide compound.
A 2025 systematic review analyzed 36 studies (35 preclinical, 1 clinical retrospective) and concluded that BPC-157 improves functional, structural, and biomechanical outcomes across multiple injury types (Vasireddi et al., 2025).
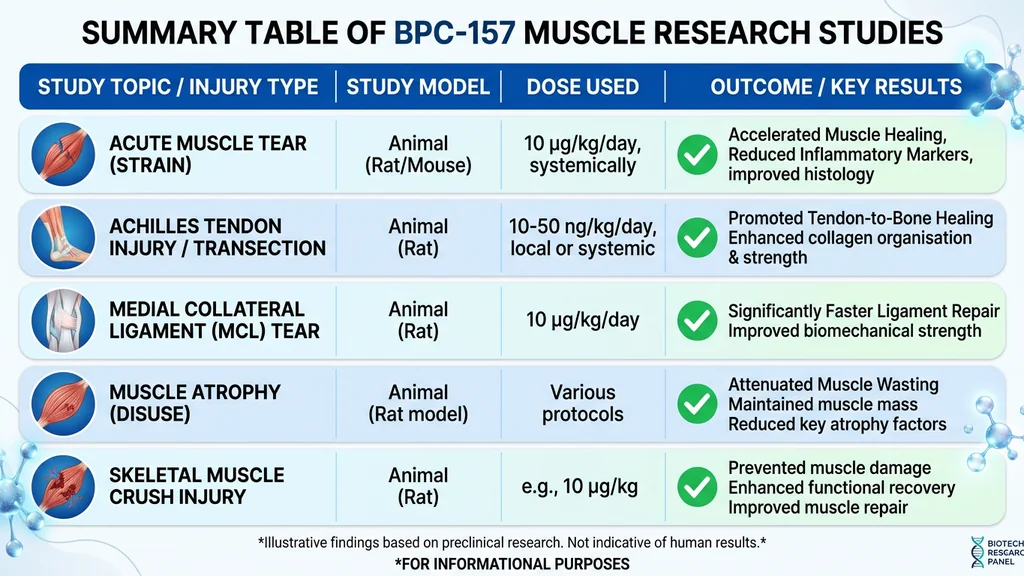
| Study | Injury Model | Key Outcome |
|---|---|---|
| Novinscak et al., 2008 | Gastrocnemius crush | Less hematoma, faster functional recovery, normalized enzyme markers |
| Staresinic et al., 2006 | Quadriceps transection | Improved load-to-failure, reduced atrophy, increased myofibril diameter |
| Pevec et al., 2010 | Corticosteroid-impaired healing | Complete reversal of steroid-induced healing impairment |
| Staresinic et al., 2021 | Myotendinous junction defect | Full function restored by day 28-42, defects disappeared |
Muscle Crush Injury
Novinscak et al. (2008) applied a standardized crush force (0.727 Ns/cm2) to rat gastrocnemius muscles, then administered BPC-157 either intraperitoneally or locally as a cream once daily for 14 days.
BPC-157-treated rats showed less hematoma and edema, no post-injury leg contracture, improved muscle fiber organization under microscopy, faster functional recovery, and normalized creatine kinase, lactate dehydrogenase, AST, and ALT levels (Novinscak et al., 2008).
Muscle crush injuries mimic the damage from heavy eccentric training, contact sports, and blunt trauma. This model is the closest analog to gym-relevant muscle damage in the BPC-157 literature.
Complete Muscle Transection
Staresinic et al. (2006) surgically cut the quadriceps muscle completely in rats, then treated them with BPC-157. Treated animals showed improved load-to-failure measurements, better motor function, larger myofibril diameter, and reduced subcutaneous gapping at the injury site (Staresinic et al., 2006).
Complete transection is comparable to a full-thickness muscle tear in humans. BPC-157 improved both structural integrity and functional output in this severe model.
Corticosteroid-Impaired Healing
Corticosteroids suppress inflammation and collagen synthesis, slowing muscle healing. Pevec et al. (2010) gave rats 6-alpha-methylprednisolone alongside muscle injury. As expected, healing worsened significantly.
BPC-157 completely reversed corticosteroid-impaired muscle healing, whether given intraperitoneally or applied locally as a cream. Functional, macroscopic, and histological assessments all confirmed the reversal (Pevec et al., 2010).
This finding matters for anyone on prescription corticosteroids (prednisone, dexamethasone) or recovering from cortisone injections while trying to maintain muscle function.
Myotendinous Junction Repair
The myotendinous junction (where muscle meets tendon) is one of the most injury-prone regions during explosive movements. Staresinic et al. (2021) created a defect in this junction that could not heal on its own.
BPC-157, given intraperitoneally (10 mcg/kg or 10 ng/kg) or orally in drinking water (0.16 mcg/mL or 0.16 ng/mL), counteracted progressive atrophy and restored full function. By days 28 and 42, defects had completely disappeared. Microscopic examination showed no remaining inflammatory infiltrate and well-oriented recovered tissue (Staresinic et al., 2021).
Two findings stand out. Oral BPC-157 was effective, suggesting systemic distribution reaches the injury site from the gut. And the peptide worked across three orders of magnitude in dosing (mcg to ng), consistent with BPC-157's broad dose-response pattern across studies.
What Happens When You Expect Anabolic Results
Two concrete scenarios show why misunderstanding BPC-157 leads to wasted money and stalled progress.
Scenario 1: The healthy lifter who buys BPC-157 for gains. You have no injuries. You spend $60-80/month on BPC-157 for 8 weeks, expecting visible muscle growth. After 8 weeks, your body composition is identical. You gained nothing because there was nothing to repair. That $480-640 would have bought 8 months of creatine monohydrate, which actually increases muscle protein synthesis by 5-10% and has decades of human trial data.
Scenario 2: The injured lifter who stacks BPC-157 with anabolics instead of using it for recovery. You have chronic patellar tendonitis that forces you to skip squats and leg press. Instead of addressing the tendon, you add a GH secretagogue for "more growth." Training volume stays limited by knee pain. After 12 weeks, your upper body grew but your legs did not. BPC-157 at 250-500 mcg/day targeting the tendon would have resolved the bottleneck within 4-6 weeks, letting you train legs again at full capacity.
The fix in both cases: match the compound to the problem. BPC-157 for tissue damage. Anabolics or secretagogues for growth stimulus. Using one where you need the other wastes time and money.
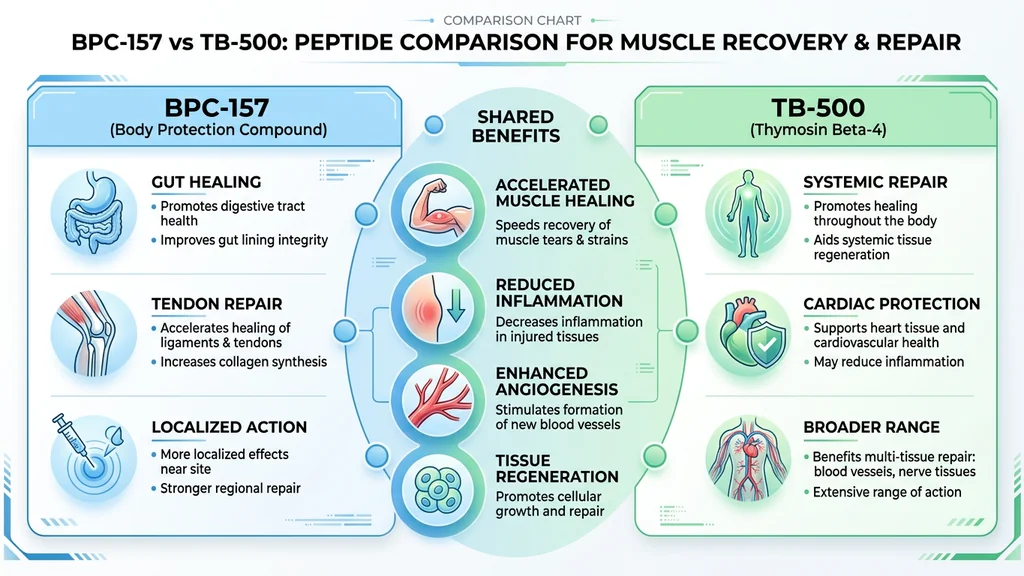
BPC-157 vs. TB-500 for Muscle Recovery
BPC-157 and TB-500 are the two most commonly used peptides for musculoskeletal healing. They work through different pathways and have different strengths.
| Feature | BPC-157 | TB-500 |
|---|---|---|
| Origin | Fragment of human gastric juice | Fragment of thymosin beta-4 |
| Primary mechanism | VEGFR2/eNOS angiogenesis, GH receptor upregulation | Actin regulation, cell migration |
| Best for | Tendon, ligament, GI, localized injuries | Muscle fiber repair, systemic inflammation, flexibility |
| Half-life | Short (estimated 1-2 hours) | Long (estimated 4-6 hours) |
| Dosing frequency | 1-2x daily | 2-3x per week |
| Typical dose | 250-500 mcg/day | 2.5-5 mg per dose (loading) |
| Route | Subcutaneous (near injury) or oral | Subcutaneous (anywhere) |
| Connective tissue evidence | Strong | Moderate |
| Muscle fiber repair evidence | Moderate | Strong |
| Anti-inflammatory | Moderate | Strong (systemic) |
| Monthly cost | $40-80 | $80-150 |
For a complete TB-500 dosing breakdown, see the TB-500 dosage chart.
When to Choose BPC-157
BPC-157 is the better choice for localized connective tissue injuries. Tendonitis (Achilles, patellar, rotator cuff), ligament strains, and injuries at the muscle-tendon junction respond well to BPC-157 injected near the affected area.
The peptide also excels when gut health is a factor. Because BPC-157 derives from gastric juice, it has protective effects on the GI tract. Athletes using NSAIDs for pain management benefit from BPC-157's gastroprotective properties (Sikiric et al., 2018).
BPC-157 is the more affordable option. Lower doses (250-500 mcg vs. 2.5-10 mg) and smaller vials keep monthly costs between $40 and $80.
When to Choose TB-500
TB-500 works best for broad muscle damage, systemic inflammation, and flexibility issues. Its primary mechanism involves regulating actin, a protein central to muscle contraction and cell movement.
TB-500's longer half-life means less frequent injections: 2-3 times per week vs. daily. Its systemic distribution reaches injury sites without requiring injection near the affected area. For someone with multiple injury sites or general recovery needs, TB-500 offers more convenience at higher cost.
Stacking BPC-157 + TB-500
Many practitioners combine both peptides. BPC-157 handles the connective tissue component. TB-500 targets muscle fiber repair. Different pathways, complementary coverage.
Common stack protocol:
- BPC-157: 250-500 mcg subcutaneous daily (near injury site)
- TB-500: 2.5-5 mg subcutaneous 2x per week (loading), then 2.5 mg 1x per week (maintenance)
- Duration: 4-8 weeks
- Estimated monthly cost: $120-230
No controlled studies have tested the combination. The stacking approach is based on complementary mechanisms and practitioner reports. Use the Peptide Stack Calculator to build your protocol.
For a full safety profile, see our guide on BPC-157 side effects.
BPC-157 Dosage Protocol for Muscle Recovery
Dosage recommendations are extrapolated from animal studies using allometric scaling from the standard rat dose of 10 mcg/kg. No human clinical trials have established optimal muscle-specific dosing. The protocols below reflect the most commonly used approaches from preclinical data and clinical practitioner experience.
Use the BPC-157 Dosage Calculator to calculate your exact dose based on vial concentration and body weight.
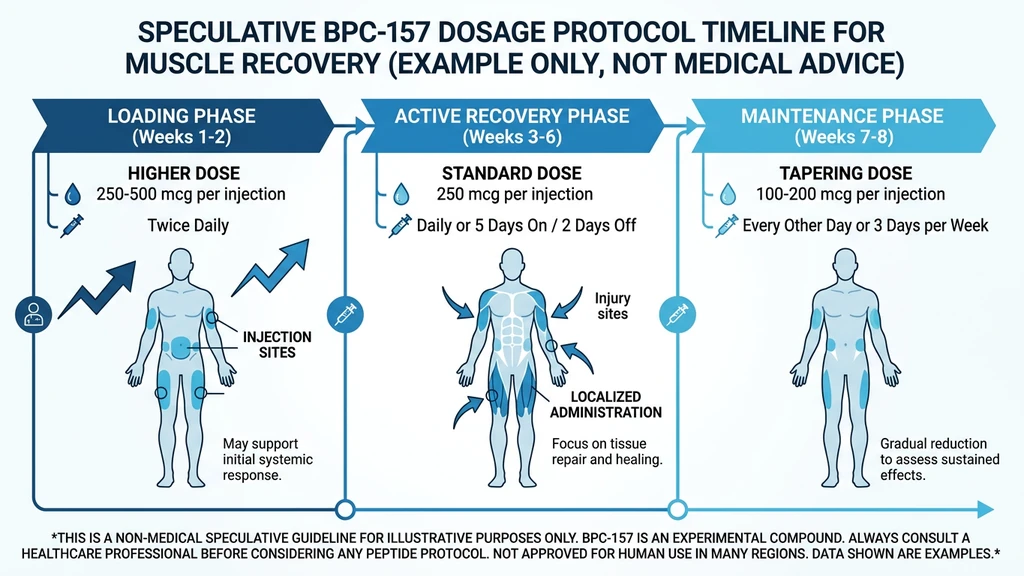
Standard Protocol
Dose: 250-500 mcg per day Frequency: Once or twice daily (split dosing: morning and evening) Route: Subcutaneous injection, ideally near the injury site Cycle length: 4-6 weeks for acute injuries, 6-8 weeks for chronic conditions Time off: 2-4 weeks between cycles
| Body Weight | Conservative Dose | Standard Dose | Upper Range |
|---|---|---|---|
| 60 kg / 132 lbs | 200 mcg/day | 300 mcg/day | 500 mcg/day |
| 80 kg / 176 lbs | 250 mcg/day | 400 mcg/day | 600 mcg/day |
| 100 kg / 220 lbs | 300 mcg/day | 500 mcg/day | 750 mcg/day |
Start at the conservative dose for the first week to assess tolerance, then move to the standard dose. The upper range is reserved for severe injuries under clinical supervision.
For injection preparation, see the injection guide and use the Peptide Reconstitution Calculator to determine your bacteriostatic water volume.
Injection Site Strategy
BPC-157 distributes systemically after subcutaneous injection. Many practitioners still recommend injecting near the injury site for concentrated local effects.
1. Quadriceps or hamstring strain. Subcutaneous injection in the thigh, near the affected area. Pinch the skin and inject into the fat layer.
2. Shoulder or rotator cuff. Subcutaneous injection in the deltoid region or upper arm on the affected side.
3. Lower back muscle strain. Subcutaneous injection in the abdominal area (lower quadrant on the affected side). The abdomen is the most comfortable injection site overall.
4. General recovery (no specific injury). Abdomen, rotating between left and right sides.
Inject subcutaneously into the fat layer. Do not inject intramuscularly.
Timing Around Training
Pre-workout (morning dose). 30-60 minutes before training. BPC-157's anti-inflammatory and vasodilatory effects may improve blood flow during the session.
Post-workout (evening dose). 1-2 hours after training or before bed. Recovery processes peak during sleep, and BPC-157's growth hormone receptor upregulation aligns with the natural nighttime GH surge (Chang et al., 2014).
Split dosing (recommended for active injuries). 250 mcg morning, 250 mcg evening. Maintains more consistent peptide exposure throughout the day.
Single daily dose (maintenance). 250-500 mcg once daily. Simpler protocol for people without active injuries who want recovery support.
Common Mistakes with BPC-157 for Muscle Recovery
Mistake #1: Using BPC-157 as a muscle builder when you have no injuries.
You spend $60-80/month for 8 weeks and see zero change in body composition. BPC-157 repairs damaged tissue. If no tissue is damaged, the peptide has nothing to act on. That $480-640 buys 16 months of creatine, which actually drives protein synthesis in healthy muscle.
Mistake #2: Injecting intramuscularly instead of subcutaneously.
Intramuscular injection causes unnecessary pain and provides no absorption advantage over subcutaneous delivery. Pinch the skin, inject into the fat layer. Every animal study demonstrating efficacy used intraperitoneal or subcutaneous routes, not intramuscular.
Mistake #3: Running a 2-week cycle and expecting full tendon repair.
Tendon and ligament tissue heals slower than muscle. In the myotendinous junction study, full repair required 28-42 days (Staresinic et al., 2021). Stopping at 2 weeks catches only the early inflammatory reduction. You miss the structural remodeling phase entirely. Commit to 4-6 weeks minimum for connective tissue injuries.
Mistake #4: Skipping the injury assessment and blaming BPC-157 when it "doesn't work."
If you have a labral tear, a herniated disc, or a complete ligament rupture, BPC-157 cannot fix structural damage that requires surgical intervention. Get imaging first. BPC-157 works on partial tears, strains, tendonitis, and inflammatory conditions. It is not a substitute for an orthopedic evaluation.
Realistic Timeline and Expectations
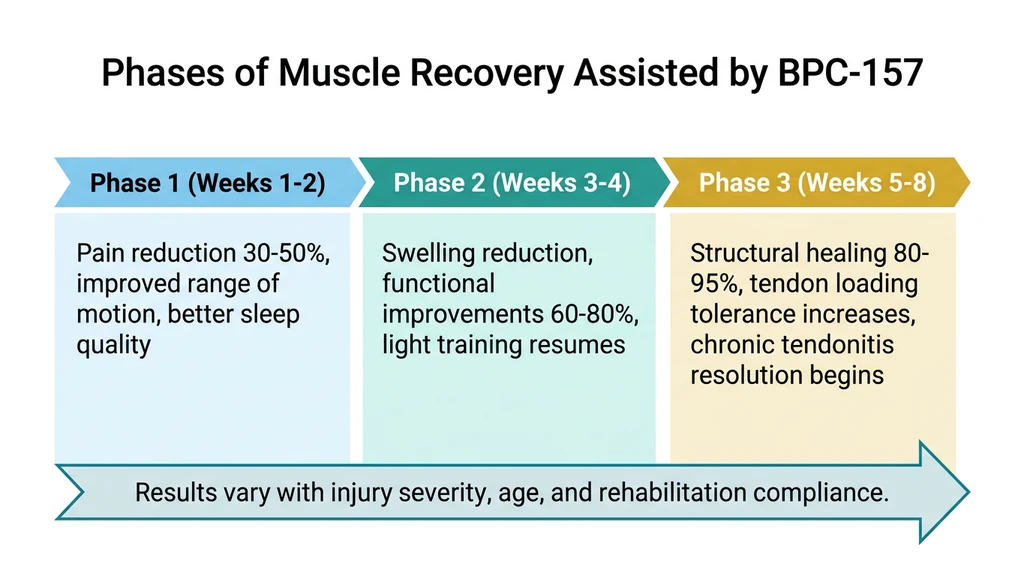
Weeks 1-2. Reduced pain and inflammation at injury sites. Some users report improved range of motion within the first week. Sleep quality may improve slightly due to reduced pain and GH receptor sensitization.
Weeks 3-4. Visible reduction in swelling. Functional improvements in the injured area. Ability to resume light training on previously injured muscles. Faster recovery between sessions becomes noticeable.
Weeks 5-8. Structural healing progresses. Tendons and ligaments that were painful during loading may tolerate normal training volume. Chronic tendonitis that persisted for months may resolve or substantially improve.
These timelines come from animal study endpoints and user reports. Individual results vary with injury severity, age, health status, and training practices.
Safety and Regulatory Status
BPC-157 is not FDA-approved for any indication. It is classified as a research peptide. No lethal or toxic dose has been reported in animal studies across doses from 6 mcg/kg to 20 mg/kg, multiple routes (intraperitoneal, intramuscular, intravenous, oral), and various frequencies (Vasireddi et al., 2025).
A single retrospective clinical study examined intraarticular BPC-157 injection for chronic knee pain. Of 12 patients, 7 reported relief lasting over 6 months. No adverse events were documented.
Known limitations of the evidence:
- 35 of 36 studies in the 2025 systematic review were preclinical (animal models)
- Long-term human safety data does not exist
- Allometric dose scaling from rats to humans is an approximation
- Most studies originate from a single research group (University of Zagreb)
- BPC-157 is banned by WADA and USADA for competitive athletes
For the complete safety profile, see BPC-157 side effects.
*This article is for educational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before using any peptides.*
Frequently Asked Questions
Does BPC-157 directly build muscle like steroids or SARMs?
No. BPC-157 does not increase protein synthesis, nitrogen retention, or mTOR activation. It repairs damaged muscle tissue, reduces inflammation, and promotes blood vessel formation through the VEGFR2-Akt-eNOS pathway (Hsieh et al., 2017). These effects support muscle growth indirectly by accelerating recovery. For direct muscle-building peptides, see peptides for muscle growth.
How long does BPC-157 take to heal a muscle injury?
Most users report pain reduction and improved range of motion within 1-2 weeks. Functional improvements appear by weeks 3-4. Full structural healing of tendons and muscle tears typically requires 4-8 weeks. The myotendinous junction study showed complete repair by days 28-42 (Staresinic et al., 2021). Use the BPC-157 Dosage Calculator to plan your cycle length.
Can I stack BPC-157 with TB-500 for faster muscle recovery?
Yes. BPC-157 and TB-500 work through different pathways: BPC-157 targets connective tissue via VEGFR2 signaling, TB-500 targets muscle fibers via actin regulation. A common protocol is BPC-157 at 250-500 mcg daily plus TB-500 at 2.5-5 mg twice weekly during loading. No controlled studies have tested the combination. See the TB-500 dosage chart for detailed protocols.
Should I inject BPC-157 near the injured muscle or in my abdomen?
BPC-157 distributes systemically regardless of injection site. Injecting near the injury may provide higher local concentration. Practitioners recommend near-site injection for localized injuries (tendonitis, specific muscle strains) and abdominal injection for general recovery. Always inject subcutaneously into the fat layer, never intramuscularly. See the injection guide for technique.
Is BPC-157 safe for long-term use?
No long-term human safety data exists. In animal studies, no toxic or lethal dose was identified across doses from 6 mcg/kg to 20 mg/kg and multiple administration routes (Vasireddi et al., 2025). Most protocols run 4-8 weeks with 2-4 weeks off between cycles. BPC-157 is not FDA-approved and is banned by WADA/USADA. Review BPC-157 side effects for the full safety profile.
What dose of BPC-157 should I use for muscle recovery?
The standard dose is 250-500 mcg per day, split into morning and evening injections. Start at the conservative end (200-250 mcg/day) for the first week. An 80 kg person typically uses 400 mcg/day. These numbers are allometrically scaled from the rat dose of 10 mcg/kg. No human trial has confirmed optimal dosing. Use the BPC-157 Dosage Calculator for a weight-based recommendation.
Does oral BPC-157 work for muscle injuries?
In the myotendinous junction study, oral BPC-157 in drinking water (0.16 mcg/mL) fully restored muscle function and eliminated the defect by day 42 (Staresinic et al., 2021). This suggests oral delivery reaches injury sites systemically. Most users still prefer subcutaneous injection for potentially higher bioavailability, but oral protocols exist for those who want to avoid needles.
Will BPC-157 help if I have no injuries and just want faster recovery between workouts?
Possibly, but the evidence is thin. BPC-157's confirmed effects center on repairing actual tissue damage, not accelerating normal post-exercise recovery in healthy muscle. If you recover normally and have no pain or injury, creatine monohydrate (3-5 g/day) has far stronger human evidence for recovery and performance. Reserve BPC-157 for situations where injury or chronic pain limits your training.
The Bottom Line
BPC-157 repairs damaged tissue. It does not build muscle directly. The preclinical evidence for accelerating healing of muscle tears, tendon damage, and connective tissue injuries is strong and consistent across 36 studies (Vasireddi et al., 2025).
If injuries limit your training, BPC-157 at 250-500 mcg/day for 4-8 weeks targets the repair bottleneck. Faster healing means more consistent training. More consistent training means more muscle over time. If you have no injuries and want hypertrophy, growth hormone secretagogues like Ipamorelin and CJC-1295 are the better peptide category.
Calculate your exact dose with the BPC-157 Dosage Calculator, prepare your vial with the Peptide Reconstitution Calculator, or build a recovery stack with the Peptide Stack Calculator. For a complete comparison of anabolic peptide options, see peptides for muscle growth.
References
- 1.Vasireddi N et al. (2025). Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review. *Am J Sports Med.* PubMed
- 2.Hsieh MJ et al. (2017). Therapeutic potential of pro-angiogenic BPC157 is associated with VEGFR2 activation and up-regulation. *J Mol Med.* 95:323-333. PubMed
- 3.Chang CH et al. (2014). Pentadecapeptide BPC 157 enhances the growth hormone receptor expression in tendon fibroblasts. *Molecules.* 19(11):19066-19077. PubMed
- 4.Chang CH et al. (2011). The promoting effect of pentadecapeptide BPC 157 on tendon healing involves tendon outgrowth, cell survival, and cell migration. *J Appl Physiol.* 110(3):774-780. Source
- 5.Novinscak T et al. (2008). Gastric pentadecapeptide BPC 157 as an effective therapy for muscle crush injury in the rat. *Surg Today.* 38(8):716-725. PubMed
- 6.Staresinic M et al. (2006). Effective therapy of transected quadriceps muscle in rat: Gastric pentadecapeptide BPC 157. *J Orthop Res.* 24(5):1109-1117. PubMed
- 7.Pevec D et al. (2010). Impact of pentadecapeptide BPC 157 on muscle healing impaired by systemic corticosteroid application. *Med Sci Monit.* 16(3):BR81-88. PubMed
- 8.Staresinic M et al. (2021). Stable Gastric Pentadecapeptide BPC 157 as a Therapy for the Disable Myotendinous Junctions in Rats. *Biomedicines.* 9(11):1547. PubMed
- 9.Vukojevic J et al. (2020). Modulatory effects of BPC 157 on vasomotor tone and the activation of Src-Caveolin-1-eNOS pathway. *Sci Rep.* 10:17444. PubMed
- 10.Sikiric P et al. (2018). BPC 157 and Standard Angiogenic Growth Factors: Gastrointestinal Tract Healing, Lessons from Tendon, Ligament, Muscle and Bone Healing. *Curr Pharm Des.* 24(18):1972-1989. PubMed
Related Articles
Peptides for Bodybuilding (2026)
Best peptides for bodybuilding: BPC-157, TB-500, MK-677, CJC-1295/Ipamorelin, HGH Fragment 176-191. Dosages and stacking protocols.
How to Take BPC-157: Dosage and Timing
How to take BPC-157: inject 250-500 mcg subcutaneously near the injury once daily for 4-8 weeks. Reconstitution, dosing, and cycle length.
How to Inject Peptides: SubQ & IM
Step-by-step peptide injection guide: SubQ vs IM technique, needle sizes, injection sites, dosing, and 5 common mistakes. BPC-157 and TB-500 examples included.
Peptides for Healing: What the Evidence Shows
Peptides for healing by tissue: tendon, bone, wound, gut, post-surgery. Which claims rest on human trials, which rest on rat studies, and what is unsafe.