You have a vial of BPC-157, a bag of insulin syringes, and a nagging injury that has not responded to rest. Here is the direct answer: inject 250 to 500mcg subcutaneously near the injury site once or twice daily, for 4 to 8 weeks. That protocol covers the vast majority of musculoskeletal uses. For gut healing, swallow 500 to 1000mcg orally on an empty stomach instead.
| Quick Reference | Details |
|---|---|
| Standard dose | 250 to 500mcg per day |
| Route (most common) | Subcutaneous injection |
| Frequency | Once or twice daily |
| Cycle length | 4 to 8 weeks |
| Injection site | Near injury or lower abdomen |
| Needle gauge | 29 to 31 gauge insulin syringe |
| Reconstitution | 2mL bacteriostatic water per 5mg vial |
| Storage | Refrigerate at 2 to 8 degrees Celsius |
| How to get it | Compounding pharmacy (prescription) or research vendor |
This guide covers every step from obtaining the peptide to your final injection: all three administration routes, dosing by condition, reconstitution math, timing, stacking, the 2026 legal landscape, and the mistakes that send beginners back to square one. For personalized syringe volumes, use the BPC-157 dosage calculator.
Medical disclaimer: BPC-157 lacks FDA approval for any medical use. All dosing reflects preclinical animal research and clinical practice observations. Consult a licensed healthcare provider before starting any peptide protocol.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
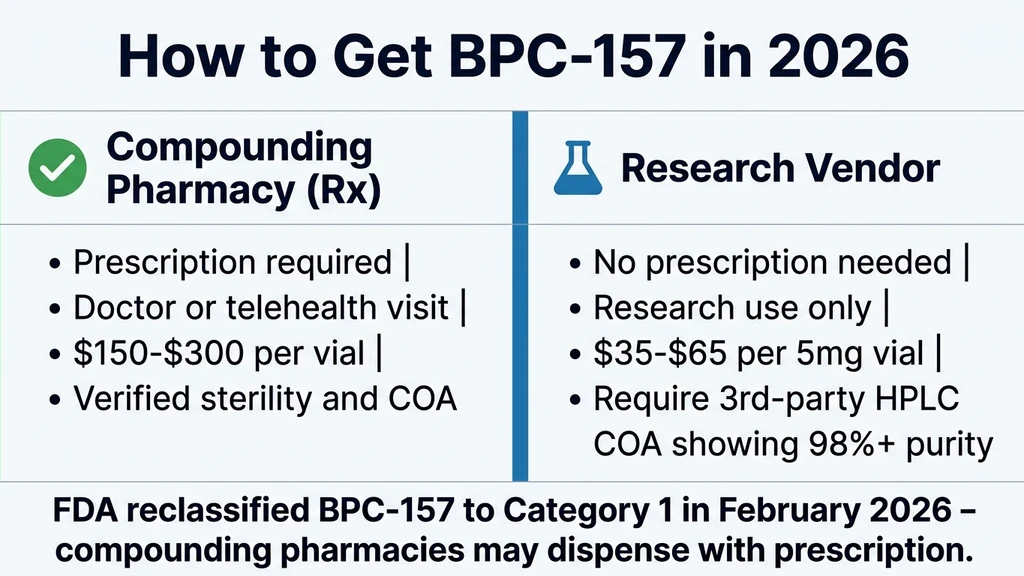
How to Get BPC-157 in 2026
In February 2026, the FDA moved BPC-157 from a restricted Category 2 substance back to Category 1, meaning it can again be dispensed through licensed compounding pharmacies with a valid prescription. This is a significant change from 2024 to 2025, when compounded BPC-157 was effectively blocked.
Compounding Pharmacy Route (Prescription)
A doctor writes a prescription, a licensed compounding pharmacy compounds the peptide, and you receive a product with verified potency, sterility, and accurate concentration. Functional medicine doctors, anti-aging specialists, and integrative health providers are the most likely to be familiar with peptide therapy. Telehealth platforms have expanded substantially and many now offer peptide consultations remotely without an in-person visit.
Compounded BPC-157 typically costs $150 to $300 per vial depending on concentration and pharmacy. The higher cost buys pharmaceutical-grade sterility testing, accurate labeling, and a legitimate medical record. For patients with documented injuries or gut conditions, this is the lowest-risk route in 2026.
Research Vendor Route
BPC-157 sold as a research chemical does not require a prescription in the United States. Reputable vendors charge approximately $35 to $65 for a 5mg vial. Quality varies dramatically. The only reliable quality signal is a third-party certificate of analysis (COA) showing HPLC purity at 98% or higher and mass spectrometry confirmation of peptide identity. No COA means walk away.
Confirm the lot number on the COA matches the lot number on your vial. Counterfeit and underdosed vials circulate widely in the research chemical market. For complete guidance on verifying vendor quality, see the peptide safety guide.
What Is BPC-157 and How Does It Work?
BPC-157 is a synthetic 15-amino-acid peptide derived from a protective protein found in human gastric juice. The name stands for Body Protection Compound. Researchers first isolated it in the early 1990s and have since published over 100 animal studies examining its effects on tissue repair, inflammation, and organ protection.
The peptide triggers healing through several overlapping mechanisms. It upregulates vascular endothelial growth factor (VEGF) to promote new blood vessel formation at injury sites. It activates the FAK-paxillin pathway, which drives tendon and ligament fibroblast migration toward damaged tissue (Chang et al., Life Sci, 2011). It modulates the nitric oxide system, which controls blood flow and inflammation (Sikiric et al., J Pharmacol Sci, 2014). And it interacts with the dopaminergic and serotonergic systems, which explains some of its reported effects on mood and gut function (Sikiric et al., Curr Pharm Des, 2018).
BPC-157 amplifies repair processes your body already runs rather than forcing biological changes the way pharmaceutical drugs do. The peptide tells your cells to heal faster and more completely. A 2025 systematic review of 36 animal studies found no lethal dose across any tested species or route of administration (Kang et al., Orthop J Sports Med, 2025). For a broader introduction to peptide therapy, see the getting started guide.
Three Ways to Take BPC-157
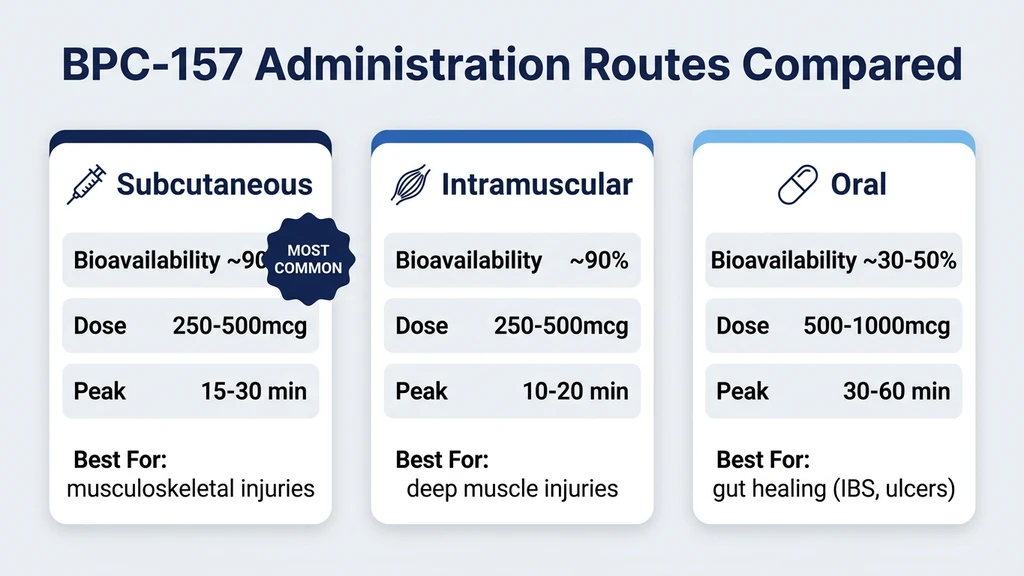
BPC-157 can be administered through three routes: subcutaneous injection, intramuscular injection, and oral ingestion. Each route has specific advantages depending on your condition, comfort level, and target tissue.
Subcutaneous Injection (Most Common)
Subcutaneous injection delivers BPC-157 into the fat layer just beneath the skin. This is the default route for most users and the method used in the majority of animal research.
Why subcutaneous wins for most situations: - Bioavailability is approximately 90%, meaning nearly all of the injected peptide reaches systemic circulation - Absorption is steady and predictable, with peak plasma levels within 15 to 30 minutes - The technique is simple enough to learn in 5 minutes - Insulin syringes (29 to 31 gauge) cause minimal discomfort - You can inject near the injury site to maximize local tissue concentration
Best for: Tendon injuries, ligament sprains, muscle tears, joint pain, post-surgical recovery, and any localized musculoskeletal condition. For specific knee injection guidance, see the knee injection site guide.
Injection sites: Lower abdomen (2 inches from the navel), near the injury, outer thigh, or upper arm. Rotate sites daily to prevent tissue irritation. For a complete step-by-step injection walkthrough including needle gauge selection and sterile technique, see how to inject BPC-157. A 200lb male and a 130lb female use the same dose at the same sites. For weight-specific protocol details, see the 200lb male dosing guide.
Intramuscular Injection
Intramuscular injection places the peptide directly into muscle tissue. Absorption is slightly faster than subcutaneous, with peak plasma concentration within 10 to 20 minutes.
When to consider intramuscular: - Deep muscle injuries (quad tear, hamstring strain, rotator cuff) - When you want to place the peptide as close to the damaged muscle fiber as possible - If subcutaneous fat is minimal and subcutaneous injection feels uncomfortable
Technique differences from subcutaneous: - Use a 25 to 27 gauge needle, 1 inch length - Insert at a 90-degree angle (not 45 degrees) - Inject into the deltoid, vastus lateralis (outer thigh), or gluteus medius - Do not aspirate for subcutaneous injections; for intramuscular, a brief aspiration confirms you have not entered a blood vessel
Drawback: Intramuscular injections carry a slightly higher risk of bruising and post-injection soreness. Most practitioners still prefer subcutaneous for BPC-157 because the peptide enters systemic circulation from any injection site and reaches damaged tissue through the bloodstream regardless of where you inject.
Oral Administration (BPC-157 Stable Variant)
BPC-157 is one of the few peptides that survives stomach acid. This property distinguishes it from nearly every other research peptide, which would be destroyed by gastric enzymes within minutes. The oral stability of BPC-157 has been confirmed across multiple studies, consistent with its origin as a fragment of a gastric protein (Sikiric et al., Curr Pharm Des, 2018).
Oral bioavailability runs approximately 30 to 50% compared to injection, meaning you need a higher dose to achieve equivalent systemic levels. Take oral BPC-157 on an empty stomach, at least 30 minutes before food, to maximize contact with the GI lining and reduce interference from digestive enzymes.
| Route | Bioavailability | Dose for Equivalent Effect | Peak Plasma Time |
|---|---|---|---|
| Subcutaneous | ~90% | 250 to 500mcg | 15 to 30 minutes |
| Intramuscular | ~90% | 250 to 500mcg | 10 to 20 minutes |
| Oral | ~30 to 50% | 500 to 1000mcg | 30 to 60 minutes |
Best for: Gut conditions (IBS, intestinal permeability, gastric ulcers, colitis). When you swallow BPC-157, it contacts the entire gastrointestinal lining directly before entering systemic circulation. This first-pass exposure delivers concentrated peptide exactly where gut injuries occur.
Format: Oral BPC-157 comes as capsules, tablets, or liquid solutions. The arginine salt form (BPC-157-Arg) is the most stable oral preparation. Some users dissolve lyophilized BPC-157 powder in water and drink it, though capsule formulations provide more consistent dosing.
Not ideal for: Musculoskeletal injuries where you want maximum bioavailability and targeted delivery near the injury site. If you are healing a torn tendon or sprained ligament, inject subcutaneously near the injury instead.
For more on oral BPC-157 research, see the BPC-157 peptide profile or the BPC-157 oral pills guide.
Step-by-Step Injection Guide
This section assumes you have a reconstituted vial of BPC-157 ready in your refrigerator. If you have not reconstituted your peptide yet, skip to the reconstitution section below and return here afterward.
Gather Your Supplies
Before your first injection, confirm you have everything on hand:
- Reconstituted BPC-157 vial (stored in the refrigerator)
- Insulin syringe: 29 to 31 gauge, 0.5 inch needle, 0.5mL or 1mL capacity
- Alcohol swabs (70% isopropyl alcohol)
- Sharps container for used needles
- Clean, flat surface with good lighting
Never reuse syringes. Each injection requires a fresh, sterile needle. Using a dull or contaminated needle introduces bacteria directly into subcutaneous tissue, creating an infection risk that no amount of peptide can fix.
Draw Your Dose
- 1.Wash your hands thoroughly with soap and water for at least 20 seconds.
- 2.Swab the vial stopper with an alcohol pad and let it air dry for 10 seconds.
- 3.Pull back the syringe plunger to the number of units you need (see the dosing table below).
- 4.Insert the needle through the center of the rubber stopper.
- 5.Push air into the vial (this equalizes pressure and makes drawing easier).
- 6.Invert the vial so the needle tip sits in the liquid.
- 7.Pull the plunger back slowly to your target volume. If you see bubbles, flick the syringe gently and push them back into the vial.
- 8.Withdraw the needle from the vial.
| Reconstitution | Concentration | Units for 250mcg | Units for 500mcg |
|---|---|---|---|
| 5mg vial + 1mL bac water | 5000mcg/mL | 5 units | 10 units |
| 5mg vial + 2mL bac water | 2500mcg/mL | 10 units | 20 units |
| 5mg vial + 2.5mL bac water | 2000mcg/mL | 12.5 units | 25 units |
Use the peptide reconstitution calculator if your vial size or water volume differs from these standard options.
Inject Subcutaneously
- 1.Choose your injection site. Lower abdomen (2 inches from the navel) is easiest for beginners. For localized injuries, inject within 1 to 3 cm of the damaged tissue.
- 2.Swab the injection site with a fresh alcohol pad. Let it air dry completely. Injecting through wet alcohol stings.
- 3.Pinch a fold of skin between your thumb and index finger.
- 4.Insert the needle at a 45-degree angle in one smooth motion. Do not hesitate or jab.
- 5.Release the skin pinch.
- 6.Push the plunger slowly and steadily. Rushing causes unnecessary pressure under the skin.
- 7.Count to 5 with the needle still inserted. This allows the liquid to disperse before withdrawal.
- 8.Withdraw the needle at the same angle you inserted it.
- 9.Press gently with a clean cotton pad if there is any bleeding. Do not rub.
- 10.Dispose of the syringe in a sharps container immediately.
The entire process takes under 2 minutes once you have practiced it a few times. Most users report feeling little more than a brief pinch. If you experience burning at the injection site, the peptide may be too cold; let the vial sit at room temperature for 3 to 5 minutes before drawing your dose.
BPC-157 Dosing: How Much to Take
The standard BPC-157 dose is 250 to 500mcg per day, administered once or twice daily. This range comes from extrapolation of animal study doses using FDA body surface area scaling, combined with clinical practice observations from peptide therapy providers.
Dosing by Condition
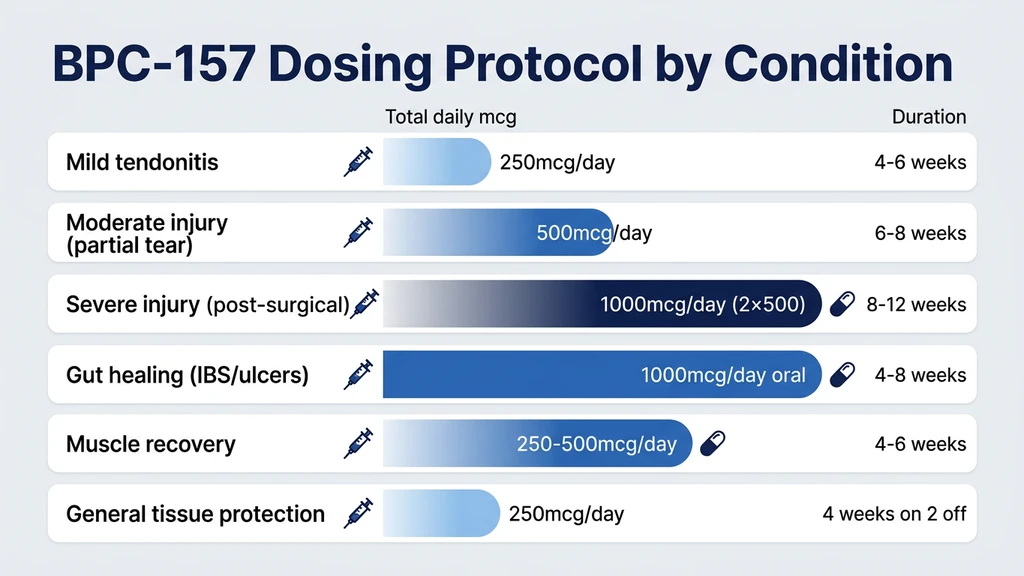
| Condition | Daily Dose | Frequency | Duration | Route |
|---|---|---|---|---|
| Mild tendonitis or strain | 250mcg | Once daily | 4 to 6 weeks | Subcutaneous near injury |
| Moderate injury (partial tear) | 500mcg | Once daily | 6 to 8 weeks | Subcutaneous near injury |
| Severe injury (full tear, post-surgical) | 500mcg | Twice daily (1000mcg total) | 8 to 12 weeks | Subcutaneous near injury |
| Gut healing (IBS, leaky gut, ulcers) | 500mcg | Twice daily | 4 to 8 weeks | Oral preferred |
| Muscle recovery and growth | 250 to 500mcg | Once daily | 4 to 6 weeks | Subcutaneous |
| General tissue protection | 250mcg | Once daily | 4 weeks on, 2 off | Subcutaneous (abdomen) |
Start at the lower end. Take 250mcg per day for the first 3 to 5 days. If you tolerate it without issues, increase to 500mcg. Jumping straight to 500mcg twice daily is unnecessary for most conditions and wastes peptide. For more on BPC-157 and exercise recovery, see the muscle growth article.
How Body Weight Affects Dosing
Body weight does not change the BPC-157 dose. BPC-157 works through receptor-mediated signaling, not plasma concentration. A 130lb woman and a 250lb man use the same 250 to 500mcg daily dose. The peptide binds to receptors in injured tissue and triggers downstream repair cascades (VEGF upregulation, FAK-paxillin activation, nitric oxide modulation). Once those receptors fire, the signal reaches full strength regardless of body mass.
Animal studies use weight-based dosing (10mcg/kg in rats), but FDA body surface area conversion yields approximately 1.6mcg/kg for humans. For a 90kg adult, that calculates to roughly 144mcg, which falls at the low end of the 250 to 500mcg clinical range. The calculation produces nearly identical human doses whether you start with a 60kg or 120kg subject. For the full breakdown, see BPC-157 dosage for a 200lb male.
For women-specific protocol considerations, see BPC-157 benefits for women.
Injection Site Selection: Near the Injury vs. Abdomen
Both work. The question is whether local concentration or convenience matters more for your situation.
Near the injury: Injecting subcutaneously within 1 to 3 cm of the damaged tissue delivers a high local concentration during the initial diffusion phase. Cerovecki et al. (2010) demonstrated that local BPC-157 administration improved ligament healing across functional, biomechanical, and histological measures in a rat MCL transection model. Local delivery consistently outperformed systemic delivery in that study.
Abdomen (systemic): The peptide enters systemic circulation and reaches all tissues, including the injury. Concentration at the injury site is lower than with local injection, but still therapeutic. Abdominal injection is easier, less intimidating for beginners, and perfectly appropriate when injury location is difficult to access or when the target is a deep structure.
Split protocol: Some users inject 60 to 70% of their daily dose near the injury and the remaining 30 to 40% in the abdomen. No published study validates this split approach, but the pharmacological reasoning is sound: maximize local tissue saturation while also providing systemic coverage.
For detailed injection site maps by knee injury type, see the knee injection guide.
How to Reconstitute BPC-157
BPC-157 arrives as a lyophilized (freeze-dried) white powder in a sealed glass vial. You must reconstitute it with bacteriostatic water before injection. This is the step that intimidates most beginners, but the process is straightforward and takes under 3 minutes.
Reconstitution Steps
- 1.Remove the plastic cap from the BPC-157 vial, exposing the rubber stopper.
- 2.Swab the stopper with an alcohol pad.
- 3.Draw bacteriostatic water into a syringe. For a 5mg vial, draw 2mL (the most common and practical dilution).
- 4.Insert the needle through the rubber stopper at an angle, aiming the tip at the glass wall inside the vial.
- 5.Release the water slowly down the inside wall of the vial. Do not spray it directly onto the powder. Direct impact can damage the peptide's molecular structure.
- 6.Let it dissolve. Gently swirl the vial in circular motions. Never shake. Aggressive shaking denatures the peptide chain. The powder should dissolve within 30 to 60 seconds, producing a clear, colorless solution.
- 7.Label the vial with the date of reconstitution and the concentration (e.g., "5mg/2mL = 2500mcg/mL").
- 8.Store immediately in the refrigerator at 2 to 8 degrees Celsius.
Use bacteriostatic water, not sterile water. Bacteriostatic water contains 0.9% benzyl alcohol, which inhibits bacterial growth and keeps your reconstituted peptide safe for up to 30 days. Sterile water has no preservative and allows bacterial contamination within 24 to 48 hours. If you need a source, see where to buy bacteriostatic water for injection. For storage specifics, see does bacteriostatic water need to be refrigerated. For a detailed guide on reconstitution technique for all peptides, see how to reconstitute peptides. For information on how long your reconstituted peptide remains potent, see how long reconstituted peptides last.
Reconstitution Math
The amount of bacteriostatic water you add determines the concentration, which determines how many units you draw per dose.
| Vial Size | Water Added | Concentration | Volume for 250mcg | Volume for 500mcg | Doses at 500mcg/day |
|---|---|---|---|---|---|
| 5mg | 1mL | 5000mcg/mL | 0.05mL (5 units) | 0.10mL (10 units) | 10 doses |
| 5mg | 2mL | 2500mcg/mL | 0.10mL (10 units) | 0.20mL (20 units) | 10 doses |
| 5mg | 2.5mL | 2000mcg/mL | 0.125mL (12.5 units) | 0.25mL (25 units) | 10 doses |
| 10mg | 2mL | 5000mcg/mL | 0.05mL (5 units) | 0.10mL (10 units) | 20 doses |
The 2mL dilution in a 5mg vial is the sweet spot for most users. It produces 20-unit draws for a 500mcg dose, which is easy to measure accurately on a standard 1mL insulin syringe (each small tick mark = 1 unit). Very small volumes (5 units) are harder to measure precisely and increase dosing error.
Use the peptide reconstitution calculator for custom vial sizes and water volumes.
Cycle Length and Timing
BPC-157 protocols follow a defined cycle with rest periods. Running the peptide continuously without breaks risks receptor downregulation, where the target receptors become less sensitive over time and the peptide loses effectiveness.
Standard Cycle Structure
| Phase | Duration | Dose | Notes |
|---|---|---|---|
| Initial assessment | Days 1 to 5 | 250mcg once daily | Monitor for side effects |
| Active healing | Weeks 1 to 4 (or 1 to 8) | 250 to 500mcg, 1 to 2x daily | Adjust based on injury severity |
| Taper (optional) | Final 3 to 5 days | Reduce to 250mcg once daily | Not strictly necessary |
| Rest period | 2 to 4 weeks | No BPC-157 | Allows receptor resensitization |
| Second cycle (if needed) | 4 to 8 weeks | Same as active phase | Reassess progress first |
A 4-week cycle is sufficient for mild injuries (tendonitis, strains). Moderate injuries (partial tears, chronic tendinopathy) typically require 6 to 8 weeks. Severe injuries and post-surgical recovery may warrant 8 to 12 weeks, though evidence for cycles beyond 8 weeks is limited to clinical observation rather than published research.
Morning vs. Evening Injection
BPC-157 interacts with the dopaminergic system, which regulates alertness and wakefulness (Sikiric et al., J Physiol Paris, 1999). Approximately 10 to 15% of users report mild sleep disruption when injecting in the evening. The effect is typically subtle: slight difficulty falling asleep rather than full insomnia.
Morning injection (recommended for most users): Inject between 6 AM and 10 AM. This aligns with your body's natural cortisol peak and avoids any potential interference with evening melatonin production. The downstream healing processes BPC-157 triggers (collagen synthesis, angiogenesis, growth factor release) persist for hours regardless of when you inject. For a complete breakdown of optimal timing windows, see when to take BPC-157.
Evening injection (acceptable if no sleep issues): Some users prefer evening injection to align with the body's overnight tissue repair window. Growth hormone peaks during deep sleep, and BPC-157's VEGF upregulation may theoretically complement this process. If evening dosing disrupts your sleep, switch to morning immediately.
Twice-daily dosing: Inject once in the morning and once in the early afternoon (before 3 PM). Avoid a late evening second dose.
For a deep dive on BPC-157 and sleep, see does BPC-157 cause insomnia.
Timing Relative to Food and Exercise
Food: No established interaction with meals exists for injectable BPC-157. You can inject before, during, or after eating without affecting absorption. For oral BPC-157, take it on an empty stomach (at least 30 minutes before food) to maximize contact with the GI lining and reduce interference from digestive enzymes.
Exercise: Inject at least 20 to 30 minutes before or after training. Intense exercise increases blood flow and heart rate, which may accelerate peptide clearance from the injection site before adequate local absorption occurs. Some users prefer post-workout injection to coincide with the body's natural inflammatory repair response triggered by exercise.
Other peptides: If stacking BPC-157 with other peptides, inject them at separate sites but at the same time of day. Drawing multiple peptides into a single syringe is technically possible but introduces contamination risk between vials. Use separate syringes.
Stacking BPC-157 with TB-500
The BPC-157 plus TB-500 combination is the most widely used peptide stack for injury recovery. The two peptides work through different mechanisms and produce complementary effects that neither achieves alone.
BPC-157 promotes localized tissue repair through VEGF upregulation, nitric oxide modulation, and fibroblast activation. TB-500 (Thymosin Beta-4) promotes systemic repair through actin regulation, which controls cell migration and tissue remodeling across the entire body. BPC-157 sends a repair crew to the specific injury site; TB-500 upgrades the repair infrastructure everywhere.
| Component | BPC-157 | TB-500 |
|---|---|---|
| Mechanism | VEGF, NO, FAK-paxillin | Actin binding, cell migration |
| Scope | Localized + systemic | Primarily systemic |
| Standard dose | 250 to 500mcg/day | 5 to 10mg/week (loading) |
| Maintenance dose | Same | 2.5 to 5mg/week |
| Route | Subcutaneous (near injury) | Subcutaneous (anywhere) |
| Cycle | 4 to 8 weeks | 4 to 8 weeks (aligned) |
Stack protocol: Run both peptides simultaneously. BPC-157 at 500mcg daily injected near the injury. TB-500 at 5 to 10mg per week split into 2 to 3 doses during the loading phase (weeks 1 to 4), then 2.5 to 5mg per week during maintenance (weeks 5 to 8). Adding TB-500 does not change the BPC-157 dose.
For a complete breakdown of this combination, including dosing for blended vials that add GHK-Cu as a third component, see the GHK-Cu, BPC-157, and TB-500 blend guide. For additional stacking combinations with other peptides, see the peptide stacking guide. Use the peptide stack calculator to plan your protocol and the peptide interaction checker to verify safety.
Storage Requirements
Peptide potency depends entirely on proper storage. BPC-157 is more stable than most peptides (its gastric origin makes it resistant to acid and heat), but it still degrades when handled carelessly.
Before Reconstitution (Lyophilized Powder)
- Refrigerator (2 to 8 degrees Celsius): Stable for 12 to 24 months
- Room temperature: Stable for 3 to 6 months, but refrigeration is always preferred
- Freezer (-20 degrees Celsius): Stable for 2 or more years (ideal for long-term storage of unopened vials)
- Avoid: Direct sunlight, temperatures above 30 degrees Celsius, humidity
Lyophilized BPC-157 is resilient. A few hours at room temperature during shipping will not destroy it. Place it in the refrigerator or freezer within 24 hours of receiving your order.
After Reconstitution (Liquid Form)
- Refrigerator (2 to 8 degrees Celsius): Use within 30 days
- Room temperature: Potency drops measurably within 10 to 14 days; avoid leaving reconstituted vials unrefrigerated
- Freezer: Do not freeze reconstituted peptides. Ice crystal formation damages the peptide structure
After reconstitution, the clock starts. Mark the date on the vial with a marker. If your cycle runs longer than 30 days at 500mcg daily from a single 5mg vial (it will not, since a 5mg vial provides only 10 days at 500mcg/day), reconstitute a fresh vial.
Never leave a reconstituted vial on the counter while you inject. Remove it from the fridge, draw your dose, and return it within 2 minutes. Cumulative room-temperature exposure adds up over a 10 to 30 day use period.
For the full storage guide covering all peptides, see how to store peptides. For degradation timelines, see how long reconstituted peptides last.
Common Mistakes Beginners Make
These are the errors that most frequently undermine BPC-157 protocols. Each one is avoidable with basic preparation.
Dosing and Technique Errors
Mistake 1: Using sterile water instead of bacteriostatic water. Sterile water contains no preservative. Bacteria begin colonizing the vial within 24 to 48 hours of reconstitution. By day 5, you are injecting a bacterial broth along with your peptide. Bacteriostatic water (0.9% benzyl alcohol) prevents this for up to 30 days.
Mistake 2: Shaking the vial after reconstitution. Vigorous shaking denatures the peptide chain through agitation-induced aggregation. The BPC-157 molecules unfold and clump together, reducing potency. Swirl gently in circular motions.
Mistake 3: Injecting too fast. Rapid injection creates a bolus of liquid that pools under the skin and causes stinging, redness, and a visible lump. Push the plunger slowly over 3 to 5 seconds. Let the liquid disperse naturally through subcutaneous tissue.
Mistake 4: Not rotating injection sites. Injecting in the same spot every day creates localized tissue irritation, small lumps, and potentially lipodystrophy (changes in fat tissue structure) over weeks. Rotate between at least 3 to 4 sites, even when injecting near an injury. Move the injection point by 1 to 2 cm each day within the target area.
Mistake 5: Miscalculating the concentration. If you add 2mL of bacteriostatic water to a 5mg vial, the concentration is 2500mcg/mL, and 500mcg equals 20 units. If you mistakenly calculate it as 5000mcg/mL (the concentration for 1mL dilution), you inject half your intended dose. Always double-check your math or use the BPC-157 dosage calculator.
Protocol Errors
Mistake 6: Quitting after 1 week. BPC-157 initiates cellular repair processes that take time to produce noticeable results. Tendon healing requires 3 to 6 weeks of consistent signaling. Users who stop at day 7 because they "don't feel anything" abandoned the protocol before it had time to work.
Mistake 7: Running indefinitely without breaks. Continuous BPC-157 use beyond 8 to 12 weeks risks receptor downregulation. The dopamine and serotonin receptors that BPC-157 modulates may become less sensitive, reducing the peptide's effectiveness. Standard practice is 4 to 8 weeks on, followed by 2 to 4 weeks off.
Mistake 8: Starting at the maximum dose. Jumping to 500mcg twice daily (1000mcg total) on day one is unnecessary. The research literature shows therapeutic effects at much lower doses. Start at 250mcg once daily for 3 to 5 days, assess your response, and titrate upward only if needed.
Mistake 9: Ignoring side effects. BPC-157 has an excellent safety profile in animal studies, with no lethal dose identified across 36 published studies (Kang et al., 2025 systematic review). But individual responses vary. If you experience persistent blood pressure changes, sleep disruption, or any unusual symptoms, reduce the dose or stop and consult a healthcare provider. For liver safety information, see does BPC-157 cause liver damage.
Danger Scenarios: When Things Go Wrong
Most BPC-157 side effects are mild and self-resolving. The real dangers come from contamination, errors in preparation, and buying counterfeit product. These scenarios are preventable, but they can cause serious harm if ignored.
Contamination Risks
Bacterial contamination is the most dangerous risk of self-administered peptide injection. It occurs when:
- You use non-sterile water for reconstitution
- You touch the rubber stopper or needle tip with your fingers
- You reuse syringes
- You store reconstituted peptides at room temperature for extended periods
- You use a vial that has been reconstituted for more than 30 days
Signs of a contaminated vial: cloudiness, visible particles, color change (from clear to yellow or brown), unusual smell. If you observe any of these, discard the vial immediately.
Signs of injection site infection: redness that spreads beyond 2 cm from the injection point, warmth, swelling that increases over 24 to 48 hours, pus, fever. Seek medical attention immediately. Do not attempt to treat an injection site infection with more BPC-157.
Wrong Concentration Errors
A concentration miscalculation can cause you to inject 2x, 5x, or 10x your intended dose. While BPC-157 has shown no lethal dose in any published study (doses up to 20mg IV in a human pilot study produced no adverse events (Staresinic et al., 2025)), massive overdosing wastes expensive peptide and may increase the risk of side effects like blood pressure fluctuation or sleep disruption.
The most common error: confusing a 5mg vial with a 10mg vial. If you add 2mL of water to a 10mg vial thinking it contains 5mg, you calculate the concentration as 2500mcg/mL when it is actually 5000mcg/mL. Every injection delivers double your target dose. Always verify the vial label before reconstitution.
Second most common error: confusing mL with units. 0.20mL equals 20 units on an insulin syringe. If you read "20" as 0.02mL instead of 0.20mL, you inject one-tenth of your intended dose. Familiarize yourself with insulin syringe markings before your first injection.
Counterfeit and Degraded Product
BPC-157 is not regulated by the FDA. Quality varies dramatically between suppliers. Underdosed, mislabeled, and outright counterfeit vials circulate widely. A vial labeled "5mg BPC-157" may contain 2mg, 0mg, or an entirely different compound.
Protective measures: - Buy from suppliers that provide third-party certificates of analysis (COA) for each batch - Verify the COA includes HPLC purity testing (should show 98% or higher purity) and mass spectrometry confirmation - Check that the lot number on the COA matches the lot number on your vial - Store properly upon receipt (refrigerate immediately)
For complete safety guidance on peptide sourcing and use, see the peptide safety guide.
BPC-157 and Alcohol
BPC-157 has been studied specifically in the context of alcohol-induced damage. Animal research shows BPC-157 protects against alcohol-induced gastric lesions, reduces liver damage markers in ethanol-exposed rats, and counteracts some neurobehavioral effects of acute alcohol intoxication (Sikiric et al., Curr Pharm Des, 2018).
This does not mean BPC-157 is a hangover cure or a free pass to drink during your cycle. Alcohol impairs tissue healing, disrupts sleep quality, increases inflammation, and may counteract the very repair processes BPC-157 promotes. Using BPC-157 to heal a torn tendon while consuming 4 drinks per night is like running a humidifier and a dehumidifier in the same room.
Practical guideline: Minimize or eliminate alcohol during your BPC-157 cycle. If you do drink, keep it to 1 to 2 drinks on rare occasions, and avoid alcohol within 4 hours of injection. For the full research breakdown, see BPC-157 and alcohol.
What to Expect: Timeline of Effects
BPC-157 does not produce overnight results. Tissue repair is a biological process measured in weeks, not hours. Understanding the typical timeline prevents premature discouragement and unnecessary dose escalation.
| Timeframe | What Happens | What You Feel |
|---|---|---|
| Days 1 to 3 | VEGF upregulation begins, angiogenesis initiates | Usually nothing noticeable |
| Days 4 to 7 | Increased blood flow to injury, fibroblast migration | Mild warmth at injury site, slight reduction in acute pain |
| Weeks 2 to 3 | Collagen deposition accelerates, tissue remodeling begins | Gradual pain reduction, improved range of motion |
| Weeks 4 to 6 | Structural repair progresses, new tissue matures | Noticeable improvement in function and pain levels |
| Weeks 6 to 8 | Continued remodeling, tissue strength increases | Significant functional recovery for most injuries |
Individual responses vary based on injury severity, age, nutrition, sleep quality, and concurrent activity level. Some users report dramatic improvement by week 2. Others need the full 8 weeks before noticing meaningful change. Both outcomes are normal.
The one universal signal that BPC-157 is working: increased warmth or a mild "buzzing" sensation at the injury site during the first week. This reflects increased blood flow from VEGF-driven angiogenesis. Not everyone notices it, but those who do can be confident the peptide is active.
Safety Profile and Side Effects
A 2025 systematic review analyzing 36 animal studies spanning 1993 to 2024 found no lethal dose of BPC-157 across any tested species or route of administration (Kang et al., 2025). The first human safety data, published in 2025, showed no adverse effects from 10mg and 20mg intravenous BPC-157 infusions in healthy adults (Staresinic et al., 2025).
BPC-157 has not undergone large-scale human clinical trials. Long-term safety data does not exist. The absence of identified toxicity in preclinical studies is encouraging but not a guarantee of safety in all humans under all conditions.
Reported side effects (from clinical observation and community reports):
| Side Effect | Frequency | Severity | Management |
|---|---|---|---|
| Injection site redness | 15 to 20% | Mild | Rotate sites, ice if needed |
| Mild nausea (oral route) | 10 to 15% | Mild | Take with small amount of water |
| Sleep disruption | 10 to 15% | Mild | Switch to morning injection |
| Headache | 5 to 10% | Mild | Hydrate, reduce dose |
| Dizziness | 3 to 5% | Mild | Reduce dose, sit during injection |
| Blood pressure fluctuation | Rare | Moderate | Monitor, consult provider |
BPC-157 interacts with blood pressure regulation through the nitric oxide system. Users with pre-existing hypertension or those taking blood pressure medications should exercise particular caution and consult their healthcare provider before starting. For more detail, see does BPC-157 cause high blood pressure.
For a comprehensive overview of peptide safety principles, see the peptide safety guide.
Frequently Asked Questions
How do I get BPC-157?
Two options exist in 2026. First: obtain a prescription from a functional medicine doctor or telehealth provider and fill it at a licensed compounding pharmacy ($150 to $300 per vial). Second: purchase from a research vendor without a prescription ($35 to $65 per 5mg vial for research use). For either route, confirm HPLC purity at 98%+ from a third-party certificate of analysis before use. See the peptide safety guide for vendor vetting criteria.
How long does it take for BPC-157 to start working?
Most users notice initial changes within 7 to 14 days, typically as reduced pain or increased warmth at the injury site. Significant structural healing takes 4 to 6 weeks. Animal studies show measurable increases in VEGF expression and fibroblast migration within 48 to 72 hours, but these cellular changes are not perceptible. Plan for a minimum 4-week cycle before evaluating results. See the full BPC-157 dosage guide for protocol timing.
Can I take BPC-157 orally instead of injecting?
Yes. BPC-157 survives stomach acid, unlike most peptides. Oral bioavailability runs approximately 30 to 50% compared to 90% for subcutaneous injection, so oral doses are higher: 500 to 1000mcg per day on an empty stomach. Oral is preferred for gut conditions (IBS, ulcers, intestinal permeability) because the peptide contacts the GI lining directly. For musculoskeletal injuries, subcutaneous injection delivers superior bioavailability. See BPC-157 oral pills for more detail.
What is the best place to inject BPC-157?
For musculoskeletal injuries: inject subcutaneously within 1 to 3 cm of the damaged tissue. Cerovecki et al. (2010) confirmed that local injection outperformed systemic delivery for ligament healing. For gut conditions or systemic use: the lower abdomen (2 inches from the navel) is easiest and most accessible. Rotate between 3 to 4 sites daily to prevent tissue irritation. See the knee injection guide for site-specific maps.
What is the best time of day to inject BPC-157?
Morning, between 6 AM and 10 AM. BPC-157 modulates dopamine receptors, which can increase alertness. Roughly 10 to 15% of users report mild sleep disruption from evening injections. Morning dosing avoids this entirely. If using twice-daily dosing, inject the second dose before 3 PM. The healing effects persist regardless of injection timing. See when to take BPC-157 for detailed timing analysis.
What happens if I miss a dose of BPC-157?
Nothing harmful. BPC-157 triggers repair cascades that persist for hours after a single injection. Missing 1 dose in a 4 to 8 week cycle has no measurable impact on outcomes. Do not double your next dose to compensate. Resume your regular schedule the following day. Consistency over weeks matters far more than any single injection.
How many vials of BPC-157 do I need for one cycle?
At 500mcg per day from a 5mg vial, each vial provides 10 doses (10 days). A 4-week cycle requires 3 vials. A 6-week cycle requires about 4 to 5 vials. An 8-week cycle requires 6 vials. At 250mcg per day, these numbers are halved: a 4-week cycle needs only 2 vials. Use the BPC-157 dosage calculator to plan your supply before starting.
Do I need to cycle off BPC-157?
Yes. Standard practice is 4 to 8 weeks on, followed by 2 to 4 weeks off. Continuous use beyond 8 to 12 weeks risks receptor downregulation, where dopamine D2 receptors and other targets become less sensitive. The rest period allows receptors to resensitize. If your injury is not fully healed after 1 cycle, take 2 to 4 weeks off and begin a second cycle.
The Bottom Line
Taking BPC-157 correctly comes down to five decisions: route (subcutaneous injection for injuries, oral for gut healing), dose (250 to 500mcg per day), timing (morning preferred), cycle length (4 to 8 weeks on, 2 to 4 weeks off), and injection site (near the injury for maximum local concentration).
The process is simpler than it appears. Reconstitute your vial with 2mL of bacteriostatic water, draw 20 units for a 500mcg dose, pinch the skin near your injury, insert at 45 degrees, push slowly, and you are done. The entire routine takes 2 minutes once you have practiced it.
What separates successful BPC-157 protocols from failed ones is not technique or dose optimization. Consistency is the deciding factor. Inject every day at the same time for the full cycle duration. Store the vial properly. Do not quit at week 1. The biology works on a timeline measured in weeks, not days.
Use the BPC-157 dosage calculator to convert your chosen dose into exact syringe units. Use the reconstitution calculator to verify your concentration math. And consult a licensed healthcare provider before beginning any peptide protocol.
Related articles: - How to Inject BPC-157: detailed injection technique, site selection, and needle gauge guide - BPC-157 Side Effects: complete safety profile with frequency and management - BPC-157 Dosage for a 200lb Male: weight-adjusted protocol and syringe unit calculator - BPC-157 Oral Pills: oral formulation research and dosing for gut conditions - What Does TB-500 Do?: the synergy partner for BPC-157 tissue repair stacks - How to Reconstitute Tirzepatide: same reconstitution process applies to all lyophilized peptides
Related Articles
Where to Inject BPC-157: Site Guide
Where to inject BPC-157 for shoulder, back, hip, gut, elbow, and Achilles injuries. Anatomical sites, local vs systemic delivery, and rotation.
BPC-157 TB-500 Dosage: Combined Protocol
BPC-157 TB-500 dosage: 250-500 mcg BPC-157 + 2-2.5 mg TB-500 daily. Weight-adjusted charts, injury-type matrix, blend vial math, and cycle timing.
KLOW Peptide: Benefits, Dosage, and KLOW vs GLOW
KLOW peptide benefits, blend composition (GHK-Cu, BPC-157, TB-500, KPV), per-component dosing math, the copper ceiling, and how KLOW differs from GLOW.
BPC-157 Dosage for 200lb Male
BPC-157 dosage for a 200lb male is 250-500mcg/day. Peptide dosing is not weight-dependent. Protocols, reconstitution math, cycle length, and stacking options.