You have two vials on your desk: one labeled BPC-157 (5 mg) and one labeled TB-500 (5 mg). Your goal is to run both peptides together for injury recovery, but every forum thread gives different numbers. The standard combined protocol is 250-500 mcg of BPC-157 plus 2-2.5 mg of TB-500, both injected subcutaneously once daily for 4-8 weeks (Gwyer et al., J Complement Integr Med, 2019). This dosing is extrapolated from individual peptide research, as no study has tested the specific combination. Body weight, injury severity, and administration route all modify these baseline numbers.
| Quick Dosage Reference | BPC-157 | TB-500 |
|---|---|---|
| Standard daily dose (injectable) | 250-500 mcg SubQ | 2-2.5 mg SubQ |
| Loading dose (weeks 1-2) | 500 mcg/day | 2.5 mg/day |
| Maintenance dose (weeks 3-6) | 250 mcg/day | 1.5 mg 2x/week |
| Oral daily dose (capsules) | 500-1,000 mcg | 1,500-3,000 mcg |
| Injection frequency | 1-2x daily | 1x daily or 2-3x/week |
| Cycle length | 4-8 weeks | 4-8 weeks |
| Washout period | 2-4 weeks | 2-4 weeks |
| Standard vial size | 5 mg | 5 mg or 10 mg |
BPC-157 is not FDA-approved. No completed human clinical trial exists for this combination. Consult a healthcare provider before use.
For individual peptide calculators, use our BPC-157 dosage calculator and TB-500 dosage calculator. For the injectable stacking overview, see our wolverine peptide stack guide.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
Why Stack BPC-157 and TB-500?
These two peptides target different phases of tissue repair. Running them together covers both the acute stabilization and long-term remodeling stages.
Think of recovering from a house fire. BPC-157 is the emergency crew: it stops the damage from spreading, stabilizes structures, and gets the water and electricity running again. It upregulates VEGF to restore blood supply and stabilizes nitric oxide for vascular function (Hsieh et al., Sci Rep, 2020). TB-500 is the rebuilding contractor: it brings in new materials, coordinates the workforce, and rebuilds the structure from the foundation. It promotes actin polymerization for cell migration and modulates inflammation to prevent scar tissue formation (Goldstein & Kleinman, Expert Opin Biol Ther, 2012).
Running both simultaneously means the emergency repair and structural rebuilding happen in parallel rather than sequentially. The non-overlapping mechanisms provide a logical basis for the combination, even though no controlled study has tested BPC-157 and TB-500 together.
Injectable Dosage Protocols
Three dosing tiers accommodate different injury severities and user experience levels. All protocols assume subcutaneous injection.
Standard Protocol (Most Common)
This is the baseline protocol for moderate injuries: partial tendon tears, chronic joint pain, muscle strains, or post-surgical recovery starting 1-2 weeks after the procedure.
| Week | BPC-157 Dose | BPC-157 Frequency | TB-500 Dose | TB-500 Frequency |
|---|---|---|---|---|
| 1-2 | 500 mcg | Once daily | 2.5 mg | Once daily |
| 3-4 | 250 mcg | Twice daily | 2 mg | 3x per week |
| 5-6 | 250 mcg | Once daily | 1.5 mg | 2x per week |
| 7-8 | 250 mcg | Once daily | None | Taper complete |
BPC-157 injection site: subcutaneously as close to the injury as possible. For a knee tendon, inject above or below the patella. For a shoulder, inject into the deltoid subcutaneous tissue near the rotator cuff. Learn where to inject BPC-157 for knee injuries or see our general how to inject BPC-157 guide.
TB-500 injection site: subcutaneously in the abdomen, thigh, or deltoid. TB-500 works systemically, so injection location matters less than for BPC-157. Rotate injection sites to prevent lipodystrophy.
Aggressive Protocol (Severe Injuries)
For acute severe injuries: complete tendon ruptures (non-surgical management), large muscle tears, or severe joint degeneration. This protocol uses higher doses for the first two weeks, then steps down.
| Week | BPC-157 Dose | BPC-157 Frequency | TB-500 Dose | TB-500 Frequency |
|---|---|---|---|---|
| 1-2 | 500 mcg | Twice daily | 2.5 mg | Once daily |
| 3-4 | 500 mcg | Once daily | 2.5 mg | 3x per week |
| 5-6 | 250 mcg | Twice daily | 2 mg | 2x per week |
| 7-8 | 250 mcg | Once daily | 1.5 mg | 2x per week |
Total BPC-157 consumption: approximately 28 mg over 8 weeks. Total TB-500 consumption: approximately 70 mg over 8 weeks.
The 2025 human IV pilot administered 20 mg of BPC-157 as a single IV bolus with no adverse events (Altern Ther Health Med, 2025). This provides context for the safety margin, though subcutaneous daily dosing and single IV bolus dosing are pharmacokinetically different.
Conservative Protocol (Prevention and Maintenance)
For users without a specific acute injury: aging athletes maintaining joint health, individuals recovering from minor repetitive strain, or those in the later stages of healing after completing a standard cycle.
| Week | BPC-157 Dose | BPC-157 Frequency | TB-500 Dose | TB-500 Frequency |
|---|---|---|---|---|
| 1-4 | 250 mcg | Once daily | 2 mg | 2x per week |
| 5-8 | 250 mcg | Every other day | 1.5 mg | 1x per week |
Total BPC-157 consumption: approximately 10.5 mg over 8 weeks. Total TB-500 consumption: approximately 22 mg over 8 weeks. This conservative approach uses roughly 40-60% less peptide than the standard protocol.
Blend Vial Dosing: Reconstitution Math
Many vendors sell pre-blended vials containing both BPC-157 and TB-500 in a single lyophilized powder. The most common blend is 10 mg total (5 mg BPC-157 + 5 mg TB-500 or other ratios). Reconstituting a blend vial requires careful math because each injection delivers both peptides in a fixed ratio.
Example: 10 mg blend vial (5 mg BPC-157 + 5 mg TB-500)
Add 2 mL of bacteriostatic water. The resulting concentration: - BPC-157: 5,000 mcg / 2 mL = 2,500 mcg/mL - TB-500: 5,000 mcg / 2 mL = 2,500 mcg/mL
To inject 250 mcg BPC-157 + 250 mcg TB-500, draw 10 units (0.1 mL) on an insulin syringe.
The problem: this fixed ratio delivers equal doses of both peptides, but the standard protocol calls for roughly 5x more TB-500 (2,500 mcg) than BPC-157 (500 mcg). A blend vial with a 1:1 ratio forces you to either underdose TB-500 or massively overdose BPC-157.
| Blend Ratio | To Get 500 mcg BPC-157 | TB-500 Delivered | Matches Protocol? |
|---|---|---|---|
| 1:1 (5mg + 5mg) | Draw 20 units | 500 mcg (low) | No, TB-500 underdosed |
| 1:5 (2mg + 10mg) | Draw 20 units | 2,000 mcg | Close to protocol |
| 1:5 (5mg + 25mg) | Draw 10 units | 2,500 mcg | Yes, matches standard |
Recommendation: if using a blend vial, choose one with a 1:5 ratio (BPC-157:TB-500) to match standard dosing protocols. Alternatively, buy separate vials for full dose flexibility. For reconstitution guidance, use our peptide reconstitution calculator and see our how to reconstitute peptides guide.
Oral Dosage Protocol
Oral BPC-157 + TB-500 capsules bypass the reconstitution complexity but introduce bioavailability considerations. For a full analysis of capsule efficacy, see our BPC-157 + TB-500 capsules guide.
| Phase | Capsules/Day | BPC-157 per Day | TB-500 per Day | Duration |
|---|---|---|---|---|
| Loading | 2 capsules | ~1,000 mcg | ~1,500-3,000 mcg | Weeks 1-2 |
| Standard | 1-2 capsules | ~500-1,000 mcg | ~750-1,500 mcg | Weeks 3-6 |
| Maintenance | 1 capsule | ~500 mcg | ~750-1,500 mcg | Weeks 7-8 |
Oral doses are higher than injectable doses to compensate for lower bioavailability. BPC-157 acetate capsules deliver approximately 3% systemically; the gut receives the full local dose. TB-500 oral bioavailability is unproven.
Timing: take capsules with a small meal in the morning. If using 2 capsules daily, space them 6-8 hours apart. Avoid dosing after 2 PM to prevent sleep disruption from BPC-157's dopaminergic effects.
Hybrid approach (oral + injectable): take oral BPC-157 capsules in the morning for GI support and baseline systemic levels. Inject TB-500 subcutaneously near the injury site in the evening for confirmed systemic delivery. This approach gives each peptide its most effective route.
Dose Adjustments by Body Weight
Heavier individuals distribute peptides across a larger volume of tissue and blood. These adjustments scale the standard protocol by body weight.
| Body Weight | BPC-157 Daily (Standard) | TB-500 Daily (Loading) | TB-500 (Maintenance) |
|---|---|---|---|
| Under 60 kg (132 lb) | 250 mcg | 2 mg | 1-1.5 mg 2x/week |
| 60-80 kg (132-176 lb) | 250-500 mcg | 2-2.5 mg | 1.5 mg 2-3x/week |
| 80-100 kg (176-220 lb) | 500 mcg | 2.5 mg | 2 mg 2-3x/week |
| Over 100 kg (220+ lb) | 500 mcg (consider 2x/day) | 2.5-3 mg | 2-2.5 mg 2-3x/week |
These weight-based adjustments are extrapolated from body surface area scaling used in pharmacology. No BPC-157 or TB-500 study has conducted formal weight-based dosing analysis in humans. The adjustments represent community consensus, not clinical evidence.
For weight-specific BPC-157 guidance, see our BPC-157 dosage for 200lb male guide and our comprehensive BPC-157 dosage by body weight chart. The BPC-157 dosage calculator accounts for body weight automatically.
Dose Adjustments by Injury Type
The nature of the injury determines which peptide to emphasize and where to inject.
| Injury Category | BPC-157 Emphasis | TB-500 Emphasis | Injection Strategy |
|---|---|---|---|
| Tendon (Achilles, patellar, rotator cuff) | Standard dose, inject near tendon | Higher dose (2.5 mg/day loading) | BPC-157 peritendinous, TB-500 abdomen |
| Joint (knee OA, hip, shoulder) | Standard dose, inject near joint | Standard dose | BPC-157 periarticular, TB-500 deltoid |
| Muscle (strain, tear) | Standard dose, inject near muscle | Higher dose | BPC-157 near tear, TB-500 abdomen |
| GI (ulcer, leaky gut, IBS) | Higher oral dose (1,000 mcg) | Optional (injectable if used) | BPC-157 oral, TB-500 SubQ abdomen |
| Post-surgical | Standard dose, inject near wound | Standard dose | Both near surgical site (after 48-72 hrs) |
Tendon injuries respond well to BPC-157 because it upregulates growth hormone receptor expression in tendon fibroblasts (Chang et al., J Mol Histol, 2011). TB-500 supports the broader remodeling phase. Injecting BPC-157 near the tendon puts the peptide where fibroblast activation matters most.
GI conditions call for oral BPC-157 as the primary agent. Sikiric et al. demonstrated oral BPC-157 heals gastric ulcers and counteracts NSAID-induced GI damage in rats (Sikiric et al., Curr Pharm Des, 2011). TB-500 is optional for GI protocols; if included, inject subcutaneously for reliable systemic delivery.
Muscle injuries benefit from TB-500's actin polymerization effects, which promote satellite cell migration into the damaged fibers. Use the higher end of TB-500 dosing (2.5 mg/day during loading) for significant muscle tears.
Cycle Duration and Washout
Running BPC-157 and TB-500 together follows the same cycling principles as individual peptide protocols, with one addition: the TB-500 taper should begin before the BPC-157 taper.
Standard 8-week cycle structure:
| Phase | Weeks | BPC-157 | TB-500 | Purpose |
|---|---|---|---|---|
| Loading | 1-2 | Full dose daily | Full dose daily | Rapid tissue saturation |
| Active healing | 3-6 | Full or standard dose | Reduced frequency | Sustained repair support |
| TB-500 taper | 7 | Maintain BPC-157 | Reduce to 1x/week | Wind down systemic peptide |
| BPC-157 taper | 8 | Reduce to every other day | Stop | Final transition |
| Washout | 9-12 | None | None | Receptor reset |
Why taper TB-500 first? TB-500 has a longer biological half-life and accumulates in tissue over the 6-week active phase. Stopping abruptly creates a sharper drop. Tapering over week 7 smooths the transition. BPC-157 has shorter-acting effects and can be tapered quickly in week 8.
Repeat cycles: wait a minimum of 2 weeks (preferably 4) before starting another cycle. This washout allows peptide receptor sensitivity to normalize. Running back-to-back cycles without a break may produce diminishing returns as receptors downregulate.
Extended protocols: some users run 12-week cycles for severe chronic injuries. No safety data covers oral or injectable BPC-157 + TB-500 use beyond 8 weeks. If extending beyond the standard cycle, consult a physician and monitor for unusual symptoms. Before starting any extended protocol, consider baseline cancer screening given both peptides' pro-angiogenic properties.
How Many Vials Do You Need?
One of the most practical questions for protocol planning is how many vials to order.
Standard Protocol (8 weeks): - BPC-157: 500 mcg daily for 2 weeks + 500 mcg daily for 4 weeks + 250 mcg daily for 2 weeks = ~17.5 mg total. Requires four 5 mg vials. - TB-500: 2.5 mg daily for 2 weeks + 2 mg 3x/week for 4 weeks + 1.5 mg 2x/week for 2 weeks = ~48.5 mg total. Requires ten 5 mg vials.
Aggressive Protocol (8 weeks): - BPC-157: 500 mcg 2x/day for 2 weeks + 500 mcg daily for 2 weeks + 250 mcg 2x/day for 4 weeks = ~28 mg total. Requires six 5 mg vials. - TB-500: 2.5 mg daily for 4 weeks + 2 mg 2x/week for 2 weeks + 1.5 mg 2x/week for 2 weeks = ~84 mg total. Requires nine 10 mg vials.
Factor in 10-15% waste from dead volume in syringes (the last 10-15 units in any vial cannot be reliably drawn). Order one extra vial per compound to account for this.
For reconstitution volumes and exact unit calculations, use our peptide reconstitution calculator.
Common Dosing Mistakes
Mistake 1: Using a 1:1 dose ratio for BPC-157 and TB-500. A user injects 500 mcg of each peptide daily. Standard protocols call for roughly 5x more TB-500 than BPC-157 by weight (2,500 mcg TB-500 vs 500 mcg BPC-157). At 1:1 dosing, TB-500 is severely underdosed. The fix: follow the standard ratio of 250-500 mcg BPC-157 to 2,000-2,500 mcg TB-500.
Mistake 2: Injecting TB-500 at the injury site when it works systemically. A user injects TB-500 directly into a sore knee, getting only local concentration when the peptide distributes systemically regardless of injection location. BPC-157 benefits from local injection; TB-500 does not. The fix: inject TB-500 in the abdomen or thigh for easy access and rotate sites. Direct BPC-157 near the injury.
Mistake 3: Using the same reconstitution volume for separate vials of different sizes. A user adds 2 mL of bacteriostatic water to both a 5 mg BPC-157 vial and a 5 mg TB-500 vial, then draws 10 units from each (250 mcg BPC-157, 250 mcg TB-500). They are underdosing TB-500 by 10x. The fix: calculate each vial's concentration separately and draw the correct volume for each target dose.
Mistake 4: Skipping the loading phase and starting at maintenance doses. A user injects 250 mcg BPC-157 and 1.5 mg TB-500 twice weekly from day one. Tissue saturation takes longer at these reduced doses, delaying the onset of noticeable effects by 2-3 weeks. The fix: run 2 weeks at full daily dosing before stepping down to maintenance frequency.
Safety Considerations
No human clinical trial has tested BPC-157 and TB-500 in combination. All dosing protocols are derived from individual peptide animal research, pharmacological extrapolation, and community reports.
BPC-157 safety profile: no lethal dose identified in animal studies. No organ toxicity, mutagenicity, or reproductive toxicity in preclinical testing (Sikiric et al., Gut Liver, 2020). The 2025 human IV pilot (20 mg single dose) reported no adverse events (Altern Ther Health Med, 2025).
TB-500 safety profile: Thymosin Beta-4 was tested in Phase I/II human trials for chronic wounds (injection) and dry eye (topical). Phase I trials administered 42-1,260 mg over 14 days with no dose-limiting toxicity. Rare cases of hypersensitivity reactions including anaphylaxis have been reported with TB-500 injections.
Angiogenesis caution: both BPC-157 and TB-500 promote new blood vessel formation. Users with a history of cancer or active tumors should avoid this stack. The theoretical risk of feeding blood supply to tumors exists with any angiogenesis-promoting protocol. Consult an oncologist before using either peptide if cancer history is present. Pre-screening is recommended before starting.
For a complete safety overview, see our BPC-157 TB-500 side effects guide. Neither peptide is FDA-approved for human use. BPC-157 is classified as a category 2 risk compound for injectable forms.
Frequently Asked Questions
What is the standard BPC-157 + TB-500 dosage?
The standard combined protocol is 250-500 mcg BPC-157 plus 2-2.5 mg TB-500, both injected subcutaneously once daily during the loading phase (weeks 1-2). Maintenance reduces to 250 mcg BPC-157 daily and 1.5-2 mg TB-500 two to three times per week for 4-6 weeks. Total cycle length is 4-8 weeks with a 2-4 week washout. These doses derive from individual peptide research, not combination studies.
How do I reconstitute separate BPC-157 and TB-500 vials?
Add 2 mL bacteriostatic water to a 5 mg BPC-157 vial (concentration: 2,500 mcg/mL). Add 2 mL to a 5 mg TB-500 vial (same concentration). For 500 mcg BPC-157, draw 20 units. For 2,500 mcg TB-500, draw 100 units (1 mL). Never mix the two reconstituted peptides in the same syringe. Use our peptide reconstitution calculator for exact volumes.
Can I mix BPC-157 and TB-500 in the same syringe?
Mixing two reconstituted peptides in one syringe is not recommended. No stability data exists for the liquid combination, and cross-contamination between vials introduces infection risk. Draw each peptide into its own syringe from its own vial. Some vendors sell pre-blended lyophilized vials where both peptides are already combined before reconstitution. These are acceptable if stored per instructions.
Should I inject BPC-157 and TB-500 at the same site?
Inject BPC-157 subcutaneously near the injury site for maximum local concentration. Inject TB-500 at a standard site (abdomen, thigh, or deltoid) since it works systemically regardless of injection location. Separating sites avoids excessive local volume and ensures each peptide distributes optimally. Space the two injections at least 2 inches apart if injecting in the same general area.
How long does the BPC-157 + TB-500 stack take to work?
Users typically report initial improvement within 1-2 weeks of daily injectable dosing. Significant changes in pain, mobility, or tissue healing become apparent by weeks 3-4. Oral capsule protocols are slower: expect 2-4 weeks for noticeable effects. Complete recovery of the target injury may take 6-12 weeks. Individual response varies with injury severity, age, and baseline health.
What is the wolverine stack dosage for a 200 lb male?
A 200 lb (91 kg) male falls in the 80-100 kg bracket. Recommended loading dose: 500 mcg BPC-157 once daily plus 2.5 mg TB-500 once daily for 2 weeks. Maintenance: 500 mcg BPC-157 daily plus 2 mg TB-500 two to three times per week for 4-6 weeks. Total 8-week cycle consumption: approximately 24.5 mg BPC-157 and 58 mg TB-500.
Is the oral or injectable dosage protocol better?
Injectable delivers both peptides at 80-95% bioavailability and is the more evidence-supported route for musculoskeletal injuries. Oral BPC-157 is effective for GI healing but delivers only 3% systemically (acetate) or up to 90% (arginate). Oral TB-500 lacks bioavailability data. For gut healing, oral BPC-157 is optimal. Combination (oral BPC-157 AM, injectable TB-500 PM) covers both targets. See our BPC-157 TB-500 capsules guide.
How many vials do I need for an 8-week standard cycle?
Standard protocol at 500 mcg BPC-157 daily for 4 weeks then tapering requires approximately four 5 mg vials of BPC-157. TB-500 at 2.5 mg daily for 2 weeks then 2 mg 3x/week for 4 weeks then tapering requires approximately ten 5 mg vials. Add 10-15% for dead volume waste. A 10 mg blend vial format reduces the vial count but limits dose flexibility.
The Bottom Line
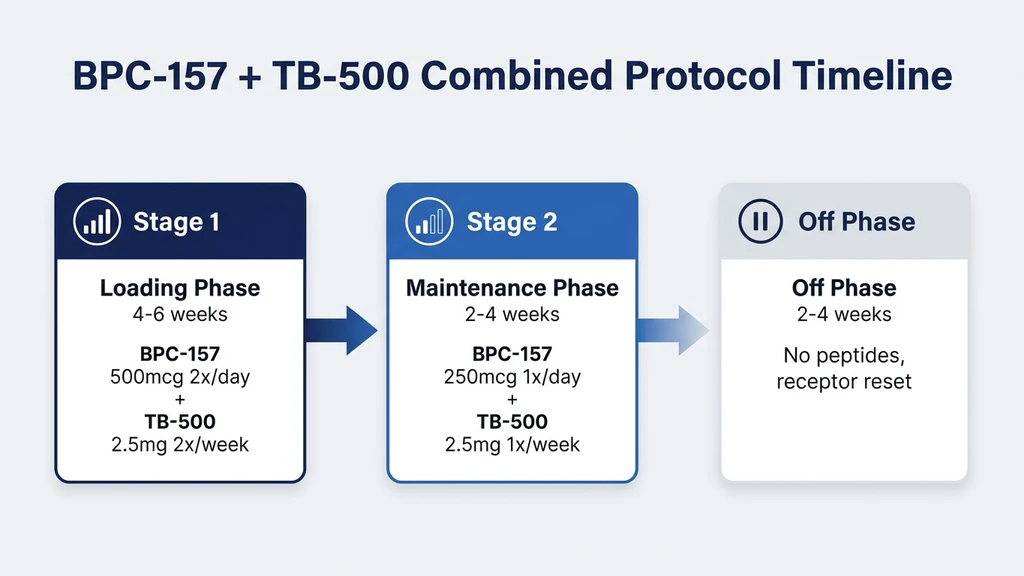
The BPC-157 + TB-500 combination protocol follows a structured approach: load at higher daily doses for 2 weeks, maintain at standard doses for 4-6 weeks, taper, then rest for 2-4 weeks. Standard injectable dosing is 250-500 mcg BPC-157 plus 2-2.5 mg TB-500 daily, adjusted by body weight and injury type. Oral protocols use higher capsule doses to compensate for lower bioavailability.
The critical dosing principle: BPC-157 benefits from local injection near the injury site, while TB-500 works systemically from any injection location. Getting this distinction wrong is the most common protocol error. Blend vial ratio matters too: a 1:5 BPC-157:TB-500 ratio matches standard dosing better than a 1:1 blend.
Calculate your exact protocol with the BPC-157 dosage calculator and TB-500 dosage calculator. For capsule-specific protocols, see our BPC-157 + TB-500 capsules guide. Review the BPC-157 + TB-500 side effects guide before starting, and see our peptide stacking guide for additional combination strategies.
Related Articles
GHK-Cu Dosage: Protocols & Charts
GHK-Cu dosage guide with injection protocols by goal (skin, hair, healing), reconstitution steps, dosage charts, side effects, and before/after timeline.
How to Take BPC-157: Dosage and Timing
How to take BPC-157: inject 250-500 mcg subcutaneously near the injury once daily for 4-8 weeks. Reconstitution, dosing, and cycle length.
BPC-157 Dosage for 200lb Male
BPC-157 dosage for a 200lb male is 250-500mcg/day. Peptide dosing is not weight-dependent. Protocols, reconstitution math, cycle length, and stacking options.
GHK-Cu + BPC-157 + TB-500 Blend Dosage
GHK-Cu + BPC-157 + TB-500 blend dosage chart for 70 mg and 42 mg vials. Per-injection breakdown in mcg, reconstitution steps, and cycling protocol.