The weight-adjusted BPC-157 dose ranges from 1.6 to 10 mcg/kg body weight per day. For a 150 lb (68 kg) person, that translates to 109 to 680 mcg daily. For a 200 lb (91 kg) person: 146 to 910 mcg daily. In clinical practice, most providers prescribe a flat 250 to 500 mcg/day regardless of body weight, because BPC-157 acts through receptor-mediated signaling rather than plasma concentration.
| Quick Reference | Value |
|---|---|
| Weight-based range | 1.6 to 10 mcg/kg/day |
| Clinical practice dose | 250 to 500 mcg/day (flat) |
| Injection route | Subcutaneous, 1 to 2x daily |
| Oral route | 500 to 1,000 mcg/day |
| Cycle length | 4 to 8 weeks on, 2 to 4 weeks off |
| Standard vial size | 5 mg lyophilized powder |
This guide covers the weight-based formula, a complete dosage chart from 120 to 280 lbs, gender considerations, route-specific adjustments, and why the calculated dose and the prescribed dose are two different numbers. Use our BPC-157 dosage calculator for personalized calculations. For a broader overview of administration methods, see how to take BPC-157.
BPC-157 is not FDA-approved for any indication. No completed human clinical trial exists. All dosing data is extrapolated from animal studies. Consult a healthcare provider before using any peptide.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
How Does the Weight-Based Formula Work?
The weight-based BPC-157 dose comes from translating animal study doses to human equivalents. Every peptide researcher faces the same problem: rats received 10 mcg/kg in the lab, but a human is not a 300-gram rat. The conversion requires a specific mathematical method.
The Animal Study Basis: 10 mcg/kg
The standard BPC-157 dose in rodent studies is 10 mcg/kg body weight, administered intraperitoneally (directly into the abdominal cavity) once daily. This dose produced tendon healing, muscle repair, gut protection, and neuroprotective effects across dozens of published studies (Chang et al., Life Sci, 2011).
The dose range across all published BPC-157 animal studies spans 6 to 50 mcg/kg. Most studies cluster around 10 mcg/kg. A 2019 systematic review cataloged the dosing protocols across the literature and confirmed this range (Gwyer et al., Cell Tissue Res, 2019).
The intraperitoneal route used in animals achieves near-100% bioavailability. Humans use subcutaneous injection, which reaches approximately 90%. This difference matters when calculating equivalent doses.
Converting Animal Doses to Human Equivalent (BSA Method)
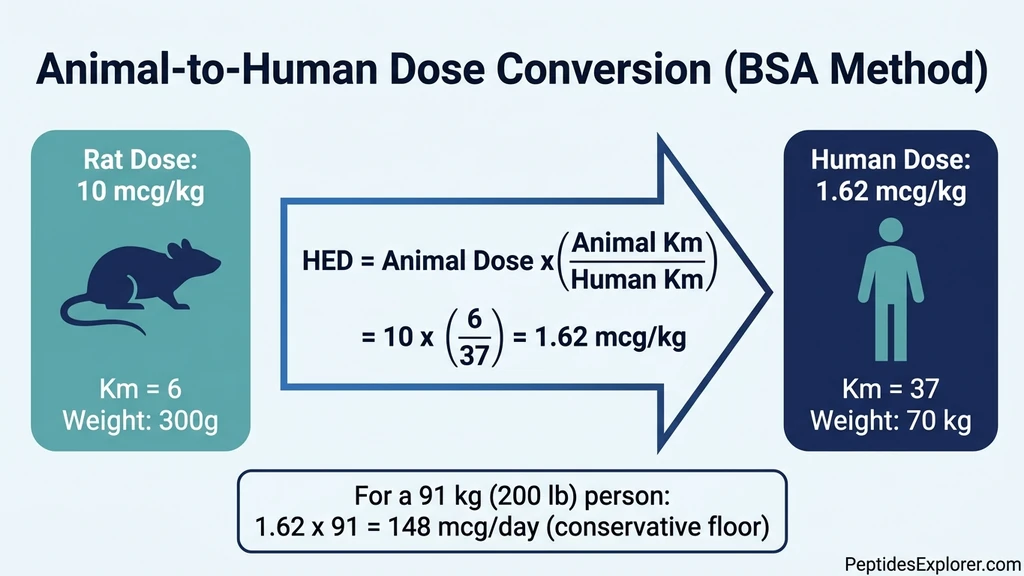
The FDA-recommended method for converting animal doses to human equivalent doses (HED) uses body surface area (BSA) normalization, not simple weight scaling. The formula was published by Reagan-Shaw et al. (FASEB J, 2008):
HED (mcg/kg) = Animal dose (mcg/kg) x (Animal Km / Human Km)
The Km factor accounts for metabolic rate differences between species. For rats, Km = 6. For humans, Km = 37.
Calculation: 10 mcg/kg x (6 / 37) = 1.62 mcg/kg human equivalent dose.
For a 91 kg (200 lb) human: 1.62 x 91 = approximately 148 mcg/day. This is the conservative floor, the minimum dose expected to produce biological activity based on the animal data. For a dedicated breakdown at this weight, see our BPC-157 dosage guide for a 200 lb male.
Why Community Doses Run Higher Than the Calculated HED
The BSA-converted minimum (1.6 mcg/kg) gives a conservative starting point. The standard community dose of 250 to 500 mcg/day runs 2 to 4 times above this floor. Three factors explain the gap.
First, bioavailability. Rat studies use intraperitoneal injection (near 100% absorption). Subcutaneous injection in humans reaches approximately 90%. The slight reduction justifies a modest upward adjustment.
Second, safety margin. BPC-157 shows no toxicity even at doses far exceeding the therapeutic range in animal models. The 2025 human safety pilot administered 10 to 20 mg intravenously (40 to 80 times the typical subcutaneous dose) with no adverse effects (Staresinic et al., Altern Ther Health Med, 2025). This wide therapeutic window allows practitioners to dose above the minimum without safety concerns.
Third, the threshold activation model. BPC-157 works by triggering receptor pathways (FAK-paxillin, VEGF, FGF, NO system), not by maintaining a specific plasma concentration (Seiwerth et al., Curr Pharm Des, 2018). Dosing above the threshold ensures consistent receptor activation even with individual absorption variability.
Full Weight-Based Dosage Chart (120 to 280 lbs)
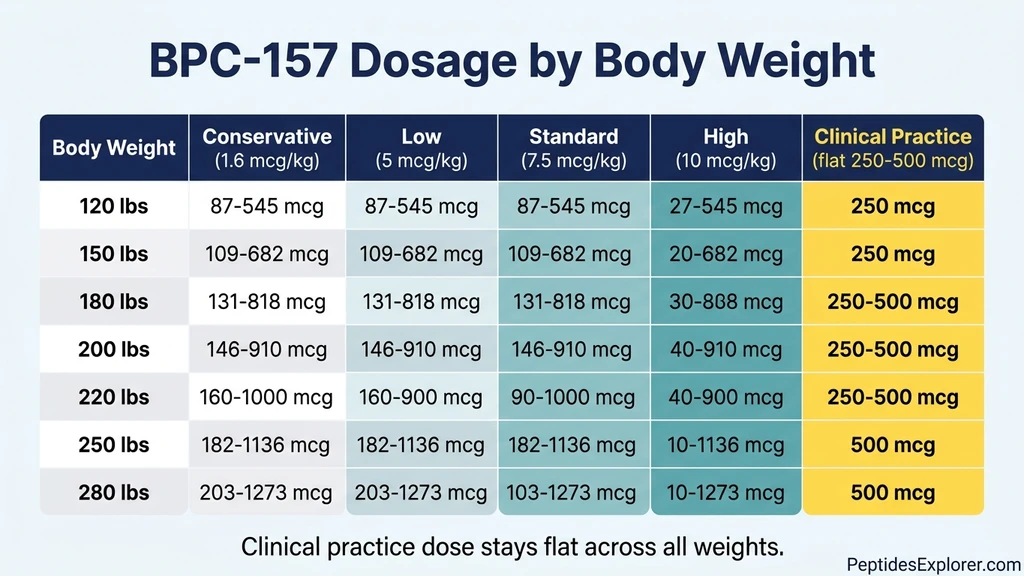
The table below covers every 10 lb increment. Five dose columns reflect different calculation methods. The "Clinical Practice" column shows what peptide therapy providers actually prescribe.
| Body Weight (lbs) | Weight (kg) | Conservative (1.6 mcg/kg) | Low (5 mcg/kg) | Standard (7.5 mcg/kg) | High (10 mcg/kg) | Clinical Practice |
|---|---|---|---|---|---|---|
| 120 | 54 | 87 mcg | 272 mcg | 409 mcg | 545 mcg | 250 mcg |
| 130 | 59 | 95 mcg | 295 mcg | 443 mcg | 590 mcg | 250 mcg |
| 140 | 64 | 102 mcg | 318 mcg | 477 mcg | 636 mcg | 250 mcg |
| 150 | 68 | 109 mcg | 341 mcg | 511 mcg | 682 mcg | 250 mcg |
| 160 | 73 | 116 mcg | 364 mcg | 545 mcg | 727 mcg | 250 mcg |
| 170 | 77 | 123 mcg | 386 mcg | 580 mcg | 773 mcg | 250 mcg |
| 180 | 82 | 131 mcg | 409 mcg | 614 mcg | 818 mcg | 250 to 500 mcg |
| 190 | 86 | 138 mcg | 432 mcg | 648 mcg | 864 mcg | 250 to 500 mcg |
| 200 | 91 | 146 mcg | 455 mcg | 682 mcg | 910 mcg | 250 to 500 mcg |
| 210 | 95 | 152 mcg | 477 mcg | 716 mcg | 955 mcg | 250 to 500 mcg |
| 220 | 100 | 160 mcg | 500 mcg | 750 mcg | 1,000 mcg | 250 to 500 mcg |
| 230 | 104 | 167 mcg | 523 mcg | 784 mcg | 1,045 mcg | 500 mcg |
| 240 | 109 | 175 mcg | 545 mcg | 818 mcg | 1,091 mcg | 500 mcg |
| 250 | 114 | 182 mcg | 568 mcg | 852 mcg | 1,136 mcg | 500 mcg |
| 260 | 118 | 189 mcg | 591 mcg | 886 mcg | 1,182 mcg | 500 mcg |
| 270 | 123 | 196 mcg | 614 mcg | 920 mcg | 1,227 mcg | 500 mcg |
| 280 | 127 | 203 mcg | 636 mcg | 955 mcg | 1,273 mcg | 500 mcg |
Notice the Clinical Practice column. It stays flat at 250 to 500 mcg across the entire weight range. This is the key insight: the weight-based calculation provides a theoretical framework, but real-world prescribing does not scale linearly with body mass.
How to Read This Chart
Conservative (1.6 mcg/kg): The human equivalent dose calculated from the BSA method. This is the mathematical floor derived from the standard rat dose of 10 mcg/kg.
Low (5 mcg/kg): A direct mcg/kg extrapolation at the lower end of the animal study range. Falls within the community standard for most body weights.
Standard (7.5 mcg/kg): The midpoint of the commonly cited animal dose range. For a 170 lb person, this yields 580 mcg, slightly above the typical 500 mcg clinical dose.
High (10 mcg/kg): The full animal study dose applied to human body weight without BSA conversion. Used by some practitioners for severe injuries or post-surgical recovery.
Clinical Practice: What peptide therapy providers actually prescribe. The convergence zone (250 to 500 mcg) sits at the low-to-standard range for medium-weight individuals. For BPC-157 benefits across different conditions, the clinical dose appears sufficient regardless of body weight.
Does BPC-157 Dosage Differ for Women vs Men?
No published evidence supports gender-specific BPC-157 dosing. The only pharmacokinetic study available, conducted in dogs, found no significant difference in plasma BPC-157 concentration between males and females (Zhang et al., Front Pharmacol, 2022).
What the Research Shows About Gender
The Zhang et al. pharmacokinetic study administered BPC-157 intravenously and subcutaneously to male and female beagle dogs. Plasma concentration curves overlapped. Clearance rates, half-life, and area under the curve (AUC) showed no statistically significant gender difference.
No human pharmacokinetic study exists for BPC-157 in either sex. Body composition differences (women typically carry higher body fat percentage) could theoretically affect subcutaneous absorption rates, but no data supports adjusting the dose based on this. For more on BPC-157 in female physiology, see BPC-157 benefits for women.
Practical Dosing by Gender
| Gender | Typical Weight Range | Starting Dose | Standard Dose |
|---|---|---|---|
| Women | 120 to 160 lbs | 250 mcg/day | 250 mcg/day |
| Men | 160 to 240 lbs | 250 mcg/day | 250 to 500 mcg/day |
| Overlap range | 160 to 180 lbs | 250 mcg/day | 250 mcg/day |
The overlap range (160 to 180 lbs) uses identical dosing for both genders. The slight upward adjustment to 500 mcg for heavier men reflects the general clinical practice pattern, not gender-specific pharmacology. Hormonal cycle phase does not appear to affect BPC-157 metabolism based on available data, though no human study has directly tested this.
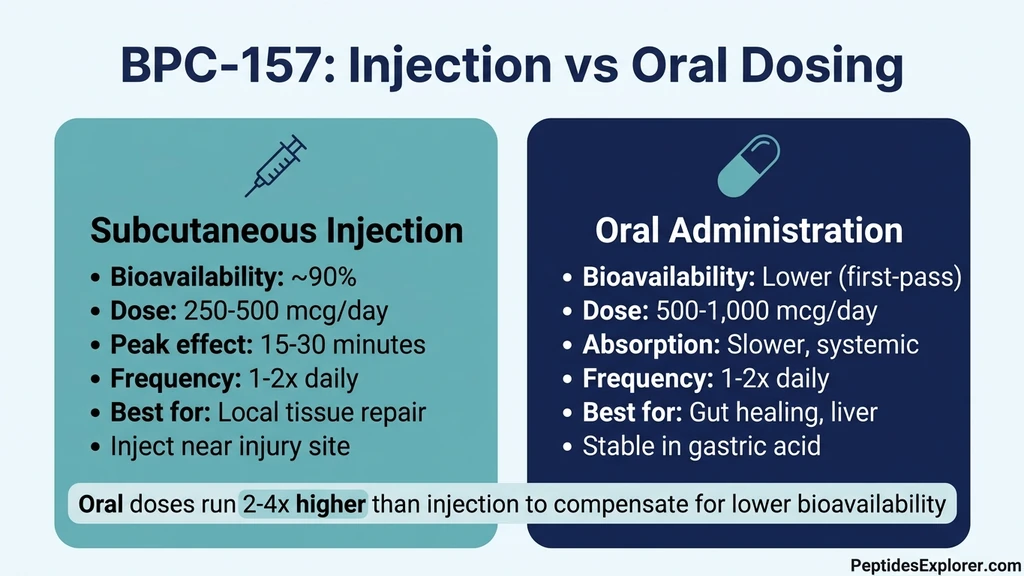
Injection vs Oral: Weight-Based Dose Adjustments
The route of administration changes how much BPC-157 reaches systemic circulation. Injection and oral dosing require separate weight-based calculations. For a detailed comparison of both routes, see BPC-157 oral vs injection.
Subcutaneous Injection Dosing by Weight
Subcutaneous injection delivers approximately 90% bioavailability. The weight chart above applies directly to this route. The standard protocol:
250 to 500 mcg injected subcutaneously once or twice daily. Inject near the injury site for local tissue repair, or in the abdomen for systemic effects. For injection site guidance, see where to inject BPC-157 and how to inject BPC-157.
Peak plasma concentration occurs within 15 to 30 minutes. The half-life is under 30 minutes, which is why some protocols call for twice-daily dosing during acute recovery phases.
Oral Dosing by Weight
BPC-157 is uniquely stable in gastric acid, unlike most peptides that degrade in the stomach within minutes. Animal studies used oral doses of 10 to 200 mcg/kg with demonstrated efficacy for gut healing, liver protection, and systemic effects (Sikiric et al., Curr Pharm Des, 2018).
Oral bioavailability is lower than injection due to first-pass metabolism. Community oral doses run higher to compensate:
| Body Weight (lbs) | Oral Dose (Gut Healing) | Oral Dose (Systemic) |
|---|---|---|
| 120 to 150 | 500 mcg/day | 500 to 750 mcg/day |
| 150 to 200 | 500 to 750 mcg/day | 750 to 1,000 mcg/day |
| 200 to 250 | 750 to 1,000 mcg/day | 1,000 mcg/day |
| 250+ | 1,000 mcg/day | 1,000 mcg 2x/day |
Oral dosing shows more weight sensitivity than injection. A larger body means greater volume of distribution, diluting the peptide that survives first-pass metabolism. The slight upward adjustment for heavier individuals is more justified here than for subcutaneous injection.
Both the arginate and acetate salt forms are available for oral use. Arginate may offer marginally better gastric stability.
Dose by Condition and Body Weight
Different injuries and conditions call for different dose intensities. The table below combines condition severity with body weight for practical protocol selection.
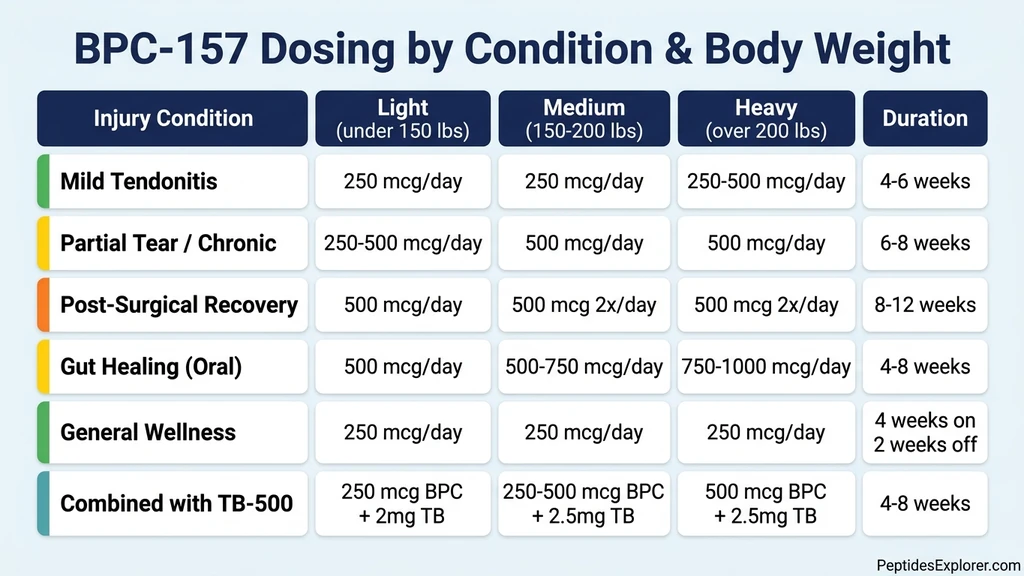
| Condition | Light (<150 lbs) | Medium (150 to 200 lbs) | Heavy (>200 lbs) | Duration |
|---|---|---|---|---|
| Mild tendonitis | 250 mcg/day | 250 mcg/day | 250 to 500 mcg/day | 4 to 6 weeks |
| Partial tear or chronic injury | 250 to 500 mcg/day | 500 mcg/day | 500 mcg/day | 6 to 8 weeks |
| Post-surgical recovery | 500 mcg/day | 500 mcg 2x/day | 500 mcg 2x/day | 8 to 12 weeks |
| Gut healing (oral) | 500 mcg/day | 500 to 750 mcg/day | 750 to 1,000 mcg/day | 4 to 8 weeks |
| General recovery and wellness | 250 mcg/day | 250 mcg/day | 250 mcg/day | 4 weeks on, 2 off |
| Combined with TB-500 | 250 mcg BPC + 2 mg TB | 250 to 500 mcg BPC + 2.5 mg TB | 500 mcg BPC + 2.5 mg TB | 4 to 8 weeks |
For the combined BPC-157 + TB-500 protocol (sometimes called the Wolverine Stack), see our detailed BPC-157 and TB-500 dosage guide. For the full comparison of these two healing peptides, see BPC-157 vs TB-500.
The pattern is consistent: body weight influences the dose mildly for injection and more noticeably for oral administration. Condition severity has a larger impact than body weight on dose selection.
Why Do Most Practitioners Use Flat Dosing?
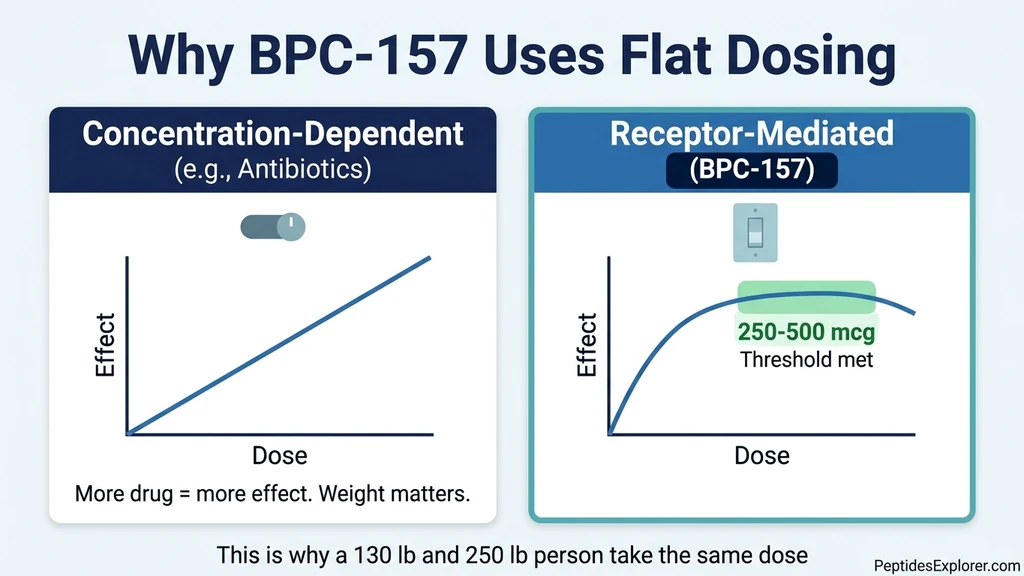
If a weight-based formula exists, why do most peptide therapy providers prescribe 250 to 500 mcg for everyone? The answer lies in how BPC-157 works at the molecular level.
Receptor-Mediated vs Concentration-Dependent Drugs
Think of a light switch. Flipping it activates the circuit. Pushing harder does not make the light brighter. BPC-157 works like that switch. It binds to FAK-paxillin pathway components, upregulates VEGF and FGF receptors, and modulates the nitric oxide system (Seiwerth et al., Curr Pharm Des, 2018). Once the receptor is activated, additional peptide molecules do not amplify the signal.
This distinguishes BPC-157 from drugs like antibiotics or anesthetics, where higher body weight genuinely requires higher doses to maintain effective plasma concentration. Those drugs work through concentration-dependent mechanisms. BPC-157 works through threshold activation. Once the threshold is met, more peptide does not equal more healing.
The Bell-Curve Dose Response
Some animal models show reduced efficacy at very high BPC-157 doses. The dose-response curve forms an inverted U: efficacy rises with dose, peaks, then declines. This has been observed across several of Sikiric's published studies.
This pattern argues against aggressive weight-based scaling for heavy individuals. A 280 lb person taking 1,273 mcg (the "high" column) may not heal faster than one taking 500 mcg. They may actually see diminished returns. The flat clinical dose of 250 to 500 mcg sits squarely at the peak of the dose-response curve for most people.
The 2025 Human Safety Pilot
The only published human BPC-157 data comes from Staresinic et al. (2025). Two adult participants received 10 mg and 20 mg intravenously. These doses are 40 to 80 times the typical 250 mcg subcutaneous dose. Dosing was flat, not weight-adjusted (Staresinic et al., Altern Ther Health Med, 2025).
No adverse effects were observed. Plasma cleared within 24 hours. While two participants cannot establish safety in any rigorous sense, the study confirms the extraordinarily wide therapeutic window and the precedent for flat dosing in human use.
For a broader perspective on peptide safety, see our peptide safety guide.
How to Calculate Your Exact Injection Volume
Knowing your dose in micrograms is only half the equation. You need to convert that number into units on an insulin syringe. The conversion depends on how you reconstitute the vial. Use our peptide reconstitution calculator for instant results, or follow the math below.
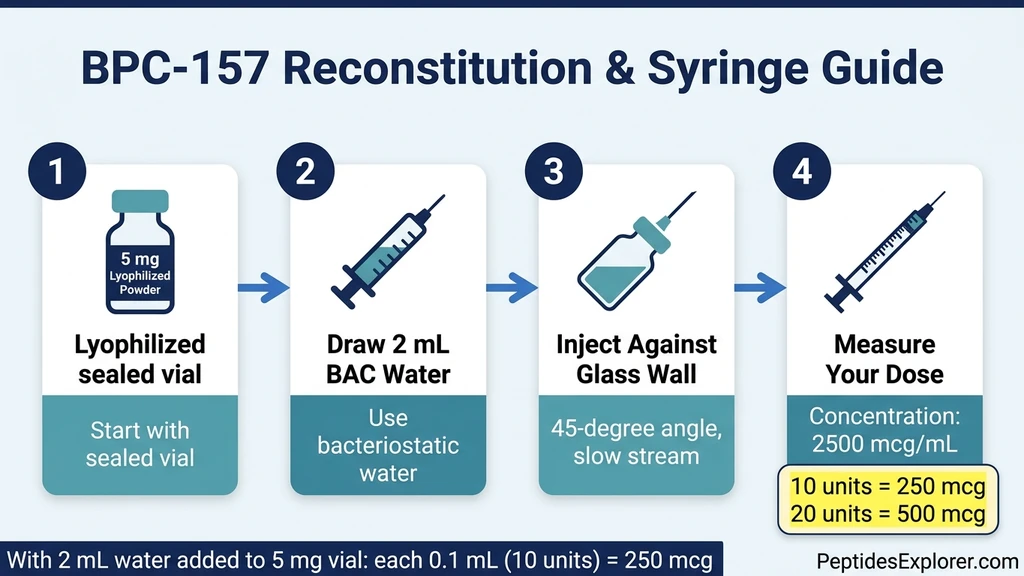
Reconstitution Table (5 mg Vial)
| Bacteriostatic Water Added | Concentration | Volume for 250 mcg | Volume for 500 mcg |
|---|---|---|---|
| 1 mL | 5,000 mcg/mL | 5 units (0.05 mL) | 10 units (0.10 mL) |
| 2 mL | 2,500 mcg/mL | 10 units (0.10 mL) | 20 units (0.20 mL) |
| 3 mL | 1,667 mcg/mL | 15 units (0.15 mL) | 30 units (0.30 mL) |
Adding more water makes each unit contain less peptide. This gives you finer dose control but uses the vial faster. Most users add 2 mL for the best balance of precision and vial longevity.
Worked Example: 170 lb Person, Low Dose (5 mcg/kg)
Step 1: Convert weight. 170 lbs / 2.2 = 77 kg.
Step 2: Calculate dose. 77 kg x 5 mcg/kg = 385 mcg.
Step 3: Choose reconstitution. 5 mg vial + 2 mL bacteriostatic water = 2,500 mcg/mL.
Step 4: Calculate volume. 385 mcg / 2,500 mcg/mL = 0.154 mL = approximately 15 units on an insulin syringe.
Step 5: Round practically. Draw to the 15-unit mark. The actual dose is 375 mcg, close enough to the target 385 mcg. Rounding to the nearest 5 units avoids the dosing errors that come from trying to eyeball fractional markings.
For automated calculations, plug your numbers into the BPC-157 dosage calculator.
Frequently Asked Questions
Does BPC-157 dosage change with body weight?
The weight-adjusted calculation (1.6 to 10 mcg/kg) provides a theoretical range, but clinical practice uses flat dosing of 250 to 500 mcg/day for all adults. BPC-157 works through receptor signaling, not plasma concentration, so body weight has minimal impact on efficacy. See our BPC-157 dosage calculator for personalized calculations.
How much BPC-157 should a 150 lb person take?
250 mcg/day subcutaneously. The weight-based calculation gives 109 to 680 mcg/day for a 150 lb (68 kg) person, and the standard clinical dose of 250 mcg falls within that range. For injuries requiring more aggressive treatment, 500 mcg/day is the typical ceiling. See our complete how to take BPC-157 guide for administration details.
Is the BPC-157 dose different for men and women?
No published evidence supports gender-specific dosing. A 2022 pharmacokinetic study in dogs found no significant difference in BPC-157 plasma concentration between males and females (Zhang et al., Front Pharmacol, 2022). Both men and women typically use 250 to 500 mcg/day. For more on female-specific considerations, see BPC-157 benefits for women.
How do you convert a rat BPC-157 dose to a human dose?
Using the FDA body surface area (BSA) method from Reagan-Shaw et al. (FASEB J, 2008): divide the rat dose (mcg/kg) by 6.2. A rat dose of 10 mcg/kg converts to approximately 1.6 mcg/kg in humans, or about 114 mcg for a 70 kg adult. Community doses of 250 to 500 mcg run 2 to 4 times above this minimum.
Should heavier people take more BPC-157?
Not necessarily for injection. The receptor-mediated mechanism means 250 to 500 mcg activates the same biological pathways regardless of body mass. For oral dosing, some practitioners slightly increase the dose for individuals over 220 lbs because oral bioavailability is affected by volume of distribution. See the oral vs injection comparison for route-specific guidance.
What is the maximum safe BPC-157 dose?
No maximum has been established in humans. Animal studies showed no toxicity at doses far exceeding the therapeutic range. The 2025 human safety pilot administered up to 20 mg intravenously, which is 40 times the typical daily subcutaneous dose, with no adverse effects (Staresinic et al., 2025). For general safety considerations, see our peptide safety guide.
The Bottom Line
The weight-based BPC-157 formula gives you a reference framework. The animal-to-human conversion (1.6 mcg/kg) sets the floor. The direct mcg/kg extrapolation (5 to 10 mcg/kg) defines the range. Clinical practice collapses this range into a flat 250 to 500 mcg for nearly everyone, because BPC-157's receptor-mediated mechanism does not require weight-proportional dosing.
Use the full weight chart as a sanity check, not a prescription. If the chart says your calculated dose is 380 mcg but your provider prescribed 250 mcg, the provider is not underdosing you. They are working from the same clinical evidence that shows threshold activation, not linear dose-response.
For oral use, body weight matters more. Heavier individuals lose more peptide to first-pass metabolism and may benefit from the upper end of the oral range.
Calculate your exact dose with our BPC-157 dosage calculator. For stacking protocols, see the BPC-157 + TB-500 dosage guide. For the full reference across all peptides, see our peptide dosage chart. Explore all peptide profiles, calculators, and research tools at PeptidesExplorer.
Related Articles
BPC-157 Dosage for 200lb Male
BPC-157 dosage for a 200lb male is 250-500mcg/day. Peptide dosing is not weight-dependent. Protocols, reconstitution math, cycle length, and stacking options.
BPC-157 TB-500 Dosage: Combined Protocol
BPC-157 TB-500 dosage: 250-500 mcg BPC-157 + 2-2.5 mg TB-500 daily. Weight-adjusted charts, injury-type matrix, blend vial math, and cycle timing.
KPV Peptide Dosage Chart by Route
KPV peptide dosage is 200-500 mcg/day. Full chart for oral (gut/IBD), injectable, topical, and nasal routes, plus the KPV + BPC-157 gut stack. PubMed-cited.
How Much Sermorelin Per Day: Complete Dosage Guide
Sermorelin dosage: 200-500 mcg/day subcutaneous before bedtime. Starting dose, titration, gender-specific protocols, and IGF-1 monitoring.