You have a loaded syringe of BPC-157, a sore shoulder, and one question: where exactly do you stick the needle? Inject subcutaneously within 1 to 3 cm of the injured structure. For a rotator cuff, that means the anterior or lateral deltoid fat pad. For an Achilles tendon, lateral to the tendon 1 to 2 cm above the heel. For gut issues like IBS or gastric ulcers, oral BPC-157 or a subcutaneous abdominal injection delivers the peptide directly to the GI tract.
Local injection near the injury creates a concentrated dose at the tissue during the first 15 to 30 minutes of diffusion, before the peptide enters systemic circulation. Cerovecki et al. (2010) demonstrated in a rat MCL transection model that local BPC-157 administration improved ligament healing across functional, biomechanical, and histological measures. A 2025 systematic review of 36 studies confirmed BPC-157 improved structural and biomechanical outcomes in ligament, tendon, muscle, and bone injuries.
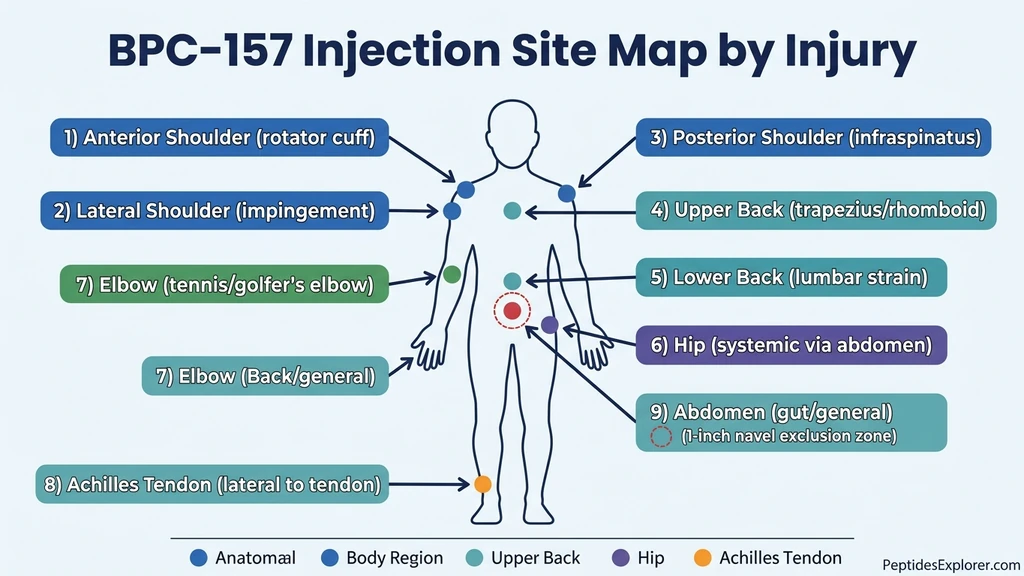
| Quick Reference: Injection Site by Injury | Primary Site | Route | Key Detail |
|---|---|---|---|
| Shoulder (rotator cuff, labrum) | Anterior/lateral deltoid fat pad | Subcutaneous | Rotate between 3 shoulder zones |
| Upper back (trapezius, rhomboid) | Subcutaneous over painful area | Subcutaneous | Pinch skin beside spine, not over it |
| Lower back (lumbar strain, disc pain) | Love handle area, lateral to spine | Subcutaneous | 2 to 4 cm from midline |
| Hip (bursitis, labral tear) | Lower abdomen (systemic) | Subcutaneous | Deep hip joint unreachable subcutaneously |
| Elbow (tennis/golfer's elbow) | 1 to 2 cm from lateral or medial epicondyle | Subcutaneous | Thin skin; use 31 gauge |
| Achilles tendon | Lateral to tendon, 1 to 2 cm above heel | Subcutaneous | Never inject into the tendon |
| Knee (ACL, MCL, meniscus) | Near joint line; see knee injection guide | Subcutaneous | Full guide covers all knee injuries |
| Gut (IBS, ulcers, colitis) | Lower abdomen or oral capsule | Subcutaneous or oral | Oral route preferred for GI conditions |
| General recovery / no specific injury | Lower abdomen, 2 inches from navel | Subcutaneous | Rotate quadrants daily |
For injection technique (needle gauge, angles, sterile protocol), see our how to inject BPC-157 guide. For dose calculations, use the BPC-157 dosage calculator. For a broader look at what BPC-157 does, read our BPC-157 benefits overview.
BPC-157 is not FDA-approved for any medical use. All information below reflects preclinical research and clinical practice observations. Consult a licensed healthcare provider before using any peptide.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
Why Injection Location Matters: Local vs. Systemic Delivery
Think of BPC-157 like a bucket of water and a house fire. Dump the bucket directly on the flames and the water hits where it matters. Toss it into a swimming pool connected to the same plumbing and a fraction reaches the fire. BPC-157 injected near an injury bathes the damaged tissue in a high peptide concentration during the first 15 to 30 minutes. Injected in the abdomen, that same dose dilutes across your entire bloodstream before a fraction arrives at the target.
The mechanism behind this local advantage involves VEGFR2 activation and nitric oxide signaling. BPC-157 upregulates VEGFR2 expression on vascular endothelial cells, promoting new blood vessel formation at the injection site through the Akt-eNOS pathway (Hsieh et al., 2017). Higher local concentration means more VEGFR2 activation, more angiogenesis, and faster healing.
Both routes work. Staresinic et al. (2006) showed that BPC-157 given intraperitoneally (systemic) still improved Achilles tendon-to-bone healing in rats. But local application consistently produced the strongest results in studies comparing both routes. Pevec et al. (2010) confirmed this pattern in a muscle and tendon healing model, finding that local BPC-157 produced superior angiogenic response compared to systemic delivery.
| Delivery Method | Best For | Advantage | Limitation |
|---|---|---|---|
| Local subcutaneous (near injury) | Accessible injuries: shoulder, elbow, Achilles, knee, back | High tissue concentration for 15 to 30 minutes | Requires identifying the correct anatomical site |
| Systemic subcutaneous (abdomen) | Deep injuries: hip joint, internal organs, general recovery | Easy technique, no anatomical knowledge needed | Lower peak concentration at injury |
| Oral (capsule or liquid) | Gut conditions: IBS, ulcers, colitis, leaky gut | Direct contact with GI mucosa | Minimal systemic absorption for musculoskeletal issues |
The practical rule: if you can pinch skin within 3 cm of the injury, inject locally. If the injury is too deep (hip socket, spinal disc), inject in the abdomen for systemic delivery. For gut conditions, oral administration puts the peptide exactly where it is needed. For safety fundamentals, see our peptide safety guide.
Shoulder Injection Sites
The shoulder is the most common BPC-157 injection target after the knee. Rotator cuff strains, labral tears, impingement syndrome, and biceps tendinopathy all respond to local subcutaneous delivery around the deltoid.
The shoulder has three practical injection zones, each targeting different structures. You rotate between these zones across your daily or twice-daily injections to prevent lipodystrophy (fat dimpling from repeated injection at one spot) and to distribute the peptide across the joint.
Anterior Shoulder (Front)
Target: supraspinatus tendon, biceps tendon, anterior labrum. This zone covers the front of the shoulder where most rotator cuff pain presents.
Find the bony point at the front tip of your shoulder (the anterior acromion). Move your fingers 2 to 3 cm below and slightly toward the chest. Pinch the skin and subcutaneous fat. Insert the needle at 45 degrees and deliver the dose. The anterior deltoid has adequate fat for subcutaneous injection in most people. If you are very lean (under 10% body fat), inject at a shallower angle (30 degrees) to stay in the fat layer.
Lateral Shoulder (Side)
Target: lateral supraspinatus, subacromial bursa, mid-deltoid. This zone covers impingement pain that flares when you raise your arm sideways.
Find the highest point of your shoulder (the lateral acromion). Move 3 cm directly downward along the outer arm. Pinch the lateral deltoid fat pad and inject at 45 degrees. This site has the most subcutaneous fat of the three shoulder zones, making it the easiest and least painful.
Posterior Shoulder (Back)
Target: infraspinatus, teres minor, posterior labrum. This zone covers the muscles responsible for external rotation and the back portion of the rotator cuff.
Reach across your chest and touch the bony ridge running along the back of your shoulder blade (the scapular spine). The injection site is 2 to 3 cm below this ridge, in the fleshy area over the infraspinatus muscle. This site is harder to reach alone. A partner helps. If self-injecting, use your opposite hand.
Shoulder rotation protocol: Anterior on day 1, lateral on day 2, posterior on day 3, then repeat. For twice-daily dosing, use two different zones per day (for example, anterior morning and lateral evening). This distributes healing factors across the entire shoulder capsule.
Upper and Lower Back Injection Sites
Back injuries present a unique challenge: the spine is off-limits for subcutaneous injection, and reaching behind yourself is awkward. The solution is straightforward. Inject into the fat lateral to the spine, not over the vertebrae.
Upper Back (Trapezius and Rhomboid Injuries)
Trapezius strains and rhomboid knots respond to subcutaneous injection in the upper back fat pad. Find the painful area. Move 3 to 4 cm laterally (toward the side of your body) away from the spine. Pinch the skin and inject at 45 degrees.
The upper back has variable fat thickness. Athletic individuals may have minimal subcutaneous tissue here. If you cannot pinch at least 1 cm of skin, inject in the lower abdomen instead for systemic delivery. Forcing a subcutaneous injection into an area with insufficient fat risks placing the needle into muscle, which changes absorption kinetics and increases bruising.
A partner makes upper back injections much easier. Self-injection is possible using your opposite hand reaching across the chest, but the angle is compromised.
Lower Back (Lumbar Strain, Disc-Related Pain)
Lower back pain from lumbar muscle strains, facet joint irritation, or disc-related nerve compression is the second most common musculoskeletal complaint worldwide. BPC-157 cannot reach a spinal disc through subcutaneous injection. The disc sits deep within the vertebral column, insulated by layers of muscle and bone. For disc-related pain, subcutaneous injection in the lower back provides systemic delivery with some local benefit to the surrounding paraspinal muscles.
Inject in the "love handle" area: 3 to 5 cm lateral to the spine, at the level of the pain. This region has generous subcutaneous fat in most people, making it an easy injection site. Rotate between left and right sides on alternating days. Perovic et al. (2019) demonstrated that BPC-157 improved spinal cord injury healing and functional recovery in rats, suggesting the peptide has neurotrophic properties relevant to spinal conditions.
For muscle strains in the erector spinae or quadratus lumborum, local injection in the love handle area puts the peptide within diffusion range of these muscles. Novinscak et al. (2008) showed BPC-157 accelerated muscle crush injury healing in rats when applied locally, restoring full function at all investigated time intervals.
Hip Injection Sites
The hip joint sits deep inside the pelvis, surrounded by thick layers of gluteal and iliac muscle. A standard subcutaneous needle (0.5 inch, 29 to 31 gauge) cannot reach it. This makes the hip the primary candidate for systemic delivery through abdominal injection.
For hip bursitis (trochanteric bursitis): The bursa sits on the outside of the hip, beneath the iliotibial band but above the greater trochanter. You can reach the overlying tissue with a subcutaneous injection. Lie on the opposite side. Find the bony prominence on the outer hip (greater trochanter). Inject subcutaneously 1 to 2 cm above or behind this point. There is moderate fat here in most individuals.
For labral tears and hip impingement: These structures sit inside the acetabulum. No subcutaneous approach reaches them. Inject in the lower abdomen using standard technique: pinch skin 2 inches lateral to the navel, insert at 45 degrees, deliver the dose. The peptide enters systemic circulation and reaches the hip through blood flow.
For hip flexor strains (iliopsoas): The iliopsoas runs deep through the pelvis. Subcutaneous injection in the lower abdominal crease (inguinal area) places the peptide near the superficial portion of the muscle. Pinch the skin at the crease where leg meets abdomen, 3 to 4 cm lateral to midline, and inject.
Krivic et al. (2008) showed BPC-157 improved muscle healing even when systemic corticosteroids impaired the process, indicating robust healing capacity through systemic delivery.
| Hip Condition | Injection Site | Can You Inject Locally? |
|---|---|---|
| Trochanteric bursitis | Outer hip, over greater trochanter | Yes, subcutaneous over the bursa |
| Labral tear | Lower abdomen (systemic) | No, too deep |
| Hip impingement (FAI) | Lower abdomen (systemic) | No, too deep |
| Hip flexor strain | Lower abdominal crease | Partially, near superficial portion |
| Gluteal tendinopathy | Upper outer buttock | Yes, subcutaneous over gluteal insertion |
| IT band syndrome | Lateral thigh, over tender area | Yes, subcutaneous along IT band |
Elbow Injection Sites
Tennis elbow (lateral epicondylitis) and golfer's elbow (medial epicondylitis) are among the most responsive conditions to local BPC-157 injection. The tendons attach superficially to bony prominences, placing them within easy reach of a subcutaneous needle.
Chang et al. (2011) demonstrated that BPC-157 promotes tendon fibroblast outgrowth, cell survival under oxidative stress, and cell migration through the FAK-paxillin signaling pathway. These effects are concentration-dependent: higher local levels mean more fibroblast activation. This makes local elbow injection particularly effective because the target tendons sit just millimeters beneath the skin.
Tennis Elbow (Lateral Epicondylitis)
Find the bony bump on the outside of your elbow (lateral epicondyle). The damaged tendon (extensor carpi radialis brevis) attaches here. Inject subcutaneously 1 to 2 cm below or behind the epicondyle, where you can pinch skin. Use a 31 gauge needle. The skin here is thin, and a finer needle reduces bruising.
Rotate between three points around the epicondyle across injections: directly below, slightly posterior (toward the back of the arm), and slightly anterior (toward the front). This distributes the peptide across the tendon's attachment zone.
Golfer's Elbow (Medial Epicondylitis)
The medial epicondyle is the bony bump on the inside of the elbow. The flexor-pronator tendon group attaches here. Inject 1 to 2 cm below the epicondyle on the inner forearm.
Caution: the ulnar nerve runs through a groove just behind the medial epicondyle. You know this nerve as the "funny bone." Inject below and slightly anterior to the epicondyle, not posterior. If you feel tingling or electrical sensation when positioning the needle, stop and reposition. You are too close to the nerve. Move 1 cm toward the front of the arm.
Achilles Tendon and Ankle Injection Sites
The Achilles tendon is the thickest tendon in the body, connecting the calf muscles to the heel bone. BPC-157 has strong preclinical evidence for Achilles healing. Staresinic et al. (2003) showed BPC-157 accelerated transected Achilles tendon healing in rats, increasing load to failure, improving functional index values, and promoting superior fibroblast and collagen formation compared to controls.
Where to inject: Lateral (outside) or medial (inside) to the Achilles tendon, 1 to 2 cm above the attachment at the heel bone (calcaneus). Pinch the skin beside the tendon and inject at 45 degrees.
Critical rule: never inject directly into the Achilles tendon. Intratendinous injection can weaken the collagen matrix and increase rupture risk. The subcutaneous tissue alongside the tendon provides adequate proximity for peptide diffusion.
For Achilles tendinopathy (mid-portion): Inject at the thickest, most tender point of the tendon, but lateral to it. Pinch the skin beside the swollen area and deliver the dose into the fat layer.
For insertional Achilles tendinopathy: The pain is at the heel bone where the tendon attaches. Inject 1 cm above the heel on the lateral or medial side. This area has minimal fat. Use a 31 gauge needle and a shallow angle (30 degrees) to stay subcutaneous.
For ankle sprains (lateral ligaments): Inject subcutaneously over the anterior talofibular ligament, located just below and in front of the lateral malleolus (the bony bump on the outside of the ankle). Pinch what skin is available and use a 31 gauge needle.
Staresinic et al. (2006) further demonstrated that BPC-157 promoted tendon-to-bone healing at the Achilles insertion and opposed the negative effects of corticosteroid use on healing.
Gut and GI Tract: Injection vs. Oral Administration
BPC-157 was discovered in human gastric juice. Its original research context was gastrointestinal healing. For gut conditions (IBS, gastric ulcers, colitis, leaky gut, NSAID-induced GI damage), you have two viable delivery routes: subcutaneous abdominal injection and oral administration.
Sikiric et al. (2011) reviewed decades of BPC-157 GI research and confirmed the peptide was effective when given intraperitoneally, orally, or locally for conditions across the entire gastrointestinal tract, from esophagus to colon. Sikiric et al. (2018) further showed BPC-157 treated colitis and ischemia-reperfusion injury in rats, rapidly restoring blood supply to damaged intestinal tissue.
Oral BPC-157 for Gut Conditions
Oral administration delivers the peptide directly to the GI mucosa. BPC-157 is stable in human gastric juice, meaning stomach acid does not destroy it. This is unusual for a peptide and is the reason oral dosing works.
For gastric ulcers, oral BPC-157 contacts the ulcerated mucosa directly. Xue et al. (2004) demonstrated significant protective effects against gastric ulcers in rats. BPC-157 has also reached Phase II clinical trials for inflammatory bowel disease (trial designations PL-10, PLD-116, PL14736) with a favorable safety profile (Sikiric et al., 2007).
Oral dosing protocol: 250 to 500 mcg taken on an empty stomach, held under the tongue for 60 to 90 seconds before swallowing. The sublingual absorption provides partial systemic uptake, while the swallowed portion contacts the gastric and intestinal lining directly. For detailed oral protocols, see how to take BPC-157. For oral-specific options, see BPC-157 oral pills or BPC-157 nasal spray guide.
Subcutaneous Abdominal Injection for Gut Healing
If you prefer injection, the lower abdomen is the site. Inject subcutaneously 2 to 3 inches lateral to the navel. The peptide enters systemic circulation and reaches the gut vasculature rapidly because the hepatic portal system drains abdominal tissue directly toward the liver and GI organs.
This route is preferable when the gut condition involves the lower intestine (Crohn's affecting the ileum, colonic inflammation) where an oral dose may not maintain adequate concentration through the full transit. Subcutaneous injection provides systemic levels that reach the entire GI tract evenly.
| Gut Condition | Preferred Route | Rationale |
|---|---|---|
| Gastric ulcer | Oral | Direct mucosal contact |
| Duodenal ulcer | Oral | Reaches duodenum within 30 to 60 minutes |
| IBS (mixed type) | Oral + subcutaneous (alternate) | Covers both local mucosal and systemic pathways |
| Ulcerative colitis | Subcutaneous (abdomen) | Oral dose may not survive full transit to colon |
| Crohn's disease (ileal) | Subcutaneous (abdomen) | Systemic delivery ensures ileal reach |
| NSAID-induced GI damage | Oral | Counteracts local mucosal damage directly |
| Leaky gut / intestinal permeability | Oral | Peptide contacts intestinal epithelium directly |
Sikiric et al. (2013) reviewed BPC-157's effects on ulcerative colitis models, confirming anti-inflammatory action, mucosal healing, and restoration of normal gut barrier function.
Wrist, Hand, and Forearm Injection Sites
Wrist and hand injuries (carpal tunnel-related tendinopathy, De Quervain's tenosynovitis, trigger finger) involve structures that sit close to the surface. The challenge is minimal subcutaneous fat. These areas demand the finest needle available (31 gauge) and a shallow injection angle.
De Quervain's tenosynovitis: The inflamed tendons run along the thumb side of the wrist. Inject subcutaneously on the dorsal (top) side of the wrist, 1 cm from the radial styloid (the bony bump at the base of the thumb side). Pinch gently. There is little fat, so use a 30 to 45 degree angle.
Carpal tunnel area: The carpal tunnel sits on the palmar (underside) of the wrist. Inject on the dorsal (top) side of the wrist, not the palmar side. The median nerve and flexor tendons run through the palmar wrist, and injecting there risks nerve irritation. Dorsal subcutaneous injection provides systemic delivery to the adjacent structures.
Trigger finger: Inject subcutaneously on the dorsal side of the affected finger's base (MCP joint area). The tendon sheath runs along the palmar side, but dorsal injection avoids the digital nerves and arteries. The peptide diffuses across the thin tissue to reach the inflamed sheath.
Forearm (pronator teres, flexor strain): Inject subcutaneously over the painful area on the inner forearm, midway between wrist and elbow. There is moderate fat here. Standard 29 to 30 gauge needle works.
Abdominal Injection for Systemic Delivery
When the injury is too deep to reach locally, when you are treating a systemic condition, or when you simply want the easiest injection site, the lower abdomen is the default.
The abdomen has the most consistent subcutaneous fat of any injection site. Even lean individuals retain a pinchable layer here. The absorption rate is predictable, and the site is easy to reach alone.
How to Inject in the Abdomen
Identify the injection zone: a band extending 2 to 4 inches on either side of the navel, avoiding the 1-inch radius directly around the navel itself (the periumbilical zone has inconsistent fat depth and more nerve endings).
Divide this area into four quadrants: upper left, upper right, lower left, lower right. Use one quadrant per injection and rotate clockwise. This prevents lipodystrophy and injection site fatigue.
Pinch a fold of skin and fat between your thumb and index finger. Insert the needle at 45 degrees into the base of the fold. Push the plunger slowly (3 to 5 seconds). Release the skin fold, withdraw the needle, and apply gentle pressure with an alcohol pad for 5 seconds. Do not rub.
When Systemic Beats Local
Systemic abdominal injection is not a compromise. For certain conditions, it is the better choice.
Multiple injuries in different body regions benefit from a single systemic injection rather than splitting the dose across several local sites. A 500 mcg dose injected in the abdomen reaches all tissues through circulation. Splitting that same dose into 125 mcg at four injury sites delivers a subtherapeutic local concentration at each one.
Post-surgical recovery, where the surgical site is bandaged or sutured, also favors systemic delivery. Injecting near a fresh surgical wound increases infection risk. Abdominal injection eliminates this concern while still delivering the peptide to the healing tissue through blood flow.
General anti-inflammatory and recovery support (athletes between competitions, post-workout recovery) does not target a single structure. Systemic delivery is the logical choice. For dosing specifics, use the BPC-157 dosage calculator. For comprehensive dosing charts, see our BPC-157 dosage chart.
Site Rotation Protocol
Injecting the same spot repeatedly causes three problems. First, lipodystrophy: the fat layer thins or hardens, creating visible dimples. Second, scar tissue formation in the subcutaneous layer, which reduces absorption over time. Third, increased pain as nerve endings in the area become sensitized.
The solution is systematic rotation. For any injection site (shoulder, knee, abdomen, back), define 3 to 4 sub-zones and cycle through them.
| Injection Target | Zone 1 | Zone 2 | Zone 3 | Zone 4 |
|---|---|---|---|---|
| Shoulder | Anterior deltoid | Lateral deltoid | Posterior deltoid | (repeat cycle) |
| Knee | Medial upper | Lateral upper | Medial lower | Lateral lower |
| Abdomen | Upper right | Lower right | Lower left | Upper left |
| Lower back | Right love handle | Left love handle | (alternate) | (alternate) |
| Elbow | Below epicondyle | Posterior to epicondyle | Anterior to epicondyle | (repeat cycle) |
| Achilles | Lateral, 2 cm above heel | Medial, 2 cm above heel | Lateral, midpoint | Medial, midpoint |
Minimum spacing rule: Allow at least 1 cm between today's injection and yesterday's injection within the same zone. If you can still see or feel the previous injection site (small bump, slight redness), move to the next zone in the rotation.
Timing and frequency: Most BPC-157 protocols call for once or twice daily injections over 4 to 6 weeks. At twice daily, you cycle through all zones in 2 days and return to the first zone on day 3, giving each site 48 hours of recovery. This spacing is sufficient to prevent lipodystrophy in protocols lasting up to 8 weeks.
Common Mistakes When Choosing Injection Sites
These four errors account for most site-selection problems with BPC-157.
Mistake 1: Injecting directly into tendons. Tendons are dense, avascular collagen bundles. Pushing a needle into a tendon is painful, damages the collagen matrix, and does not improve peptide delivery. Inject in the subcutaneous fat beside the tendon, within 1 to 3 cm. The peptide diffuses into the tendon through the paratenon and local vasculature.
Mistake 2: Choosing the wrong depth. Pushing a short insulin needle too deep in a lean area (knee, elbow, wrist) places the peptide intramuscularly instead of subcutaneously. Intramuscular injection is not harmful, but absorption kinetics change: faster peak, shorter duration. If you are lean, reduce the insertion angle to 30 degrees to keep the needle in the fat layer.
Mistake 3: Splitting doses across too many sites. Injecting 100 mcg at five different injury sites sounds logical but delivers a subtherapeutic concentration everywhere. Research doses in animal studies typically range from 10 mcg/kg applied locally at a single site. A 500 mcg dose at one site provides adequate local concentration. If you have two injuries, alternate sites across daily injections rather than splitting each dose.
Mistake 4: Ignoring the abdomen as a legitimate option. Some users fixate on local injection even when the target is unreachable (deep hip, spinal disc, internal organs). BPC-157 is systemically active. Sikiric et al. (2018) documented healing effects across tendons, ligaments, muscles, bone, and GI tissue from both local and systemic routes. Abdominal injection is not a consolation prize. For deep structures, it is the correct choice.
Combining BPC-157 with TB-500: Injection Site Strategy
Many users stack BPC-157 with TB-500 for enhanced healing. TB-500 (Thymosin Beta-4) promotes cell migration and reduces inflammation through different pathways than BPC-157. The two peptides complement each other.
For combined use, inject both peptides at the same general site but not in the exact same spot. Inject BPC-157 first, then move 1 to 2 cm away and inject TB-500. Alternatively, inject one in the morning and the other in the evening, rotating positions within the zone.
TB-500 is primarily systemic in its action. Unlike BPC-157, it does not show a strong local vs. systemic concentration advantage. This means TB-500 can be injected in the abdomen regardless of injury location, while BPC-157 goes near the injury. This split simplifies the protocol: BPC-157 local, TB-500 abdominal.
For detailed stacking protocols, see BPC-157 vs TB-500. For combined dosing, check our BPC-157 + TB-500 dosage guide. For side effect considerations, read BPC-157 + TB-500 side effects.
Frequently Asked Questions
Does it matter where you inject BPC-157?
Yes. Local injection within 1 to 3 cm of the injury creates a concentrated dose at the tissue during the first 15 to 30 minutes of diffusion. Cerovecki et al. (2010) demonstrated stronger ligament healing with local versus systemic BPC-157 in a rat MCL model. For injuries you cannot reach subcutaneously (deep hip, spinal disc), abdominal injection provides effective systemic delivery.
Where is the best place to inject BPC-157 for shoulder pain?
Inject subcutaneously in the anterior, lateral, or posterior deltoid fat pad, within 2 to 3 cm of the painful structure. For rotator cuff issues, the anterior and lateral zones cover the supraspinatus and biceps tendons. Rotate between all three zones across injections. Use a 29 to 30 gauge, 0.5-inch insulin syringe at 45 degrees.
Can you inject BPC-157 in the stomach area for all injuries?
Yes. Abdominal subcutaneous injection provides systemic delivery that reaches all tissues through blood circulation. It is less targeted than local injection, but it works for every condition. For deep structures like the hip joint or spinal disc, abdominal injection is the recommended approach because subcutaneous needles cannot reach those areas.
Should I inject BPC-157 near my Achilles tendon or in my stomach?
Near the Achilles tendon. Inject subcutaneously on the lateral or medial side of the tendon, 1 to 2 cm above the heel bone. Never inject into the tendon itself. Staresinic et al. (2003) showed BPC-157 accelerated transected Achilles healing in rats with local application, increasing load to failure and collagen formation.
Where do you inject BPC-157 for gut issues like IBS?
Oral administration is preferred for most GI conditions. BPC-157 is stable in gastric juice and contacts the intestinal mucosa directly. Take 250 to 500 mcg on an empty stomach. For lower bowel conditions (colitis, Crohn's), subcutaneous abdominal injection provides more consistent systemic levels throughout the entire GI tract.
How close to the injury should the BPC-157 injection be?
Within 1 to 3 cm. You do not need to inject directly at the injury. Subcutaneous injection creates a diffusion gradient, and the peptide spreads through local tissue over 15 to 30 minutes. Inject in the fat layer beside tendons, ligaments, or joints. Closer is better, but 3 cm still provides meaningful local concentration.
Can I inject BPC-157 in multiple sites at the same time?
You can, but splitting the dose reduces concentration at each site. A 500 mcg dose split across 4 sites delivers only 125 mcg per location, which may fall below the effective local threshold. If you have multiple injuries, alternate sites across daily injections: shoulder on day 1, elbow on day 2. Use the full dose at each site.
Where to inject BPC-157 for lower back pain?
Inject subcutaneously in the love handle area, 3 to 5 cm lateral to the spine at the level of the pain. This region has adequate fat in most people. Alternate between left and right sides daily. For disc-related pain, the peptide reaches the area through systemic circulation since spinal discs are too deep for subcutaneous delivery.
The Bottom Line
Inject BPC-157 subcutaneously within 1 to 3 cm of the injured structure for maximum local concentration. For accessible injuries (shoulder, elbow, Achilles, knee, back), local injection delivers the peptide directly to the healing tissue. For deep injuries (hip socket, spinal disc), abdominal injection provides systemic delivery that still reaches the target through circulation. For gut conditions, oral administration puts the peptide in direct contact with the GI mucosa.
Rotate between 3 to 4 sub-zones at each injection site across daily injections to prevent lipodystrophy and maintain consistent absorption. Never inject directly into tendons. Use a 29 to 31 gauge insulin syringe at 45 degrees. If you cannot pinch at least 1 cm of skin at the injection site, switch to an area with more subcutaneous fat or reduce the needle angle to 30 degrees.
Use the BPC-157 dosage calculator to determine the correct dose for your protocol. For step-by-step injection technique, see how to inject BPC-157. For knee-specific injection sites, see where to inject BPC-157 for knee pain. For a complete overview of what this peptide does, read our BPC-157 benefits guide. For safety fundamentals, see the peptide safety guide.
Related BPC-157 articles: - BPC-157 Dosage Chart - complete dosing reference by condition - BPC-157 vs TB-500 - choosing between or stacking healing peptides - BPC-157 Benefits for Women - female-specific considerations - BPC-157 Oral vs Injection - comparing delivery routes - BPC-157 Muscle Growth - hypertrophy and recovery applications - Does BPC-157 Cause High Blood Pressure? - cardiovascular safety - Peptides for Recovery - broader recovery peptide options - Peptides for Inflammation - anti-inflammatory peptide comparison
Explore all peptide profiles and tools at PeptidesExplorer.
Related Articles
How to Take BPC-157: Dosage and Timing
How to take BPC-157: inject 250-500 mcg subcutaneously near the injury once daily for 4-8 weeks. Reconstitution, dosing, and cycle length.
Where to Inject BPC-157 for Knee Pain
Exact injection sites for BPC-157 knee pain: subcutaneous locations by injury type, needle gauge, angles, and site rotation technique.
Where to Inject Sermorelin: Best Sites & Technique
Where to inject sermorelin for best results. Abdomen, thigh, and upper arm injection sites ranked, plus step-by-step subcutaneous technique and timing protocol.
How to Inject BPC-157: Sites & Guide
How to inject BPC-157 subcutaneously: step-by-step technique, injection site selection by injury, needle gauge, reconstitution, and sterile protocol.