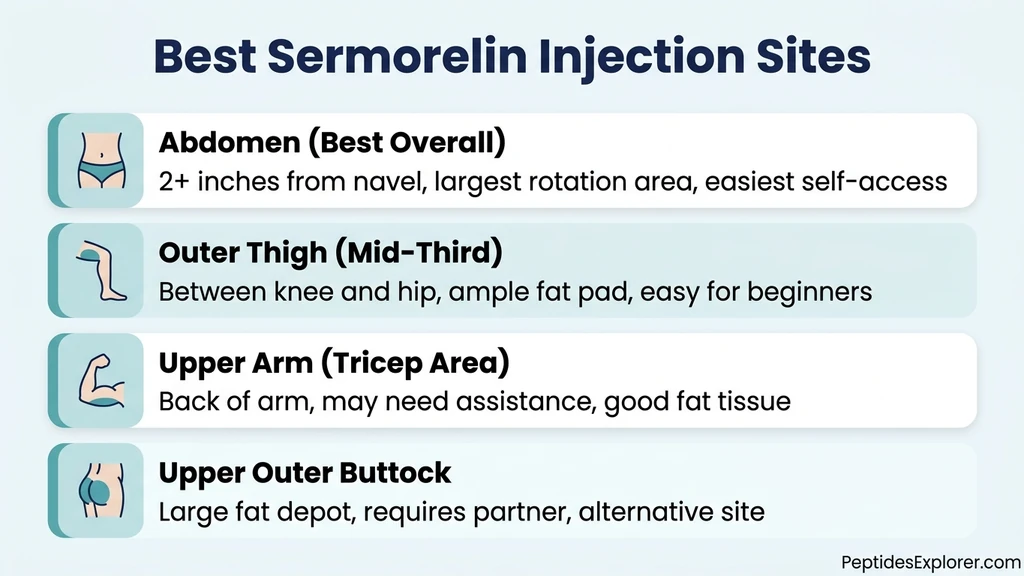
You reconstituted your vial of sermorelin, drew the dose into a syringe, and now you need to decide where to put the needle. Inject sermorelin subcutaneously into the abdominal fat pad, at least two inches from the navel. The abdomen provides the thickest fat layer, the largest rotation area, and the most consistent absorption of any self-accessible site. The front of the thigh and the back of the upper arm are solid alternatives.
Sermorelin (GRF 1-29) is a growth hormone-releasing hormone analog with a plasma half-life of just 10 to 20 minutes. It works by triggering a natural GH pulse from the pituitary, and that pulse peaks within 15 to 30 minutes of injection (Walker et al., 1994). Because the peptide clears so quickly, injection technique and timing matter more than they do for longer-acting compounds like CJC-1295. Injecting into the wrong tissue layer or at the wrong time of day can blunt the GH response you paid for.
| Quick Reference | Details |
|---|---|
| Best site | Abdomen (2+ inches from navel) |
| Alternative sites | Front/outer thigh, back of upper arm, upper outer buttock |
| Route | Subcutaneous (not intramuscular) |
| Needle gauge | 29 to 31 gauge, 0.5 inch |
| Injection angle | 45 degrees (or 90 degrees with short needle in adequate fat) |
| Timing | 30 to 60 minutes before bed, on an empty stomach |
| Typical dose | 100 to 300 mcg/day |
| Site rotation | Different spot every injection, never same location two nights in a row |
For dosing protocols and fat loss data, see sermorelin for fat loss. For general injection technique covering all peptides, see the peptide injections complete guide. If you are new to reconstituting peptides, use our peptide reconstitution calculator.
Sermorelin is not FDA-approved for adult use. It received FDA approval in 1997 (Geref Diagnostic) for diagnosing GH deficiency in children, but the manufacturer voluntarily withdrew it in 2008 for commercial reasons. All adult use is off-label. Consult a licensed healthcare provider before using any peptide.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
Why Injection Site Selection Matters for Sermorelin
Sermorelin must reach the bloodstream through subcutaneous fat to trigger GH release from the pituitary. Unlike BPC-157, which benefits from local injection near an injury, sermorelin works systemically. It travels through the bloodstream to the anterior pituitary regardless of where you inject it. The injection site affects absorption speed and comfort, not the target organ.
Subcutaneous injection deposits the peptide into the fat layer between the skin and the muscle fascia. From there, sermorelin absorbs into capillaries at a controlled rate. Intramuscular injection, by contrast, delivers the peptide into densely vascularized muscle tissue, causing faster absorption and a shorter, sharper peak. For a peptide with a 10 to 20 minute half-life, that difference can mean a less sustained GH pulse. A pharmacokinetic analysis of GHRH analogs confirmed that subcutaneous delivery produces a more physiological GH release pattern compared to intravenous or intramuscular routes (Sievertsen et al., 1991).
The second variable is fat pad thickness. Thicker fat means the needle stays in subcutaneous tissue rather than punching through into muscle. A 2014 ultrasound study measured subcutaneous thickness across common injection sites and found the abdomen averaged 1.5 to 3 cm, the thigh 0.5 to 2 cm, and the upper arm 0.5 to 1.5 cm (Gibney et al., Curr Med Res Opin, 2010). Leaner individuals have thinner fat pads and higher risk of accidental intramuscular injection, especially at the thigh and arm.
| Factor | Abdomen | Front/Outer Thigh | Back of Upper Arm | Upper Outer Buttock |
|---|---|---|---|---|
| Fat pad thickness | 1.5 to 3 cm | 0.5 to 2 cm | 0.5 to 1.5 cm | 1 to 3 cm |
| Self-access | Easy | Easy | Difficult | Difficult |
| Rotation area | Largest | Large | Small | Large |
| Risk of IM injection | Very low | Moderate in lean users | Moderate | Low |
| Pain level | Low | Low to moderate | Low | Low |
For a detailed comparison of injection sites across different peptides, see best injection sites for tirzepatide, which covers the same anatomical principles.
The Abdomen: Best Sermorelin Injection Site
The abdomen ranks first for sermorelin injection for three reasons: it has the thickest subcutaneous fat in most adults, it offers the largest rotation surface area, and you can reach it without a mirror or a partner. Most clinical protocols for GHRH analogs specify abdominal subcutaneous injection as the default site.
Exact Location and Boundaries
The usable injection zone forms a wide band below the ribs, above the hip bones, and at least two inches (5 cm) from the navel in every direction. Think of a picture frame around your belly button. Everything inside the frame is off-limits. Everything outside it, between the ribs and the hips, is fair territory.
Avoid the waistline where belts and waistbands create friction. Stay away from visible veins, stretch marks, moles, scars, and any area with redness from a previous injection. The area lateral to the navel (the flanks or "love handle" region) often has the deepest fat pad and is an excellent default spot.
Divide the usable zone into quadrants: upper left, upper right, lower left, lower right. Rotate through these quadrants across four consecutive injections. Within each quadrant, shift the exact puncture point by at least one inch each time. This gives you dozens of distinct injection locations before you return to any spot.
Why the Abdomen Ranks First
Subcutaneous fat in the periumbilical abdomen averages 2 to 3 cm in most adults, even in relatively lean individuals. This thickness provides a generous target for the needle, virtually eliminating the risk of accidental intramuscular injection with a standard 0.5-inch (12.7 mm) insulin needle. The abdomen also has rich capillary density in the subcutaneous layer, promoting reliable absorption.
The surface area advantage is significant for long-term protocols. Sermorelin is typically used daily for 12 to 16 weeks or longer. At one injection per night, you need at minimum 84 distinct sites over 12 weeks. The abdomen provides that easily. The thigh and upper arm, with their smaller zones, require more careful planning to avoid re-using spots.
For a deep dive into sermorelin cycling protocols, see is sermorelin safe.
Abdominal Injection Technique
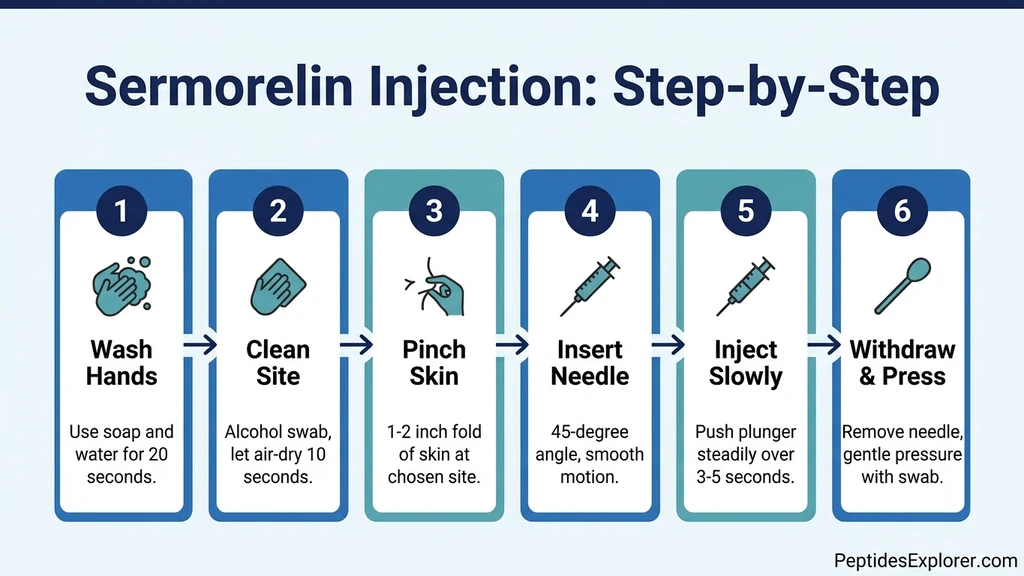
- 1.Wash your hands thoroughly with soap and water for at least 20 seconds.
- 2.Clean the injection site with an alcohol swab using a circular motion from center outward. Let the skin air-dry completely (about 10 seconds). Injecting through wet alcohol stings.
- 3.Pinch a 1 to 2 inch fold of skin between your thumb and index finger. This lifts the fat away from the muscle.
- 4.Insert the needle at a 45-degree angle in a smooth, swift motion. If using a short needle (5/16 inch or 8 mm) and you have adequate fat (can pinch 2+ inches), you can insert at 90 degrees.
- 5.Release the skin pinch gently once the needle is in place.
- 6.Push the plunger slowly and steadily over 3 to 5 seconds. Slow injection reduces stinging.
- 7.Withdraw the needle at the same angle you inserted it. Apply gentle pressure with a clean cotton ball or gauze for 5 to 10 seconds. Do not rub the site.
For a visual walkthrough of this technique applied across all peptides, see how to inject peptides.
Alternative Injection Sites
The abdomen is the default, but three alternative sites work well when you need to rest an abdominal area or simply prefer variety. Each has tradeoffs in accessibility and fat thickness.
Front and Outer Thigh
The injection zone covers the middle third of the front or outer thigh, between the knee and the hip. Stay at least four inches above the kneecap and four inches below the hip crease. The vastus lateralis muscle lies underneath, so adequate fat is essential to avoid intramuscular delivery.
Thigh injections are easy to self-administer. You can inject while sitting, which relaxes the muscle and makes the fat layer more accessible. The main limitation is fat thickness: lean individuals, particularly men with low body fat in the legs, may have only 0.5 cm of subcutaneous tissue here. If you cannot pinch at least one inch of skin and fat, use the abdomen instead.
Pinch a fold of skin on the outer thigh. Insert the needle at 45 degrees. Inject slowly and withdraw. The outer thigh tends to bruise slightly more than the abdomen because the skin is thinner and there are more superficial capillaries. This is cosmetic, not harmful.
Back of the Upper Arm
The tricep area on the back of the upper arm has adequate subcutaneous fat in most adults, particularly women. The injection zone is the fleshy area between the shoulder and the elbow, roughly halfway up the back of the arm.
The challenge is self-access. Injecting into your own upper arm requires reaching across with the opposite hand while holding a syringe, which is awkward and compromises your angle. If you have a partner who can administer the injection, the upper arm is a comfortable, low-pain site. If you inject alone, save this site for occasional rotation and stick with the abdomen and thigh as primary sites.
Upper Outer Buttock
The upper outer quadrant of the buttock provides a deep fat pad comparable to the abdomen (1 to 3 cm in most adults). It has a large rotation area and low pain. The downside is accessibility: self-injection here requires twisting and is difficult to do with precision.
To locate the correct quadrant, imagine dividing one buttock into four equal sections. The upper outer section (farthest from the spine and above the midline of the buttock) is the safe zone. Injecting too low or too medially risks hitting the sciatic nerve, which runs through the lower buttock. Stay in the upper outer quadrant and you are well clear of the nerve.
This site works best with a partner. For solo injectors, the abdomen and thigh are more practical choices.
Site Rotation: Why It Matters and How to Do It
Injecting the same spot repeatedly causes lipodystrophy, a condition where the subcutaneous fat layer either hardens (lipohypertrophy) or thins (lipoatrophy) at the injection site. Lipohypertrophy creates firm lumps under the skin that impair absorption, meaning less sermorelin reaches the bloodstream. Lipoatrophy creates visible depressions. Both are preventable with proper rotation.
A study on insulin-injecting diabetic patients found that 64.4% of those who did not rotate sites developed lipohypertrophy, compared to 5% of consistent rotators (Blanco et al., Diabetes Metab, 2013). While this data comes from insulin (a much larger molecule injected in higher volumes), the tissue damage mechanism is identical: repeated mechanical trauma plus localized peptide exposure causes fibroblast proliferation and collagen deposition.
The 4-Quadrant Rotation System
The simplest rotation method divides the abdomen into four quadrants around the navel:
| Day | Quadrant | Description |
|---|---|---|
| Monday | Upper Right | Above navel, right side |
| Tuesday | Lower Right | Below navel, right side |
| Wednesday | Upper Left | Above navel, left side |
| Thursday | Lower Left | Below navel, left side |
| Friday | Right Thigh | Outer mid-thigh |
| Saturday | Upper Right | Shift 1 inch from Monday's spot |
| Sunday | Lower Right | Shift 1 inch from Tuesday's spot |
Within each quadrant, shift the exact puncture point by at least one inch (2.5 cm) from the previous injection in that zone. Keep a simple log or use a body map to track which spots you have used recently. A 5-day on, 2-day off sermorelin protocol naturally creates variety since you need five sites per week rather than seven.
For guidance on storing your reconstituted sermorelin between injections, see our storage guide. Proper storage prevents degradation that could change the injection characteristics.
Step-by-Step Subcutaneous Injection Technique
This section covers the complete injection process from vial to disposal. If you have never injected a peptide before, read the how to inject peptides guide first for foundational concepts.
Supplies You Need
Gather everything before you start. Working with a complete setup prevents you from setting down a capped needle and scrambling for an alcohol swab mid-injection.
- Reconstituted sermorelin vial (stored at 2 to 8 degrees Celsius; see how to store peptides)
- Insulin syringe with attached needle: 29 to 31 gauge, 0.5 inch (12.7 mm) length, 0.5 mL or 1 mL capacity
- Alcohol swabs (2): one for the vial stopper, one for the injection site
- Sharps container for needle disposal
- Cotton ball or gauze pad
- Clean, flat surface with good lighting
Use the peptide reconstitution calculator to determine your dose volume based on the concentration of your reconstituted vial.
Drawing the Dose
- 1.Remove the vial from the refrigerator. Let it sit at room temperature for 2 to 3 minutes. Cold solution can sting more upon injection.
- 2.Clean the vial stopper with an alcohol swab and let it dry.
- 3.Pull back the syringe plunger to draw air equal to your intended dose volume. If your dose is 0.1 mL (10 units on a 100-unit syringe), pull the plunger to the 10-unit mark.
- 4.Insert the needle through the center of the rubber stopper. Push the air into the vial. This equalizes pressure and makes drawing easier.
- 5.Invert the vial so the needle tip is submerged in liquid. Pull the plunger back slowly to your dose mark.
- 6.Check for air bubbles. Tap the syringe barrel with your fingernail to float any bubbles to the top. Push the plunger slightly to expel them back into the vial. Re-draw if you pushed out too much solution.
- 7.Remove the needle from the vial. Do not touch the needle to anything. Do not recap unless you have a one-handed recapping technique.
Performing the Injection
- 1.Clean the injection site with a fresh alcohol swab. Circular motion, center outward. Let the skin air-dry.
- 2.Pinch a skin fold at the chosen site with your non-dominant hand.
- 3.Hold the syringe like a pencil with your dominant hand.
- 4.Insert the needle at a 45-degree angle in one smooth motion. The needle should glide in easily. If you feel significant resistance, you may be hitting scar tissue or a firm area. Withdraw and reposition one inch away.
- 5.Inject the solution by pushing the plunger steadily over 3 to 5 seconds.
- 6.Pause for 5 seconds with the needle still in place after the plunger is fully depressed. This allows the solution to disperse and prevents leakback through the needle track.
- 7.Withdraw the needle at the same angle. Apply gentle pressure with a cotton ball for 10 seconds. Do not rub.
- 8.Dispose of the syringe immediately in a sharps container. Never reuse needles.
If a small drop of liquid appears at the injection site after withdrawal, you lost a negligible amount. This is normal and does not require re-injection.
Needle Gauge and Length Selection
A 29 to 31 gauge needle with a 0.5-inch (12.7 mm) length is the standard for subcutaneous peptide injection. The gauge refers to the needle's diameter: higher numbers mean thinner needles. A 31-gauge needle is the thinnest commonly available and causes the least pain.
| Needle Gauge | Diameter | Pain Level | Best For |
|---|---|---|---|
| 29 gauge | 0.33 mm | Low | Standard subcutaneous, all body types |
| 30 gauge | 0.30 mm | Very low | Standard subcutaneous, normal to higher body fat |
| 31 gauge | 0.25 mm | Minimal | Thin skin areas (arm), needle-sensitive users |
The 0.5-inch length is appropriate for most adults when injecting at 45 degrees into a pinched skin fold. If you are very lean (under 12% body fat for men, under 18% for women) and injecting into the thigh or arm, a 5/16-inch (8 mm) needle at 45 degrees provides extra safety margin against intramuscular penetration. For abdominal injection in most adults, a 0.5-inch needle at either 45 or 90 degrees stays safely in fat tissue.
For a broader look at needle selection across all injectable peptides, see the how to inject BPC-157 guide, which covers the same gauge and length principles.
Timing: Why You Should Inject Before Bed
Sermorelin timing is not optional. Injecting at the wrong time of day or in the wrong metabolic state can reduce the GH response by 50% or more. The two critical variables are circadian timing and fasting state.
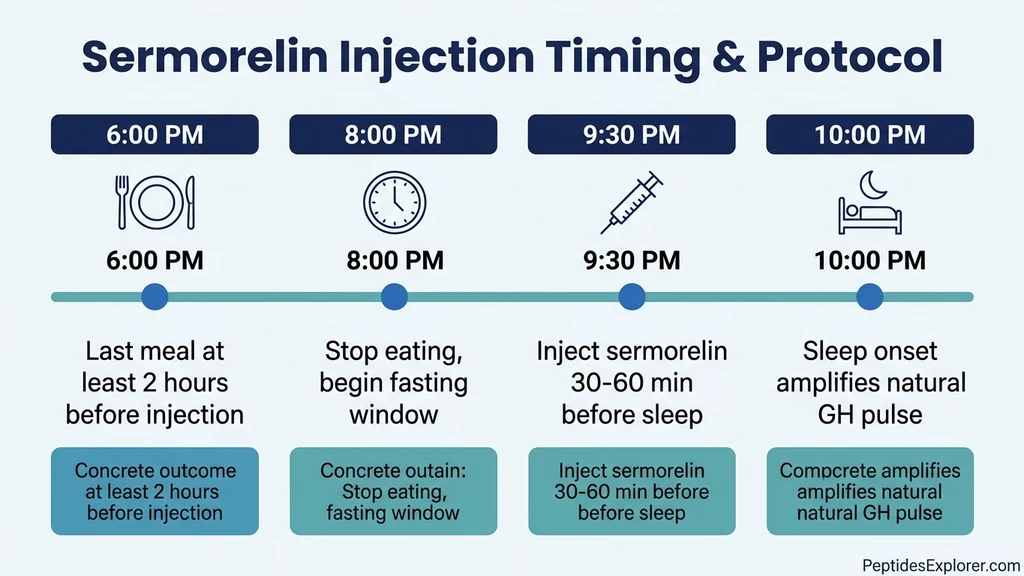
Circadian timing. Growth hormone release follows a circadian rhythm with the largest natural pulse occurring during the first 90 minutes of slow-wave sleep. Injecting sermorelin 30 to 60 minutes before sleep stacks the pharmacological GH pulse on top of the physiological one, producing the highest total GH output. A study on GHRH 1-29 administration showed that bedtime injection produced significantly greater 24-hour GH secretion compared to morning or afternoon dosing (Thorner et al., J Clin Endocrinol Metab, 1990).
Fasting state. Elevated blood glucose and insulin suppress GH release from the pituitary. Insulin directly inhibits somatotroph function, and glucose itself triggers insulin release. Injecting sermorelin after a meal blunts the GH response. Wait at least two hours after your last meal, ideally three. No food, juice, milk, or caloric beverages. Water and black coffee are fine.
| Timing Factor | Optimal | Acceptable | Avoid |
|---|---|---|---|
| Time of day | 30 to 60 min before sleep | Within 2 hours of bedtime | Morning or midday |
| Fasting window | 3+ hours after last meal | 2 hours after last meal | Within 1 hour of eating |
| Pre-injection food | Nothing | Small protein-only snack | Carbohydrate-rich meal |
| Post-injection food | Nothing until morning | Nothing for 30+ minutes | Immediate snacking |
What if you work night shifts? Inject 30 to 60 minutes before your primary sleep period, regardless of clock time. The GH amplification depends on sleep onset, not whether it is dark outside. If you sleep from 8 AM to 4 PM, inject at 7:00 to 7:30 AM.
For a full breakdown of sermorelin dosing across different goals, see sermorelin for fat loss. For stacking with ipamorelin to amplify the GH pulse further, see the CJC-1295/ipamorelin dosage calculator.
What to Avoid: Common Injection Mistakes
Most sermorelin injection problems are preventable. The following mistakes are the ones clinicians report most frequently in patients self-administering GHRH analogs.
Injecting Into Muscle Instead of Fat
Accidental intramuscular injection is the most common technical error, especially in lean individuals injecting into the thigh or arm. Signs include sharper pain during injection, faster-than-expected absorption (which may cause facial flushing), and bruising at the site.
Prevention: always pinch a skin fold before inserting the needle. If you cannot pinch at least one inch of tissue at your chosen site, switch to the abdomen. Use a 45-degree angle rather than 90 degrees at leaner sites. Never inject straight down into the thigh without pinching.
Injecting the Same Spot Repeatedly
Repeated injection at one location causes lipohypertrophy within weeks. The hardened tissue absorbs peptide erratically, sometimes faster and sometimes slower than normal fat. Patients who develop lipohypertrophy often report that sermorelin "stopped working" when in reality their absorption became unpredictable.
Prevention: follow the 4-quadrant rotation system described above. Keep a simple injection log. If you feel a lump or firmness at a previously used site, avoid that area for at least four weeks. For safe peptide administration principles, see the peptide safety guide.
Injecting After a Meal
Postprandial hyperglycemia and the resulting insulin spike are the most potent suppressors of GH release. Clinical data shows that oral glucose loading reduces GHRH-stimulated GH output by up to 75% (Vance et al., J Clin Endocrinol Metab, 1985). Injecting sermorelin within an hour of a carbohydrate-heavy meal is a near-total waste of the dose.
Prevention: set a hard cutoff. No food for at least two hours before injection. If you ate late, push the injection back rather than injecting in a fed state. A delayed injection on an empty stomach produces better results than a perfectly-timed injection on a full stomach.
Reusing Needles
Insulin syringes are single-use. After one puncture, the silicone coating on the needle tip is disrupted and the point dulls. Reusing a needle increases pain, causes more tissue trauma, raises infection risk, and can introduce bacteria into your vial (contaminating every future dose). A microscopy analysis showed that needle tips develop visible barbs and hooks after a single use, tearing rather than parting tissue on subsequent insertions.
Prevention: use a new syringe and needle for every injection. At roughly $0.15 to $0.30 per unit, insulin syringes are among the cheapest medical supplies available. The cost of a single skin infection from a reused needle exceeds a year's supply of fresh syringes.
Skipping Alcohol Prep
The skin harbors bacteria, most commonly Staphylococcus epidermidis and Staphylococcus aureus. While the risk of infection from a single unswabbed subcutaneous injection is low (estimated at less than 0.1%), daily injection over months compounds that risk significantly. Alcohol swabbing reduces bacterial colony counts at the injection site by over 90%.
Prevention: swab every time. Let the alcohol dry completely before injecting. Wet alcohol pushed into subcutaneous tissue stings and can cause a localized inflammatory reaction.
Injection Site Reactions: What Is Normal and What Is Not
Clinical trials of sermorelin reported that injection site reactions were the most common adverse event, occurring in roughly 1 in 6 patients (16.5%). Most reactions are mild and resolve within 24 to 48 hours. The Sermorelin Acetate prescribing information lists the following local reactions: pain, swelling, and redness at the injection site (RxList, Sermorelin Acetate).
| Reaction | Frequency | Duration | Action Required |
|---|---|---|---|
| Mild redness (< 2 cm) | Common (10-15%) | 1 to 24 hours | None; normal histamine response |
| Itching at site | Common (5-10%) | 1 to 12 hours | Avoid scratching; cold compress if needed |
| Small welt or bump | Occasional (3-5%) | 12 to 48 hours | Rotate away from this area for 2 weeks |
| Bruising | Occasional (3-5%) | 3 to 7 days | Hit a capillary; apply gentle pressure longer next time |
| Pain lasting > 24 hours | Uncommon (1-2%) | 24 to 72 hours | Possible IM injection; check technique and angle |
| Hardened lump (lipohypertrophy) | Develops over weeks | Weeks to months | Stop using this site; rotate more aggressively |
| Spreading redness (> 5 cm), warmth, fever | Rare (< 0.5%) | N/A | Seek medical attention. Possible cellulitis |
| Hives, difficulty breathing | Very rare (< 0.1%) | N/A | Call 911. Anaphylactic reaction |
In clinical studies, only 3 out of 350 patients (0.86%) discontinued sermorelin therapy due to injection site reactions (Vittone et al., 1997). The incidence of hypothyroidism during sermorelin therapy was 6.5%, which is a systemic effect unrelated to injection site. For a comprehensive safety overview, see is sermorelin safe.
Reducing injection site reactions: - Let the reconstituted solution reach room temperature before injecting (2 to 3 minutes out of the fridge) - Inject slowly (3 to 5 seconds) - Use the thinnest needle available (31 gauge) - Rotate sites religiously - Let alcohol dry completely before puncturing
If you experience persistent redness, warmth, or swelling that expands beyond 5 cm from the injection site, or if you develop fever, contact your healthcare provider immediately. These signs may indicate cellulitis (bacterial skin infection), which requires antibiotic treatment.
Sermorelin vs. Other Peptides: Does Injection Site Change?
Sermorelin is a systemic peptide. Unlike tissue-targeted compounds like BPC-157, the injection site does not change sermorelin's mechanism of action. All subcutaneous sites deliver sermorelin into the bloodstream, where it travels to the pituitary. This distinguishes it from healing peptides that benefit from local injection near the injury.
| Peptide | Injection Site Logic | Best Site |
|---|---|---|
| Sermorelin | Systemic; site does not affect target organ | Abdomen (absorption consistency) |
| CJC-1295 | Systemic; similar to sermorelin | Abdomen |
| Ipamorelin | Systemic; often stacked with CJC-1295 | Abdomen |
| BPC-157 | Local preferred; inject near injury site | Site-specific |
| Tirzepatide | Systemic; FDA sites: abdomen, thigh, arm | Abdomen |
If you stack sermorelin with CJC-1295 or ipamorelin, inject all peptides into the same general area (abdomen) but at different spots within the zone, separated by at least two inches. Do not mix peptides in the same syringe unless specifically instructed by your prescribing provider. Mixing can alter peptide stability and pH.
For stacking calculators and dosing, use the CJC-1295/ipamorelin dosage calculator. For the full comparison of sermorelin vs. CJC-1295, see CJC-1295 vs sermorelin.
Reconstitution and Storage Essentials
Proper reconstitution and storage directly affect injection quality. A degraded peptide solution can cause more injection site irritation and reduced efficacy.
Reconstitution. Sermorelin typically comes as a lyophilized (freeze-dried) powder in a sealed vial. Add bacteriostatic water slowly along the inner wall of the vial. Do not shake. Swirl gently until the powder dissolves completely. A clear, colorless solution indicates proper reconstitution. If the solution is cloudy, discolored, or contains particles, do not use it. Use our peptide reconstitution calculator to determine the exact volume of water to add for your desired concentration.
Storage after reconstitution. Store the reconstituted vial at 2 to 8 degrees Celsius (standard refrigerator). Do not freeze. Reconstituted sermorelin remains stable for approximately 14 to 28 days depending on the preservative in your bacteriostatic water. Record the reconstitution date on the vial with a marker. See how to store peptides for detailed temperature and duration guidelines.
Pre-injection warming. Cold solution causes vasoconstriction at the injection site, which slows absorption and increases discomfort. Remove the vial from the refrigerator 2 to 3 minutes before drawing your dose. Do not microwave, heat, or place the vial in hot water. Room temperature exposure for a few minutes is sufficient.
For sourcing, see where to buy sermorelin.
Special Populations: Adjustments for Body Type and Age
Not everyone can use the same injection angle, needle length, and default site. Body composition, age, and skin quality all affect technique.
Lean Individuals (Under 15% Body Fat)
Men under 12% and women under 18% body fat have thinner subcutaneous layers, particularly at the thigh and upper arm. For these individuals:
- Primary site: Abdomen (periumbilical fat is often the last fat depot to thin)
- Angle: 45 degrees or shallower (30 degrees for very lean)
- Needle: 31 gauge, 5/16 inch (8 mm) if available
- Pinch technique: Essential. Always lift a skin fold before inserting.
If you cannot pinch one inch of skin even at the abdomen, consult your prescribing provider about shorter needle options or alternative delivery methods.
Higher Body Fat Individuals
Individuals with BMI over 30 or significant abdominal adiposity have thicker fat pads that comfortably accommodate a 0.5-inch needle at 90 degrees. The main concern shifts from accidental IM injection (very unlikely) to ensuring the needle reaches deep enough into the subcutaneous layer for consistent absorption.
- Angle: 90 degrees is appropriate with a 0.5-inch needle
- Pinch: Optional at 90 degrees; some providers recommend injecting without pinching to allow the needle to reach deeper subcutaneous tissue
- Site selection: All four primary sites work well; the abdomen remains the default
Older Adults (Over 60)
Aging skin is thinner, more fragile, and bruises more easily due to reduced collagen and capillary fragility. Older adults using sermorelin for age-related GH decline should:
- Use 31-gauge needles to minimize tissue trauma
- Apply gentle pressure for 15 to 20 seconds after withdrawal (longer than the standard 10 seconds)
- Rotate more aggressively since older skin recovers more slowly from repeated punctures
- Avoid the upper arm unless assisted, as older skin in this area is often too thin
- Prefer the abdomen where subcutaneous fat is typically preserved even in age-related body composition changes
Sermorelin was originally studied for age-related GH decline and showed sustained efficacy over 24 months in older adults (Vittone et al., 1997). For a comprehensive look at sermorelin safety across populations, see is sermorelin safe.
Frequently Asked Questions
Where is the best place to inject sermorelin?
The abdomen is the best sermorelin injection site for most people. Inject subcutaneously at least two inches from the navel, in the fat pad between the ribs and hip bones. The abdomen has the thickest fat layer (1.5 to 3 cm), the largest rotation area, and the easiest self-access. The front of the thigh and back of the upper arm are alternatives. For technique details, see our how to inject peptides guide.
Can I inject sermorelin in my thigh?
Yes. The front or outer thigh (middle third between knee and hip) is a valid subcutaneous injection site for sermorelin. Pinch a fold of skin and inject at 45 degrees. The thigh has less fat than the abdomen (0.5 to 2 cm vs. 1.5 to 3 cm), so lean individuals should use the abdomen instead. For injection site comparison data, see best injection sites for tirzepatide, which covers the same anatomical sites.
What time of day should I inject sermorelin?
Inject sermorelin 30 to 60 minutes before bedtime on an empty stomach (at least 2 hours after your last meal). Bedtime injection amplifies the natural GH pulse that occurs during early sleep. Injecting after a meal, especially one high in carbohydrates, blunts the GH response by up to 75%. For dosing and timing protocols, see sermorelin for fat loss.
Do I inject sermorelin subcutaneously or intramuscularly?
Subcutaneously. Sermorelin is administered as a subcutaneous injection into the fat layer just beneath the skin. Use a 29 to 31 gauge insulin needle, 0.5 inches long, at a 45-degree angle into a pinched skin fold. Intramuscular injection causes faster absorption and a less physiological GH pulse pattern. For reconstitution before injection, use our peptide reconstitution calculator.
What needle size should I use for sermorelin injections?
Use a 29 to 31 gauge needle, 0.5 inches (12.7 mm) long. A 31-gauge needle is the thinnest commonly available and causes the least pain. For very lean individuals, a 5/16-inch (8 mm) needle at 45 degrees reduces the risk of accidental intramuscular injection. Standard insulin syringes (0.5 or 1.0 mL) with attached needles work perfectly. For a broader needle selection guide, see how to inject BPC-157.
How do I rotate sermorelin injection sites?
Divide the abdomen into four quadrants (upper right, lower right, upper left, lower left) and rotate through them across consecutive injections. Within each quadrant, shift the exact puncture point by at least one inch each time. Add the thigh to your rotation on day 5 or 6. This prevents lipodystrophy, a condition where repeated injection causes fat hardening or thinning. For safe injection practices, see the peptide safety guide.
Is it normal for the injection site to be red after sermorelin?
Mild redness (under 2 cm in diameter) lasting 1 to 24 hours is normal and occurs in 10 to 15% of sermorelin users. It is a histamine response to the needle puncture and the peptide solution. If redness spreads beyond 5 cm, feels warm to the touch, or is accompanied by fever, contact your healthcare provider. These signs may indicate infection. For a full safety profile, see is sermorelin safe.
Can I stack sermorelin with CJC-1295 or ipamorelin using the same injection site?
You can inject stacked peptides into the same general area (the abdomen), but use different spots within the zone, separated by at least two inches. Do not mix peptides in the same syringe unless your prescribing provider specifically instructs it. Calculate your stacking doses with the CJC-1295/ipamorelin dosage calculator. For comparison of these GHRH analogs, see CJC-1295 vs sermorelin.
What happens if I inject sermorelin into muscle instead of fat?
Accidental intramuscular injection causes faster absorption, a sharper but shorter GH pulse, more pain at the site, and increased bruising. It is not dangerous, but it is not optimal. Prevention: always pinch a skin fold before inserting, inject at 45 degrees, and use the abdomen where fat is thickest. If you cannot pinch one inch of skin at your chosen site, switch to the abdomen. For general safety, see the peptide safety guide.
Where can I buy sermorelin for injection?
Sermorelin is available through compounding pharmacies with a prescription and from peptide research suppliers. Quality varies significantly between sources. For a ranked list of verified suppliers with third-party testing, see where to buy sermorelin. Always verify that your source provides a certificate of analysis (COA) with purity above 98%.
The Bottom Line
The best place to inject sermorelin is the abdomen, at least two inches from the navel, using a 29 to 31 gauge insulin needle at 45 degrees. The thigh and upper arm serve as rotation alternatives. Inject 30 to 60 minutes before sleep on an empty stomach to maximize the GH response. Rotate sites across four abdominal quadrants to prevent lipohypertrophy, and never reuse a needle.
Sermorelin is a short-acting peptide with a 10 to 20 minute half-life. Getting the technique and timing right is the difference between a strong GH pulse and a wasted dose. If you are new to peptide injection, practice the pinch-and-insert technique on the abdomen where the fat pad is most forgiving. Within a week, the process takes under 60 seconds.
For your next steps: calculate your sermorelin dose with the peptide reconstitution calculator, review sermorelin safety data, and explore stacking with CJC-1295 or ipamorelin for amplified GH release. For sourcing, see where to buy sermorelin.
Helpful Tools
Related Articles
Where to Inject BPC-157: Site Guide
Where to inject BPC-157 for shoulder, back, hip, gut, elbow, and Achilles injuries. Anatomical sites, local vs systemic delivery, and rotation.
How to Inject BPC-157: Sites & Guide
How to inject BPC-157 subcutaneously: step-by-step technique, injection site selection by injury, needle gauge, reconstitution, and sterile protocol.
Best Place to Inject Tirzepatide: 3 Sites Ranked
Best tirzepatide injection site: abdomen wins on absorption. Compare abdomen, thigh, and upper arm with rotation maps and BMI guidance.
Does Sermorelin Increase Testosterone?
Does sermorelin increase testosterone? Not directly. It boosts GH, which supports testosterone via IGF-1 and improved sleep. Evidence reviewed.