
You are holding a Mounjaro pen or a vial of compound tirzepatide, and you need to pick a spot. The abdomen is the best place to inject tirzepatide for most people. It provides the largest subcutaneous fat pad (1.5 to 3 cm), the easiest self-access, and the most consistent absorption. The front of the thigh and the back of the upper arm are the two alternative FDA-cleared sites. The Mounjaro prescribing information states that similar exposure is achieved at all three sites. What differs between them is fat pad thickness, ease of self-access, and comfort, not how fast the drug reaches peak concentration.
| Injection Site | Fat Pad | Self-Access | Absorption Speed | Best For |
|---|---|---|---|---|
| Abdomen | 1.5 to 3 cm | Easy | Similar exposure | First choice, most users |
| Front/outer thigh | 0.5 to 2 cm | Easy | Similar exposure | Abdomen rotation rest |
| Back of upper arm | 0.5 to 1.5 cm | Difficult | Similar exposure | With helper only |
| Bioavailability (all sites) | ~80% | — | — | Equivalent AUC |
For precise dose calculations, use our tirzepatide dosage calculator. For the full escalation schedule, see the tirzepatide dosage chart. Tirzepatide (Mounjaro, Zepbound) is not FDA-approved for use outside labeled indications. Consult a healthcare provider before starting or adjusting your injection regimen.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
Injection Sites Compared: Abdomen vs Thigh vs Upper Arm
All three FDA-approved sites deliver adequate tirzepatide exposure. The Mounjaro prescribing information states that similar exposure is achieved with subcutaneous administration in the abdomen, thigh, or upper arm. Total drug exposure does not change with location, and no published study reports a clinically meaningful difference in Tmax between the three sites. Median Tmax is 24 hours, with an individual range of 8 to 72 hours that swamps any site effect. Site choice is a comfort and skin-health decision, not a pharmacokinetic one. See GLP-1 injection sites for the label language across the whole class.

| Factor | Abdomen | Front/Outer Thigh | Back of Upper Arm |
|---|---|---|---|
| Fat pad thickness | 1.5 to 3 cm | 0.5 to 2 cm | 0.5 to 1.5 cm |
| Self-access | Easy | Easy | Difficult (needs helper) |
| Absorption speed (Tmax) | No meaningful difference | No meaningful difference | No meaningful difference |
| Rotation area | Largest | Large | Smallest |
| IM injection risk | Very low | Higher in lean users | Moderate |
| Pain level | Low | Low to moderate | Low |
| Bruising risk | Low | Moderate | Low to moderate |
Subcutaneous bioavailability is approximately 80% across all three sites. Tirzepatide's 8 to 72-hour Tmax window reflects individual variation more than site selection. Injection site reactions occurred in 3 to 7% of SURMOUNT trial participants, classified as mild in the majority of cases (Jastreboff et al., NEJM, 2022).
Abdomen: The Preferred Injection Site
The abdomen ranks first for three reasons: thickest subcutaneous fat layer, largest rotation surface, and easiest self-access angle. Most users can inject here without a mirror or assistance.
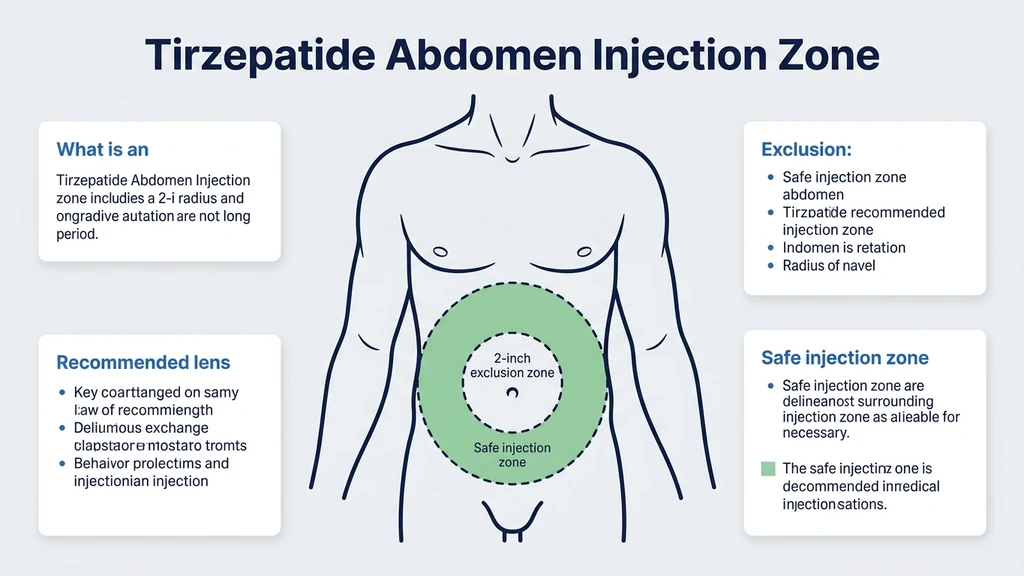
Exact Location and Boundaries
The usable injection zone sits below the ribs, above the hip bones, and at least 2 inches (5 cm) from the navel in every direction. Avoid the waistline where clothing creates friction. Stay away from visible veins, scars, stretch marks, and any area showing active redness or irritation.
Think of your abdomen as a clock face centered on the navel. The injection ring extends from 2 inches out to the edge of your torso. That ring provides dozens of distinct sites for weekly rotation, far more than the thigh or upper arm can offer.
Why the Abdomen Ranks First
Subcutaneous fat in the abdomen averages 1.5 to 3 cm in most adults. This thickness keeps the needle tip in fat tissue rather than muscle, which is critical for proper subcutaneous absorption. Tirzepatide absorbs differently when injected intramuscularly: faster initial uptake, higher Cmax spikes, and potentially more GI side effects during that dosing interval.
The abdomen is the default for a practical reason, not a pharmacokinetic one. Tirzepatide reaches peak plasma concentration between 8 and 72 hours after the dose, and that spread is driven by the individual rather than by the site. For lean individuals, the abdomen still provides more subcutaneous tissue than the other two sites and remains the first choice across all body composition categories.
Abdomen Injection: Step-by-Step for Pen and Syringe
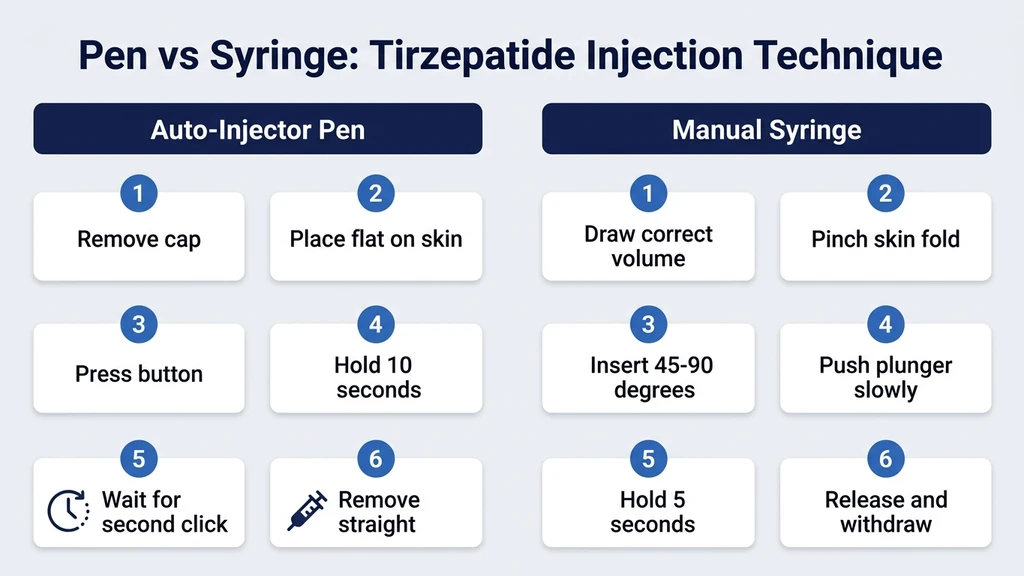
For Mounjaro or Zepbound auto-injector pen:
- 1.Remove from refrigerator 30 minutes before injection. Let the pen reach room temperature. Cold tirzepatide stings more and may slow auto-delivery.
- 2.Clean the site with a 70% isopropyl alcohol swab. Let skin air-dry 10 seconds. Wet skin on the needle path causes stinging.
- 3.Uncap the pen by pulling the cap straight off. Do not twist.
- 4.Place the base flat against clean skin. Do not pinch the abdomen for pen injections. Press and hold the activation button until the first click.
- 5.Hold for 10 seconds without moving. Wait for the second click confirming full dose delivery.
- 6.Remove straight up. Apply gentle pressure with a dry cotton ball for 10 seconds. Do not rub.
For compound tirzepatide with a manual syringe:
- 1.Draw the correct volume using your prescribed dose and reconstitution concentration. See the compound tirzepatide dosage chart for unit conversions.
- 2.Clean with alcohol and let dry completely.
- 3.Pinch a skin fold if abdominal fat is minimal (less than 1 inch of pinchable tissue).
- 4.Insert at 90 degrees for ample abdominal fat, 45 degrees if fat is thin.
- 5.Push the plunger slowly over 5 to 10 seconds.
- 6.Hold the needle in place for 5 seconds after delivery completes.
- 7.Release the skin fold, withdraw the needle, apply gentle pressure.
Front and Outer Thigh: The Best Alternative
The thigh is the second-best site and the preferred alternative when the abdomen needs rest during a rotation cycle. It offers a large, visible surface that makes self-injection straightforward.
Exact Location and Boundaries
The injection zone covers the middle third of the front and outer thigh: from roughly a hand-width above the kneecap to a hand-width below the hip crease. Inject in the front or slightly outer quadrant. Avoid the inner thigh where nerves and blood vessels cluster near the surface. Avoid the back of the thigh where the hamstring sits close to the skin.
Thigh Pros and Cons
The thigh provides a large, visible surface with full self-access. You can see exactly where the needle enters, which builds injection confidence for newer users.
The drawback is thinner fat: subcutaneous tissue averages only 0.5 to 2 cm, about half the abdomen's range. In lean individuals (BMI under 25), this creates real risk of accidental intramuscular injection. Muscle tissue absorbs tirzepatide faster, which can intensify nausea and GI symptoms during that dosing interval. Pinch the skin and inject at 45 degrees if you can lift less than 1 inch of thigh tissue.
Some users report more bruising and mild pain at the thigh. This reflects the thinner fat cushion and denser nerve endings in the quadriceps area.
Thigh Injection: Step-by-Step
1. Sit in a chair with your leg relaxed. Tensed muscle makes needle insertion harder and increases bruising.
2. Identify the middle-third zone of your outer thigh. The target area is roughly the size of your palm.
3. Clean the site with alcohol, let dry.
4. Assess fat thickness. If you can pinch less than 1 inch, use 45 degrees and a skin fold. More than 1 inch, use 90 degrees without a fold.
5. For the pen: place flat against skin, press the button, hold 10 seconds until the second click.
6. For the syringe: pinch if needed, insert at the appropriate angle, inject slowly over 5 to 10 seconds, hold 5 seconds, then withdraw.
7. Apply gentle pressure. Do not rub. A small red dot or minor bruise is normal and resolves within days.
Back of Upper Arm: Requires Assistance
The posterior upper arm is the third FDA-approved site. It works well when a partner or healthcare provider administers the injection. Self-injection here requires significant flexibility and a mirror.
Exact Location and Boundaries
The target area sits on the back of the upper arm, midway between the shoulder and the elbow, focused on the fleshy posterior portion. Avoid the outer arm where the deltoid sits close to the surface. Avoid the inner arm where veins and nerves run near the skin. The usable zone is smaller than the abdomen or thigh, requiring more precise placement.
When to Choose the Upper Arm
Three situations make the upper arm the right choice. First, both the abdomen and thigh are in rotation rest. Second, you experience persistent injection site reactions at the abdomen or thigh but not the arm. Third, a healthcare provider is administering the injection in a clinical setting.
The upper arm has the thinnest fat pad (0.5 to 1.5 cm). Accidental intramuscular injection is more likely here, especially in muscular or lean individuals. Whoever administers the injection should pinch the skin and inject at a 45-degree angle. A shorter needle (4 to 5 mm) reduces intramuscular risk further.
How to Rotate Injection Sites Properly
Rotation prevents lipodystrophy and maintains consistent absorption. Injecting the same spot every week damages subcutaneous tissue, creating firm lumps that alter drug uptake unpredictably.
The 4-Quadrant Rotation System
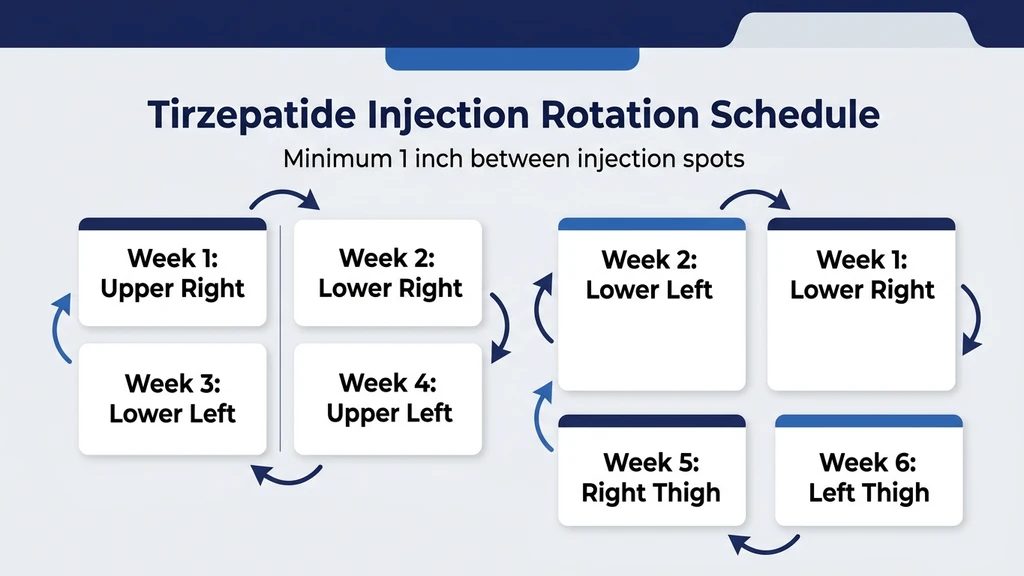
Divide your abdomen into four quadrants: upper right, lower right, lower left, upper left. Rotate clockwise each week. Within each quadrant, place the injection at least 1 inch (2.5 cm) from the previous spot in that quadrant.
A practical 6-site schedule: Week 1, upper right abdomen. Week 2, lower right abdomen. Week 3, lower left abdomen. Week 4, upper left abdomen. Week 5, right thigh. Week 6, left thigh. Then repeat. This gives each zone at least 5 weeks of recovery before the next injection returns there.
Track each injection location and date in a phone note or a small journal. Ten seconds of record-keeping prevents months of lipodystrophy.
Why Rotation Prevents Lipodystrophy
Repeated injection at the same spot causes lipohypertrophy: a buildup of fibrous fatty tissue that feels rubbery under the skin. Studies in insulin-dependent diabetes show up to 39% variability in drug absorption from lipohypertrophic areas compared to healthy subcutaneous tissue. The same mechanism applies to tirzepatide: a preferred injection spot develops erratic permeability that produces inconsistent weekly drug levels and unpredictable effects.
Rotating preserves tissue integrity. Visible lumps or skin texture changes at an injection site are signs to stop using that area and let it recover before returning.
Injection Tracking Methods
Three methods work consistently. First, a printed body map where you mark each injection with the date. Second, a phone note: write the site name (e.g., "abdomen lower right") and date immediately after each injection. Third, a repeating weekly phone reminder that includes a note field for the last site used.
The goal: never inject the same square inch more than once every 4 to 6 weeks.
Reducing Pain, Bruising, and Injection Site Reactions
Injection site reactions occurred in 3 to 7% of SURMOUNT trial participants, classified as mild in the majority (Jastreboff et al., NEJM, 2022). A published case report documented a tirzepatide ISR presenting as a firm erythematous plaque that resolved with topical corticosteroid treatment (PMC, 2023). Proper technique reduces both frequency and severity. For detailed reaction management, see our guide on tirzepatide injection site reactions.
Pre-Injection Preparation
Room temperature medication. Remove the pen or vial from the refrigerator 30 minutes before injection. Do not microwave, heat in water, or shake. Cold tirzepatide stings more and may increase localized reaction risk.
Clean and dry. Use a 70% isopropyl alcohol swab and let skin air-dry for at least 10 seconds. Injecting through wet alcohol causes burning at the needle entry point.
Optional ice. Press a cold pack against the site for 20 to 30 seconds before swabbing. This numbs superficial nerve endings and reduces the pinch sensation. Remove the ice before applying alcohol.
During-Injection Technique
Pinch for thin areas. Use a skin fold for the thigh, upper arm, and lean abdomen. Place the pen flat without pinching for areas with ample subcutaneous fat.
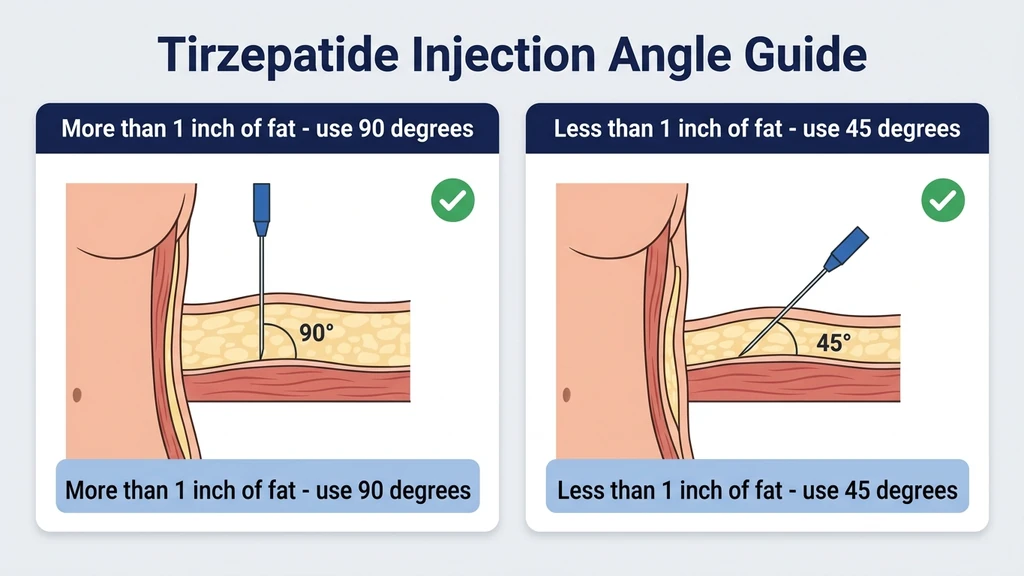
Angle by fat thickness. Use 90 degrees when subcutaneous fat exceeds 1 inch of pinchable tissue. Use 45 degrees when the fat layer is thin. The objective: deposit drug in fat, not muscle.
Slow delivery. For syringe injection, push the plunger over 5 to 10 seconds. Hold the needle in place for 5 to 10 seconds after dose delivery before withdrawing.
Post-Injection Care
Apply light pressure with a dry cotton ball for 10 seconds. Do not rub the injection site. Rubbing disperses the drug too rapidly, increasing local inflammation and bruising.
Mild redness or a small bump is normal and resolves within 1 to 2 hours. Bruising smaller than a coin fades in 3 to 7 days. Contact your prescriber if a lump grows over several days, if warmth and redness spread beyond 2 inches from the injection point, or if pain worsens after the first 24 hours.
Managing Persistent Reactions
If ISRs recur consistently at the same body region, switch to a different site for 4 to 6 weeks. The abdomen often triggers fewer reactions than the thigh, possibly because the thicker fat cushion buffers peptide absorption with less tissue disruption.
For mild reactions (redness, itch, small welt), an oral antihistamine and cool compress for 20 minutes provides relief. For reactions that persist beyond 48 hours or enlarge significantly, consult your prescriber. Rotating away from the reactive site while it heals is the primary management strategy.
Pen vs Compound Syringe: Key Differences
Mounjaro and Zepbound use a pre-filled, single-use auto-injector pen with a pre-attached 31-gauge hidden needle. You press the pen against skin, push a button, and the device auto-delivers the dose. The needle retracts after injection. You never see or manually handle the needle.
Compound tirzepatide from a 503A or 503B pharmacy comes in a lyophilized vial that you reconstitute with bacteriostatic water, then draw into a manual syringe (29 to 31 gauge, 5/16 to 1/2 inch recommended). This requires more preparation: calculating the correct volume from the reconstituted concentration, removing air bubbles, and controlling injection speed manually.
See our guides on how to reconstitute tirzepatide and compound tirzepatide safety for preparation details. The injection site selection principles are identical for both delivery methods.
Needle Gauge and Depth for Compound Syringe
The Mounjaro and Zepbound pen uses a 31-gauge, 4 mm pre-attached needle, optimized for subcutaneous delivery in adults of average body composition.
For compound tirzepatide, the standard recommendation is 29 to 31-gauge with a 5/16 inch (8 mm) length. Lean individuals may benefit from a shorter 4 mm needle at the thigh and upper arm to avoid intramuscular delivery. Individuals with more subcutaneous tissue can use a 1/2-inch (12 mm) needle at the abdomen without concern.
Finer gauge needles (31-gauge) cause less tissue trauma and are appropriate for all three sites. Coarser gauges (28 or larger) increase discomfort per injection without clinical benefit.
Special Considerations by Body Composition
Body composition determines the optimal injection angle and needle depth. Using the same approach for all individuals increases intramuscular injection risk in lean users and reduces delivery precision for others.
Lean Individuals (BMI Under 25)
Subcutaneous fat may be as thin as 0.5 cm at the thigh and 1 cm at the abdomen for lean users. Use a 45-degree angle with a pinched skin fold at every site. Shorter needles (4 to 5 mm) reduce the chance of reaching muscle.
The abdomen remains best for lean users because it retains more subcutaneous tissue even at low body fat percentages. Avoid the thigh if you can pinch less than 1 inch of fat. If using the upper arm, always have a helper administer, and always pinch.
Higher BMI Individuals
At higher body fat levels, subcutaneous tissue is thicker and 90-degree injection delivers the drug properly. Standard pen needles and 1/2-inch syringe needles reach the subcutaneous layer without difficulty.
All three sites work well at higher BMI. The abdomen still offers the most rotation space. The thigh and upper arm become more viable as fat pad thickness increases, since adequate subcutaneous tissue ensures consistent subcutaneous delivery. Avoid injecting into skin folds or stretch marks, which have disrupted vasculature and unpredictable absorption rates.
When to Call Your Doctor
Most injection discomfort is minor and self-resolving. Three situations require medical attention.
Signs of systemic allergic reaction: Hives spreading beyond the injection site, facial or lip swelling, difficulty breathing, or rapid heartbeat. These require emergency evaluation. The Mounjaro prescribing information lists hypersensitivity reactions as a potential serious adverse reaction (FDA Prescribing Information, 2022).
Persistent lump or nodule: A firm area at the injection site that does not resolve within 2 weeks may indicate lipohypertrophy, an abscess, or a granuloma. Your prescriber should evaluate it.
Spreading redness with worsening pain: Signs of cellulitis (skin infection). Expanding redness beyond 2 inches from the injection point combined with increasing pain and warmth warrants same-day evaluation. Infection at injection sites is rare with proper sterile technique but it can occur. For the complete step-by-step technique guide, see how to inject tirzepatide. For systemic safety data, see our tirzepatide long-term side effects review. For medication safety, see our tirzepatide drug interactions guide.
Frequently Asked Questions
Does it matter where you inject tirzepatide?
Yes, for comfort and skin health, but not for drug exposure or absorption speed. The Eli Lilly PK study (NCT04050670) confirmed equivalent AUC across the abdomen, thigh, and upper arm. The abdomen provides the thickest fat pad (1.5 to 3 cm), making it the preferred site. All three FDA-approved sites deliver approximately 80% bioavailability. See the tirzepatide dosage chart for dose-specific guidance.
Is the stomach or thigh better for tirzepatide injection?
The abdomen is better for most people. It has a thicker fat pad (1.5 to 3 cm vs 0.5 to 2 cm), lower bruising risk, and faster peak absorption. The thigh is the best alternative when the abdomen is in rotation rest or shows persistent reactions. Lean individuals with less than 1 inch of pinchable thigh fat should inject at 45 degrees to avoid intramuscular delivery. See our injection site reaction guide for managing any localized issues.
Can I inject tirzepatide in my buttocks?
The buttocks are not an FDA-approved injection site for tirzepatide. The prescribing information specifies three sites: abdomen, thigh, and upper arm. No pharmacokinetic data exists for buttock injections. Stick to the three approved locations and rotate using the 4-quadrant abdomen system plus alternating thighs.
How far apart should tirzepatide injection sites be?
Space each injection at least 1 inch (2.5 cm) from the previous site within the same body region. Allow at least 4 to 6 weeks before returning to the same quadrant. The 4-quadrant abdomen rotation plus alternating thighs provides 6 distinct zones, giving each area 5 or more weeks of recovery time. For compound tirzepatide dosing specifics, see the compound tirzepatide dosage chart.
Can I inject tirzepatide in the same area every week?
Injecting the same small area every week causes lipohypertrophy, a fibrous tissue buildup that disrupts absorption by up to 39%. Rotate across at least 4 distinct zones. Using the same general region (e.g., abdomen) is acceptable if you move at least 1 inch from the previous spot each time. The 4-quadrant system with 1-inch minimum separation prevents tissue damage and absorption variability.
What angle should I inject tirzepatide?
Use 90 degrees if you can pinch more than 1 inch of fat at the injection site. Use 45 degrees when the fat layer is thin (less than 1 inch). The auto-injector pen is designed for 90-degree placement against the skin. Manual syringe users should assess fat thickness at each site and adjust accordingly. Lean individuals should always use 45 degrees at the thigh and upper arm.
Does injection site affect tirzepatide weight loss results?
No. The Eli Lilly pharmacokinetic study confirmed equivalent total drug exposure (AUC) across all three approved sites. Weight loss depends on dose, adherence, diet, and metabolic factors. The injection site influences comfort and absorption timing but not the total amount absorbed. Choose the site that enables consistent, comfortable rotation every week. For real-world results data, see our tirzepatide before and after guide.
The Bottom Line
The abdomen is the best place to inject tirzepatide: thickest fat pad and largest rotation area among the three FDA-cleared sites. The thigh is the strongest alternative for rotation rest weeks. The upper arm works with a helper.
Rotation prevents lipodystrophy. The 4-quadrant abdomen system plus alternating thighs gives each zone at least 5 to 6 weeks of recovery. Proper technique, including correct angle, slow injection, room-temperature medication, a 10-second hold after delivery, and no rubbing, reduces the 3 to 7% injection site reaction rate documented in the SURMOUNT trials.
Use our tirzepatide dosage calculator to confirm your dose before injection. For step-by-step device technique, see how to inject tirzepatide. For compound preparation, see how to reconstitute tirzepatide. If injection site reactions persist despite proper rotation, consult your prescriber about site management or evaluation for localized sensitivity.
The same three sites are approved across the whole class. GLP-1 injection sites compares the Ozempic, Wegovy, Mounjaro and Zepbound labels side by side.
Related Articles
GLP-1 Injection Sites: The 3 Approved Spots
GLP-1 injection sites: abdomen, front thigh, back of upper arm. What the Ozempic, Wegovy, Mounjaro and Zepbound labels say, plus a rotation plan that works.
How to Inject Tirzepatide: Full Guide
How to inject tirzepatide step by step: Mounjaro autoinjector pen technique, compounded vial subcutaneous injection, injection sites, and rotation schedule.
Cheapest Tirzepatide: Every Route Priced (2026)
The cheapest tirzepatide in 2026: manufacturer self-pay vials from $299/month, $25 insured copays, true cost per milligram, and why compounded copies ended.
Does Tirzepatide Help With Inflammation?
Does tirzepatide help with inflammation? Yes: CRP drops 32.9%, IL-6 drops 17.8% in trials. SURMOUNT data and adipose tissue mechanisms.