You ordered compounded tirzepatide. The vial arrived as a white powder. The bacteriostatic water sits next to it. Your provider prescribed a dose in milligrams, but the vial has no mixing instructions and the syringe reads in units.
To reconstitute tirzepatide: draw bacteriostatic water into a syringe, inject it slowly against the glass wall of the peptide vial, and swirl gently until the powder dissolves. For a 5mg vial, add 1 mL of water to get 5 mg/mL. For a 10mg vial, add 1 mL for 10 mg/mL or 2 mL for 5 mg/mL. The entire process takes under five minutes.
The rest of this guide covers every vial size, concentration tables, syringe unit conversions, storage rules, and the specific mistakes that lead to dosing errors. For instant math on any combination, use the Peptide Reconstitution Calculator.
*This article is for research and educational purposes only. It is not medical advice. Tirzepatide is a prescription medication. Consult a licensed healthcare provider before using any GLP-1 receptor agonist.*
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
What You Need Before Starting
Gather all supplies before opening the vial. Once the rubber stopper is punctured, you want to move efficiently to minimize contamination risk.
Required materials:
- Lyophilized tirzepatide vial (5mg, 10mg, 15mg, or 30mg)
- Bacteriostatic water (0.9% benzyl alcohol preserved)
- 3 mL or 5 mL syringe with an 18 to 21 gauge drawing needle
- Insulin syringes for dosing (U-100, 29 to 31 gauge, 0.3 mL or 0.5 mL)
- Alcohol swabs (70% isopropyl)
- Fine-point marker or label tape
- Clean, flat work surface
Optional but recommended:
- Sharps container for used needles
- Nitrile gloves
- 0.22 micron syringe filter (if concerned about particulate contamination)
The drawing syringe is for transferring water into the peptide vial. The insulin syringes are for measuring and injecting individual doses afterward. These are two different tools. Never use the same syringe for both tasks. For a full explanation of syringe types and gauge selection, see the peptide safety guide.
Bacteriostatic Water vs Sterile Water
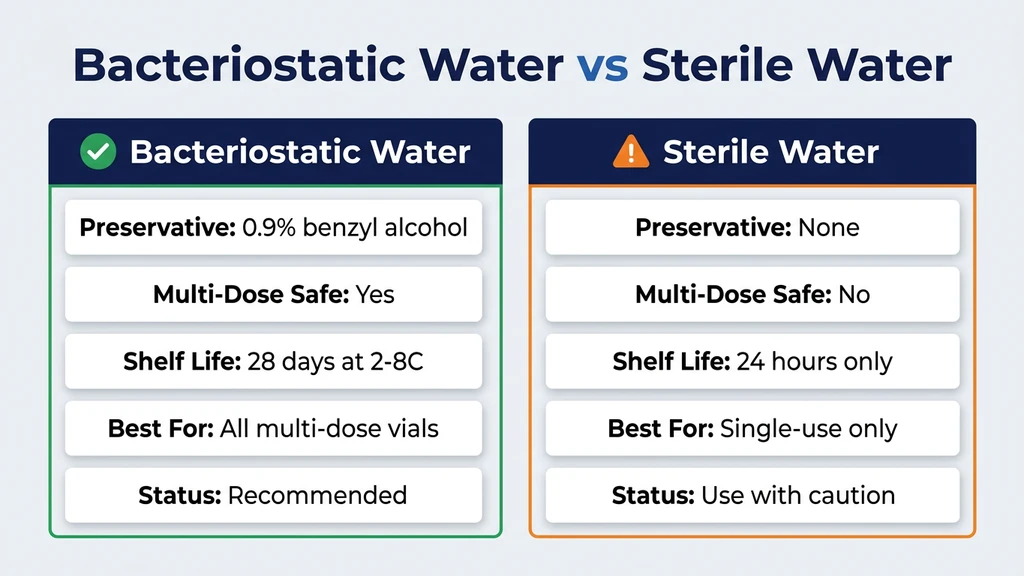
Bacteriostatic water (BAC water) contains 0.9% benzyl alcohol as a preservative. This antimicrobial agent inhibits bacterial growth inside the vial after each needle puncture. BAC water extends the usable life of reconstituted tirzepatide to 28 days when refrigerated at 2 to 8 degrees Celsius.
Sterile water contains no preservative. It is acceptable for single-use reconstitution where the entire vial is consumed within 24 hours. For multi-dose vials (anything you plan to draw from more than once), sterile water is a contamination risk. Each needle insertion introduces potential bacteria, and without benzyl alcohol, nothing stops them from multiplying.
Normal saline (0.9% sodium chloride) is sometimes used for other peptides, but bacteriostatic water is the standard and recommended solvent for tirzepatide reconstitution. If you need a reliable source, see where to buy bacteriostatic water for injection. Stick with BAC water unless your prescriber specifically directs otherwise.
For a deeper comparison of solvents across peptide types, see how much bacteriostatic water for semaglutide, which covers the same principles in detail.
| Solvent | Preservative | Multi-Dose Safe? | Shelf Life After Mixing | Best For |
|---|---|---|---|---|
| Bacteriostatic water | 0.9% benzyl alcohol | Yes | 28 days at 2-8°C | All multi-dose vials |
| Sterile water | None | No | 24 hours | Single-use only |
| Normal saline (0.9% NaCl) | None | No | 24 hours | Not standard for tirzepatide |
Step-by-Step Reconstitution Process
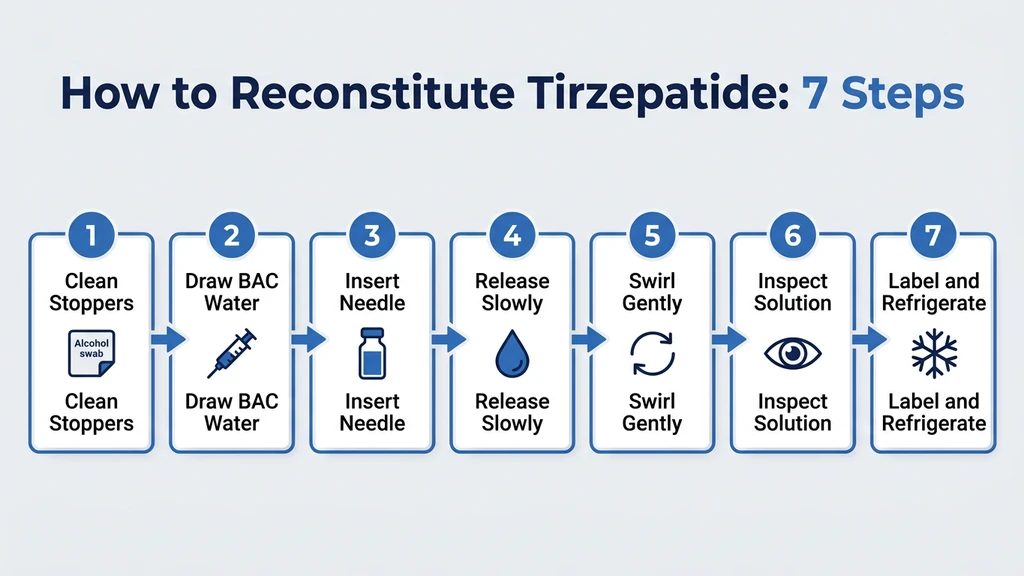
Follow these seven steps. The process takes two to five minutes from start to finish.
- 1.Clean both vial stoppers. Wipe the tirzepatide vial stopper and the bacteriostatic water vial stopper with separate alcohol swabs. Let each air dry for 10 seconds. This removes surface bacteria that could enter the vial during needle insertion.
- 1.Draw bacteriostatic water. Attach the drawing needle (18 to 21 gauge) to the 3 mL syringe. Insert it into the BAC water vial, invert the vial, and pull the plunger to your target volume. Refer to the concentration tables below to choose how much water to add. Tap the syringe barrel to dislodge air bubbles and push them out.
- 1.Insert the needle into the tirzepatide vial. Push the needle through the center of the rubber stopper at a slight angle with the bevel facing up. This prevents coring (punching a rubber fragment into the solution). Once through the stopper, straighten the needle.
- 1.Release the water slowly against the glass wall. Aim the needle tip at the inside wall of the vial, not directly onto the powder cake. Push the plunger steadily over 30 to 60 seconds. Let the water trickle down the glass and pool at the bottom beneath the lyophilized powder.
- 1.Remove the syringe and swirl gently. Hold the vial between your thumb and forefinger and rotate it in slow circles. Never shake. Vigorous agitation creates foam and can denature the peptide through mechanical shearing. Most tirzepatide powder dissolves within 1 to 3 minutes of gentle swirling.
- 1.Inspect the solution. Reconstituted tirzepatide should be clear and colorless to very slightly yellow. Hold the vial up to a light source. If you see particles, cloudiness, or discoloration, do not inject. A few small bubbles on the surface are normal and will dissipate within minutes.
- 1.Label and refrigerate immediately. Write the peptide name, concentration (e.g., "Tirzepatide 10 mg/mL"), and today's date on the vial. Store upright in the refrigerator at 2 to 8 degrees Celsius. The solution is now ready for dosing.
If undissolved powder remains after 5 minutes of swirling, place the vial upright in the refrigerator for 10 to 15 minutes, then swirl again. Do not apply heat. Do not shake. Patience dissolves what force cannot.
Concentration Tables by Vial Size
The reconstitution formula is: Concentration (mg/mL) = Peptide amount (mg) / Water added (mL).
This determines how much liquid you draw per dose. More water means a lower concentration, which means a larger draw volume per dose. Larger draw volumes are easier to measure accurately on an insulin syringe. Less water means a higher concentration and smaller, harder-to-read draw volumes.
The tables below cover all four common tirzepatide vial sizes at multiple water volumes. Find your vial size and choose a water volume that matches your dose range. For any combination not listed, the Peptide Reconstitution Calculator gives instant results.
5 mg Vial
The 5mg vial is common for starting doses during the initial titration phase (2.5 mg per week).
| BAC Water Added | Concentration | 2.5 mg Dose = | Syringe Units (U-100) |
|---|---|---|---|
| 0.5 mL | 10 mg/mL | 0.25 mL | 25 units |
| 1 mL | 5 mg/mL | 0.50 mL | 50 units |
| 2 mL | 2.5 mg/mL | 1.00 mL | 100 units |
Recommended for 5mg vials: Add 1 mL for a 5 mg/mL concentration. At this concentration, the starting dose of 2.5 mg requires 50 units on your syringe, which is easy to read and measure. Adding 0.5 mL gives 10 mg/mL, which works but produces smaller draw volumes that are slightly harder to measure on larger syringes.
A single 5mg vial provides two doses at 2.5 mg per week (two weeks of the starting dose). If you plan to titrate up quickly, a larger vial is more cost-effective.
10 mg Vial
The 10mg vial is the most versatile size. It covers both the 2.5 mg starting dose and the first escalation to 5 mg per week.
| BAC Water Added | Concentration | 2.5 mg = | 5 mg = | Syringe Units per 2.5 mg |
|---|---|---|---|---|
| 0.5 mL | 20 mg/mL | 0.125 mL | 0.25 mL | 12.5 units |
| 1 mL | 10 mg/mL | 0.25 mL | 0.50 mL | 25 units |
| 2 mL | 5 mg/mL | 0.50 mL | 1.00 mL | 50 units |
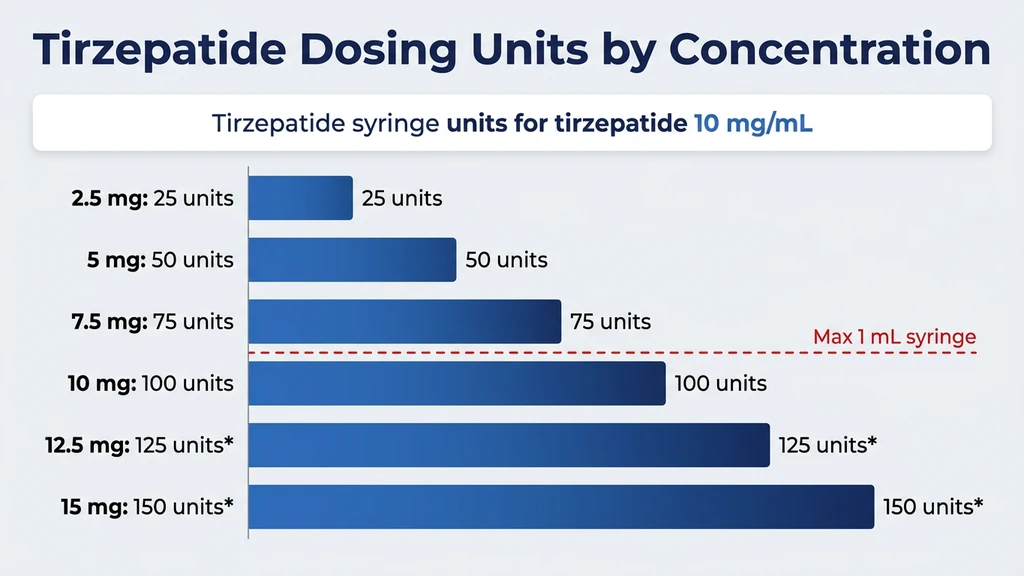
Recommended for 10mg vials: Add 1 mL for 10 mg/mL. This is the most common concentration dispensed by compounding pharmacies. At 10 mg/mL, the tirzepatide dosage chart in units shows clean conversion numbers: 2.5 mg = 25 units, 5 mg = 50 units.
A 10mg vial at 2.5 mg per week lasts 4 weeks. At 5 mg per week, it lasts 2 weeks. The 28-day stability window of reconstituted solution aligns well with the 4-week supply at the starting dose.
15 mg Vial
The 15mg vial suits users on mid-range doses of 5 to 7.5 mg per week.
| BAC Water Added | Concentration | 5 mg = | 7.5 mg = | Syringe Units per 5 mg |
|---|---|---|---|---|
| 1 mL | 15 mg/mL | 0.33 mL | 0.50 mL | 33 units |
| 1.5 mL | 10 mg/mL | 0.50 mL | 0.75 mL | 50 units |
| 3 mL | 5 mg/mL | 1.00 mL | 1.50 mL* | 100 units |
*Exceeds a 1 mL (100-unit) insulin syringe. Use a higher concentration or split into two draws.*
Recommended for 15mg vials: Add 1.5 mL for 10 mg/mL. This normalizes the concentration to the same value as a standard 10mg/1mL reconstitution, making dosing arithmetic consistent if you switch between vial sizes. At 5 mg per week, the vial provides 3 weeks of doses within the 28-day stability window.
30 mg Vial
The 30mg vial is designed for higher maintenance doses of 10 to 15 mg per week.
| BAC Water Added | Concentration | 10 mg = | 12.5 mg = | 15 mg = | Syringe Units per 10 mg |
|---|---|---|---|---|---|
| 1.5 mL | 20 mg/mL | 0.50 mL | 0.625 mL | 0.75 mL | 50 units |
| 2 mL | 15 mg/mL | 0.67 mL | 0.83 mL | 1.00 mL | 67 units |
| 3 mL | 10 mg/mL | 1.00 mL | 1.25 mL* | 1.50 mL* | 100 units |
*Exceeds a 1 mL (100-unit) insulin syringe. Use a higher concentration or split into two draws.*
Recommended for 30mg vials: Add 1.5 mL for 20 mg/mL. This keeps draw volumes manageable even at 15 mg doses (0.75 mL = 75 units). At 10 mg per week, the vial provides 3 weeks of doses. At 15 mg per week, it lasts 2 weeks.
If you are unsure which vial size to purchase, check the number of units for your specific dose with the Tirzepatide Dosage Calculator.
Master Dosing Conversion Table
This single table covers every standard tirzepatide dose at the four most common concentrations. Bookmark it. Print it. Tape it to your refrigerator.
All values are for a U-100 insulin syringe, where 100 units = 1 mL.
| Dose | 5 mg/mL | 10 mg/mL | 15 mg/mL | 20 mg/mL |
|---|---|---|---|---|
| 2.5 mg | 50 units (0.50 mL) | 25 units (0.25 mL) | 17 units (0.17 mL) | 12.5 units (0.125 mL) |
| 5 mg | 100 units (1.00 mL) | 50 units (0.50 mL) | 33 units (0.33 mL) | 25 units (0.25 mL) |
| 7.5 mg | 150 units* | 75 units (0.75 mL) | 50 units (0.50 mL) | 37.5 units (0.375 mL) |
| 10 mg | 200 units* | 100 units (1.00 mL) | 67 units (0.67 mL) | 50 units (0.50 mL) |
| 12.5 mg | 250 units* | 125 units* | 83 units (0.83 mL) | 62.5 units (0.625 mL) |
| 15 mg | 300 units* | 150 units* | 100 units (1.00 mL) | 75 units (0.75 mL) |
*Exceeds a 100-unit (1 mL) syringe. Use a higher concentration or split into two injections.*
The formula behind every number in this table: Units = (Dose in mg / Concentration in mg/mL) x 100. For example, 7.5 mg at 10 mg/mL: (7.5 / 10) x 100 = 75 units. For a detailed walkthrough of this calculation, see how many units is 2.5 mg of tirzepatide.
Use the Peptide Unit Converter to double-check any conversion before drawing your dose.
How to Draw Your Dose After Reconstitution
Reconstitution gets the solution into the vial. Drawing gets the right amount into your syringe. This second step is where most dosing errors happen.
Choosing the right insulin syringe:
| Syringe Size | Total Capacity | Best For | Smallest Graduation |
|---|---|---|---|
| 0.3 mL (30 units) | 30 units | Doses under 25 units | 0.5 units |
| 0.5 mL (50 units) | 50 units | Doses of 10 to 50 units | 1 unit |
| 1.0 mL (100 units) | 100 units | Doses of 25 to 100 units | 2 units |
Match the syringe to your draw volume. If your dose requires 25 units at 10 mg/mL (the 2.5 mg starting dose), a 0.3 mL or 0.5 mL syringe gives the clearest markings. A 1.0 mL syringe works but the 25-unit line sits only a quarter of the way up, making it harder to read precisely.
Drawing step by step:
- 1.Roll the reconstituted vial gently between your palms 5 to 10 times. This ensures uniform concentration throughout the solution.
- 2.Wipe the vial stopper with a fresh alcohol swab.
- 3.Pull air into the insulin syringe equal to your target draw volume. For 25 units, pull the plunger to 25 units of air.
- 4.Insert the needle through the stopper and push the air into the vial. This equalizes pressure and prevents vacuum buildup over multiple draws.
- 5.Invert the vial so the stopper faces down. Pull the plunger past your target by 5 to 10 units.
- 6.Tap the syringe barrel to move air bubbles toward the needle. Push the plunger slowly until it sits exactly at your target mark and the air is expelled.
- 7.Withdraw the needle from the vial.
This air-replacement technique prevents negative pressure from accumulating inside the vial. Without it, each successive draw becomes harder and pulls less liquid than intended. For complete injection technique, see the peptide injection guide.
Storage After Reconstitution
Proper storage determines whether your tirzepatide remains potent for the full 28-day window or degrades within a week.
Reconstituted solution (mixed with BAC water): - Refrigerate at 2 to 8 degrees Celsius (36 to 46 degrees Fahrenheit) - Store the vial upright with the stopper facing up - Protect from direct light - Stable for up to 28 days. See how long does tirzepatide last in the fridge for a full stability breakdown - Do not freeze reconstituted tirzepatide. Ice crystal formation denatures the peptide irreversibly
Unreconstituted powder (lyophilized): - Store in the freezer at -20 degrees Celsius for maximum shelf life (months to years) - Refrigerated storage at 2 to 8 degrees Celsius is acceptable for several months - Room temperature tolerance: 2 to 4 weeks without significant degradation - Keep the desiccant packet in the container to absorb moisture
Practical storage tips: - Store vials on a middle shelf of the refrigerator, not in the door. Door shelves experience temperature fluctuations of 5 to 10 degrees with each opening. - Use a dedicated container or small box to prevent the vial from being knocked over. - If you travel with reconstituted tirzepatide, use an insulated cooler bag with an ice pack. Keep the vial between 2 and 8 degrees Celsius. A car glove compartment in summer can exceed 60 degrees Celsius and will destroy the peptide in hours.
For comprehensive storage guidance covering all peptide types, read how to store peptides. For shelf life data by peptide, see how long do reconstituted peptides last.
Common Mistakes and How to Avoid Them
Five errors account for the vast majority of reconstitution problems with compounded tirzepatide. Each is preventable.
Mistake 1: Spraying water directly onto the powder cake. The force of the stream can partially denature the peptide by disrupting hydrogen bonds in the folded GLP-1/GIP agonist structure. The solution may look normal but deliver reduced potency. Fix: aim the needle at the glass wall and let the water trickle down slowly over 30 to 60 seconds.
Mistake 2: Shaking the vial to dissolve the powder. Shaking creates foam, introduces air, and subjects the peptide to mechanical stress. Tirzepatide is a 39-amino-acid peptide with a fatty acid sidechain (a C20 icosanoyl moiety) that makes it sensitive to agitation-induced aggregation. Fix: swirl gently. If the powder is stubborn, refrigerate the vial for 10 to 15 minutes and swirl again.
Mistake 3: Using the wrong water volume for the vial size. Adding 2 mL to a 30mg vial gives 15 mg/mL. Adding 2 mL to a 10mg vial gives 5 mg/mL. Same volume of water, completely different concentrations. If you follow a guide written for a different vial size, every injection will be off. Fix: always check the vial label for the peptide mass before calculating your water volume.
Mistake 4: Forgetting to label the vial. Reconstituted tirzepatide is a clear, colorless liquid. So is reconstituted semaglutide, BPC-157, and bacteriostatic water itself. An unlabeled vial is an accident waiting to happen. Fix: write the peptide name, concentration, and reconstitution date on the vial immediately after mixing. Use tape or a fine-point permanent marker.
Mistake 5: Using sterile water for a multi-dose vial. Sterile water has no antimicrobial preservative. After the first needle puncture, bacteria can enter and multiply unchecked. By the third or fourth draw, the solution may contain a clinically relevant bacterial load. Fix: always use bacteriostatic water for any vial you plan to draw from more than once. If you already reconstituted with sterile water, use the vial within 24 hours and discard the remainder.
Danger Scenarios: What Goes Wrong with Bad Math
Reconstitution errors produce silent dosing errors. You inject what appears to be the correct number of units, but the concentration is wrong and the actual dose is higher or lower than intended. With tirzepatide, which has a steep dose-response curve for gastrointestinal side effects, these errors carry real consequences.
Scenario 1: Half the water, double the dose. You have a 10mg vial. You intend to add 2 mL for 5 mg/mL but accidentally add only 1 mL. The actual concentration is 10 mg/mL. You draw 50 units thinking you are getting 2.5 mg. You actually inject 5.0 mg. That is double the starting dose and equivalent to jumping straight to week 5 of the standard titration. Expect severe nausea, vomiting, and possibly diarrhea lasting 48 to 72 hours. Clinical trial data from the SURMOUNT-1 study showed that gastrointestinal adverse events were significantly more common during dose escalation periods (Jastreboff et al., 2022, NEJM).
Scenario 2: Wrong vial assumption. You have a 30mg vial but follow instructions written for a 10mg vial. You add 1 mL of water thinking you are making 10 mg/mL. The actual concentration is 30 mg/mL. When you draw 25 units for what you believe is 2.5 mg, you inject 7.5 mg. That is three times your intended dose. At this level, the risk of severe gastrointestinal distress is high, and you may require medical attention for dehydration from persistent vomiting.
Scenario 3: Contaminated solution from improper sterile technique. You reconstitute with bacteriostatic water but skip the alcohol swab step. Over 3 weeks of use, bacteria introduced during the first needle puncture multiply to a level that causes injection-site infection. Symptoms include localized redness, swelling, warmth, and pain at the injection site. In severe cases, an abscess can form requiring incision and drainage.
The safeguard for all three: Always verify the vial label before adding water. Calculate or confirm using the Peptide Reconstitution Calculator. Write the concentration on the vial. Use clean technique every time.
Tirzepatide Reconstitution vs Semaglutide Reconstitution
If you have reconstituted semaglutide before, the process for tirzepatide is nearly identical. The mechanics (add water, aim at glass, swirl, refrigerate) do not change. The differences are practical, not procedural.
| Factor | Tirzepatide | Semaglutide |
|---|---|---|
| Mechanism | Dual GIP/GLP-1 receptor agonist | GLP-1 receptor agonist only |
| Common vial sizes | 5, 10, 15, 30 mg | 5, 10 mg |
| Standard reconstitution volume | 1 to 3 mL depending on vial | 1 to 2 mL depending on vial |
| Dose range (weekly) | 2.5 to 15 mg | 0.25 to 2.4 mg |
| Solution appearance | Clear, colorless to slightly yellow | Clear, colorless |
| Shelf life (reconstituted, BAC water) | 28 days at 2-8°C | 28 days at 2-8°C |
| Shake tolerance | Low (swirl only) | Low (swirl only) |
The most important difference is dose magnitude. Tirzepatide doses are roughly 2 to 6 times larger than semaglutide doses for equivalent clinical effect. This means tirzepatide vials tend to be larger (10 to 30 mg vs 5 to 10 mg for semaglutide), and the draw volumes per dose are correspondingly larger. If you are switching from semaglutide to tirzepatide, the semaglutide to tirzepatide switching guide covers dose equivalence and titration protocol.
The reconstitution math is the same for both: Concentration = mg / mL. The syringe reading technique is the same. The storage conditions are the same. If you can reconstitute one, you can reconstitute the other. For semaglutide-specific water volumes, see how much bacteriostatic water for semaglutide.
How Many Doses Per Vial?
This table shows how many weekly doses each vial size provides at standard tirzepatide titration doses. Use it to plan how many vials you need per month and to ensure you use the reconstituted solution within the 28-day stability window.
| Vial Size | Weekly Dose | Doses per Vial | Weeks of Supply | Within 28-Day Window? |
|---|---|---|---|---|
| 5 mg | 2.5 mg | 2 | 2 weeks | Yes |
| 10 mg | 2.5 mg | 4 | 4 weeks | Yes |
| 10 mg | 5 mg | 2 | 2 weeks | Yes |
| 15 mg | 5 mg | 3 | 3 weeks | Yes |
| 15 mg | 7.5 mg | 2 | 2 weeks | Yes |
| 30 mg | 10 mg | 3 | 3 weeks | Yes |
| 30 mg | 15 mg | 2 | 2 weeks | Yes |
Notice that every combination in this table falls within the 28-day stability window. This is by design. Tirzepatide vial sizes and standard doses align so that you use the entire vial before the reconstituted solution expires. If you take longer than 4 weeks to finish a vial, the solution may have lost potency. Discard any reconstituted solution older than 28 days regardless of how much remains.
Tirzepatide is administered as a once-weekly subcutaneous injection. The standard titration schedule starts at 2.5 mg per week for 4 weeks, then increases to 5 mg per week for another 4 weeks, with subsequent increases of 2.5 mg every 4 weeks up to a maximum of 15 mg per week (Mounjaro prescribing information, Eli Lilly). Your prescriber may adjust this schedule based on tolerability and response.
For a visual titration schedule with exact syringe units at every dose level, see the tirzepatide dosage chart in units.
Choosing the Right Syringe for Your Concentration
The syringe you use matters as much as the reconstitution itself. A syringe that is too large for your draw volume introduces measurement error. A syringe that is too small cannot hold the required volume.
Every insulin syringe is calibrated in "units." On a U-100 syringe, 100 units equals 1 mL. Each unit equals 0.01 mL. The markings printed on the barrel translate directly to volume. When your calculation says "draw 25 units," you are drawing 0.25 mL.
Syringe selection guide by dose and concentration:
| Your Dose | At 5 mg/mL | At 10 mg/mL | At 20 mg/mL | Recommended Syringe |
|---|---|---|---|---|
| 2.5 mg | 50 units | 25 units | 12.5 units | 0.5 mL (50-unit) |
| 5 mg | 100 units | 50 units | 25 units | 0.5 mL or 1.0 mL |
| 7.5 mg | 150 units* | 75 units | 37.5 units | 1.0 mL (100-unit) |
| 10 mg | 200 units* | 100 units | 50 units | 1.0 mL (100-unit) |
| 15 mg | 300 units* | 150 units* | 75 units | 1.0 mL (100-unit) |
*Exceeds syringe capacity. Use a higher concentration or split into two injections.*
At concentrations of 10 mg/mL and above, even the maximum 15 mg dose fits within a 1 mL syringe (75 units at 20 mg/mL). This is one reason compounding pharmacies favor 10 to 20 mg/mL as standard concentrations.
If your calculated draw volume falls below 10 units on any syringe, switch to a 0.3 mL (30-unit) syringe with half-unit markings. At volumes this small, each unit of error on the syringe represents a proportionally large dosing error. The Peptide Unit Converter shows exact unit counts for any concentration and dose combination.
Troubleshooting Common Problems
The powder will not dissolve. Set the vial upright in the refrigerator for 10 to 15 minutes. Then swirl again for 2 to 3 minutes. Tirzepatide lyophilized powder occasionally takes longer to dissolve, especially in vials that were exposed to temperature fluctuations during shipping. If clumps remain after 30 minutes of gentle swirling and cold rest, the peptide may have degraded. Contact the supplier before using it.
Foam on the surface of the solution. A thin layer of small bubbles is normal and dissipates within 5 to 10 minutes of undisturbed rest. A thick, persistent foam indicates the vial was shaken or the water was injected too forcefully. Let the vial sit undisturbed in the refrigerator for 15 minutes. Draw from beneath the foam layer. The peptide in the foam is likely partially denatured and should not be injected.
The solution looks cloudy or has visible particles. Discard the vial. Cloudiness in a reconstituted peptide solution can indicate bacterial contamination, peptide aggregation from improper handling, or a degraded product. Do not attempt to filter and use a cloudy solution. A fresh vial reconstituted with proper technique will always be clear.
Slight yellow tint to the solution. A very faint yellow color is within the normal range for reconstituted tirzepatide, according to the Mounjaro prescribing information. This differs from semaglutide, which should be completely colorless. If the yellow tint is pronounced or the solution appears amber or brown, discard it.
Rubber stopper fragments in the vial. This happens when the needle cores the stopper. Prevention: insert at a 45-degree angle with the bevel facing up before straightening to 90 degrees. If you spot fragments, draw the solution through a 0.22 micron syringe filter before each injection, or discard the vial and reconstitute a fresh one.
Reconstitution Tips for Beginners
If this is your first time reconstituting any peptide, three habits will prevent virtually every common error.
Habit 1: Read the vial label twice. Before drawing bacteriostatic water, confirm the peptide name and the mass printed on the label. A 10mg vial and a 30mg vial of tirzepatide look identical from the outside. The only difference is the number on the label. Reading it twice takes 5 seconds and eliminates the most dangerous reconstitution mistake.
Habit 2: Write on the vial before you put it in the refrigerator. The moment you finish swirling, pick up the marker and write the concentration and date. Do not tell yourself you will remember. In a refrigerator with multiple vials, an unlabeled clear solution is indistinguishable from every other unlabeled clear solution.
Habit 3: Use a calculator for every new vial. Even if you have reconstituted the same vial size 10 times, confirm the math. Complacency is the root of dosing errors. The Peptide Reconstitution Calculator takes less time than second-guessing yourself.
For a general reconstitution guide that covers all peptide types, see how to reconstitute peptides. For GHK-Cu specifically (which has a unique solvent restriction), see how to reconstitute GHK-Cu. If you plan to reconstitute the newer triple agonist, see how to reconstitute retatrutide. The same fundamental technique applies to every lyophilized peptide: clean, draw, aim at the wall, swirl, label, refrigerate.
Frequently Asked Questions
How much bacteriostatic water do I add to a 10mg tirzepatide vial?
Add 1 mL for a 10 mg/mL concentration, which is the most common standard. At this concentration, 2.5 mg equals 25 units and 5 mg equals 50 units on a U-100 insulin syringe. Confirm any other vial size with the peptide reconstitution calculator.
How long does reconstituted tirzepatide last in the fridge?
Reconstituted tirzepatide mixed with bacteriostatic water remains stable for 28 days when stored at 2 to 8 degrees Celsius. Do not freeze it after reconstitution. If the solution becomes cloudy before 28 days, discard it. See how long do reconstituted peptides last for the full stability breakdown across peptides.
Can I use sterile water instead of bacteriostatic water for tirzepatide?
You can, but the vial must be used within 24 hours because sterile water contains no antimicrobial preservative. Bacteriostatic water (preserved with 0.9% benzyl alcohol) allows multi-dose use over 28 days. For a fuller comparison, see bacteriostatic water vs sterile water.
How many units is 2.5 mg of tirzepatide at 10 mg/mL?
At 10 mg/mL, 2.5 mg of tirzepatide equals 25 units on a U-100 insulin syringe. The formula is (2.5 mg / 10 mg per mL) times 100 = 25 units. At 5 mg/mL, the same dose is 50 units. For a complete unit chart at every dose, see tirzepatide dosage chart in units.
What happens if I add too much water to my tirzepatide vial?
Adding extra water does not destroy the peptide. It lowers the concentration, which means you draw a larger volume per dose. Recalculate using the formula: new concentration equals vial mass divided by total water added. For a 10mg vial with 3 mL of water, the concentration is 3.33 mg/mL. The tirzepatide dosage calculator handles the adjusted math.
Do I need to shake the vial to dissolve tirzepatide?
Never shake a tirzepatide vial. Shaking causes foaming and can denature the peptide through mechanical stress. Swirl gently for 1 to 3 minutes. If powder remains, refrigerate the vial for 10 to 15 minutes and swirl again. The same swirl-only rule applies to every peptide: see how to reconstitute peptides.
Can I reconstitute tirzepatide and semaglutide with the same bacteriostatic water bottle?
Yes. A single 30 mL bottle of bacteriostatic water works for reconstituting any peptide, including semaglutide. Clean the BAC water stopper with an alcohol swab before each draw and use a fresh syringe for each vial. One bottle provides enough water for dozens of reconstitutions across peptides.
What is the best concentration for compounded tirzepatide?
A concentration of 10 mg/mL is the most practical for the majority of users. At this concentration, the 2.5 mg starting dose requires 25 units and the 10 mg maintenance dose requires 100 units, both fitting standard insulin syringes. Concentrations of 20 mg/mL suit higher doses above 10 mg per week. See the tirzepatide dosage calculator for any combination.
The Bottom Line
Reconstituting tirzepatide follows the same five steps as any lyophilized peptide: clean the stoppers, draw bacteriostatic water, inject slowly against the glass wall, swirl gently, and refrigerate. The entire process takes under five minutes.
The critical variable is getting the concentration right. Confirm the vial size on the label, choose your water volume from the tables above, and write the resulting concentration on the vial immediately after mixing. When in doubt, verify with the Peptide Reconstitution Calculator.
For weekly dosing schedules and titration protocols, see the tirzepatide dosage chart in units. For unit conversions at your specific concentration, use the Tirzepatide Dosage Calculator. For the full pharmacology profile, visit the tirzepatide peptide page.
Related articles: - Is Reconstitution Solution the Same as Bacteriostatic Water?: comparing diluent types for peptide mixing - Bacteriostatic Water vs Sterile Water: which solvent to use and why it matters - Does Tirzepatide Expire?: shelf life for lyophilized vs reconstituted tirzepatide - How to Take BPC-157: reconstitution and injection guide for another common peptide - Does Tirzepatide Burn Fat?: what to expect once you start dosing - Does Tirzepatide Cause Headaches?: side effects during the first weeks - Can You Drink Alcohol on Tirzepatide?: safety considerations once you begin treatment - How to Inject Tirzepatide: injection technique after reconstitution - Is Compound Tirzepatide Safe?: safety assessment for compounded tirzepatide products - Tirzepatide Injection Site Reaction: preventing and managing injection site issues
Related Articles
How to Reconstitute Retatrutide
How to reconstitute retatrutide step by step for 5mg, 10mg, and 20mg vials. Concentration tables, BAC water volumes, syringe units per dose, and storage guide.
Cheapest Tirzepatide: Every Route Priced (2026)
The cheapest tirzepatide in 2026: manufacturer self-pay vials from $299/month, $25 insured copays, true cost per milligram, and why compounded copies ended.
What to Eat on Tirzepatide: Diet Guide
What to eat on tirzepatide to minimize nausea, prevent muscle loss, and maximize results. Protein targets, meal plans, foods to avoid, and hydration.
Does Tirzepatide Expire? Shelf Life
Tirzepatide expires in 24-36 months as powder and 28 days once reconstituted. Learn storage temps, degradation signs, and potency loss timelines.