You are six weeks into tirzepatide and down 14 pounds. A colleague's wedding is Saturday. The open bar starts at six. One question stands between you and a champagne toast.
There is no absolute contraindication to drinking alcohol while taking tirzepatide. The FDA prescribing information for Mounjaro and Zepbound does not list alcohol as a prohibited substance. But "not prohibited" and "safe without consequence" are different categories entirely. Alcohol interacts with tirzepatide through at least four distinct pathways: altered tolerance, hypoglycemia risk, prolonged gastric retention, and compounded dehydration. Clinical reports and pharmacological evidence suggest that most tirzepatide users who continue drinking experience meaningfully worse outcomes than those who abstain (Jastreboff et al., 2022).
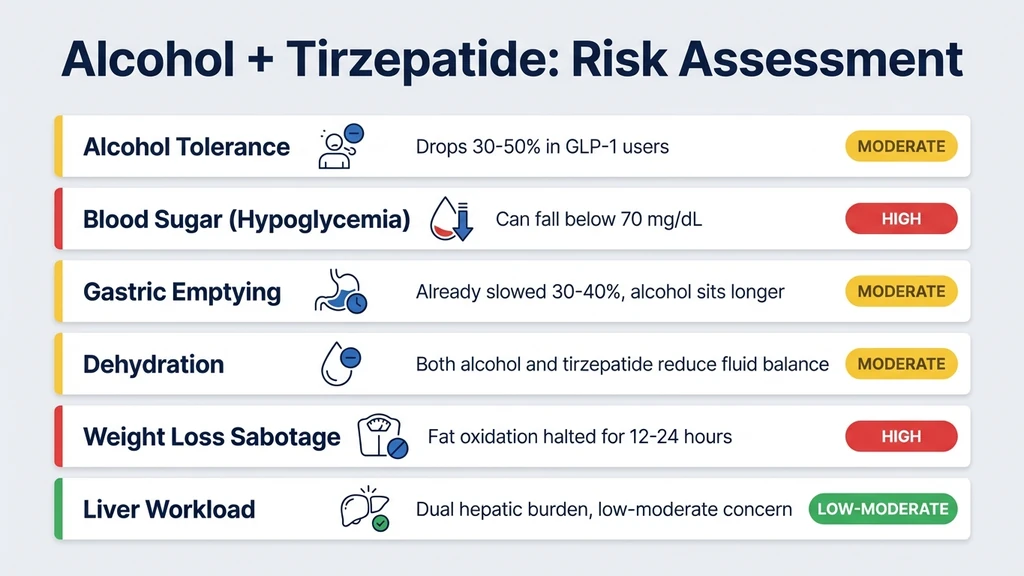
| Factor | What Happens | Risk Level |
|---|---|---|
| Alcohol tolerance | Drops 30-50% in many GLP-1 users | Moderate |
| Blood sugar | Can fall below 70 mg/dL, especially with meals skipped | High if diabetic |
| Gastric emptying | Already slowed 30-40%; alcohol sits longer | Moderate |
| Dehydration | Both alcohol and tirzepatide reduce fluid balance | Moderate |
| Weight loss | Alcohol halts fat oxidation for 12-24 hours | Sabotage |
| Liver workload | Dual hepatic burden from ethanol + drug metabolism | Low-Moderate |
For dosing protocols, see our tirzepatide dosage chart. For broader safety information, see our peptide safety guide.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
The Short Answer: Not Prohibited, But Not Without Risk
Tirzepatide's prescribing label does not ban alcohol. No clinical trial has specifically studied the combination in a controlled setting. The absence of data is not the same as evidence of safety.
What exists is a growing body of pharmacological reasoning, post-marketing reports, and patient experience. GLP-1 receptor agonists as a class alter how the body handles ethanol. Semaglutide users report the same patterns. Retatrutide users, working with a triple-agonist mechanism, report them even more intensely.
The risks fall into two categories. The first is acute: what happens the night you drink. The second is chronic: what happens to your weight loss, liver health, and treatment trajectory over weeks and months of continued drinking. Both categories deserve attention.
Why Alcohol Hits Harder on Tirzepatide
Thousands of GLP-1 agonist users report the same experience: two drinks feel like four. A glass of wine that previously caused a mild buzz now produces slurred speech and unsteadiness. This is not psychological. The mechanism is pharmacological, and it operates through at least two pathways.
Delayed Gastric Emptying Changes Absorption Kinetics
Tirzepatide slows gastric emptying by 30-40% through GLP-1 receptor activation in the vagal nerve pathways (Nauck et al., 2021). Under normal conditions, alcohol moves from the stomach to the small intestine within 15-30 minutes, where 80% of absorption occurs. When gastric emptying is slowed, alcohol pools in the stomach longer.
This creates an unpredictable absorption curve. Instead of a smooth rise in blood alcohol over 30-60 minutes, the alcohol may sit in the stomach for an extended period and then release into the small intestine in a larger bolus when gastric motility briefly increases. The result is a delayed but steeper peak in blood alcohol concentration.
A person who previously reached a blood alcohol concentration of 0.06% after two glasses of wine might now hit 0.08-0.10% from the same amount, simply because the absorption pattern has changed. The total ethanol consumed is identical. The peak concentration is higher. The subjective experience is dramatically different.
Reduced Food Intake Removes the Buffer
Tirzepatide reduces caloric intake by 20-30% at therapeutic doses. Most users eat smaller meals. Many skip meals entirely, particularly breakfast and lunch. Food in the stomach slows alcohol absorption and reduces peak blood alcohol concentration by as much as 40%.
A user who previously drank two cocktails alongside a full dinner now drinks two cocktails with a small appetizer or nothing at all. The alcohol arrives at the small intestine with minimal food buffer. Peak blood alcohol rises faster and higher.
This combination of delayed gastric emptying and reduced food intake explains why so many tirzepatide users feel intoxicated faster and more intensely than they expect. The effect is consistent across the GLP-1 class. Users of semaglutide report identical patterns, as documented in patient forums and post-marketing surveillance data.
Hypoglycemia: The Most Dangerous Acute Risk
Alcohol suppresses hepatic gluconeogenesis, the liver's production of new glucose from non-carbohydrate sources. This process accounts for roughly 50% of fasting glucose production. Tirzepatide independently lowers blood glucose through enhanced insulin secretion and improved insulin sensitivity.
When both act simultaneously, blood sugar can drop to dangerous levels. The clinical threshold for hypoglycemia is below 70 mg/dL. Severe hypoglycemia, defined as requiring assistance from another person, begins below 54 mg/dL. At 40 mg/dL, confusion, seizures, and loss of consciousness become possible (Cryer, 2015).
Who Faces the Highest Risk
The risk is highest for tirzepatide users who also take insulin or sulfonylureas (glipizide, glimepiride). These medications drive blood sugar down through mechanisms that do not respond to falling glucose levels. Add alcohol's suppression of gluconeogenesis and tirzepatide's own glucose-lowering effect, and the result can be a rapid slide from 90 mg/dL to 50 mg/dL over 2-3 hours.
The SURPASS clinical program reported hypoglycemia in 0.4-0.9% of tirzepatide users on monotherapy and 10-14% of those co-prescribed sulfonylureas (Frias et al., 2021). Alcohol amplifies these rates. Users without diabetes face lower but not zero risk, particularly if they skip meals while drinking.
A Scenario Worth Understanding
A 42-year-old woman takes tirzepatide 10 mg for weight loss. She skips dinner and drinks three glasses of wine over 4 hours at a work event. By 11 PM, she feels dizzy and confused. Her blood sugar has dropped to 52 mg/dL. The symptoms mimic alcohol intoxication: slurred speech, unsteadiness, impaired judgment. Her friends assume she has had too much to drink. The actual problem is hypoglycemia compounded by alcohol.
The danger is that hypoglycemia symptoms and alcohol intoxication symptoms overlap almost completely. Sweating, confusion, poor coordination, and drowsiness describe both conditions. Without a glucose meter, distinguishing one from the other is nearly impossible. This masking effect is the single most dangerous aspect of combining alcohol with tirzepatide.
Protective Measures
Always eat a meal containing protein and complex carbohydrates before or during drinking. Never drink on an empty stomach while taking tirzepatide. If you take insulin or a sulfonylurea alongside tirzepatide, consider checking blood glucose before drinking, 2 hours into drinking, and before bed. Keep glucose tablets or juice accessible. Set a firm limit of 1-2 drinks per occasion.
These precautions matter more on tirzepatide than off it. The margin between "pleasantly buzzed" and "medically hypoglycemic" narrows significantly when GLP-1 agonists and alcohol act together. For dosage guidance, use our tirzepatide dosage calculator.
Prolonged Intoxication and Delayed Recovery
Under normal physiology, the liver metabolizes alcohol at a steady rate of approximately one standard drink per hour. This rate is not significantly altered by tirzepatide. What changes is the duration of the subjective experience.
Because gastric emptying is slowed, alcohol continues entering the bloodstream for a longer period after the last drink. A person who stops drinking at midnight may still be absorbing alcohol at 2 AM. The hangover arrives later, lasts longer, and compounds with tirzepatide's own gastrointestinal effects.
Nausea is the most common side effect of GLP-1 agonists, affecting 40-45% of semaglutide users during dose titration. Tirzepatide causes nausea in 12-18% at the 5-10 mg range and up to 24% at 15 mg. Alcohol-induced nausea on top of medication-induced nausea creates a compounding effect that many users describe as the worst hangover of their lives after just 2-3 drinks.
Vomiting introduces an additional concern. Tirzepatide is administered as a weekly subcutaneous injection and is not affected by vomiting. But vomiting accelerates dehydration, depletes electrolytes, and can damage the esophageal lining. Users who experience constipation on tirzepatide may find that alcohol-triggered vomiting and subsequent dehydration worsen their GI symptoms for days afterward.
The Liver Burden: Two Metabolic Demands at Once
The liver processes both alcohol and tirzepatide. Ethanol metabolism occurs primarily through alcohol dehydrogenase and the cytochrome P450 system (specifically CYP2E1). Tirzepatide is a peptide and is not metabolized through cytochrome P450 pathways. It is cleared through proteolytic degradation, the same process that breaks down endogenous proteins.
This means direct pharmacokinetic competition at the enzyme level is unlikely. The concern is broader: overall hepatic workload.
Chronic alcohol use elevates liver enzymes (ALT, AST) and promotes fatty liver disease. An estimated 25% of adults in the United States have non-alcoholic fatty liver disease (NAFLD). Many people starting tirzepatide for weight loss already have some degree of hepatic steatosis. Adding regular alcohol consumption to this baseline elevates the overall metabolic demand on a liver that may already be stressed.
Tirzepatide actually improves liver fat in most users. The SURPASS-3 MRI substudy found a 74% relative reduction in liver fat with tirzepatide 15 mg after 52 weeks. Alcohol directly opposes this benefit. Ethanol metabolism generates acetaldehyde and promotes triglyceride synthesis in hepatocytes. Drinking regularly while taking tirzepatide undermines one of the drug's most significant metabolic benefits.
For broader safety context, review our peptide safety guide. If considering switching from semaglutide to tirzepatide, note that alcohol interaction profiles are similar across the GLP-1 class.
Dehydration: A Compounding Problem
Alcohol is a diuretic. It suppresses antidiuretic hormone (vasopressin), causing the kidneys to excrete more water than the volume of fluid consumed. A standard beer produces a net fluid loss of approximately 100-150 mL beyond the volume of the beer itself.
Tirzepatide does not directly cause dehydration. But it creates conditions that lead to inadequate fluid intake. Reduced appetite means less food-derived water (food provides roughly 20% of daily fluid intake). Nausea reduces the desire to drink fluids. Constipation, which affects 6-12% of tirzepatide users, worsens when hydration drops.
The combined effect: a tirzepatide user who drinks 3-4 alcoholic beverages may become significantly more dehydrated than they would have pre-treatment. Dehydration worsens hangovers, impairs kidney function, concentrates electrolytes, and can trigger headaches and fatigue that persists for 24-48 hours.
Practical countermeasure: alternate every alcoholic drink with a full glass of water. Aim for at least 16 ounces of water before bed after any drinking occasion. On tirzepatide, the baseline hydration target should be 80-100 ounces of water daily even without alcohol.
Alcohol and Weight Loss: The Numbers That Matter
This is where occasional drinking becomes a strategic decision rather than a safety one. The numbers are stark.
Alcohol contains 7 calories per gram, nearly double the 4 calories per gram in protein or carbohydrates. A standard glass of wine delivers 120-150 calories. A craft IPA contains 200-300 calories. A margarita can exceed 400 calories. Three drinks at a wedding deliver 400-900 calories, potentially erasing a full day of the caloric deficit tirzepatide creates.
But caloric content is only half the problem. The other half is metabolic prioritization.
Alcohol Halts Fat Burning
When ethanol enters the bloodstream, the liver treats it as a priority substrate. All other metabolic processes, including fat oxidation, are suppressed until ethanol is fully metabolized. A landmark study found that alcohol reduces whole-body fat oxidation by 73% for the duration of ethanol metabolism (Siler et al., 1999).
For a person consuming 3 standard drinks, ethanol metabolism takes approximately 3-5 hours. During this window, the body burns essentially zero fat regardless of how large a caloric deficit tirzepatide has created. The fat-burning machinery shuts down entirely.
The practical impact: a tirzepatide user who drinks every Friday and Saturday loses approximately 2 of 7 weekly fat-burning windows. Over a 12-week treatment course, that amounts to 24 days of suppressed fat oxidation. The difference between 5% and 8% total body weight loss may come down to this single variable.
Alcohol Increases Food Intake
Alcohol lowers inhibition and stimulates appetite through GABA pathway activation. The same user who carefully avoids high-calorie foods all week orders nachos, pizza, and dessert after three drinks. A 2021 meta-analysis found that acute alcohol consumption increases food intake by an average of 300-400 additional calories per drinking session beyond the calories in the alcohol itself.
Tirzepatide's appetite suppression is one of its most powerful mechanisms. The drug reduces hunger hormone signaling and increases satiety signaling. Alcohol temporarily overrides both effects. For the 4-6 hours of a drinking session, the appetite control that tirzepatide provides is partially or fully negated.
Use our peptide interaction checker to review potential compound interactions before combining any substances with your protocol.
The 'Ozempic Effect': Why Some Users Lose Interest in Alcohol
A striking phenomenon has emerged since GLP-1 agonists became widely prescribed. Many users report a spontaneous and dramatic reduction in the desire to drink alcohol. This has been nicknamed the "Ozempic effect" in popular media, though it occurs with tirzepatide, semaglutide, and retatrutide alike.
The effect is not anecdotal. Preclinical research has consistently demonstrated that GLP-1 receptor agonists reduce alcohol intake in rodent models. A 2023 systematic review identified 15 preclinical studies showing that GLP-1 receptor agonists reduced alcohol consumption by 30-50% in rodents trained to self-administer ethanol (Klausen et al., 2022).
The mechanism involves dopamine signaling. Alcohol activates the mesolimbic dopamine pathway, the brain's reward circuit. GLP-1 receptors are expressed in the nucleus accumbens and ventral tegmental area, two key nodes of this circuit. When tirzepatide activates these receptors, it appears to modulate the dopamine response to alcohol, making drinking feel less rewarding.
What Users Report
Surveys of GLP-1 agonist users suggest that 30-50% notice a meaningful reduction in alcohol cravings. Some describe forgetting to finish a drink. Others say the taste of alcohol becomes unpleasant. A smaller subset reports complete loss of interest in drinking for the first time in decades.
The effect is variable. Not everyone experiences it. Among those who do, the onset typically occurs within the first 4-8 weeks of treatment. There are currently no human randomized controlled trials specifically testing GLP-1 agonists for alcohol use disorder, though several are underway. Preliminary human data from a semaglutide trial showed a 25% reduction in heavy drinking days compared to placebo.
For users hoping to reduce their alcohol intake, tirzepatide's neurological effects may provide an unexpected benefit. For users who enjoy social drinking and want to continue, the reduced desire may require conscious effort to overcome, which raises its own question about whether the craving reduction is worth ignoring.
Safe Drinking Guidelines While on Tirzepatide

No physician can endorse drinking while taking a GLP-1 agonist in the same way they might say "exercise for 30 minutes." The safest approach is abstinence during treatment. But for users who choose to drink occasionally, harm reduction is the practical alternative.
Before Drinking
Eat a full meal containing at least 20 grams of protein and complex carbohydrates 1-2 hours before your first drink. This slows alcohol absorption and provides a glucose buffer against hypoglycemia. If you take insulin or a sulfonylurea, check your blood sugar. A pre-drinking glucose below 100 mg/dL warrants extra caution.
Time your tirzepatide injection away from planned drinking events. If you inject on Friday, consider shifting to Saturday morning or Sunday. There is no pharmacokinetic interaction that changes based on injection timing — tirzepatide stays in your system for weeks with a half-life of about 5 days — but users report feeling fewer GI side effects when the injection and alcohol are separated by 24-48 hours.
While Drinking
Set a firm limit of 1-2 standard drinks. A standard drink is 12 oz beer (5% ABV), 5 oz wine, or 1.5 oz spirits. Alternate every alcoholic drink with a full glass of water. Avoid sugary cocktails: the combination of high sugar content and alcohol creates larger blood glucose swings.
Drink slowly. With delayed gastric emptying, the intoxication you feel at 9 PM may not reflect your peak blood alcohol level, which could arrive at 10:30 PM. Front-loading drinks in the first hour is particularly risky on tirzepatide because the delayed absorption curve means the full effect has not yet materialized.
Monitor how you feel compared to your pre-tirzepatide baseline. If one drink produces effects that previously required two or three, your tolerance has shifted. Respect the new threshold.
After Drinking
Drink at least 16-20 ounces of water before bed. Eat a small snack containing carbohydrates to maintain blood glucose overnight. Set an alarm to check blood sugar during the night if you are diabetic and took insulin earlier in the day.
The next morning, prioritize hydration, electrolytes, and a balanced meal. Do not skip your next tirzepatide dose because of a hangover. Consistency with weekly injections matters more for treatment outcomes than avoiding a single overlapping day. Use our semaglutide dosage calculator if you are considering switching to semaglutide and want to compare dosing schedules.
Danger Scenarios: When Drinking Becomes a Medical Emergency
Most tirzepatide users who have a drink or two at dinner will not experience a medical emergency. But certain scenarios elevate risk significantly.
Binge Drinking on a Fasting Day
A 35-year-old man on tirzepatide 15 mg has not eaten since the previous night. He attends a party and drinks 5 beers over 3 hours on an empty stomach. His blood sugar drops from 88 mg/dL to 48 mg/dL. He becomes confused and combative. Friends call an ambulance. Emergency room staff administer IV dextrose and fluids. His blood alcohol level is 0.14%, significantly higher than expected from 5 beers, because delayed gastric emptying concentrated the absorption window and no food buffer existed.
This scenario is preventable. Eating before drinking and limiting intake to 1-2 drinks eliminates the worst-case outcome.
Alcohol Combined with Sulfonylureas and Tirzepatide
Sulfonylureas force insulin secretion regardless of blood glucose level. Alcohol blocks gluconeogenesis. Tirzepatide enhances endogenous insulin release. Three glucose-lowering forces acting simultaneously can produce severe hypoglycemia below 40 mg/dL, a level associated with seizures, loss of consciousness, and in rare cases, death.
The SURPASS trials documented clinically significant hypoglycemia (below 54 mg/dL) in 10-14% of participants taking tirzepatide with a sulfonylurea. Adding alcohol to this combination creates an unacceptable risk profile. Users on triple therapy (tirzepatide + sulfonylurea + alcohol) should consider eliminating one variable entirely.
Driving After Drinking on Tirzepatide
The altered absorption kinetics matter here. A driver who waits 2 hours after their last drink may still be well above the legal blood alcohol limit of 0.08% because gastric emptying delayed the absorption curve. The "one hour per drink" rule of thumb is unreliable on GLP-1 agonists. Peak intoxication may occur 60-90 minutes later than expected.
Rideshare or a designated driver is not optional. It is the only responsible choice when delayed absorption makes self-assessment of intoxication unreliable.
What the Research Shows
No published randomized controlled trial has specifically studied the tirzepatide-alcohol interaction in humans. The evidence base draws from related areas.
SURMOUNT-1 (Jastreboff et al., 2022) 2,539 participants. Alcohol was not excluded. GI adverse events (nausea, diarrhea, constipation) were the most common side effects but were not stratified by alcohol consumption. The absence of specific alcohol safety warnings in the study conclusions suggests no acute safety signals were detected during the 72-week trial (PubMed).
GLP-1 Agonists and Alcohol: Preclinical Evidence (Klausen et al., 2022) Systematic review of 15 studies. GLP-1 receptor agonists consistently reduced alcohol intake by 30-50% in rodent models. The mechanism involves modulation of mesolimbic dopamine signaling. Alcohol's rewarding properties are blunted by GLP-1 receptor activation (PubMed).
Gastric Emptying Mechanism (Nauck et al., 2021) GLP-1 receptor agonists slow gastric emptying by 30-40% through vagal nerve pathways. This delay alters the absorption kinetics of orally consumed substances, including alcohol. The effect is strongest during early treatment and partially attenuates over weeks (PubMed).
Alcohol and Fat Oxidation (Siler et al., 1999) Eight healthy volunteers. Alcohol reduced whole-body fat oxidation by 73% and lipid oxidation by 79% for the duration of ethanol metabolism. This study explains why even moderate drinking significantly impairs the fat loss that tirzepatide promotes (PubMed).
Hypoglycemia Mechanisms (Cryer, 2015) Comprehensive review of hypoglycemia pathophysiology. Alcohol suppresses hepatic gluconeogenesis, the primary defense against falling blood sugar during fasting. Combined with insulin secretagogues or exogenous insulin, alcohol-induced hypoglycemia can be severe and prolonged (PubMed).
For a comparison of tirzepatide with related compounds, see our retatrutide vs tirzepatide guide. For alcohol interactions with other peptides, see our BPC-157 and alcohol article.
Related Side Effects and Considerations
Does Tirzepatide Cause Hair Loss? Rapid weight loss and nutritional deficiencies drive telogen effluvium during GLP-1 agonist treatment. The same pattern occurs with semaglutide-related hair loss. Alcohol depletes B vitamins and zinc, both critical for hair follicle health. Drinking while on tirzepatide may accelerate hair thinning in susceptible individuals.
Does Tirzepatide Cause Constipation? Alcohol-induced dehydration worsens constipation. Tirzepatide already slows gut transit by 30-40%. Adding a dehydrating agent to a system with reduced motility compounds the problem. Extra water on drinking days is essential.
Does Semaglutide Cause Fatigue? Hangovers are worse on GLP-1 agonists. Fatigue from alcohol-induced dehydration and poor sleep quality stacks with the tiredness some tirzepatide users experience during dose titration. For a timeline of when these GI effects resolve, see how long do semaglutide side effects last. The compounded effect can last 48-72 hours after moderate drinking.
Does Semaglutide Cause Nausea? Nausea is the most common GI side effect across the GLP-1 class. Alcohol-induced nausea on top of medication-induced nausea produces severe discomfort that users consistently describe as disproportionate to the amount consumed.
For a complete overview of tirzepatide dosing and units, see our tirzepatide dosage chart and semaglutide dosage chart in mL.
Frequently Asked Questions
How many drinks can you safely have on tirzepatide?
Most healthcare providers recommend limiting intake to 1-2 standard drinks per occasion. A standard drink equals 12 oz beer, 5 oz wine, or 1.5 oz spirits. Staying at 1 drink is the lowest-risk option. With delayed gastric emptying slowing absorption by 30-40%, even 2 drinks can produce effects equivalent to 3-4 drinks pre-treatment.
Does tirzepatide lower alcohol tolerance?
Yes. An estimated 30-50% of GLP-1 agonist users report noticeably lower alcohol tolerance. The mechanism involves delayed gastric emptying that alters absorption kinetics, plus reduced food intake that removes the buffer effect of a full stomach. Peak blood alcohol concentration from 2 drinks may reach 0.08-0.10% instead of the expected 0.04-0.06%.
Can drinking on tirzepatide cause hypoglycemia?
It can, particularly in users taking sulfonylureas or insulin alongside tirzepatide. Alcohol suppresses hepatic gluconeogenesis, and blood sugar can drop below 54 mg/dL. The SURPASS trials reported hypoglycemia in 10-14% of users on combination therapy. Always eat a meal containing 20+ grams of protein and carbohydrates before drinking.
Will alcohol stop tirzepatide from working?
Alcohol does not block tirzepatide's mechanism at the receptor level. The drug continues activating GLP-1 and GIP receptors regardless of drinking. But alcohol undermines weight loss results by adding 7 calories per gram, halting fat oxidation by up to 73%, and stimulating an additional 300-400 calories of food intake per drinking session.
How long should you wait to drink after a tirzepatide injection?
There is no mandatory waiting period. Tirzepatide has a half-life of approximately 5 days, meaning it is always active during weekly dosing. However, many users report that GI side effects like nausea peak 24-48 hours after injection. Spacing your injection and drinking by at least 48 hours reduces the chance of compounded nausea and vomiting.
Does tirzepatide reduce alcohol cravings?
Preclinical data from 15 studies shows GLP-1 receptor agonists reduce alcohol consumption by 30-50% in animal models. Surveys suggest 30-50% of human users notice reduced desire to drink. The mechanism involves GLP-1 receptor modulation of dopamine signaling in the brain's reward circuit, specifically the nucleus accumbens and ventral tegmental area.
Is wine safer than beer or spirits on tirzepatide?
No type of alcohol is inherently safer. The risk depends on total ethanol consumed, not the source. One 5 oz glass of wine, one 12 oz beer, and one 1.5 oz shot of spirits all contain approximately 14 grams of pure ethanol. Sugary cocktails carry additional risk because high sugar content creates larger blood glucose swings alongside the hypoglycemia risk.
Can you drink alcohol while taking Mounjaro or Zepbound?
Mounjaro and Zepbound are both brand names for tirzepatide. The same precautions apply to both. Neither prescribing label lists alcohol as a contraindication, but both carry warnings about hypoglycemia risk with insulin or sulfonylureas. The 30-40% delay in gastric emptying affects alcohol absorption identically regardless of which brand you use.
The Bottom Line
Alcohol is not contraindicated with tirzepatide. No clinical trial has identified a dangerous pharmacokinetic interaction. But the pharmacological reality is unfavorable at every level: altered tolerance, hypoglycemia risk, prolonged intoxication, dehydration, suppressed fat oxidation, and undermined weight loss.
The safest approach is abstinence during active treatment. For users who choose to drink occasionally, limiting intake to 1-2 standard drinks, eating a full meal beforehand, alternating with water, and avoiding driving resolve most acute risks.
Many users find the decision made for them. GLP-1 receptor activation in the brain's reward circuitry reduces alcohol's appeal in 30-50% of users. The champagne toast at that wedding may not sound as appealing as it did before you started tirzepatide.
Use our tirzepatide dosage calculator to plan your protocol. For interaction concerns, check our peptide interaction checker. For a comparison of GLP-1 options, see retatrutide vs tirzepatide.
Related articles: - Does Tirzepatide Burn Fat? — alcohol blocks 73% of the fat oxidation tirzepatide enables - Why Am I Not Losing Weight on Semaglutide? — alcohol is reason #7 for GLP-1 weight loss stalls - Does Tirzepatide Cause Headaches? — dehydration from alcohol compounds headache risk - Does Tirzepatide Cause Diarrhea? — alcohol worsens GI side effects - How Does Retatrutide Work? — the next-generation triple agonist - How to Reconstitute Tirzepatide — preparation guide for research peptide users - Does Tirzepatide Expire? — shelf life and storage - Tirzepatide Injection Site Reaction — injection site management during treatment - Is Compound Tirzepatide Safe? — safety considerations for compounded products
Explore all peptide profiles and safety tools at PeptidesExplorer.
Related Articles
Is Compounded Tirzepatide Safe?
Is compounded tirzepatide safe? Learn FDA 503A/503B rules, quality risks, how to verify a compounding pharmacy, and brand vs compounded differences.
Can You Drink on Semaglutide? Risks
Can you drink on semaglutide? No ban, but risks include hypoglycemia, prolonged intoxication, 73% fat-burn suppression, and worse GI side effects.
Does Tirzepatide Cause Hair Loss?
Tirzepatide-related hair thinning affects 5.7% of users at the highest dose. Learn why it happens, how it compares to semaglutide, and how to minimize it.
Does Compounded Tirzepatide Work? Real Data
Does compounded tirzepatide work? Review SURMOUNT data, salt form differences (base, acetate, sodium), potency gaps, and FDA status in 2026.