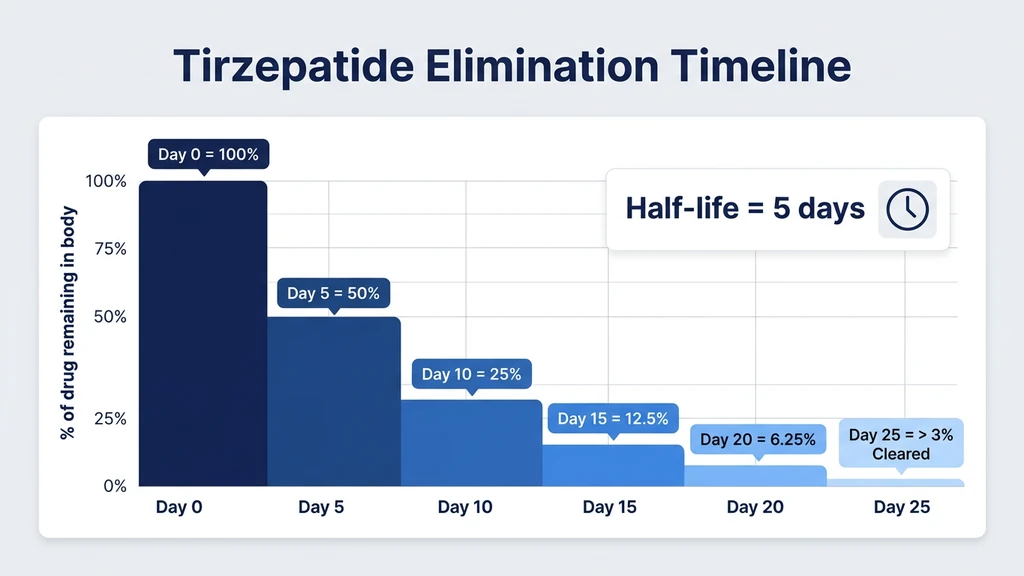
You took your last injection of tirzepatide five days ago. The appetite suppression is fading, and you want to know when the drug will be completely out of your body. Tirzepatide has an elimination half-life of approximately 5 days (120 hours). After your last injection, the drug takes roughly 25 days to clear your system entirely. That timeline reflects five half-lives, the pharmacological standard for considering a medication fully eliminated.
The FDA-approved prescribing information for Mounjaro and Zepbound reports a mean half-life of 5 days (approximately 120 hours) across all studied doses (Eli Lilly, Mounjaro Prescribing Information, 2022). Population pharmacokinetic analyses from the SURPASS clinical program confirmed this value, with steady-state concentrations reached after approximately 4 weeks of once-weekly dosing (Urva et al., Clin Pharmacokinet, 2022).
| Time After Last Dose | % of Drug Remaining | What You May Notice |
|---|---|---|
| Day 0 (injection day) | 100% | Full appetite suppression, active GIP + GLP-1 effects |
| Day 5 (1 half-life) | 50% | Appetite begins returning, glucose effects still present |
| Day 10 (2 half-lives) | 25% | Noticeable hunger increase, reduced nausea if present |
| Day 15 (3 half-lives) | 12.5% | Most side effects fading, appetite close to baseline |
| Day 20 (4 half-lives) | 6.25% | Minimal drug activity, blood sugar effects largely gone |
| Day 25 (5 half-lives) | 3.1% | Considered fully cleared, pre-treatment baseline |
For dosing protocols and titration schedules, see our tirzepatide dosage chart in units. For dose conversion help, use our tirzepatide dosage calculator.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
What Is Half-Life and Why Does It Matter for Tirzepatide?
Half-life measures the time it takes for your body to eliminate 50% of a drug from your bloodstream. Think of it like draining a bathtub with a slow leak. After 5 days, the tub is half empty. After another 5 days, half of what remained drains out, leaving a quarter. The process repeats until the water level is negligible. Tirzepatide clears in the same stepwise fashion, losing half its concentration every 5 days.
This 5-day half-life is what makes once-weekly dosing possible. A drug with a 4-hour half-life would require multiple daily doses to maintain therapeutic levels. Tirzepatide's slow elimination means a single injection on Monday still produces meaningful GIP and GLP-1 receptor activation the following Sunday.
Pharmacologists consider a drug "fully eliminated" after 5 half-lives. For tirzepatide, that equals approximately 25 days. At that point, only 3.1% of the original dose remains, a level too low to produce clinical effects. Population PK modeling from the SURPASS program validated this timeline across demographics, body weights, and dose levels (Urva et al., 2022).
Steady-state concentrations add another layer. During weekly dosing, each new injection arrives before the previous dose fully clears. Drug levels accumulate until input equals output, a balance called steady state. Tirzepatide reaches steady state after approximately 4-5 weekly doses. If you stop after months of treatment, you are clearing a higher total body burden than someone who took a single injection. The 25-day timeline still applies, but your starting concentration is higher.
The Dual Mechanism: How GIP and GLP-1 Activity Fades
Tirzepatide is the first approved dual GIP and GLP-1 receptor agonist. Both pathways contribute to its effects on appetite, blood sugar, and body weight, but they do not shut off simultaneously during the elimination period.
GLP-1 receptor effects include appetite suppression, delayed gastric emptying, and enhanced insulin secretion. These are the effects most users notice first when starting tirzepatide and the ones they notice fading first after stopping. Clinical observations suggest appetite suppression weakens significantly by day 7-10 after the last dose, even though drug levels remain above zero.
GIP receptor effects include potentiation of insulin secretion, regulation of fat metabolism, and modulation of bone turnover. GIP-mediated effects on lipid metabolism may persist longer because they involve downstream enzymatic changes that outlast the receptor signal itself. A study examining tirzepatide's dual receptor pharmacology found that GIP receptor activation produces distinct metabolic effects that complement GLP-1 activity (Willard et al., Mol Metab, 2020).
The practical result: appetite and nausea fade within 1-2 weeks after your last dose. Blood sugar regulation loosens over 2-3 weeks. Weight regain begins gradually as caloric intake rises and metabolic rate adjustments reverse. A 72-week extension analysis from SURMOUNT-1 showed that participants who discontinued tirzepatide regained approximately two-thirds of lost weight within 1 year of stopping (Jastreboff et al., NEJM, 2022).
Understanding this timeline matters for anyone planning to switch medications, undergo surgery, or transition off treatment. It also explains why side effects like diarrhea and headaches resolve within the first two weeks after stopping.
Factors That Affect How Long Tirzepatide Stays in Your System
Not everyone clears tirzepatide at the same rate. Several physiological and clinical factors shift the timeline by hours to days.
Body Weight and Composition
Tirzepatide is a large peptide (molecular weight ~4,810 Da) that distributes into tissues based on body composition. Population PK analysis showed that body weight is the most significant covariate affecting tirzepatide exposure. Heavier individuals have a larger volume of distribution, meaning the drug spreads into more tissue and takes slightly longer to clear (Urva et al., 2022).
A person weighing 120 kg may retain measurable tirzepatide levels 1-2 days longer than a person weighing 70 kg after the same dose. The difference is modest but real. It partly explains why the recommended titration starts at the same 2.5 mg dose regardless of body weight: the drug's self-adjusting pharmacokinetics produce proportionally similar exposure across the weight range.
Dose Level
Higher doses produce higher peak concentrations and take marginally longer to fall below the detection threshold. A person stopping after months on 15 mg has more drug in circulation than someone stopping at 5 mg. The half-life itself does not change with dose (it remains approximately 5 days across the 5-15 mg range), but the absolute amount to clear is larger.
The SURPASS-1 trial confirmed dose-proportional pharmacokinetics: doubling the dose approximately doubled the area under the curve (AUC), while half-life remained stable (Rosenstock et al., NEJM, 2021). For our tirzepatide dosage chart, these PK properties guide the standard titration schedule.
Kidney Function
Tirzepatide is primarily cleared through proteolytic degradation rather than renal excretion. Mild to moderate renal impairment does not significantly alter tirzepatide pharmacokinetics. The Mounjaro prescribing information states no dose adjustment is needed for patients with eGFR above 30 mL/min/1.73 m2 (Eli Lilly, 2022).
Severe renal impairment (eGFR below 30) has not been extensively studied. Users with kidney disease should discuss elimination timing with their prescriber, particularly before surgical procedures requiring full drug clearance.
Liver Function
Unlike small-molecule drugs metabolized by cytochrome P450 enzymes, tirzepatide is a peptide degraded by general proteolysis. Hepatic impairment has a minimal effect on its clearance. Clinical pharmacology studies found no clinically meaningful changes in tirzepatide exposure in subjects with mild, moderate, or severe hepatic impairment (Urva et al., 2022).
This is relevant for users concerned about alcohol interactions. While alcohol does not alter tirzepatide clearance directly, it can exacerbate side effects like nausea and dehydration during the elimination period.
Age and Sex
Population PK modeling found no clinically significant effect of age (18-75 years) or sex on tirzepatide half-life. Women had approximately 10-15% higher exposure than men after adjusting for body weight, but this difference did not require dose modification (Urva et al., 2022).
Older adults may experience a marginally slower clearance due to reduced proteolytic activity, but the magnitude is small enough that the 25-day full-clearance estimate holds across adult age ranges.
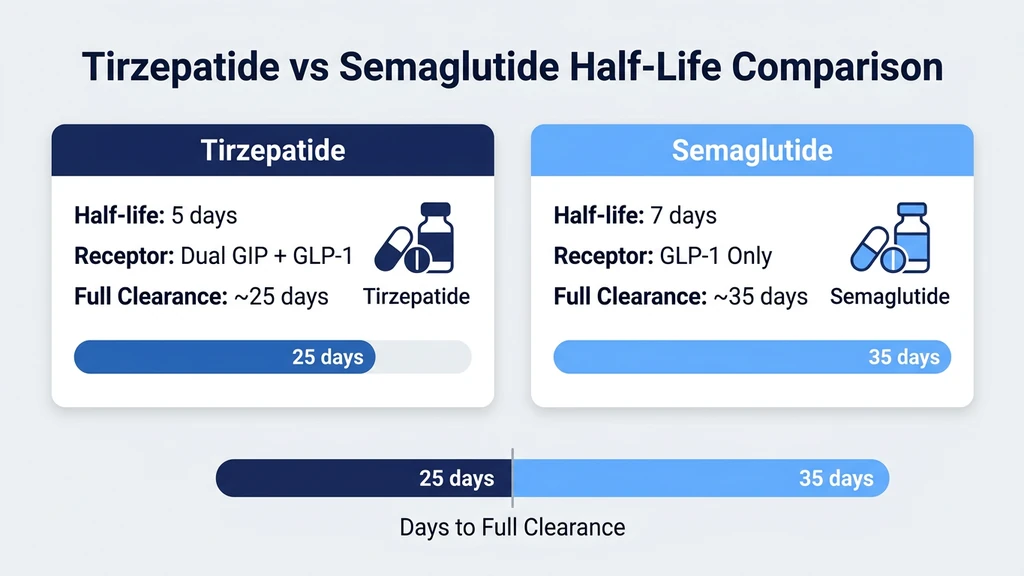
Tirzepatide vs. Semaglutide: Half-Life Comparison
Users switching between tirzepatide and semaglutide need to understand how their elimination timelines compare. Both are once-weekly injectables, but their half-lives differ.
| Property | Tirzepatide (Mounjaro/Zepbound) | Semaglutide (Ozempic/Wegovy) |
|---|---|---|
| Half-life | ~5 days (120 hours) | ~7 days (168 hours) |
| Time to full clearance (5 half-lives) | ~25 days | ~35 days |
| Steady-state reached | ~4-5 weeks | ~4-5 weeks |
| Receptor targets | GIP + GLP-1 (dual) | GLP-1 only |
| Dosing frequency | Once weekly | Once weekly |
Semaglutide's longer half-life (7 days vs. 5 days) means it takes approximately 35 days to fully clear, compared to 25 days for tirzepatide. The Ozempic prescribing information reports a half-life of approximately 1 week (Novo Nordisk, 2017).
Switching from semaglutide to tirzepatide: Most prescribers recommend starting tirzepatide one week after the last semaglutide injection. Because semaglutide is still present at that point (about 50% remaining), the GLP-1 receptor stimulation overlaps. This overlap generally smooths the transition but may increase GI side effects temporarily. Our semaglutide to tirzepatide switching guide covers detailed protocols.
Switching from tirzepatide to semaglutide: Tirzepatide clears faster, so a one-week washout leaves less overlap. Starting semaglutide 7-10 days after the last tirzepatide injection is common practice.
The semaglutide-tirzepatide conversion calculator can help determine equivalent doses when transitioning between the two drugs. For semaglutide dosing specifics, see the semaglutide dosage chart in mL.
What Happens When Tirzepatide Leaves Your System?
Stopping tirzepatide triggers a series of physiological reversals that unfold over weeks to months. Knowing the sequence helps set realistic expectations.
Days 1-7: Side Effects Fade First
The most common side effects, nausea, reduced appetite, and constipation, begin easing within the first week. Gastric emptying speed normalizes as GLP-1 receptor stimulation weakens. Users who experienced injection-day nausea or headaches notice those symptoms stop entirely.
Food becomes appealing again. Portion sizes start creeping upward. The reduced interest in eating that tirzepatide produces is pharmacological, not behavioral, and it reverses as drug levels fall. This is the window where building sustainable eating habits before stopping becomes critical.
Days 7-14: Appetite Returns to Baseline
By the end of the second week, appetite suppression is largely gone. Blood sugar regulation loosens, especially in people with type 2 diabetes whose glycemic control depended on tirzepatide. Fasting glucose and post-meal glucose levels rise toward pre-treatment values.
This period can feel abrupt. Users who lost 20-30% of their body weight on tirzepatide often describe a "switch flipping" around day 10, when hunger returns with intensity they had forgotten. Planning meals, maintaining protein intake, and continuing exercise during this transition prevents reactive overeating.
Weeks 3-4: Drug Considered Cleared
By day 25, tirzepatide is pharmacologically cleared. Any remaining traces (below 3.1% of the last dose) produce no measurable clinical effect. Blood tests for HbA1c, lipids, and liver enzymes now reflect your physiology without drug influence.
For users undergoing surgery, most anesthesiologists prefer tirzepatide to be stopped 2-3 weeks before elective procedures. The concern centers on delayed gastric emptying: tirzepatide slows stomach emptying, increasing aspiration risk during anesthesia. By 3 weeks post-last-dose, gastric motility has normalized in most patients.
Months 1-12: Weight Regain Pattern
The SURMOUNT-1 extension data documented what happens after discontinuation at 72 weeks. Participants who stopped tirzepatide regained approximately 14 of the 21 percentage points of weight lost (roughly two-thirds) over the following year (Jastreboff et al., 2022). Weight regain was not immediate; it accumulated steadily over 12 months.
This regain is not a failure of willpower. Tirzepatide suppresses appetite through receptor-mediated pathways that override volitional control. When the drug clears, those pathways revert. Metabolic adaptation, where the body lowers its resting metabolic rate after weight loss, compounds the problem. The biological drive to regain weight is powerful and persistent.
Strategies to mitigate regain include maintaining high protein intake (1.2-1.6 g/kg/day), structured exercise (both resistance and aerobic), and discussing long-term pharmacotherapy options with your prescriber. Our article on does tirzepatide burn fat explains the metabolic mechanisms in detail.
Dose-Dependent Duration: Does a Higher Dose Stay Longer?
The half-life of tirzepatide does not change with dose. Whether you inject 2.5 mg or 15 mg, the drug eliminates at the same rate: 50% every 5 days. What changes is the starting amount.
Consider two runners starting at different points on a track. Runner A starts 100 meters ahead. Runner B starts 600 meters ahead. Both run at the same speed. Runner B takes longer to finish because the starting distance is greater, but the speed is identical. Tirzepatide works the same way. A 15 mg dose starts with six times the drug mass of a 2.5 mg dose, so it takes slightly longer for absolute levels to drop below the detection threshold, even though the percentage decline per half-life is the same.
| Last Dose | Peak Level (relative) | Time to <1% Remaining |
|---|---|---|
| 2.5 mg | 1x | ~25 days |
| 5 mg | 2x | ~26 days |
| 10 mg | 4x | ~27 days |
| 15 mg | 6x | ~28 days |
The practical difference between doses is 1-3 days, clinically negligible. For planning purposes, the 25-day estimate applies regardless of your final dose level.
At steady state (after 4+ weeks of weekly dosing), the drug accumulates to approximately 1.5-2x the single-dose level. This means the effective starting concentration when you stop is higher than a single injection would produce. Even so, five half-lives still brings levels below clinical relevance.
For understanding how your specific dose translates to units for injection, see how many units is 2.5 mg of tirzepatide. For titration planning, the tirzepatide dosage calculator maps out each step.
Practical Scenarios: When Clearance Timing Matters
Several real-world situations require knowing exactly how long tirzepatide persists in your body.
Before Surgery
The American Society of Anesthesiologists issued guidance in 2023 recommending that GLP-1 receptor agonists be held before elective surgery due to delayed gastric emptying and aspiration risk. For weekly injectables like tirzepatide, the recommendation is to skip at least one dose (hold for 7+ days) before the procedure.
Many anesthesiologists prefer a longer washout of 2-3 weeks, especially for abdominal surgery. At 14 days post-last-dose (approximately 3 half-lives), 12.5% of the drug remains, and gastric motility is approaching normal. Discuss the specific timeline with your surgical team. Bring documentation of your last injection date.
Starting a New Medication
If switching from tirzepatide to another GLP-1 agonist (like semaglutide) or to an entirely different medication class, your prescriber will factor in the clearance timeline. Starting semaglutide while tirzepatide is still active means overlapping GLP-1 receptor stimulation, which increases the risk of nausea, vomiting, and diarrhea.
For most medication switches, a 1-2 week gap between the last tirzepatide dose and the first dose of the new medication is standard. The semaglutide to tirzepatide switching guide provides protocols for the most common transitions.
Drug Testing and Lab Work
Tirzepatide is not a controlled substance and does not appear on standard drug panels (5-panel, 10-panel, or 12-panel tests). It will not cause a positive result for any commonly tested substance.
However, tirzepatide does affect lab values. HbA1c, fasting glucose, insulin levels, liver enzymes (ALT, AST), and lipid panels will reflect the drug's metabolic effects until it fully clears. If your prescriber orders baseline labs to assess your metabolic status without drug influence, wait at least 4 weeks after your last injection for the most accurate results.
Pregnancy Planning
Tirzepatide is classified as a potential teratogenic risk based on animal data. The prescribing information recommends stopping tirzepatide at least 2 months before a planned pregnancy (Eli Lilly, 2022). The 2-month buffer exceeds the 25-day pharmacological clearance by a wide margin, providing an additional safety window.
Women who become pregnant while on tirzepatide should contact their prescriber immediately. The drug will clear within 25 days of the last injection, but early fetal development during that window warrants medical guidance.
Important Warnings
Do not stop tirzepatide abruptly without consulting your prescriber, especially if you have type 2 diabetes. Blood sugar levels will rise as the drug clears, and insulin or other glucose-lowering medications may need adjustment. Unmanaged hyperglycemia during the transition period can produce dangerous glucose spikes.
The elimination timeline described here is based on population averages. Individual variation exists. Users with unusual body composition, rare metabolic conditions, or polypharmacy may clear tirzepatide faster or slower than the 25-day estimate.
Tirzepatide delays gastric emptying. Even after your last dose, this effect persists for 1-2 weeks. If you experience persistent vomiting, severe abdominal pain, or signs of gastroparesis (feeling full after a few bites, bloating, acid reflux) beyond 3 weeks post-last-dose, seek medical evaluation. These symptoms should resolve as the drug clears; persistence suggests a separate cause.
For information about tirzepatide storage and shelf life, see does tirzepatide expire. For reconstitution guidance, see how to reconstitute tirzepatide. For injection technique, see our peptide injections complete guide.
Frequently Asked Questions
How long does tirzepatide stay in your system after the last injection?
Tirzepatide takes approximately 25 days to fully clear your system after the last injection. The drug has a half-life of about 5 days, meaning 50% is eliminated every 5 days. After 5 half-lives (25 days), less than 3.1% remains, which is pharmacologically insignificant.
What is the half-life of tirzepatide (Mounjaro)?
Tirzepatide has an elimination half-life of approximately 5 days (120 hours). This was confirmed across the SURPASS clinical trial program and population pharmacokinetic studies. The half-life does not change based on dose level, meaning 2.5 mg and 15 mg are both eliminated at the same rate.
Does tirzepatide stay in your system longer at higher doses?
The half-life remains the same (~5 days) regardless of dose. However, higher doses start with more drug mass, so absolute levels take 1-3 extra days to drop below detection limits. A 15 mg dose fully clears in approximately 28 days versus 25 days for a 2.5 mg dose. The clinical difference is negligible.
How long before surgery should I stop tirzepatide?
Most anesthesiologists recommend stopping tirzepatide at least 7-14 days before elective surgery, with some preferring a 2-3 week washout. The concern is delayed gastric emptying, which increases aspiration risk during anesthesia. Discuss your specific timeline with your surgical team and bring your last injection date.
Does tirzepatide show up on a drug test?
No. Tirzepatide is not a controlled substance and does not appear on standard 5-panel, 10-panel, or 12-panel drug tests. It is a peptide hormone, not an amphetamine, opioid, or other tested substance class. It does affect metabolic lab values (HbA1c, glucose, lipids) until fully cleared.
How long does tirzepatide suppress appetite after stopping?
Appetite suppression typically weakens noticeably within 7-10 days of the last injection and returns to near-baseline by day 14. Some residual reduction may persist until day 20, but most users report full return of pre-treatment hunger levels within 2-3 weeks of stopping.
Does tirzepatide or semaglutide stay in your system longer?
Semaglutide stays longer. Its half-life is approximately 7 days versus 5 days for tirzepatide. Semaglutide takes about 35 days to fully clear (5 half-lives), compared to 25 days for tirzepatide. This difference matters when switching between the two medications.
How long after stopping tirzepatide will I regain weight?
Weight regain begins gradually within weeks of stopping as appetite returns to baseline. SURMOUNT-1 data showed participants regained approximately two-thirds of lost weight over the 12 months following discontinuation. The regain is driven by restored appetite and metabolic adaptation, not behavioral failure.
The Bottom Line
Tirzepatide has a half-life of approximately 5 days and takes roughly 25 days to fully clear your system. That timeline holds across dose levels (2.5 mg to 15 mg), body weights, and age ranges. The half-life does not change; only the starting concentration varies.
Appetite suppression fades within 1-2 weeks. Blood sugar effects resolve over 2-3 weeks. Side effects like nausea, constipation, and headaches stop within the first 10 days. Weight regain begins gradually and accumulates over months if pharmacotherapy is not continued.
For surgery, stop tirzepatide at least 1-2 weeks before the procedure. For pregnancy planning, the recommended washout is 2 months. For switching to semaglutide, a 1-week gap is standard practice. For accurate baseline labs, wait 4 weeks after your last dose.
Use our tirzepatide dosage calculator to plan titration schedules. For dosing details, see our tirzepatide dosage chart in units. For switching guidance, see the semaglutide to tirzepatide switching guide.
Related tirzepatide articles: - Does Tirzepatide Burn Fat? — how tirzepatide produces weight loss and what reverses when you stop - Does Tirzepatide Cause Diarrhea? — GI side effects that resolve as the drug clears - Does Tirzepatide Cause Hair Loss? — telogen effluvium timing relative to drug clearance - Can You Drink on Tirzepatide? — alcohol interactions during the elimination period - Does Tirzepatide Expire? — storage and shelf life for unused product - How to Reconstitute Tirzepatide — preparation guide for compounded tirzepatide - Not Losing Weight on Semaglutide? — troubleshooting the related GLP-1 agonist
More from this series: - How Long Does Semaglutide Stay in Your System? — 7-day half-life and 5-week elimination comparison - Does Tirzepatide Make You Tired? — fatigue data and fixes during active treatment - How Long Does Tirzepatide Last in the Fridge? — storage timelines for reconstituted and lyophilized forms - How Many mg Is 20 Units of Tirzepatide? — unit-to-mg conversion for compounded tirzepatide - How Long Do Semaglutide Side Effects Last? — clinical timelines for nausea, fatigue, and GI symptoms
Explore all peptide profiles and tools at PeptidesExplorer.
Related Articles
Semaglutide: How Long in Your System?
Semaglutide stays in your system for about 5 weeks after your last injection. Learn the 7-day half-life, elimination timeline, and factors affecting clearance.
Does Tirzepatide Help With Inflammation?
Does tirzepatide help with inflammation? Yes: CRP drops 32.9%, IL-6 drops 17.8% in trials. SURMOUNT data and adipose tissue mechanisms.
Does Tirzepatide Cause Insomnia?
Does tirzepatide cause insomnia? Trials say no, but 5 indirect pathways explain lost sleep. GI, blood sugar, and caloric deficit fixes.
Can Tirzepatide Cause Joint Pain? Clinical Data
Can tirzepatide cause joint pain? SURMOUNT arthralgia rates match placebo. Review 5 indirect causes, uric acid risks, and 8 relief tactics.