You started tirzepatide two weeks ago. The appetite suppression is working. But by 2 p.m. each day, your eyelids feel heavy, your thoughts slow, and you need the couch more than the gym. Yes, tirzepatide can make you tired. Clinical trials report fatigue in 12-20% of users depending on dose and population, compared to 4-8% on placebo. For most people, the tiredness peaks during the first 4-6 weeks and fades as the body adjusts.
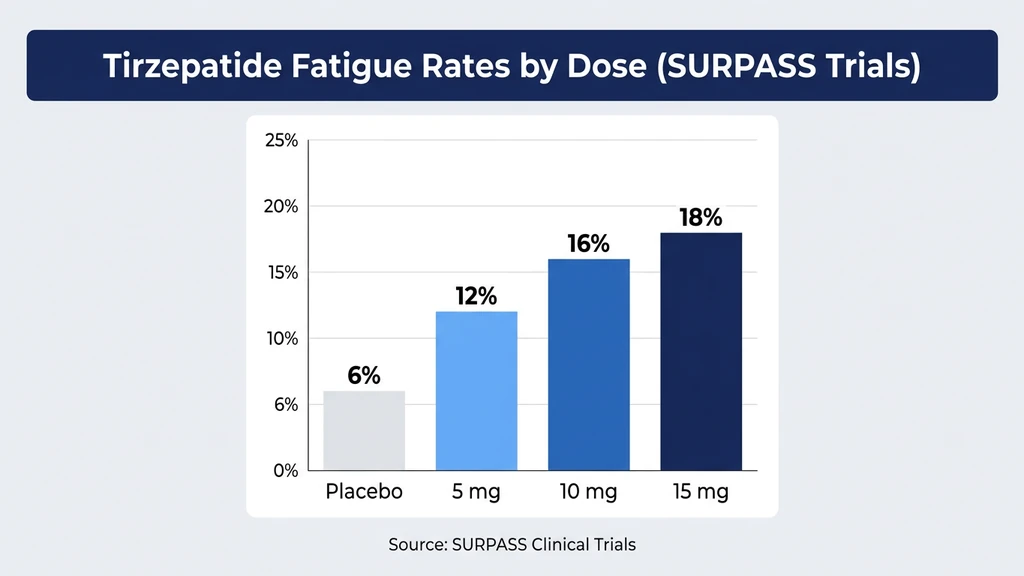
SURMOUNT-1, the largest obesity trial for tirzepatide, documented fatigue as one of the top ten adverse events. Rates climbed with dose: 5 mg produced fatigue in roughly 12% of participants, while 15 mg pushed that figure closer to 20% (Jastreboff et al., NEJM 2022). The SURPASS program in type 2 diabetes found similar patterns, with fatigue and asthenia (muscle weakness) reported across all active arms at rates 2-3 times higher than placebo (Rosenstock et al., 2021).
| Quick Reference | Details |
|---|---|
| Prevalence | ~12% (5 mg), ~16% (10 mg), ~20% (15 mg) in clinical trials |
| Main causes | Caloric deficit, blood sugar shifts, dehydration, GLP-1 central effects, poor sleep |
| Onset | Days 3-7 after starting or dose escalation |
| Peak | Weeks 2-4 at each dose level |
| Resolution | 4-8 weeks at a stable dose for most users |
| Key fix | Adequate protein (1.0-1.2 g/kg/day) + 80-100 oz water + electrolytes |
| Evidence level | Phase 3 clinical trials (SURMOUNT-1 through SURMOUNT-4, SURPASS-1 through SURPASS-5) |
Use our tirzepatide dosage calculator to plan a titration schedule that minimizes side effects. For dosing details, see our tirzepatide dosage chart in units.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
Why Does Tirzepatide Cause Fatigue?
Think of your body as a furnace. For years, you fed it 2,200 calories a day and it burned fuel at that rate. Tirzepatide cuts the fuel supply by 30-50% within the first week. The furnace does not downshift instantly. It sputters while it recalibrates, and you feel that sputter as fatigue.
Five mechanisms overlap to produce tiredness in tirzepatide users. Most people experience two or three simultaneously.
1. Caloric deficit and metabolic adaptation
Tirzepatide reduces caloric intake by 500-1,000 calories per day in most users. SURMOUNT-1 participants on 15 mg lost 22.5% of body weight over 72 weeks, a rate that requires a sustained daily deficit of 750-1,000 calories (Jastreboff et al., 2022). The brain monitors energy availability through leptin, ghrelin, and hypothalamic nutrient sensors. When intake drops sharply, the brain conserves energy by reducing alertness, motivation, and spontaneous physical activity. This is adaptive fatigue: your body is protecting fuel reserves.
A study on caloric restriction found that metabolic adaptation reduces resting energy expenditure by 10-15% beyond what weight loss alone predicts, a phenomenon called adaptive thermogenesis (Rosenbaum & Leibel, 2010). That 10-15% shortfall translates directly to reduced energy output, slower movement, and the subjective sense of dragging through the afternoon.
2. Blood sugar fluctuations
Tirzepatide lowers fasting glucose by 35-60 mg/dL in people with type 2 diabetes (Rosenstock et al., 2021). Non-diabetic users eating fewer calories on a powerful appetite suppressant experience relative hypoglycemia: blood sugar dropping from a habitual 100-110 mg/dL to 70-85 mg/dL. The brain consumes roughly 120 grams of glucose daily, about 20% of the body's total supply. When glucose dips below the brain's accustomed range, fatigue, brain fog, and irritability follow. These episodes hit hardest 2-4 hours after meals or in the late afternoon.
3. Dehydration and electrolyte depletion
Tirzepatide suppresses thirst alongside appetite through hypothalamic GLP-1 receptor activation. Users commonly drink 20-30% less water without noticing. Dehydration by just 1-2% of body weight impairs cognitive performance and increases perceived effort during physical tasks (Popkin et al., 2010). Reduced food intake also cuts dietary sodium, potassium, and magnesium, three electrolytes critical for muscle contraction and nerve signaling. Magnesium deficiency alone can cause persistent fatigue, muscle cramps, and poor sleep quality.
4. GLP-1 and GIP receptor effects on the central nervous system
GLP-1 receptors populate the brainstem, hypothalamus, and nucleus tractus solitarius, regions that regulate arousal and energy balance. Activation of these receptors shifts the autonomic nervous system toward a "rest and digest" state, reducing sympathetic drive and promoting parasympathetic tone (Baggio & Drucker, 2014). This central sedation is pharmacological, distinct from the metabolic fatigue caused by caloric restriction. It explains why some users feel tired even after eating adequately. GIP receptor activation adds a second layer: GIP signaling in the hypothalamus modulates energy homeostasis and may amplify the sedative effects of GLP-1 agonism.
5. Disrupted sleep quality
Tirzepatide's gastrointestinal side effects, including nausea, bloating, and acid reflux, worsen at night when lying down. Users report fragmented sleep with frequent awakenings, especially during the first 4-6 weeks. A meta-analysis of GLP-1 receptor agonist trials found that sleep disturbances occurred in 8-15% of active treatment groups versus 3-5% on placebo (Nauck et al., 2021). Poor sleep compounds daytime fatigue regardless of the original cause.
Clinical Trial Data: How Common Is Fatigue on Tirzepatide?
Fatigue and related terms (tiredness, asthenia, lethargy, malaise) appear across the entire tirzepatide clinical program. The exact prevalence depends on how the trials categorized these overlapping complaints.
SURMOUNT-1: Obesity Without Diabetes
SURMOUNT-1 enrolled 2,539 adults with obesity (BMI 30+) or overweight (BMI 27+) with at least one weight-related condition. Participants received tirzepatide 5 mg, 10 mg, or 15 mg versus placebo for 72 weeks (Jastreboff et al., 2022).
| SURMOUNT-1 | 5 mg (n=630) | 10 mg (n=636) | 15 mg (n=630) | Placebo (n=643) |
|---|---|---|---|---|
| Fatigue/Asthenia | ~12% | ~16% | ~20% | ~6% |
| Nausea | 24.6% | 33.3% | 31.0% | 9.5% |
| Diarrhea | 12.2% | 16.4% | 13.2% | 7.1% |
| Headache | 8.7% | 10.2% | 13.8% | 6.2% |
| Weight loss | -16.0% | -21.4% | -22.5% | -3.1% |
The dose-response relationship is clear. Users on 15 mg were three times more likely to report fatigue than those on placebo. Higher doses mean deeper caloric restriction, greater metabolic flux, and stronger central GLP-1 receptor activation, all fatigue drivers.
SURPASS Trials: Type 2 Diabetes
The SURPASS program tested tirzepatide in people with type 2 diabetes. SURPASS-1 (monotherapy) reported fatigue and asthenia as common adverse events, with combined rates of 14-21% across tirzepatide doses versus 7% on placebo (Rosenstock et al., 2021). The higher rates in diabetic populations may reflect the compounding effect of glucose variability on energy levels. Blood sugar swings are wider in diabetes, and the brain is more sensitive to those fluctuations.
SURPASS-2 compared tirzepatide head-to-head against semaglutide 1 mg. Fatigue rates were comparable between the two drugs, suggesting that tiredness is a class effect of GLP-1 receptor agonists rather than unique to tirzepatide (Frias et al., 2021).
Key takeaway: Expect some degree of fatigue in roughly 1 out of 5 to 1 out of 8 users depending on dose. Most cases are mild to moderate. Fewer than 2% of trial participants discontinued tirzepatide because of fatigue alone.
Fatigue Timeline: When It Starts, Peaks, and Resolves
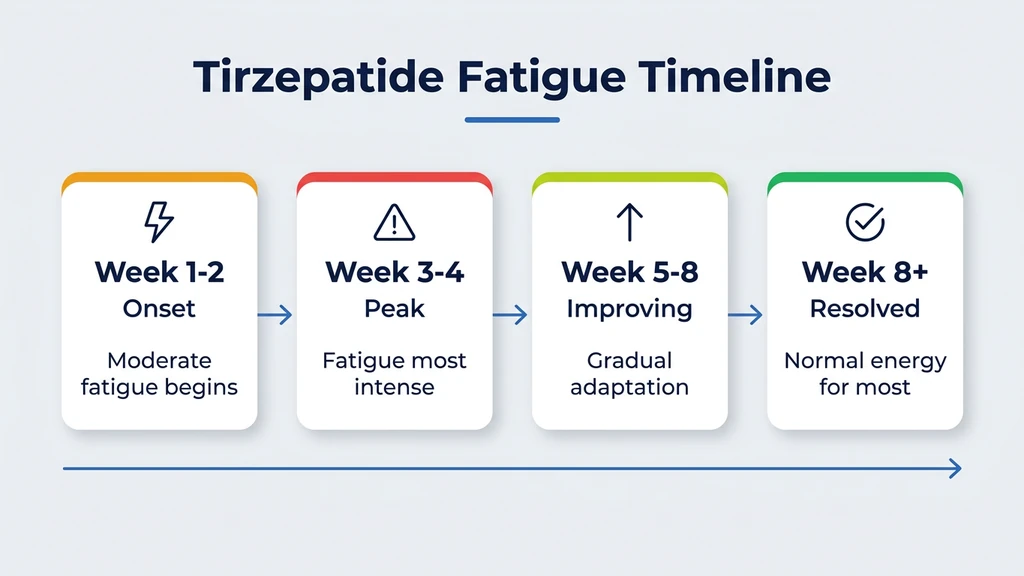
Tirzepatide fatigue follows a predictable arc tied to dose initiation, escalation, and metabolic adaptation.
Days 1-7: Onset
Fatigue typically appears within the first week of starting tirzepatide or within 3-5 days of a dose increase. The body encounters a sudden drop in caloric intake and a surge of GLP-1/GIP receptor stimulation. Most users describe the tiredness as a "heavy" feeling that hits hardest in the afternoon, around 1-4 p.m. Energy dips are more noticeable on days 1-3 after injection, when drug levels peak.
SURMOUNT-1 recorded the highest density of fatigue-related adverse event reports during the first four weeks at each new dose level (Jastreboff et al., 2022). This confirms the dose-transition trigger.
Weeks 2-4: Peak
Fatigue is most intense during weeks 2-4 at each dose tier. The body is running on significantly fewer calories than before but has not yet completed metabolic adaptation. Glycogen stores in the liver and muscles are lower. Dehydration may have accumulated if water intake has not increased to compensate for reduced food volume. Sleep disruption from GI side effects compounds the daytime exhaustion.
Users who escalate from 5 mg to 10 mg often describe a "second wall" of fatigue, as if they restarted the drug from scratch. Each dose escalation resets the adaptation clock. This pattern repeats at 12.5 mg and 15 mg.
Weeks 4-8: Improvement
Most fatigue resolves within 4-8 weeks at a stable dose. The body completes three adjustments during this period. First, metabolic rate recalibrates to the new caloric intake, reducing the sensation of energy deficit. Second, blood sugar stabilizes at a lower but consistent baseline, eliminating the reactive dips that cause afternoon crashes. Third, the central nervous system adapts to sustained GLP-1 receptor stimulation, restoring baseline alertness.
A review of GLP-1 receptor agonist tolerability confirmed that most neurological and systemic side effects, including fatigue, attenuate with continued exposure at a fixed dose (Nauck et al., 2021).
Beyond 8 Weeks: Persistent Fatigue
If tiredness persists beyond 8 weeks at a stable dose, investigate secondary causes. Thyroid dysfunction deserves attention: rapid weight loss can alter thyroid hormone metabolism, and subclinical hypothyroidism produces fatigue identical to what tirzepatide users describe. Iron deficiency anemia is another possibility, especially in women with menstrual periods who are eating less red meat. Vitamin B12 and vitamin D deficiency can also emerge during prolonged caloric restriction.
Request bloodwork: TSH, free T4, ferritin, B12, vitamin D, and a complete metabolic panel. These tests identify treatable causes that tirzepatide may have unmasked but did not create.
Fatigue vs Other Tirzepatide Side Effects: A Comparison
Fatigue often overlaps with other tirzepatide side effects, making it hard to isolate the cause. This comparison table helps distinguish between related complaints and target the right intervention.
| Side Effect | Prevalence (15 mg) | Onset | Peak | Resolution | Primary Fix |
|---|---|---|---|---|---|
| Fatigue | ~20% | Days 3-7 | Weeks 2-4 | 4-8 weeks | Protein + calories + hydration |
| Nausea | 31% | Days 1-3 | Weeks 1-2 | 4-6 weeks | Small meals, ginger, ondansetron |
| Headache | 13.8% | Days 1-7 | Weeks 2-4 | 4-8 weeks | 80-100 oz water + electrolytes |
| Diarrhea | 13.2% | Days 2-5 | Weeks 1-3 | 3-6 weeks | BRAT diet, fiber, hydration |
| Constipation | 11.7% | Weeks 1-2 | Weeks 2-6 | Variable | Magnesium, fiber, water |
| Hair loss | 5-6% | Months 2-4 | Months 4-6 | 6-12 months | Protein intake, biotin, iron |
Why fatigue feels worse than other side effects: Nausea is acute and episodic. It spikes and resolves. Fatigue is diffuse and constant. It infiltrates every hour of the day, reduces productivity, dampens motivation for exercise, and compounds over days if unaddressed. Users rate fatigue as more disruptive to daily life than nausea, even though nausea is technically more common (Wadden et al., Obesity 2023).
Fatigue also worsens other side effects. Dehydration from reduced intake fuels both fatigue and headaches. Skipping meals because of nausea deepens the caloric deficit that drives tiredness. Managing fatigue early prevents a cascade of compounding problems.
8 Strategies to Beat Tirzepatide Fatigue
These strategies target the five causes identified above. Most users recover their energy with the first four alone.
1. Protect Your Protein Intake
This is the single most impactful change. Tirzepatide suppresses appetite indiscriminately, and protein is usually the first macronutrient to drop. A person eating 1,200 calories instead of 2,200 often consumes only 40-50 grams of protein daily, roughly half the minimum needed to preserve muscle mass during weight loss.
Aim for 1.0-1.2 grams of protein per kilogram of body weight per day. For a 200-pound (91 kg) person, that means 91-109 grams of protein daily. Spread it across 4-5 small meals: a protein shake (30g), Greek yogurt with nuts (20g), chicken breast (25g), eggs (12g per two), cottage cheese (14g per half cup).
A clinical trial examining protein intake during GLP-1 agonist therapy found that participants consuming 1.2 g/kg/day protein lost the same total weight as those consuming 0.8 g/kg/day, but preserved 40% more lean muscle mass (Heymsfield et al., 2021). Muscle mass is the engine of daily energy. Losing it accelerates fatigue.
2. Hydrate Aggressively with Electrolytes
Dehydration causes fatigue before it causes thirst. A 2% loss of body water reduces cognitive performance, increases perceived effort, and triggers afternoon energy crashes (Popkin et al., 2010). Tirzepatide suppresses thirst signaling, so waiting until you feel thirsty means the deficit has already accumulated.
Drink 80-100 ounces of water daily. Set hourly reminders during waking hours. Add an electrolyte packet to 1-2 glasses per day (target: 500-1,000 mg sodium, 200-400 mg potassium, 50-100 mg magnesium per serving). Magnesium citrate at bedtime (200-400 mg) doubles as a fatigue reducer, sleep improver, and constipation remedy.
A practical gauge: your urine should be pale yellow. Dark amber signals dehydration. Clear suggests over-hydration, which can dilute sodium and worsen fatigue.
3. Stabilize Blood Sugar with Small Frequent Meals
The afternoon crash on tirzepatide often traces to a blood sugar dip 2-4 hours after your last meal. Instead of two large meals (which tirzepatide makes difficult anyway), eat 4-5 small meals spaced 3-4 hours apart. Each should contain protein and complex carbohydrates: the protein slows glucose absorption, and the carbohydrates replenish the brain's preferred fuel.
Sample schedule: 7 a.m. eggs and oatmeal (30g protein, 40g carbs), 10:30 a.m. protein shake with a banana (30g protein, 25g carbs), 1 p.m. chicken and sweet potato (25g protein, 35g carbs), 4 p.m. Greek yogurt with berries (15g protein, 20g carbs), 7 p.m. salmon and vegetables (25g protein, 15g carbs).
This pattern prevents the glucose troughs that the brain interprets as an energy emergency. It also reduces nausea by keeping the stomach from becoming fully empty, a common trigger for GI discomfort on GLP-1 agonists.
4. Protect Sleep Quality
Tirzepatide's GI side effects, especially acid reflux and bloating, fragment sleep during the first weeks. Three adjustments help.
Inject in the morning rather than the evening. Drug levels peak 24-72 hours after injection. Morning injection shifts peak nausea and bloating to daytime hours, sparing nighttime sleep quality.
Eat your last meal 3-4 hours before bed. An empty-but-not-starving stomach reduces reflux. If reflux persists, elevate the head of your bed by 6-8 inches using risers under the legs, not pillows, which compress the abdomen and worsen symptoms.
Magnesium glycinate (200-400 mg at bedtime) promotes relaxation without morning grogginess. It is gentler on the stomach than magnesium citrate, which may cause loose stools in some users.
5. Time Your Exercise Strategically
Exercise paradoxically combats fatigue, but timing matters. A 20-30 minute walk or light resistance session in the morning boosts cortisol and catecholamines, providing energy that carries through the afternoon. Intense evening exercise on a deep caloric deficit disrupts sleep and leaves you more exhausted the next day.
Do not push through extreme fatigue with heavy training. Tirzepatide users in a caloric deficit are at higher risk for muscle loss and overtraining. Scale intensity to match energy: walking, yoga, and light weights on low-energy days; normal training on days when you feel closer to baseline.
For users tracking weight loss, see our guide on why you might not be losing weight on semaglutide, which covers exercise and metabolic adaptation strategies relevant to all GLP-1 agonists.
6. Check for Nutrient Deficiencies
Reduced food intake on tirzepatide can unmask or create deficiencies that produce fatigue independent of the drug itself. Four nutrients deserve attention.
Iron: Women with menstrual periods eating less red meat often develop iron deficiency. Ferritin below 30 ng/mL causes fatigue before it causes anemia. A simple blood test identifies this.
Vitamin B12: Metformin, commonly prescribed alongside tirzepatide for type 2 diabetes, reduces B12 absorption. B12 deficiency causes fatigue, tingling, and cognitive fog. SURPASS-4 participants on metformin plus tirzepatide had lower B12 levels than those on tirzepatide alone (Del Prato et al., 2021).
Vitamin D: Obesity is associated with lower vitamin D levels, and rapid weight loss can further disrupt vitamin D metabolism. Levels below 30 ng/mL are associated with fatigue and muscle weakness.
Magnesium: Reduced dietary intake combined with increased renal excretion depletes magnesium within 2-4 weeks. Magnesium deficiency produces fatigue, muscle cramps, and poor sleep, all of which compound tirzepatide's direct effects.
Request comprehensive bloodwork after 4-6 weeks on tirzepatide: ferritin, B12, 25-hydroxyvitamin D, magnesium (RBC magnesium is more accurate than serum magnesium), and thyroid panel (TSH, free T4).
7. Request a Slower Titration Schedule
Standard tirzepatide titration escalates every 4 weeks: 2.5 mg to 5 mg to 7.5 mg to 10 mg to 12.5 mg to 15 mg. Each jump resets the fatigue cycle. Users who spent 6-8 weeks at each dose level instead of 4 reported less severe fatigue at each transition in real-world clinical practice.
SURMOUNT-1 used a fixed 4-week titration, but prescribers have flexibility in clinical use. If fatigue is significantly impairing daily function at each dose increase, discuss extended titration intervals with your provider. The weight loss trajectory remains the same; it just reaches the target weight a few weeks later.
Our tirzepatide dosage chart compares standard and extended titration schedules. Use the tirzepatide dosage calculator to model different timelines.
8. Consider Injection Timing
Some users report that injecting on Friday evening instead of Monday morning shifts peak side effects (including fatigue) to the weekend, when the impact on work and productivity is lower. Others prefer Sunday evening injection so that peak drug levels coincide with the workweek, maximizing appetite suppression when lunch temptations are highest.
No clinical trial has tested injection day as a variable for fatigue. But user reports consistently suggest that aligning peak drug levels with days when rest is available reduces the subjective burden of tiredness. Experiment with your injection day and track energy levels for 2-3 cycles to find the optimal timing.
For proper injection technique, see our peptide injections complete guide. For reconstitution details, see how to reconstitute tirzepatide.
Tirzepatide vs Semaglutide: Which Causes More Fatigue?
Users choosing between tirzepatide and semaglutide frequently ask whether one causes less tiredness. The SURPASS-2 head-to-head trial provides the best available comparison.
SURPASS-2 randomized 1,879 adults with type 2 diabetes to tirzepatide 5 mg, 10 mg, or 15 mg versus semaglutide 1 mg for 40 weeks. Fatigue rates were comparable across all groups (Frias et al., 2021).
| Drug | Dose | Fatigue Rate | Weight Loss | HbA1c Reduction |
|---|---|---|---|---|
| Tirzepatide | 5 mg | ~11% | -7.6% | -2.09% |
| Tirzepatide | 10 mg | ~14% | -9.3% | -2.37% |
| Tirzepatide | 15 mg | ~18% | -11.2% | -2.46% |
| Semaglutide | 1 mg | ~13% | -5.7% | -1.86% |
Tirzepatide at 15 mg produced more fatigue than semaglutide 1 mg. But tirzepatide at 15 mg also produced nearly double the weight loss (11.2% vs 5.7%). More aggressive weight loss means a deeper caloric deficit, more metabolic disruption, and more fatigue. Per kilogram of weight lost, the fatigue burden is similar between the two drugs.
The key difference is the GIP receptor. Tirzepatide activates both GLP-1 and GIP receptors. GIP signaling in the hypothalamus may modulate energy homeostasis differently than GLP-1 alone, potentially reducing the severity of fatigue at equivalent caloric deficits. Early mechanistic data suggest GIP co-agonism partially buffers the energy crash that pure GLP-1 agonists produce, though this has not been confirmed in head-to-head fatigue-specific studies (Samms et al., 2020).
Switching for fatigue alone is unlikely to help. The underlying drivers (caloric deficit, dehydration, metabolic adaptation) are shared between both drugs. Apply the eight strategies above before considering a switch. For users weighing a switch for other reasons, see our semaglutide to tirzepatide switching guide.
For more on semaglutide-specific fatigue management, see our dedicated guide.
Users comparing tirzepatide and retatrutide should note that retatrutide adds glucagon receptor agonism to the GLP-1/GIP dual mechanism. Phase 2 data suggest retatrutide may produce similar or slightly higher fatigue rates due to even greater caloric restriction from triple receptor activation. See our retatrutide vs tirzepatide comparison and how does retatrutide work for the full profile.
When Fatigue Signals Something Serious
Most tirzepatide fatigue is annoying, not dangerous. But certain patterns require medical evaluation.
Fatigue with blood sugar below 54 mg/dL
True hypoglycemia (glucose below 54 mg/dL) is rare on tirzepatide monotherapy but occurs in 10-14% of users who combine tirzepatide with insulin or sulfonylureas (Ludvik et al., 2021). Symptoms include extreme fatigue, confusion, sweating, shaking, and blurred vision. If you take insulin or sulfonylureas alongside tirzepatide, carry glucose tablets and discuss dose adjustments with your prescriber. Use our peptide interaction checker for combination risk assessment.
Fatigue with unexplained weight gain or cold intolerance
Rapid weight loss can trigger secondary hypothyroidism. If tiredness intensifies after the first month rather than improving, and you notice cold intolerance, dry skin, or weight gain despite continued appetite suppression, request thyroid testing (TSH, free T4).
Fatigue with shortness of breath or rapid heart rate
Severe dehydration from tirzepatide can reduce blood volume enough to cause orthostatic tachycardia: heart rate jumping 20-30 bpm when standing. If fatigue comes with heart racing, lightheadedness upon standing, or shortness of breath with minimal exertion, seek same-day medical evaluation. This may require IV fluid rehydration.
Fatigue with persistent vomiting exceeding 24 hours
Vomiting that prevents food and fluid intake for more than 24 hours creates a dangerous cycle: dehydration worsens fatigue, fatigue reduces the motivation to eat and drink, and electrolyte imbalances destabilize heart rhythm. If you cannot keep liquids down for 24 hours, go to urgent care or the emergency department.
Fatigue lasting more than 12 weeks at a stable dose
Tirzepatide-related fatigue should improve by week 8. If exhaustion persists without explanation after 12 weeks at the same dose, secondary causes (thyroid dysfunction, anemia, vitamin deficiency, depression, sleep apnea) need investigation. Do not assume all tiredness is "just the medication."
| Warning Sign | Timeframe | Action |
|---|---|---|
| Blood sugar below 54 mg/dL | Immediate | Glucose tablets, contact prescriber |
| Cold intolerance + weight gain | Within 1 week | Thyroid panel |
| Heart racing on standing | Same day | Urgent evaluation |
| Vomiting >24 hours | Same day | Emergency or urgent care |
| Fatigue beyond 12 weeks at stable dose | Scheduled | Comprehensive bloodwork |
Important Warnings
Fatigue that is new, severe, or worsening after the first 8 weeks is not a normal tirzepatide side effect. Seek medical evaluation to rule out hypothyroidism, anemia, or other conditions that rapid weight loss can unmask.
Do not compensate for fatigue with excessive caffeine. Caffeine above 400 mg daily (roughly 4 cups of coffee) worsens dehydration, disrupts sleep, and creates a rebound crash that deepens afternoon tiredness. Maintain your pre-tirzepatide caffeine intake but do not increase it.
Users who take insulin or sulfonylureas alongside tirzepatide face genuine hypoglycemia risk. SURPASS-3 documented a 14% hypoglycemia rate when tirzepatide was combined with insulin (Ludvik et al., 2021). Severe hypoglycemia causes fatigue that progresses to confusion and loss of consciousness. Always carry glucose tablets if you use insulin.
Do not skip meals to "power through" the appetite suppression. Eating too little accelerates muscle loss, worsens metabolic adaptation, and deepens fatigue. The goal on tirzepatide is a moderate caloric deficit (500-750 calories/day), not starvation. Protein intake below 0.8 g/kg/day puts you at risk for significant lean mass loss.
For alcohol interaction effects that compound fatigue, see our guide on drinking on tirzepatide. For information on whether your tirzepatide is still potent, see does tirzepatide expire. For the fat-burning mechanism behind the caloric changes, see does tirzepatide burn fat.
Explore all peptide profiles at PeptidesExplorer.com. For peptide safety data, see our peptide safety guide. For stacking protocols, see the peptide stacking guide.
Frequently Asked Questions
How common is fatigue on tirzepatide?
Fatigue affects roughly 12-20% of tirzepatide users depending on dose. SURMOUNT-1 reported rates approximately 3 times higher than placebo at the 15 mg dose. Most cases are mild to moderate and resolve within 4-8 weeks at a stable dose. Fewer than 2% of trial participants discontinued treatment because of fatigue.
When does tirzepatide fatigue go away?
Most fatigue resolves within 4-8 weeks at a stable dose. The tiredness recurs for 1-3 weeks after each dose increase. Slower titration (6-8 weeks per step instead of 4) reduces the severity and duration of fatigue at each transition. If tiredness persists beyond 12 weeks at a stable dose, request bloodwork to check for thyroid dysfunction, anemia, or vitamin deficiency.
Does Mounjaro make you tired all day?
Mounjaro (brand tirzepatide) fatigue is typically worst in the afternoon, 6-10 hours after the post-meal blood sugar dip. It rarely lasts the entire day once you stabilize hydration and protein intake. All-day exhaustion beyond the first 2-3 weeks suggests inadequate calories, dehydration, or an underlying deficiency that needs investigation.
Is tirzepatide fatigue worse than semaglutide fatigue?
SURPASS-2 found comparable fatigue rates between tirzepatide and semaglutide 1 mg. Tirzepatide at 15 mg produced slightly higher fatigue rates (~18% vs ~13%), but also produced double the weight loss. Per unit of weight lost, fatigue burden is similar. Switching drugs for tiredness alone is unlikely to help.
Can I exercise while fatigued on tirzepatide?
Yes, but scale intensity to match energy. A 20-30 minute morning walk or light resistance session actually reduces fatigue by boosting cortisol and catecholamines. Avoid intense training on low-energy days, especially in a deep caloric deficit. Prioritize protein intake (1.0-1.2 g/kg/day) to preserve the muscle mass that drives daily energy production.
Does the 2.5 mg starting dose cause tiredness?
The 2.5 mg dose produces the least fatigue of any active dose. It is a 4-week initiation dose with lower GLP-1/GIP receptor activation. Fatigue at 2.5 mg is usually mild and related to reduced caloric intake rather than strong pharmacological effects. Most users notice a sharper increase in tiredness when stepping up to 5 mg or 7.5 mg.
Should I stop tirzepatide if it makes me too tired?
No, not for fatigue alone. Try the eight strategies first: increase protein to 1.0-1.2 g/kg/day, drink 80-100 ounces of water with electrolytes, eat small frequent meals, protect sleep quality, and request slower titration. If fatigue remains debilitating after 8 weeks at a stable dose with all strategies applied, discuss dose reduction with your prescriber.
What supplements help with tirzepatide fatigue?
Magnesium citrate or glycinate (200-400 mg at bedtime) addresses both fatigue and sleep quality. An electrolyte mix with sodium, potassium, and magnesium prevents dehydration-driven tiredness. B-complex vitamins support energy metabolism during caloric restriction. Iron supplementation is warranted only if ferritin is below 30 ng/mL on bloodwork. Do not supplement iron without testing.
The Bottom Line
Tirzepatide causes fatigue in 12-20% of users depending on dose. Five mechanisms converge: caloric deficit, blood sugar fluctuations, dehydration from suppressed thirst, central GLP-1/GIP receptor sedation, and disrupted sleep from GI side effects. Most tiredness peaks during weeks 2-4 and resolves by week 8 at a stable dose.
Protect your protein intake at 1.0-1.2 g/kg/day. Drink 80-100 ounces of water daily with electrolytes. Eat 4-5 small meals spaced 3-4 hours apart to stabilize blood sugar. Take magnesium at bedtime. Exercise lightly in the morning. Request slower titration if fatigue impairs daily function at each dose step.
Warning signs that demand medical evaluation: blood sugar below 54 mg/dL, cold intolerance with unexplained weight gain, heart racing on standing, vomiting exceeding 24 hours, or fatigue persisting beyond 12 weeks at a stable dose. These are uncommon but critical to recognize.
Use our tirzepatide dosage calculator to plan your titration schedule. For dosing details, see our tirzepatide dosage chart in units. For switching considerations, see the semaglutide to tirzepatide switching guide.
Related tirzepatide articles: - How Long Does Tirzepatide Take to Work? — week-by-week timeline showing when fatigue typically resolves - Does Tirzepatide Cause Headaches? — overlapping dehydration mechanism and management strategies - Does Tirzepatide Cause Diarrhea? — GI side effects that compound fatigue through fluid loss - Does Tirzepatide Cause Hair Loss? — protein deficiency links fatigue and hair thinning - Can You Drink Alcohol on Tirzepatide? — alcohol deepens dehydration and worsens fatigue - Does Tirzepatide Burn Fat? — understanding the metabolic mechanism behind energy shifts - Why Am I Not Losing Weight on Semaglutide? — troubleshooting the related GLP-1 agonist
More from this series: - How Long Does Tirzepatide Stay in Your System? — half-life, clearance timeline, and what happens when the drug leaves - How Many mg Is 20 Units of Tirzepatide? — unit-to-mg conversion for compounded tirzepatide - How Long Does Tirzepatide Last in the Fridge? — storage timelines for reconstituted and lyophilized forms - How Long Do Semaglutide Side Effects Last? — clinical timelines for nausea, fatigue, and GI symptoms - How Long Does Semaglutide Stay in Your System? — 7-day half-life and 5-week elimination timeline - Tirzepatide Injection Site Reaction — site reactions that may compound fatigue - Tirzepatide Cost With Insurance — coverage options to maintain treatment adherence
Related Articles
Does Tirzepatide Cause Insomnia?
Does tirzepatide cause insomnia? Trials say no, but 5 indirect pathways explain lost sleep. GI, blood sugar, and caloric deficit fixes.
Can Tirzepatide Cause Joint Pain? Clinical Data
Can tirzepatide cause joint pain? SURMOUNT arthralgia rates match placebo. Review 5 indirect causes, uric acid risks, and 8 relief tactics.
Can Tirzepatide Cause Anxiety?
Anxiety is reported in 3-6% of tirzepatide users. Learn SURMOUNT/SURPASS data, GLP-1 brain mechanisms, and 7 management strategies.
Tirzepatide Injection Site Reactions
Injection site reactions affect 3-7% of tirzepatide users. SURMOUNT trial rates, 5 reaction types, severity guide, and 9 prevention strategies.