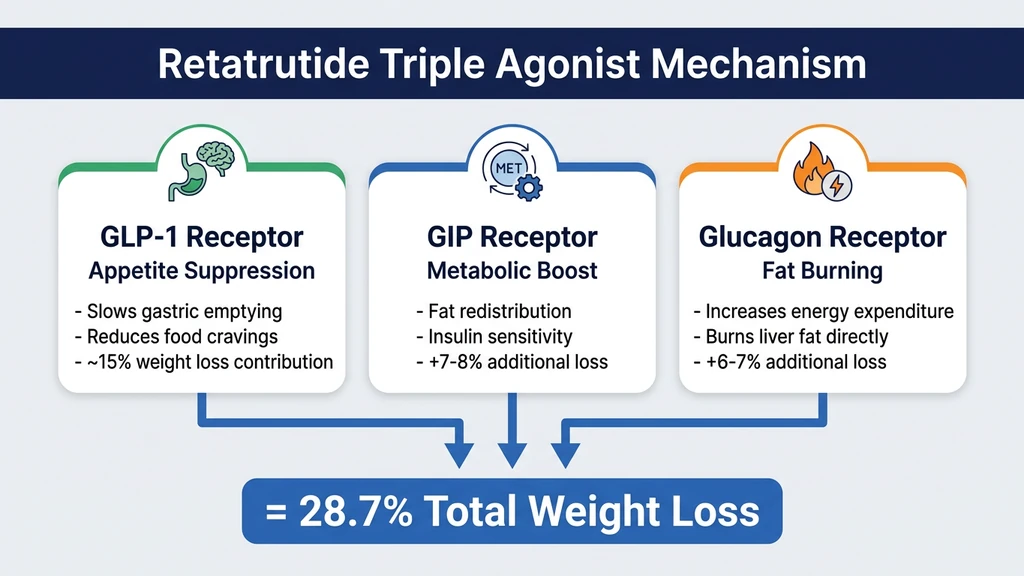
A single weekly injection activates three hormone receptors in your body, and the result is the largest drug-induced weight loss ever recorded. Retatrutide works by simultaneously targeting GLP-1, GIP, and glucagon receptors. GLP-1 suppresses appetite. GIP improves metabolic signaling. Glucagon forces your body to burn stored fat for energy, especially in the liver. Together, these three pathways produced 28.7% body weight loss over 68 weeks in Phase 3 trials (Lilly Press Release, Dec 2025).
No other drug in development or on the market activates all three receptors. Ozempic targets one. Zepbound targets two. Retatrutide targets all three. That third receptor, glucagon, is the reason a person starting at 250 pounds could expect to lose over 70 pounds in 16 months.
| Quick Reference | Details |
|---|---|
| Drug name | Retatrutide (LY3437943) |
| Maker | Eli Lilly |
| Mechanism | Triple agonist: GLP-1 + GIP + Glucagon |
| Structure | Synthetic peptide, 39 amino acids |
| Half-life | ~6 days (once-weekly dosing) |
| Max weight loss | 28.7% at 68 weeks (12 mg dose) |
| Liver fat reduction | 82% in MASLD substudy |
| FDA status | Phase 3 clinical trials (not approved) |
| Expected approval | Mid-2027 |
This article explains the retatrutide mechanism of action in plain language, breaks down what each receptor does, shows why three receptors outperform two, and walks through the clinical data supporting each claim. For the full drug overview including availability and pricing, see our complete retatrutide guide. For side effect details, see our retatrutide side effects guide.
This is educational content. Consult a healthcare provider before starting any medication.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
The Three Keys: GLP-1, GIP, and Glucagon Receptors
Picture three separate locks on three separate doors inside your body. Behind one door sits your appetite control center. Behind another sits your metabolic processing system. Behind the third sits your energy furnace, the part of you that burns stored fat.
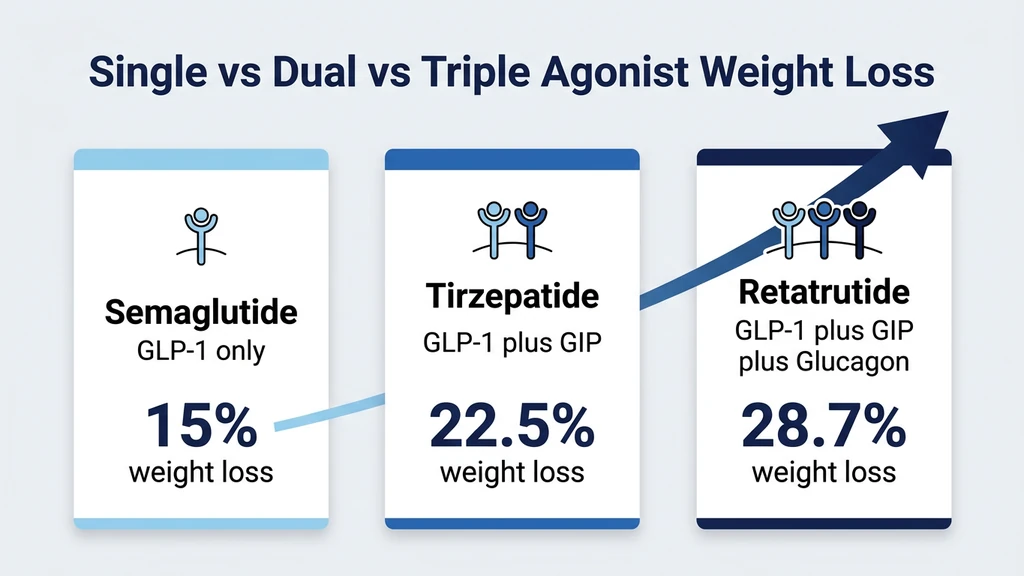
Older weight loss drugs carry one key. Semaglutide (Ozempic, Wegovy) opens the appetite door alone. Tirzepatide (Mounjaro, Zepbound) carries two keys, opening both appetite and metabolism. Retatrutide carries all three keys. It opens every door at once.
The technical term for this is "triple agonist." An agonist is simply a molecule that activates a receptor. A receptor is a protein on the surface of a cell that triggers a specific biological response when the right molecule binds to it. Retatrutide is shaped to fit three different receptor types, and each binding event triggers a distinct chain of effects in your body (Jastreboff et al., NEJM 2023).
This is not a theoretical advantage. Each additional receptor target has corresponded to roughly 6 to 8 extra percentage points of weight loss in clinical trials. One receptor produces about 15% loss. Two receptors produce about 22.5%. Three receptors produce 28.7%. The pattern is consistent and measurable.
How a 39-Amino-Acid Peptide Activates Three Receptors
Retatrutide is a synthetic peptide, a short chain of 39 amino acids designed in a laboratory to mimic natural gut hormones. Your body already produces GLP-1, GIP, and glucagon naturally after meals. These hormones last only minutes before enzymes break them down. Retatrutide was engineered with chemical modifications that resist enzymatic breakdown, extending its half-life to approximately 6 days (Coskun et al., Nature 2022).
A fatty acid chain attached to the peptide allows it to bind to albumin, a protein in your blood, which acts as a slow-release reservoir. This is the same strategy used in semaglutide and tirzepatide, but retatrutide's specific amino acid sequence was designed to engage all three receptor types with calibrated potency. It hits GLP-1 and GIP receptors at full strength while activating the glucagon receptor at a lower, controlled intensity to avoid dangerous blood sugar spikes.
The result: one injection, once per week, maintains therapeutic levels in your bloodstream for seven days straight. No daily pills, no multiple injections, no infusion centers.
GLP-1: The Appetite Brake
GLP-1 (glucagon-like peptide-1) is a hormone produced by L-cells in your small intestine after you eat. Its natural job is to tell your brain: "We have enough food. Stop eating." Retatrutide mimics this hormone, but instead of lasting 2 minutes like natural GLP-1, the synthetic version persists for days.
The appetite suppression works through two distinct pathways. First, GLP-1 receptor activation slows gastric emptying. Food stays in your stomach 30 to 40% longer than normal. You eat a quarter of a sandwich and feel like you ate the whole thing. Second, GLP-1 acts directly on the hypothalamus, the brain region that regulates hunger and satiety. It dampens the neural circuits that produce cravings and reduces the reward sensation from eating calorie-dense foods (Drucker, 2018).
This is the same mechanism behind Ozempic, Wegovy, and every other GLP-1 receptor agonist on the market. It is the most validated pathway in obesity pharmacology, with over a decade of clinical evidence. GLP-1 agonists also improve insulin secretion in a glucose-dependent manner, meaning they boost insulin only when blood sugar is elevated, which makes them effective for type 2 diabetes as well.
Why GLP-1 Alone Hits a Ceiling Around 15%
Semaglutide at its highest approved dose (2.4 mg weekly) produces approximately 15% body weight loss over 68 weeks. That was groundbreaking when the STEP 1 trial results published in 2021 (Wilding et al., NEJM 2021). But it also revealed a ceiling.
At 15% weight loss, your body fights back. Metabolic adaptation kicks in. Your resting metabolic rate drops. Hormones like leptin and ghrelin shift to make you hungrier. Your body interprets the weight loss as a threat and activates compensatory mechanisms to restore the lost mass. GLP-1 alone cannot overcome all of these defenses because it only addresses one side of the equation: how much you eat. It does nothing to increase how much energy you burn.
This is where the second and third receptors become critical. Retatrutide does not just rely on appetite suppression to push past the 15% barrier. It recruits additional biological pathways that address metabolism and energy expenditure directly. For a comparison of dosing protocols across GLP-1 agonists, see our peptide dosage chart.
GIP: The Metabolic Booster
GIP (glucose-dependent insulinotropic polypeptide) is a hormone released by K-cells in the upper small intestine. For decades, researchers ignored GIP because early studies suggested it played a minor role in weight regulation. That changed when Eli Lilly combined GIP with GLP-1 in tirzepatide and saw weight loss jump from 15% to 22.5% (Jastreboff et al., NEJM 2022).
GIP activation does something GLP-1 cannot do on its own: it changes how your body distributes and processes fat. Research indicates that GIP signaling shifts fat storage away from visceral fat (the metabolically dangerous fat wrapped around your organs) toward subcutaneous fat (the less harmful fat under your skin). This redistribution alone improves metabolic health markers like insulin resistance, blood lipids, and inflammatory markers, even before significant weight loss occurs.
GIP also enhances insulin sensitivity in adipose tissue, making fat cells more responsive to metabolic signals. Think of it as upgrading your body's fat processing software. GLP-1 reduces the incoming load of food. GIP makes your body handle the remaining food more efficiently. The combination explains why tirzepatide produces 50% more weight loss than semaglutide despite sharing the GLP-1 component.
The GIP Paradox: Agonism vs. Antagonism
Here is something that puzzled researchers for years. Some studies showed that blocking GIP receptors also produced weight loss in animal models. How can both activating and blocking the same receptor lead to the same outcome?
The answer appears to involve receptor desensitization. At high sustained doses, GIP agonism may effectively downregulate the receptor over time, producing an effect that resembles antagonism at the cellular level. This paradox is still being investigated, but the clinical results are clear: adding GIP agonism to GLP-1 consistently improves weight loss outcomes in human trials (Samms et al., 2020).
In retatrutide, GIP works the same way it does in tirzepatide. The metabolic boosting effect is preserved. The difference is that retatrutide adds a third pathway on top of it, pushing results further than dual agonism alone. Use our tirzepatide dosage calculator to explore the dual agonist dosing, or the retatrutide dosage calculator for the triple agonist protocol.
Glucagon: The Fat Burner That Changes Everything
This is the receptor that separates retatrutide from every approved weight loss drug. Glucagon is a hormone produced by alpha cells in the pancreas. Its primary natural role: when blood sugar drops too low, glucagon tells the liver to convert stored glycogen into glucose and release it into the bloodstream. It is the body's emergency energy release switch.
But glucagon does more than rescue low blood sugar. It increases resting energy expenditure through a process called thermogenesis. Your body converts stored fat into heat. You burn more calories sitting in a chair, sleeping, or watching television. One study measured a 15 to 20% increase in energy expenditure following glucagon receptor activation in metabolic studies (Habegger et al., 2010).
If GLP-1 is the brake pedal on food intake and GIP is the tune-up for your engine, glucagon is the accelerator on fat burning. Retatrutide applies all three simultaneously. You eat less, process food better, and burn more energy at rest. No single-target or dual-target drug achieves this combination.
How Glucagon Clears Liver Fat
The liver is glucagon's primary target organ. When glucagon receptors on liver cells activate, they trigger fatty acid oxidation, the biochemical process of breaking down stored fat molecules and converting them into usable energy. The liver literally burns its own fat stores.
This explains retatrutide's remarkable liver fat data. In a substudy of 98 participants with metabolic dysfunction-associated steatotic liver disease (MASLD, formerly called fatty liver disease), the 12 mg dose reduced liver fat by 82.4%. At the 8 mg dose, 79% of participants saw their liver fat drop below the 5% threshold that defines a healthy liver (Hartman et al., Nature Medicine 2024).
Semaglutide reduces liver fat by roughly 40 to 50%, primarily as a downstream effect of overall weight loss. Tirzepatide improves that to about 55%. Retatrutide nearly doubles both because it attacks liver fat from two directions: indirect reduction through body weight loss and direct fat burning in liver cells through glucagon signaling. For anyone with elevated liver enzymes or an ultrasound showing fatty liver, this distinction is clinically significant.
The Blood Sugar Balancing Act
Here is the obvious concern with activating glucagon receptors: glucagon raises blood sugar. That is its primary biological function. Giving a glucagon agonist to someone with type 2 diabetes sounds counterproductive. Why stimulate a hormone that increases glucose production?
The answer is elegant engineering. Retatrutide's GLP-1 and GIP components counterbalance the glucose-raising effect of glucagon. GLP-1 stimulates insulin release and suppresses glucagon secretion from the pancreas (note: this is natural glucagon suppression, distinct from the drug's glucagon receptor activation). GIP further enhances insulin sensitivity. The net effect: blood sugar stays stable or even improves, while the fat-burning benefits of glucagon are fully captured (Coskun et al., Nature 2022).
In the Phase 2 trial, participants with type 2 diabetes saw their HbA1c (a measure of average blood sugar over 3 months) drop by up to 2.02 percentage points. This is a clinically meaningful improvement, comparable to tirzepatide in type 2 diabetes trials. The glucagon component did not cause hyperglycemia because the other two receptors held blood sugar in check.
Why Three Receptors Beat Two: The Quantified Case
Each generation of incretin-based obesity drugs has added a receptor target and gained a measurable increment in efficacy. The progression is not theoretical. It is documented across multiple independent clinical trials with thousands of participants.
| Generation | Drug | Receptors | Max Weight Loss | Trial Duration | Key Trial |
|---|---|---|---|---|---|
| First | Semaglutide (Wegovy) | GLP-1 | ~15% | 68 weeks | STEP 1 (Wilding et al., 2021) |
| Second | Tirzepatide (Zepbound) | GLP-1 + GIP | ~22.5% | 72 weeks | SURMOUNT-1 (Jastreboff et al., 2022) |
| Third | Retatrutide | GLP-1 + GIP + Glucagon | 28.7% | 68 weeks | TRIUMPH-4 (Lilly, Dec 2025) |
The increments are consistent: +7.5 percentage points from adding GIP, then +6.2 percentage points from adding glucagon. This pattern suggests that each receptor contributes a distinct, additive mechanism rather than simply amplifying the same pathway. You are not getting "more of the same." You are getting three different biological levers pulling in the same direction.
A direct comparison is important: these numbers come from separate trials with different patient populations, different durations, and different starting BMIs. A head-to-head trial comparing retatrutide directly against tirzepatide (NCT06662383, 800 participants) will report results around December 2026. That will be the first apples-to-apples comparison under identical conditions. For a detailed breakdown of retatrutide versus tirzepatide across every metric, see our retatrutide vs tirzepatide comparison.
What Each Receptor Contributes to Weight Loss
Breaking down the contribution of each receptor helps explain why the triple combination is more than the sum of its parts.
GLP-1 contributes approximately 15 percentage points of weight loss. This comes almost entirely from reduced calorie intake. People eat 20 to 35% fewer calories because they feel full faster and experience fewer cravings. This is the most well-studied pathway, with consistent results across semaglutide, liraglutide, and other GLP-1 agonists.
GIP adds approximately 7 to 8 percentage points. This comes from improved metabolic efficiency, fat redistribution, and enhanced satiety signaling. The combination of GLP-1 and GIP produces a more robust appetite suppression effect than either hormone alone, while also improving how the body handles the calories that are consumed.
Glucagon adds approximately 6 to 7 percentage points. This comes from increased energy expenditure and direct fat oxidation, particularly in the liver. Unlike the first two receptors, glucagon acts on the output side of the energy equation. You are not just eating less. You are burning more. This is the metabolic advantage that pushed retatrutide past the 25% threshold.
The interaction effects between all three receptors may also play a role. GIP appears to amplify the appetite-suppressing effect of GLP-1, while glucagon's thermogenic effect may be enhanced in the context of improved insulin signaling from the other two pathways. For dosing guidance on each generation of drug, see our semaglutide dosage calculator or retatrutide dosage guide.
Clinical Trial Results: The Numbers Behind the Mechanism
Understanding how retatrutide works is useful. Seeing the clinical data that proves it works is essential. Two major trials provide the foundation for everything claimed about this drug.
Phase 2 Trial: 338 Patients, 48 Weeks
Published in the New England Journal of Medicine in July 2023, this was the first large trial of retatrutide in humans with obesity. Led by researcher Anja Jastreboff at Yale, it randomized 338 adults to one of five retatrutide doses or placebo and tracked them for 48 weeks (Jastreboff et al., NEJM 2023).
| Dose | Weight Loss at 24 Weeks | Weight Loss at 48 Weeks | Achieved 15%+ Loss |
|---|---|---|---|
| Placebo | -1.6% | -2.1% | 0% |
| 1 mg | -7.2% | -8.7% | ~10% |
| 4 mg | -12.9% | -17.1% | ~65% |
| 8 mg | -17.3% | -22.8% | ~75% |
| 12 mg | -17.5% | -24.2% | 83% |
Two findings jumped out. First, weight loss was still accelerating at 48 weeks. The slope of the weight loss curve had not flattened. This suggested longer treatment would produce even greater results, a prediction confirmed by the Phase 3 data. Second, at the 12 mg dose, every single participant lost at least 5% of their body weight. That 100% response rate is unusual in obesity trials, where 20 to 30% of patients on semaglutide fail to lose meaningful weight.
Phase 3 TRIUMPH-4: 445 Patients, 68 Weeks
The first Phase 3 results came from TRIUMPH-4, which enrolled 445 adults with obesity and knee osteoarthritis. Results were announced in December 2025, covering 68 weeks (about 16 months) of treatment (Lilly Press Release, Dec 2025).
| Metric | 9 mg Dose | 12 mg Dose | Placebo |
|---|---|---|---|
| Average weight loss | 26.4% (64.2 lbs) | 28.7% (71.2 lbs) | 2.1% |
| Knee pain improvement | Significant | 75.8% reduction | Moderate |
| Blood pressure reduction | Significant | 14 mmHg systolic | Modest |
The 28.7% result exceeded what most researchers expected. To put it in perspective: a person weighing 250 pounds at baseline would weigh about 178 pounds after 16 months on the 12 mg dose. That is a transformation from a BMI of 40 (severely obese) to a BMI of 28.7 (barely overweight).
The weight loss curve was still descending at the 68-week mark. The final number with longer treatment could be even higher. Seven additional Phase 3 trials are running under the TRIUMPH program, including a main obesity trial (TRIUMPH-1, 2,300 participants) expected to report in mid-2026.
The Broader TRIUMPH Program
Eli Lilly is running a comprehensive set of Phase 3 trials to test retatrutide across multiple conditions. The full program includes over 5,800 participants across seven trials.
| Trial | Condition | Participants | Expected Results |
|---|---|---|---|
| TRIUMPH-1 | Obesity (primary) | 2,300 | Mid-2026 |
| TRIUMPH-2 | Obesity + Type 2 Diabetes | 1,000 | Mid-2026 |
| TRIUMPH-3 | MASLD (fatty liver) | 700+ | 2026-2027 |
| TRIUMPH-4 | Obesity + Knee OA | 445 | Reported Dec 2025 |
| Head-to-head vs. Tirzepatide | Direct comparison | 800 | Dec 2026 |
The head-to-head trial against tirzepatide (NCT06662383) is the most anticipated. Cross-trial comparisons are useful but imperfect. Identical conditions, identical patient selection, identical endpoints will give a definitive answer about whether the third receptor truly produces clinically superior outcomes. For a preview of how the two drugs compare based on existing data, see our retatrutide vs tirzepatide analysis.
Beyond Weight Loss: Liver Fat and Diabetes Benefits
The headline weight loss numbers dominate media coverage. But two additional findings from retatrutide trials may matter just as much for long-term health outcomes.
Liver Fat: 82% Reduction That No Other Drug Matches
Metabolic dysfunction-associated steatotic liver disease (MASLD), previously called nonalcoholic fatty liver disease (NAFLD), affects roughly 25% of adults in the United States. It is the most common chronic liver condition in the world. Left untreated, it can progress to inflammation (steatohepatitis), scarring (fibrosis), cirrhosis, and liver cancer. Until recently, no approved drug existed specifically for MASLD.
A substudy published in Nature Medicine in 2024 enrolled 98 participants from the Phase 2 trial who had confirmed MASLD. The results were striking (Hartman et al., Nature Medicine 2024):
| Dose | Liver Fat Reduction | Liver Fat Normalized (<5%) |
|---|---|---|
| Placebo | +0.3% (worsened) | 0% |
| 1 mg | -42.9% | 27% |
| 4 mg | -57.0% | 52% |
| 8 mg | -81.4% | 79% |
| 12 mg | -82.4% | 86% |
At the 12 mg dose, 86 out of 100 participants with fatty liver had their liver fat return to healthy levels within 24 weeks. No liver toxicity was observed from the drug itself. The glucagon receptor is the driving force. Glucagon directly instructs liver cells to oxidize (burn) their stored fat. Semaglutide and tirzepatide reduce liver fat indirectly by lowering overall body weight. Retatrutide attacks from both directions: overall weight reduction plus direct hepatic fat burning.
A dedicated MASLD trial (TRIUMPH-3, NCT07035093) is part of the Phase 3 program. If the results hold, retatrutide could become the first drug approved for both obesity and MASLD, addressing two epidemics with a single injection.
Type 2 Diabetes: HbA1c Reduction Up to 2.02 Points
In the Phase 2 trial, a subset of 281 participants with type 2 diabetes received retatrutide or placebo for 36 weeks. The highest dose (12 mg) reduced HbA1c by 2.02 percentage points, bringing the average from a diabetic range down to near-normal levels (Rosenstock et al., Lancet 2023).
For context, an HbA1c of 6.5% or above indicates diabetes. A drop of 2 percentage points from, say, 8.5% to 6.5% represents a meaningful transition from poorly controlled diabetes to the diagnostic threshold. Many participants crossed below 6.5%, effectively achieving glycemic remission while on the drug.
The triple mechanism is particularly well-suited for type 2 diabetes. GLP-1 enhances insulin secretion when blood sugar is elevated. GIP improves insulin sensitivity in peripheral tissues. And while glucagon normally raises blood sugar, the counterbalancing effects of GLP-1 and GIP prevent hyperglycemia while allowing glucagon's fat-burning benefits to operate freely. The TRIUMPH-2 trial (1,000 participants with obesity and type 2 diabetes) will provide the definitive Phase 3 data.
How Retatrutide Compares to Every Other Weight Loss Drug
The obesity drug landscape has expanded dramatically since 2021. Here is how retatrutide stacks up against every major competitor, approved or in development.
| Drug | Mechanism | Receptors | Max Weight Loss | Liver Fat Reduction | FDA Status | Dosing |
|---|---|---|---|---|---|---|
| Semaglutide (Wegovy) | Single agonist | GLP-1 | ~15% (68 wk) | ~40-50% | Approved 2021 | Weekly injection |
| Tirzepatide (Zepbound) | Dual agonist | GLP-1 + GIP | ~22.5% (72 wk) | ~55% | Approved 2023 | Weekly injection |
| Retatrutide | Triple agonist | GLP-1 + GIP + Glucagon | 28.7% (68 wk) | 82% | Phase 3 | Weekly injection |
| CagriSema (Novo Nordisk) | Dual hormone | GLP-1 + Amylin | ~20% | ~40% | Filed 2026 | Weekly injection |
| Orforglipron (Eli Lilly) | Single agonist | GLP-1 (oral) | ~14-15% | TBD | Phase 3 | Daily pill |
| Survodutide (Boehringer) | Dual agonist | GLP-1 + Glucagon | ~15% (46 wk) | ~65% | Phase 3 | Weekly injection |
Several patterns emerge from this comparison. Retatrutide leads on two metrics: total weight loss and liver fat reduction. No other drug comes close on either measure. Survodutide also targets glucagon (paired with GLP-1, without GIP) and shows strong liver data (~65% fat reduction), but its weight loss numbers lag behind retatrutide, likely because it lacks the GIP component.
CagriSema pairs GLP-1 with amylin, a different satiety hormone. It may preserve more lean muscle mass during weight loss, but its total weight loss (~20%) falls short of both tirzepatide and retatrutide. Orforglipron represents a different value proposition entirely: a daily pill with no needles, targeting patients who refuse injections.
Outside the incretin drug class, other peptides target body composition through different pathways. AOD-9604 is a fragment of human growth hormone that stimulates lipolysis without affecting blood sugar. CJC-1295 increases growth hormone release, which supports lean mass preservation during weight loss. Neither approaches retatrutide's efficacy for total weight reduction, but they operate through entirely different mechanisms and are sometimes used alongside GLP-1 agonists in clinical practice.
For a detailed head-to-head breakdown of the two closest competitors, see our retatrutide vs tirzepatide comparison. Check for potential interactions between any of these compounds using our peptide interaction checker.
Timeline: What to Expect Week by Week on Retatrutide
Based on Phase 2 and Phase 3 trial data, here is the expected progression for someone starting retatrutide at the standard titration schedule. Individual results vary significantly, but the general pattern is consistent across published data.
| Timeframe | Dose (Typical) | What Happens | Expected Weight Loss |
|---|---|---|---|
| Weeks 1-4 | 2 mg | Mild appetite reduction begins. GI side effects (nausea, mild diarrhea) may appear. Stomach adjusts to slower emptying. | 2-3% |
| Weeks 5-8 | 4 mg | Appetite suppression becomes noticeable. Portion sizes naturally decrease. Nausea often peaks during first week at new dose, then fades. | 5-7% |
| Weeks 9-12 | 8 mg | Strong appetite reduction. Food noise (constant background thinking about food) diminishes substantially. Energy expenditure begins increasing from glucagon activation. | 9-13% |
| Weeks 13-24 | 12 mg | Full therapeutic effect. Maximum appetite suppression and energy expenditure. Weight loss accelerates. Liver fat dropping rapidly. | 15-18% |
| Weeks 24-48 | 12 mg | Steady weight loss continues without plateau. Unlike single-agonist drugs, the glucagon component helps resist metabolic adaptation. | 20-24% |
| Weeks 48-68 | 12 mg | Weight loss continues but rate begins slowing. Body approaches new equilibrium. 28.7% average loss achieved at 68 weeks. | 25-29% |
Two observations from the clinical data stand out. First, retatrutide did not show the weight loss plateau that typically appears at 6 to 9 months with semaglutide. The glucagon component appears to resist metabolic adaptation by actively increasing energy expenditure, counteracting the body's natural tendency to conserve energy during calorie restriction. Second, the side effect burden is front-loaded. Most GI complaints resolve within the first 12 weeks as the body adjusts to each dose level.
For the complete dosing protocol with injection preparation instructions, see our retatrutide dosage guide. Calculate your personalized dose schedule with our retatrutide dosage calculator. For general injection technique, see our peptide injections complete guide.
Side Effects: The Trade-Off for Three Receptors
More receptor targets means more biological activity, and that means more side effects. Retatrutide's side effect profile is manageable for most people but noticeably heavier than semaglutide or tirzepatide.
| Side Effect | Retatrutide 12 mg | Tirzepatide 15 mg | Semaglutide 2.4 mg |
|---|---|---|---|
| Nausea | 43% | 31% | 44% |
| Diarrhea | 33% | 23% | 30% |
| Vomiting | 21% | 12% | 24% |
| Constipation | 25% | 17% | 24% |
| Dysesthesia | 20.9% | Rare | Rare |
| Discontinuation rate | 18.2% | ~7% | ~7% |
The GI side effects (nausea, diarrhea, vomiting, constipation) follow the same pattern as other incretin drugs: they peak during dose escalation and improve significantly at stable doses. Slow titration (increasing the dose every 4 weeks) substantially reduces their severity.
The notable outlier is dysesthesia, a new side effect unique to retatrutide. This presents as tingling, burning, or abnormal skin sensitivity, sometimes described as the feeling of a foot falling asleep, but in random body areas. It affected 20.9% of participants at 12 mg and 8.8% at 9 mg. The glucagon receptor is the suspected cause, as drugs without glucagon activation do not produce this effect. In the Phase 3 trial, dysesthesia was generally mild and did not cause significant discontinuation (BioSpace, Dec 2025).
For a comprehensive guide to managing these side effects including timing strategies and dietary adjustments, see our retatrutide side effects guide. For general safety principles when using any peptide, see our peptide safety guide.
Frequently Asked Questions
Frequently Asked Questions
How does retatrutide work differently from Ozempic?
Ozempic (semaglutide) activates one receptor: GLP-1, which reduces appetite and slows digestion. Retatrutide activates three receptors: GLP-1, GIP, and glucagon. The additional GIP receptor improves metabolic fat processing. The glucagon receptor increases energy expenditure and directly burns liver fat. This triple mechanism produces 28.7% weight loss versus approximately 15% for Ozempic.
What does triple agonist mean in simple terms?
An agonist is a molecule that activates a specific receptor in your body. A triple agonist activates three different receptors simultaneously. Retatrutide activates GLP-1 (appetite suppression), GIP (metabolic improvement), and glucagon (fat burning). Each receptor controls a different biological process. Activating all three produces greater combined effects than targeting one or two receptors alone.
Is the glucagon receptor activation dangerous?
Glucagon naturally raises blood sugar, which is a concern for people with diabetes. In retatrutide, the GLP-1 and GIP components counterbalance this effect. Phase 2 trial data showed blood sugar improvements (HbA1c dropped up to 2.02 points), not increases. However, glucagon activation is the likely cause of dysesthesia (tingling skin sensations) reported in about 1 in 5 people at the highest dose.
How long does retatrutide stay in your system?
Retatrutide has a half-life of approximately 6 days. This means it takes about 6 days for half the drug to clear your system. After stopping, it takes roughly 4 to 5 half-lives (24 to 30 days) for the drug to fully clear. The long half-life is why once-weekly dosing maintains consistent therapeutic levels without daily administration.
Can retatrutide reverse fatty liver disease?
In a clinical substudy of 98 participants with MASLD (fatty liver disease), retatrutide at 12 mg reduced liver fat by 82.4% over 24 weeks. Among those participants, 86% had their liver fat return to healthy levels below 5%. These results are the strongest liver fat data for any obesity drug tested so far, driven by glucagon receptor activation in liver cells.
Why does retatrutide cause more nausea than other weight loss drugs?
Retatrutide activates three receptor pathways instead of one or two. The GLP-1 component slows gastric emptying by 30 to 40%, and the combined signaling from all three receptors produces stronger GI effects during the adjustment period. Nausea rates are about 43% on the 12 mg dose, compared to 31% for tirzepatide. Most nausea resolves within the first 4 to 8 weeks at each dose level.
When will retatrutide be FDA approved?
Eli Lilly has not confirmed a submission date, but the most likely timeline is: application filing in late 2026 or early 2027, FDA review over 6 to 10 months, and pharmacy availability in late 2027 or early 2028. The main Phase 3 trial (TRIUMPH-1, 2,300 participants) is expected to report results in mid-2026. For access options today, see our guide to getting retatrutide.
Does retatrutide work for people who plateaued on semaglutide or tirzepatide?
No published data directly addresses switching from semaglutide or tirzepatide to retatrutide. However, the mechanism supports the concept. If GLP-1 alone produced a plateau at 15%, adding GIP and glucagon activation targets metabolic pathways that GLP-1 does not reach. The glucagon component increases energy expenditure, which could overcome the metabolic adaptation that causes plateaus on single-agonist drugs.
The Bottom Line
Retatrutide works through a mechanism that no approved drug replicates. Three receptor targets. Three distinct biological effects. GLP-1 reduces how much you eat. GIP improves how your body processes food and fat. Glucagon increases how much energy you burn at rest and directly clears fat from your liver. The result is 28.7% weight loss, 82% liver fat reduction, and meaningful improvements in blood sugar control.
The clinical data is early but compelling. Phase 2 results in the New England Journal of Medicine. Phase 3 results confirming and exceeding those numbers. Seven ongoing trials with over 5,800 participants. A head-to-head comparison against tirzepatide due in December 2026 will be the most important data point of the year.
Retatrutide is not available yet. It cannot be prescribed at any pharmacy in the world as of March 2026. For researchers working with the compound, see our guide on how to reconstitute retatrutide. If you need treatment now, semaglutide and tirzepatide are proven, FDA-approved, and available today. Starting either one does not prevent switching to retatrutide after approval. For current options, explore our peptide dosage chart, use our peptide interaction checker, or read our guide to getting retatrutide.
Related articles: - Does Tirzepatide Burn Fat? — how the dual agonist compares for fat loss - Why Am I Not Losing Weight on Semaglutide? — when a single agonist plateaus - Does Tirzepatide Cause Headaches? — common side effects shared across the GLP-1 class - Does Tirzepatide Cause Diarrhea? — GI side effects to expect with incretin agonists - Can You Drink Alcohol on Tirzepatide? — alcohol interactions with GLP-1 agonists
We will update this guide as TRIUMPH trial results report throughout 2026.
Helpful Tools
Related Articles
How Long Does Retatrutide Take to Work?
Retatrutide suppresses appetite within days, produces weight loss by week 4, and delivers up to 24.2% loss at 48 weeks in trials.
GLP-3 Peptide: What It Really Is
GLP-3 does not exist. What clinics call 'GLP-3' is retatrutide (LY3437943), Eli Lilly's triple agonist targeting GLP-1, GIP, and glucagon receptors.
Retatrutide Availability & Timeline
Retatrutide is expected to receive FDA approval in mid-2027 with pharmacy availability in late 2027. Full timeline and Phase 3 trial status.
Retatrutide: Mechanism & Trial Results
Retatrutide (LY3437943) is a triple agonist weight loss drug by Eli Lilly. 28.7% weight loss in trials, 82% liver fat reduction. Not yet FDA-approved.