You injected your fourth weekly dose of tirzepatide yesterday. By mid-afternoon, a dull pressure settled behind your eyes and spread across your forehead. You took ibuprofen. It helped for three hours, then the pain returned. Yes, tirzepatide can cause headaches. Clinical trials report headache rates of 9-18% depending on dose, compared to 6-9% on placebo. Most headaches are mild, peak during the first 4-8 weeks, and resolve as the body adapts to the drug.
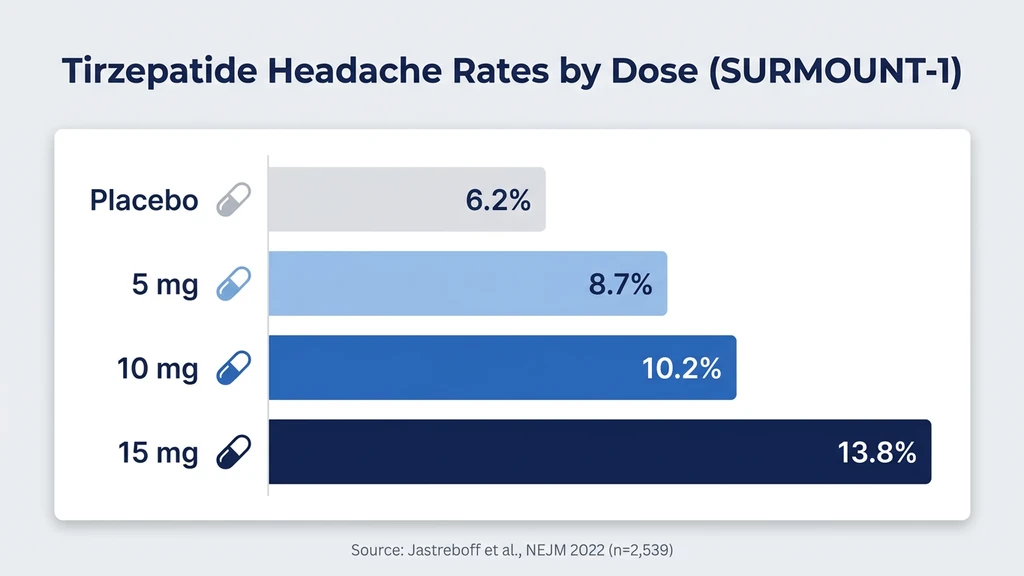
The SURMOUNT-1 trial documented headaches in 8.7% of participants on 5 mg, 10.2% on 10 mg, and 13.8% on 15 mg, versus 6.2% on placebo (Jastreboff et al., NEJM 2022). In the SURPASS program for type 2 diabetes, rates ran slightly higher across doses, with the SURPASS-1 monotherapy trial reporting headache in 12.4-18.0% of tirzepatide arms versus 8.9% placebo (Rosenstock et al., 2021).
| Quick Reference | Details |
|---|---|
| Prevalence | 8.7% (5 mg), 10.2% (10 mg), 13.8% (15 mg) in SURMOUNT-1 |
| Main causes | Dehydration, blood sugar shifts, GLP-1 receptor effects, caloric restriction |
| Onset | Days 1-7 after starting or dose escalation |
| Peak | Weeks 2-4 at each dose level |
| Resolution | 4-8 weeks at a stable dose |
| Key fix | 80-100 oz water + electrolytes daily |
| Evidence level | Phase 3 clinical trials (SURMOUNT-1, SURPASS-1 through SURPASS-5) |
For dosing protocols, see our tirzepatide dosage chart. For safety information, see our peptide safety guide.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
What Causes Headaches on Tirzepatide?
Picture your brain floating in a thin cushion of fluid inside your skull. That fluid depends on precise hydration, stable glucose, and balanced electrolytes. Tirzepatide disrupts all three simultaneously, especially during the first weeks of treatment and after each dose increase.
Four mechanisms drive headaches in tirzepatide users. Most people experience a combination rather than a single cause.
1. Dehydration from reduced fluid intake
Tirzepatide suppresses appetite and thirst through GLP-1 and GIP receptor activation in the hypothalamus. Users report drinking 20-30% less water without realizing it. A study examining GLP-1 agonist effects on fluid balance found that reduced oral intake combined with increased renal sodium excretion produced a net fluid deficit in the first 2-4 weeks of therapy (Blonde et al., 2022). Dehydration shrinks the brain's protective fluid cushion. The brain tugs against its anchoring membranes. The result is a diffuse, pressure-like headache that worsens in the afternoon.
2. Blood sugar fluctuations
Tirzepatide lowers fasting glucose by 35-60 mg/dL in type 2 diabetes trials (Rosenstock et al., 2021). Non-diabetic users eating fewer calories on a powerful appetite suppressant may experience relative hypoglycemia, blood sugar dropping from a habitual 100-110 mg/dL to 70-80 mg/dL. The brain, which consumes 20% of the body's glucose despite weighing 2% of its mass, responds to this shift with headache, lightheadedness, and irritability. These episodes typically occur 2-4 hours after meals.
3. GLP-1 receptor-mediated effects on the central nervous system
GLP-1 receptors exist throughout the brainstem, hypothalamus, and area postrema. Activation alters neurotransmitter signaling, including serotonin and dopamine pathways involved in pain perception. A review of GLP-1 receptor agonist neurological effects found that central receptor activation modulates nociceptive processing and may lower the headache threshold in susceptible individuals (Baggio & Drucker, 2014). This mechanism explains why some users develop headaches even with adequate hydration and stable blood sugar.
4. Caloric restriction and nutrient shifts
Reducing daily intake from 2,200 calories to 1,200 calories, common on tirzepatide, triggers a metabolic adjustment period. Caffeine intake often drops with overall food and beverage consumption. Caffeine withdrawal headaches start 12-24 hours after the last dose and peak at 20-51 hours (Juliano & Griffiths, 2004). Sodium and magnesium levels also shift as appetite decreases, contributing to electrolyte-related head pain.
Clinical Trial Data: How Common Are Headaches?
Headache is one of the most frequently reported adverse events across the entire tirzepatide clinical program. Two large trial families provide the clearest picture.
SURMOUNT-1: Obesity Without Diabetes
SURMOUNT-1 enrolled 2,539 adults with obesity (BMI 30+) or overweight (BMI 27+) with at least one weight-related condition. Participants received tirzepatide 5 mg, 10 mg, or 15 mg versus placebo for 72 weeks. Headache was among the top five adverse events (Jastreboff et al., 2022).
| SURMOUNT-1 | 5 mg (n=630) | 10 mg (n=636) | 15 mg (n=630) | Placebo (n=643) |
|---|---|---|---|---|
| Headache | 8.7% | 10.2% | 13.8% | 6.2% |
| Nausea | 24.6% | 33.3% | 31.0% | 9.5% |
| Constipation | 6.2% | 9.2% | 11.7% | 3.9% |
| Weight loss | -16.0% | -21.4% | -22.5% | -3.1% |
The dose-response pattern is clear: higher doses produce more headaches, more nausea, and more weight loss. The 15 mg group reported headache at more than double the placebo rate.
SURPASS Trials: Type 2 Diabetes
The SURPASS program tested tirzepatide in people with type 2 diabetes, a different population with distinct metabolic profiles.
SURPASS-1 (monotherapy) reported headache in 12.4% (5 mg), 15.4% (10 mg), and 18.0% (15 mg) versus 8.9% on placebo (Rosenstock et al., 2021). Higher rates compared to SURMOUNT-1 may reflect the additional burden of blood sugar changes in a diabetic population, where glucose swings are larger and more symptomatic.
| SURPASS-1 (Diabetes) | 5 mg | 10 mg | 15 mg | Placebo |
|---|---|---|---|---|
| Headache | 12.4% | 15.4% | 18.0% | 8.9% |
| HbA1c reduction | -1.87% | -1.89% | -2.07% | +0.04% |
SURPASS-2, which compared tirzepatide head-to-head against semaglutide, found headache rates of 10.4-13.0% with tirzepatide versus 11.8% with semaglutide 1 mg. The difference was not statistically significant, suggesting headache risk is a class effect of GLP-1 receptor agonists rather than unique to tirzepatide (Frias et al., 2021).
Key takeaway: Expect headache in roughly 1 out of 8 to 1 out of 6 users depending on dose. Most cases are mild to moderate, and fewer than 1% of trial participants discontinued tirzepatide because of headaches alone.
Headache Types: What Users Report
Not all tirzepatide headaches feel the same. Identifying the type helps target the right fix.
Tension-Type Headache
The most common type on tirzepatide. A steady, bilateral pressure around the forehead and temples, like wearing a hat two sizes too small. Intensity ranges from 3/10 to 5/10 on a pain scale. Usually starts in the afternoon and persists for 2-6 hours.
Tension-type headaches on tirzepatide trace back to dehydration and the stress of caloric restriction. The paracervical and temporalis muscles tighten as hydration drops. Standard over-the-counter analgesics (acetaminophen 500-1000 mg or ibuprofen 200-400 mg) resolve most episodes within 30-60 minutes.
Dehydration Headache
Distinct from tension headache by one feature: it worsens when you stand up quickly. A dehydration headache feels like the brain is sloshing against the skull, worse with movement and positional changes. Often accompanied by dark urine, dry mouth, and fatigue that many tirzepatide users report.
Tirzepatide reduces thirst signaling via hypothalamic GLP-1 receptors. Many users on 10-15 mg report that they "forget to drink" because the normal thirst cue weakens alongside appetite suppression. A person who normally drinks 70 ounces of water daily may drop to 40-50 ounces without noticing. That 30% reduction, sustained over several days, produces a clinically meaningful fluid deficit.
The fix is mechanical: set hourly water reminders. Drink before you feel thirsty. Add electrolyte packets to one or two glasses per day. Most dehydration headaches resolve within 2-4 hours of rehydrating with 16-32 ounces of electrolyte-enhanced water.
Blood Sugar Headache
This headache appears 2-4 hours after meals and comes with shaking hands, sweating, irritability, or brain fog. It signals relative hypoglycemia: blood sugar that is technically in the normal range (65-80 mg/dL) but lower than your body is accustomed to.
Non-diabetic users rarely hit true hypoglycemia (below 54 mg/dL) on tirzepatide monotherapy. But a person whose fasting glucose typically runs 105 mg/dL will feel symptoms at 75 mg/dL because the brain calibrates its "normal" based on recent averages. This adaptation takes 2-4 weeks.
Small, protein-rich snacks every 3-4 hours prevent the glucose dips. A handful of almonds, a hard-boiled egg, or a protein shake containing 20-30 grams of protein provides a slow, steady glucose source that bypasses the rapid swings.
Users on tirzepatide who also take sulfonylureas or insulin face genuine hypoglycemia risk. SURPASS-3 documented a 14% rate of hypoglycemia when tirzepatide was combined with insulin degludec, compared to just 1.2% on tirzepatide alone (Ludvik et al., 2021). If you take insulin or sulfonylureas, discuss dose adjustments with your prescriber before starting tirzepatide. Check our peptide interaction checker for more information.
Caffeine Withdrawal Headache
This one surprises people. Before tirzepatide, you drank three cups of coffee daily. After starting, you lost interest in your second and third cups because appetite suppression extends to beverages. Your daily caffeine dropped from 300 mg to 100 mg without deliberate effort.
Caffeine withdrawal headache is bilateral, throbbing, and typically starts 12-24 hours after the usual caffeine dose is missed. It peaks at 20-51 hours and can last 2-9 days (Juliano & Griffiths, 2004). The cure is simple: maintain your caffeine intake deliberately, or taper by 25% per week if you want to reduce consumption.
When Do Tirzepatide Headaches Start and Stop?
Headaches on tirzepatide follow a predictable pattern tied to dose initiation and escalation.
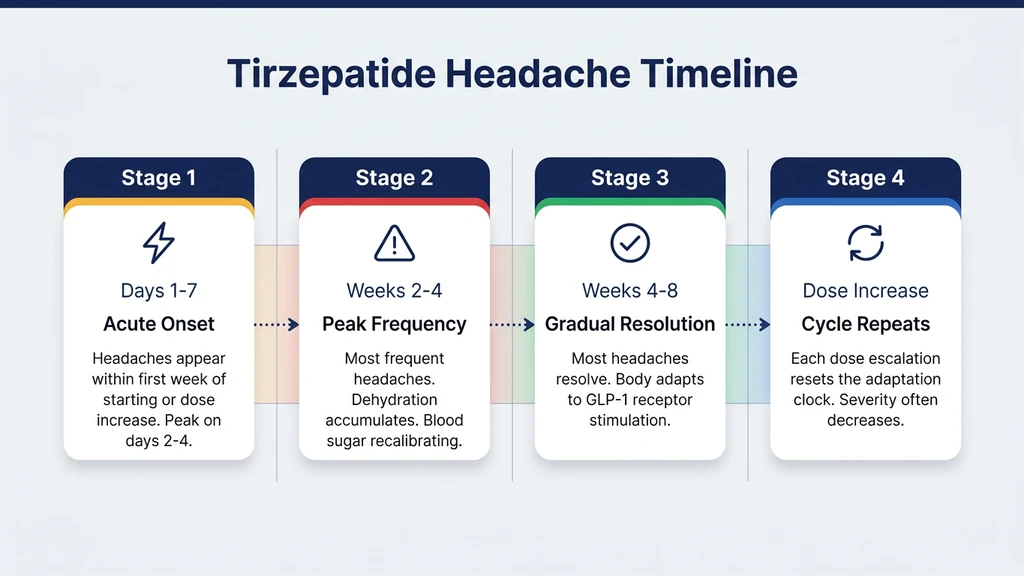
Days 1-7: Acute Onset
Headaches appear within the first week of starting tirzepatide or within 3-5 days of a dose increase. The body encounters a sudden surge in GLP-1 and GIP receptor activation. Appetite drops. Fluid intake falls. Blood sugar shifts. For most users, the headache peaks on days 2-4 and is mild enough to manage with over-the-counter pain relief.
SURMOUNT-1 recorded adverse events throughout the 72-week trial. The highest density of headache reports clustered in the first 4 weeks of each new dose level, confirming the dose-transition trigger (Jastreboff et al., 2022).
Weeks 2-4: Peak Frequency
Headaches are most frequent during weeks 2-4 at each dose. The gap between the body's old equilibrium and the new pharmacological state is widest. Dehydration accumulates if hydration habits have not changed. Blood sugar may still be recalibrating.
Users who escalate from 5 mg to 10 mg often describe a "second wave" of headaches that feels like starting the drug over again. This is normal. Each dose escalation resets the adaptation clock.
Weeks 4-8: Gradual Resolution
Most headaches resolve within 4-8 weeks at a stable dose. The body upregulates compensatory mechanisms, including restored thirst signaling, improved glucose homeostasis, and neurological adaptation to sustained GLP-1 receptor stimulation. A review of GLP-1 agonist tolerability confirmed that most neurological side effects, including headache, attenuate with continued exposure at a fixed dose (Nauck et al., 2021).
If headaches persist beyond 8 weeks at a stable dose, investigate secondary causes: medication interactions, vision changes, sleep quality, or blood pressure shifts. Keep in mind that tirzepatide stays in your system for weeks after each injection, so side effects can linger even between doses.
After Dose Increases: The Cycle Repeats
Standard tirzepatide titration moves from 2.5 mg to 5 mg to 7.5 mg to 10 mg to 12.5 mg to 15 mg, each step separated by 4 weeks. Users who experience headaches at each transition can expect the pattern to repeat at each escalation, though severity often decreases with successive increases.
Slower titration, spending 6-8 weeks at each dose instead of 4, reduces headache severity significantly. Discuss extended titration with your prescriber if headaches are affecting daily function. Our tirzepatide dosage calculator helps plan different titration schedules.
Quantified Danger: When a Headache Signals Something Serious
Most tirzepatide headaches are nuisances, not emergencies. But certain patterns demand immediate medical evaluation. Here is how to distinguish between a normal side effect and a warning sign.
Thunderclap headache (pain reaching maximum intensity within 60 seconds)
This is never normal. A headache that hits peak severity in under a minute raises concern for subarachnoid hemorrhage, cerebral venous thrombosis, or hypertensive emergency. This requires emergency evaluation regardless of tirzepatide use. Call 911 or go to the nearest emergency department.
Headache with blood pressure above 180/120 mmHg
Tirzepatide typically lowers blood pressure by 4-8 mmHg systolic over time. A sudden spike above 180/120 mmHg with headache signals hypertensive urgency. Certain food interactions, missed blood pressure medications, or rebound hypertension from abruptly stopping antihypertensives can cause this. Take a reading if your headache is unusually severe. If systolic exceeds 180, seek same-day medical evaluation.
Headache with persistent vomiting lasting more than 24 hours
Nausea is common on tirzepatide, but vomiting that prevents fluid intake for more than 24 hours creates a dangerous dehydration spiral. Electrolyte imbalances from sustained vomiting can cause cardiac arrhythmias. If you cannot keep water down for 24 hours, seek medical attention.
Headache with visual changes (blurred vision, double vision, or vision loss)
New visual symptoms alongside headache may indicate increased intracranial pressure, a rare but documented concern with rapid weight changes. A case series documented idiopathic intracranial hypertension in patients with significant body weight fluctuations (Daniels et al., 2007). Vision changes with headache warrant urgent ophthalmological and neurological evaluation.
Headache with fever above 101.5F (38.6C) and neck stiffness
This combination suggests meningitis or encephalitis, unrelated to tirzepatide but critical to rule out. Do not assume a headache with fever and neck stiffness is a drug side effect. Seek emergency care.
Headache after a fall or head injury
Users experiencing lightheadedness from tirzepatide's blood sugar and blood pressure effects may fall. Post-traumatic headache, especially with confusion, nausea, or loss of consciousness, requires CT imaging to rule out intracranial hemorrhage.
| Red Flag | Timeframe | Action |
|---|---|---|
| Thunderclap (peak in <60 seconds) | Immediate | Call 911 |
| BP above 180/120 mmHg | Same day | Emergency or urgent care |
| Vomiting >24 hours | Same day | Emergency or urgent care |
| Visual changes | Same day | Urgent ophthalmology/neurology |
| Fever >101.5F + neck stiffness | Immediate | Emergency department |
| Post-fall headache with confusion | Immediate | Emergency department |
7 Strategies to Prevent and Treat Tirzepatide Headaches
These seven strategies target the four causes identified above. Most users resolve their headaches with the first three alone.
1. Drink 80-100 Ounces of Water Daily
This is the single most effective intervention. Tirzepatide suppresses thirst alongside appetite, so waiting until you feel thirsty means you are already dehydrated. Set a phone alarm every hour during waking hours. Keep a water bottle within arm's reach at all times.
Spread intake throughout the day. Chugging 32 ounces at once worsens the bloating and nausea that tirzepatide can already cause. Aim for 8-12 ounces per hour across 10-12 waking hours.
A practical test: your urine should be pale yellow. Dark yellow or amber means you need more water. Clear means you may be over-hydrating (which can dilute sodium and worsen headaches). Pale straw color is the target.
2. Add Electrolytes to Your Water
Water alone is not enough if sodium, potassium, and magnesium are depleted. Tirzepatide increases renal sodium excretion, and reduced food intake lowers dietary electrolyte consumption (Blonde et al., 2022).
Add an electrolyte packet (look for 500-1000 mg sodium, 200-400 mg potassium, 50-100 mg magnesium per serving) to 1-2 glasses of water daily. Brands like LMNT, Liquid IV, or Drip Drop are commonly used. Alternatively, add a pinch of salt and a squeeze of lemon to water.
Magnesium citrate (200-400 mg at bedtime) doubles as a headache preventive and a remedy for constipation, another common tirzepatide side effect. If you are managing both headaches and constipation, magnesium addresses both with a single supplement.
3. Eat Small Protein-Rich Meals Every 3-4 Hours
Blood sugar headaches respond to steady glucose delivery. Instead of two large meals, eat 4-5 small meals containing 20-30 grams of protein each. Protein provides a slow, stable glucose source through gluconeogenesis, preventing the rapid drops that trigger head pain.
Sample mini-meals: 2 hard-boiled eggs (12g protein), Greek yogurt with nuts (18-20g), a protein shake (25-30g), half a chicken breast with vegetables (25g). Even when tirzepatide suppresses appetite, small protein-focused portions are usually tolerable.
This strategy also protects against hair loss and fatigue, both driven by inadequate protein during rapid weight loss.
4. Maintain Your Caffeine Intake
If you drank 2-3 cups of coffee daily before tirzepatide, keep drinking them. Appetite suppression often extends to beverages, and inadvertent caffeine reduction causes withdrawal headaches that compound the drug's direct effects.
If you want to reduce caffeine, taper intentionally: cut by 25% per week. Going from 300 mg daily to 100 mg overnight produces a 2-9 day withdrawal headache on top of the tirzepatide adjustment. Separate the variables. Get stable on tirzepatide first, then reduce caffeine later if desired.
5. Use OTC Pain Relief Strategically
Acetaminophen (500-1000 mg every 6-8 hours, max 3000 mg daily) or ibuprofen (200-400 mg every 6-8 hours with food) resolves most tirzepatide headaches within 30-60 minutes. Ibuprofen is preferable for dehydration and tension headaches because it also reduces inflammation.
Two cautions: do not exceed 10 days of continuous NSAID use without medical guidance due to kidney and GI risk. And watch for medication overuse headache (rebound headache), which develops if you take pain relievers more than 15 days per month. If headaches require daily medication beyond the first 2 weeks, talk to your prescriber about preventive strategies rather than reactive pain relief.
6. Request a Slower Titration Schedule
Standard tirzepatide titration moves up every 4 weeks. If headaches are significant at each dose increase, ask your prescriber about extended titration: 6-8 weeks at each dose instead of 4. This gives the body more time to adapt and reduces the severity of side effects at each transition.
SURMOUNT-1 used a fixed 4-week titration. Real-world clinical practice allows flexibility. Many prescribers already use 6-week intervals for patients with prominent side effects. The weight loss is slightly slower but the trajectory remains the same. Our tirzepatide dosage chart outlines both standard and extended schedules.
7. Track Patterns with a Headache Diary
Record the timing, severity (1-10 scale), duration, and associated factors (hydration, meals, caffeine, sleep, dose day) for each headache. After 2-3 weeks, patterns emerge that reveal the primary cause.
If headaches cluster on injection days, the GLP-1 receptor surge is the likely driver, and a slower titration may help. If they peak in the afternoon, dehydration is probable. If they follow skipped meals, blood sugar is the culprit. Identifying the specific pattern lets you target the right strategy instead of guessing.
Bring the diary to your next prescriber visit. Objective data helps guide decisions about dose adjustments, supportive medications, or additional testing.
Tirzepatide vs Semaglutide: Which Causes More Headaches?
This is the most common question from users considering or switching between the two drugs. The SURPASS-2 head-to-head trial provides a direct answer.
SURPASS-2 randomized 1,879 adults with type 2 diabetes to tirzepatide 5 mg, 10 mg, or 15 mg versus semaglutide 1 mg for 40 weeks. Headache rates were comparable across all groups (Frias et al., 2021).
| Drug | Dose | Headache Rate | Weight Loss | HbA1c Reduction |
|---|---|---|---|---|
| Tirzepatide | 5 mg | 10.4% | -7.6% | -2.09% |
| Tirzepatide | 10 mg | 11.2% | -9.3% | -2.37% |
| Tirzepatide | 15 mg | 13.0% | -11.2% | -2.46% |
| Semaglutide | 1 mg | 11.8% | -5.7% | -1.86% |
Tirzepatide at 5 mg produced fewer headaches than semaglutide 1 mg. Tirzepatide at 15 mg produced slightly more. The range overlaps substantially. No statistically significant difference was found.
What does differ is the weight loss. Tirzepatide 15 mg produced nearly double the weight loss of semaglutide 1 mg (11.2% vs 5.7%). More aggressive weight loss means more dehydration, more caloric restriction, and more metabolic flux, all headache drivers. Per unit of weight lost, the headache burden is similar.
For users comparing tirzepatide and retatrutide, early Phase 2 data suggest retatrutide may produce similar or slightly higher GI side effect rates due to its triple receptor agonism (GLP-1 + GIP + glucagon). Our retatrutide vs tirzepatide comparison covers the full side effect profile.
Switching for headaches alone is unlikely to help. If headaches on tirzepatide 10 mg are troublesome, switching to semaglutide 2.4 mg will not eliminate them because the underlying causes (dehydration, caloric restriction, receptor activation) are shared. Instead, apply the seven strategies above. If those fail, discuss dose reduction or slower titration with your prescriber.
For users weighing a switch for other reasons, see our semaglutide to tirzepatide switching guide and semaglutide dosage calculator.
Important Warnings
Headache that is new, severe, or accompanied by any neurological symptom (vision changes, speech difficulty, weakness, confusion) is not a normal tirzepatide side effect. Seek immediate evaluation.
Do not exceed acetaminophen 3000 mg or ibuprofen 1200 mg in 24 hours without medical guidance. NSAIDs carry kidney and gastrointestinal risks, especially in dehydrated patients, which tirzepatide users are more likely to be.
Users who take insulin or sulfonylureas alongside tirzepatide face genuine hypoglycemia risk. SURPASS-3 documented a 14% hypoglycemia rate when tirzepatide was combined with insulin (Ludvik et al., 2021). Severe hypoglycemia causes headaches that precede confusion and loss of consciousness. Always carry glucose tablets if you use insulin.
Report persistent headaches lasting more than 8 weeks at a stable dose to your prescriber. While most headaches resolve, persistent cases may require investigation for secondary causes unrelated to tirzepatide (hypertension, sleep apnea, medication interactions).
For injection technique that minimizes discomfort and side effects, see our peptide injections complete guide.
Frequently Asked Questions
How common are headaches on tirzepatide?
SURMOUNT-1 data shows headache in 8.7% of users at 5 mg, 10.2% at 10 mg, and 13.8% at 15 mg, versus 6.2% on placebo. SURPASS-1 reported higher rates in diabetic patients (12.4-18.0%). Most cases are mild to moderate and resolve within 4-8 weeks at a stable dose. Fewer than 1% discontinued treatment for headache.
When do tirzepatide headaches go away?
Most headaches resolve within 4-8 weeks at a stable dose as the body adapts to GLP-1 receptor stimulation. Headaches typically recur for 1-2 weeks after each dose increase. Slower titration (6-8 weeks per step instead of 4) reduces the frequency and intensity of recurrences.
Does tirzepatide cause migraines?
Clinical trials do not distinguish between headache types in their adverse event reporting. Users with a history of migraines may experience increased frequency during dose titration. GLP-1 receptor activation affects serotonin pathways involved in migraine pathophysiology. Discuss prophylactic migraine medication with your prescriber if attacks increase.
Are headaches worse on Mounjaro or Ozempic?
SURPASS-2 compared tirzepatide and semaglutide directly. Headache rates were 10.4-13.0% for tirzepatide versus 11.8% for semaglutide 1 mg. The difference was not statistically significant. Per unit of weight lost, headache burden is similar between the two drugs. Switching for headaches alone is unlikely to provide relief.
Can dehydration from tirzepatide cause severe headaches?
Yes. Tirzepatide suppresses thirst alongside appetite. Users report drinking 20-30% less water without awareness. Sustained dehydration over days produces increasingly severe headaches, worsened by standing and physical activity. Drinking 80-100 ounces of water daily with electrolytes prevents dehydration headaches in the majority of users.
Should I stop tirzepatide if I get headaches?
No, not for headaches alone. Over 99% of trial participants continued treatment despite headaches. Try hydration (80-100 oz water with electrolytes), small frequent protein meals, and OTC pain relief first. If headaches persist beyond 8 weeks at a stable dose or are accompanied by neurological symptoms, contact your prescriber.
Does the 2.5 mg starting dose cause headaches?
The 2.5 mg starting dose has the lowest headache rate of any active dose, though exact rates were not separately reported in all trials since 2.5 mg is a 4-week initiation dose only. Headaches at 2.5 mg are typically mild and related to reduced food and fluid intake rather than strong receptor activation.
What is the best painkiller for tirzepatide headaches?
Ibuprofen (200-400 mg with food) is preferred because it addresses both pain and the mild inflammation component. Acetaminophen (500-1000 mg) is an alternative with less GI risk. Avoid using either for more than 10 consecutive days. If headaches require daily medication beyond 2 weeks, see your prescriber for preventive strategies.
The Bottom Line
Tirzepatide causes headaches in 9-18% of users depending on dose and population. Four mechanisms overlap: dehydration from suppressed thirst, blood sugar shifts, central GLP-1 receptor activation, and caloric restriction effects including inadvertent caffeine reduction. Most headaches are mild, cluster during the first 4-8 weeks and after dose increases, and resolve with straightforward interventions.
Drink 80-100 ounces of water daily with electrolytes. Eat small protein-rich meals every 3-4 hours. Maintain your caffeine intake deliberately. Take ibuprofen or acetaminophen as needed, but not daily beyond 2 weeks. Request slower titration if headaches impair daily function at each dose step.
Red flags that demand emergency evaluation: thunderclap onset (peak within 60 seconds), blood pressure above 180/120 mmHg, vomiting exceeding 24 hours, vision changes, or fever with neck stiffness. These are rare but critical to recognize.
Use our tirzepatide dosage calculator to plan your titration schedule. For dosing details, see our tirzepatide dosage chart in units. For switching considerations, see the semaglutide to tirzepatide switching guide.
Related tirzepatide articles: - How Long Does Tirzepatide Take to Work? — week-by-week timeline showing when headaches typically resolve - Tirzepatide Maintenance Dose After Weight Loss — step-down protocols that reduce side effect burden - Does Tirzepatide Cause Diarrhea? — another common GI side effect with overlapping management strategies - Can You Drink Alcohol on Tirzepatide? — alcohol worsens dehydration headaches on GLP-1 agonists - Does Tirzepatide Burn Fat? — understanding the weight loss mechanism behind the side effects - How to Reconstitute Tirzepatide — proper preparation for research peptide users - How to Inject Tirzepatide — injection technique that minimizes side effects - Tirzepatide Injection Site Reaction — managing injection-related discomfort
Explore all peptide profiles and tools at PeptidesExplorer.
Related Articles
Does Tirzepatide Cause Insomnia?
Does tirzepatide cause insomnia? Trials say no, but 5 indirect pathways explain lost sleep. GI, blood sugar, and caloric deficit fixes.
Can Tirzepatide Cause Joint Pain? Clinical Data
Can tirzepatide cause joint pain? SURMOUNT arthralgia rates match placebo. Review 5 indirect causes, uric acid risks, and 8 relief tactics.
Can Tirzepatide Cause Anxiety?
Anxiety is reported in 3-6% of tirzepatide users. Learn SURMOUNT/SURPASS data, GLP-1 brain mechanisms, and 7 management strategies.
Tirzepatide Injection Site Reactions
Injection site reactions affect 3-7% of tirzepatide users. SURMOUNT trial rates, 5 reaction types, severity guide, and 9 prevention strategies.