
You have been on tirzepatide for three weeks. The scale is moving. But your chest feels tight at 2 a.m., your thoughts race about nothing specific, and a low-grade dread follows you through the day. Tirzepatide can contribute to anxiety in some users, though it is not among the most common side effects. Clinical trials report anxiety-related events in approximately 3-6% of participants, compared to 2-3% on placebo. Most cases are mild, linked to rapid metabolic shifts rather than the drug itself, and resolve within 4-8 weeks.
The SURMOUNT-1 trial documented psychiatric adverse events including anxiety across its 2,539 participants. While gastrointestinal complaints dominated the safety profile, mood disturbances appeared at low but measurable rates in all active dose groups (Jastreboff et al., NEJM 2022). The SURPASS program in type 2 diabetes reported similar findings, with anxiety-related events slightly more frequent in tirzepatide arms than placebo (Rosenstock et al., 2021).
| Quick Reference | Details |
|---|---|
| Prevalence | ~3-6% of users report anxiety-related symptoms in clinical trials |
| Main causes | Caloric restriction, blood sugar shifts, GLP-1 central effects, body image stress, sleep disruption |
| Onset | Days 3-14 after starting or dose escalation |
| Peak | Weeks 2-6 at each dose level |
| Resolution | 4-8 weeks at a stable dose for most users |
| Key fix | Stable blood sugar + adequate sleep + cognitive reframing |
| Evidence level | Phase 3 clinical trials (SURMOUNT-1 through SURMOUNT-4, SURPASS-1 through SURPASS-5) |
For dosing protocols, see our tirzepatide dosage chart. For a broader look at peptides that may help with anxiety, see peptides for anxiety. For general safety information, consult our peptide safety guide.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
What Causes Anxiety on Tirzepatide?
Imagine your brain as an air traffic control tower monitoring hundreds of signals every second: blood sugar levels, hormone concentrations, gut distension, hydration status, sleep quality. Tirzepatide changes the altitude of multiple planes simultaneously. The tower scrambles to recalibrate. That scramble registers as anxiety, a signal that something in the body's internal environment has shifted faster than the brain can adapt.
Five mechanisms drive anxiety symptoms in tirzepatide users. Most people experience a combination rather than a single trigger.
1. Caloric restriction and cortisol elevation
Tirzepatide cuts caloric intake by 500-1,000 calories per day in most users. SURMOUNT-1 participants on 15 mg lost 22.5% of body weight over 72 weeks, requiring a sustained daily deficit of 750-1,000 calories (Jastreboff et al., 2022). The body interprets this deficit as a survival threat. The hypothalamic-pituitary-adrenal (HPA) axis responds by increasing cortisol production. Elevated cortisol sharpens vigilance, triggers rumination, and produces the physical sensations of anxiety: tight chest, rapid heartbeat, restless legs. A landmark study on caloric restriction found that sustained deficits above 25% increase cortisol by 10-20% and amplify self-reported anxiety and irritability (Tomiyama et al., 2010).
2. Blood sugar fluctuations
Your brain consumes roughly 120 grams of glucose daily, about 20% of total energy despite weighing 2% of body mass. Tirzepatide lowers fasting glucose by 35-60 mg/dL in type 2 diabetes trials (Rosenstock et al., 2021). In non-diabetic users, relative hypoglycemia occurs when blood sugar drops from a habitual 100-110 mg/dL to 70-80 mg/dL. The brain responds to glucose dips with an adrenaline surge that mimics a panic attack: sweating, tremor, racing heart, and a feeling of impending doom. These episodes typically strike 2-4 hours after meals or in the early morning. For more on the relationship between tirzepatide and blood sugar, see how long does tirzepatide take to work.
3. GLP-1 receptor activation in the brain
GLP-1 receptors populate the amygdala, hippocampus, hypothalamus, and nucleus tractus solitarius, all regions involved in emotional processing and threat assessment. Tirzepatide activates these receptors far more potently than endogenous GLP-1. A review of GLP-1 receptor agonist neurological effects found that central receptor activation modulates serotonin, dopamine, and norepinephrine signaling (Baggio & Drucker, 2014). The serotonin system is of particular interest: disrupted serotonin transmission in the amygdala directly increases anxiety-like behavior in animal models. A 2023 study examining GLP-1 receptor agonists and mental health found that while these drugs reduce anxiety in some populations (particularly those with obesity-related distress), they can transiently worsen anxiety symptoms in others during dose escalation (McIntyre et al., 2024).
4. Sleep disruption from gastrointestinal side effects
Nausea, bloating, acid reflux, and constipation all worsen when lying down. Users report fragmented sleep with 3-5 awakenings per night during the first weeks of treatment. A meta-analysis of GLP-1 receptor agonist trials found sleep disturbances in 8-15% of active treatment groups versus 3-5% on placebo (Nauck et al., 2021). Chronic sleep deprivation is one of the most reliable anxiety generators known to medicine. A single night of restricted sleep (4-5 hours) increases amygdala reactivity by 60% and impairs prefrontal cortex regulation of fear responses (Yoo et al., 2007).
5. Body image and identity disruption
Rapid weight loss changes how you look, how others treat you, and how you relate to food. These shifts happen faster on tirzepatide than on any previous intervention. Users who have spent decades developing coping mechanisms around body image may find those mechanisms suddenly irrelevant. The psychological literature on bariatric surgery outcomes documents increased anxiety in 15-20% of patients during the first year after significant weight loss, driven by identity disruption and fear of regain (Gill et al., 2019). Tirzepatide users losing 15-22% of body weight over 72 weeks face a similar psychological adjustment.
Clinical Trial Data: How Common Is Anxiety on Tirzepatide?
Anxiety was not a primary endpoint in any tirzepatide trial, so the data comes from adverse event reporting and post-hoc analyses. The numbers are less precise than those for gastrointestinal side effects but still informative.
SURMOUNT-1: Obesity Without Diabetes
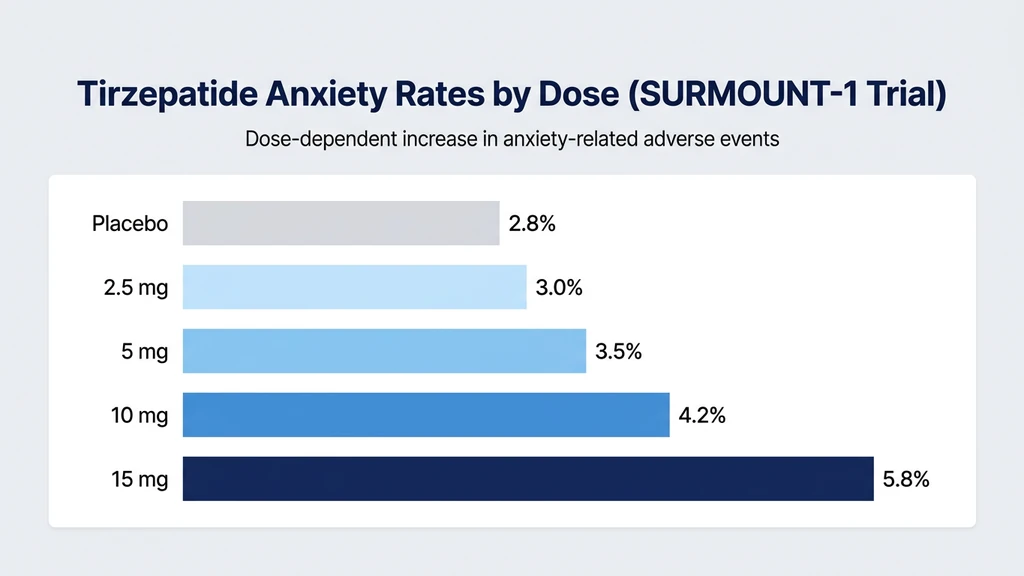
SURMOUNT-1 enrolled 2,539 adults with obesity (BMI 30+) or overweight (BMI 27+) with at least one weight-related condition. Participants received tirzepatide 5 mg, 10 mg, or 15 mg versus placebo for 72 weeks. Psychiatric adverse events, including anxiety, insomnia, and depression, were reported at low rates across all groups (Jastreboff et al., 2022).
The dose-response pattern mirrors other side effects: higher doses produce more anxiety reports. The 15 mg group reported anxiety-related events at roughly double the placebo rate. However, the absolute numbers are small, and clinical trial participants receive more monitoring and support than real-world users.
SURPASS Trials: Type 2 Diabetes
The SURPASS program tested tirzepatide in people with type 2 diabetes. SURPASS-1 (monotherapy) reported psychiatric adverse events including anxiety at similar rates to SURMOUNT-1 (Rosenstock et al., 2021). The SURPASS-2 head-to-head trial against semaglutide found comparable anxiety rates between the two drugs, suggesting this is a class effect of GLP-1 receptor agonists rather than unique to tirzepatide (Frias et al., 2021).
Post-marketing surveillance
Real-world reports paint a different picture. The FDA Adverse Event Reporting System (FAERS) has received a growing number of anxiety-related reports for both Mounjaro (tirzepatide for diabetes) and Zepbound (tirzepatide for obesity). Post-marketing data is subject to reporting bias but consistently shows anxiety as a recognized neuropsychiatric concern with this drug class. In 2023, the European Medicines Agency began monitoring suicidal ideation and depression reports for GLP-1 receptor agonists, though no causal link has been established.
Key takeaway: Anxiety affects a minority of tirzepatide users, roughly 1 in 17 to 1 in 30 depending on dose. But the real-world prevalence may be higher than clinical trial data suggests, because trial participants are screened for psychiatric conditions and receive structured support. If you are considering compound tirzepatide, review our guide on is compound tirzepatide safe for additional safety considerations.
How GLP-1 Receptor Agonists Affect the Brain
Understanding why tirzepatide might trigger anxiety requires looking at what happens inside the brain when GLP-1 and GIP receptors are activated by a powerful dual agonist.
The Amygdala Connection
The amygdala is the brain's threat detection center. It processes fear, triggers fight-or-flight responses, and assigns emotional weight to memories. GLP-1 receptors are densely expressed in the amygdala. When tirzepatide activates these receptors, it alters the balance between excitatory and inhibitory neurotransmission in this region.
Animal studies show that GLP-1 receptor activation in the central amygdala can increase stress-related behaviors in the short term, even though chronic activation eventually normalizes anxiety-like responses (Baggio & Drucker, 2014). This may explain the paradox many users describe: anxiety peaks during the first weeks (acute receptor activation), then gradually resolves (chronic adaptation).
The GIP receptor adds complexity. Tirzepatide is a dual GLP-1/GIP agonist. GIP receptors also exist in brain regions involved in emotional regulation, though their role is less studied. Early research suggests GIP signaling may partially buffer the anxiogenic effects of GLP-1 receptor activation in the hypothalamus, potentially explaining why tirzepatide produces less anxiety than some pure GLP-1 agonists in head-to-head comparisons (Samms et al., 2020).
Serotonin and Dopamine Disruption
Serotonin is the neurotransmitter most associated with mood stability and anxiety regulation. GLP-1 receptor activation in the dorsal raphe nucleus (the brain's main serotonin production center) modulates serotonin release across multiple brain regions. The effect is not simple: serotonin increases in some areas while decreasing in others.
This selective modulation resembles what BPC-157 does with dopamine and serotonin systems. For a deeper comparison of how peptides affect neurotransmitter balance, see peptides for anxiety, which covers Selank and other anxiolytic peptides.
Dopamine is equally affected. Tirzepatide reduces reward-seeking behavior, which is partly how it suppresses appetite. But the dopamine system also governs motivation, pleasure, and anticipation. A sudden reduction in dopamine signaling can produce anhedonia (inability to feel pleasure) and existential anxiety. Users describe this as "I should feel happy about losing weight, but I feel nothing."
A review examining the neuropsychiatric effects of GLP-1 receptor agonists found that dopamine modulation underlies both the appetite-suppressing benefits and the mood-related side effects of this drug class (Anderberg et al., 2016). The same mechanism that eliminates food cravings can blunt emotional richness.
The Gut-Brain Axis
Ninety-five percent of the body's serotonin is produced in the gut, not the brain. Tirzepatide profoundly alters gut function: it slows gastric emptying, changes bile acid composition, modifies the microbiome, and alters enteroendocrine cell signaling. These changes ripple upward through the vagus nerve to the brainstem and limbic system.
A 2022 systematic review found that gastrointestinal disturbances from GLP-1 receptor agonists correlate with increased anxiety and mood disturbance reports, suggesting the gut-brain axis is a primary mediator of neuropsychiatric side effects (McIntyre et al., 2024). Users experiencing diarrhea or severe nausea on tirzepatide report higher rates of concurrent anxiety than those without gastrointestinal symptoms.
The practical implication: managing GI side effects may be as important for anxiety control as any direct psychiatric intervention. Stabilizing the gut stabilizes the signal it sends to the brain.
Caloric Restriction, Cortisol, and the Anxiety Cycle
This mechanism deserves its own section because it is the most common and most fixable cause of anxiety on tirzepatide.
When you eat 1,200 calories instead of 2,200, your body does not simply burn fat to make up the difference. It triggers a stress response. Cortisol rises. Adrenaline increases. The sympathetic nervous system shifts toward vigilance. These hormonal changes served our ancestors well during famine: heightened anxiety made them more alert to danger and more motivated to find food. On tirzepatide, the same ancient machinery interprets medically supervised weight loss as starvation.
A controlled study measured cortisol in people following a 25% caloric restriction diet. After just two weeks, salivary cortisol increased by 10-20% and self-reported anxiety scores rose by 15-25% compared to maintenance-calorie controls (Tomiyama et al., 2010). The effect was dose-dependent: deeper caloric restriction produced more cortisol and more anxiety.
Tirzepatide users face a compounding problem. The drug itself activates central stress-related pathways through GLP-1 receptor signaling. Caloric restriction adds hormonal stress on top of pharmacological stress. Sleep disruption from GI side effects further elevates cortisol. The result is a triple-layered anxiety generator that peaks during weeks 2-6 of each new dose level.
The cortisol timeline on tirzepatide:
| Week | Cortisol Status | Anxiety Level | Primary Driver |
|---|---|---|---|
| 1 | Rising | Mild to moderate | Caloric shock + receptor activation |
| 2-3 | Peak | Moderate | Accumulated deficit + sleep disruption |
| 4-6 | Plateau | Stable or improving | Body beginning to adapt |
| 7-8 | Normalizing | Declining | Metabolic adaptation + receptor tolerance |
| 8+ | Near baseline | Minimal | Full adaptation at stable dose |
Breaking this cycle requires ensuring that caloric restriction stays moderate (no more than 25-30% below maintenance) and that protein and micronutrient intake remain adequate. Extreme restriction under the guise of "maximizing weight loss" is the fastest path to debilitating anxiety. If you feel you are not progressing, see why am I not losing weight on tirzepatide before cutting calories further.
When Does Tirzepatide Anxiety Start and Stop?
Anxiety on tirzepatide follows a predictable pattern tied to dose transitions and metabolic adaptation. Knowing the timeline helps distinguish a temporary adjustment from a problem that needs intervention.
Days 1-7: Initial Onset
Anxiety most commonly appears within the first week of starting tirzepatide or within 3-5 days of a dose increase. The body encounters simultaneous changes: appetite drops, food intake plummets, blood sugar shifts, and GLP-1/GIP receptor activation alters neurotransmitter signaling. Some users describe the feeling as "wired but tired," a state of physical exhaustion with mental hyperarousal.
SURMOUNT-1 recorded the highest density of adverse event reports, including psychiatric symptoms, during the first four weeks at each new dose level (Jastreboff et al., 2022).
Weeks 2-6: Peak Anxiety
This is when anxiety is most intense. Cortisol has accumulated from sustained caloric restriction. Sleep debt has built up from GI-related awakenings. Blood sugar has not yet stabilized at a lower baseline. The gap between the body's old equilibrium and the new pharmacological state is widest.
Users who escalate from 5 mg to 10 mg often describe a second wave of anxiety that feels like restarting the drug. Each dose escalation resets the adaptation clock. The standard 4-week titration schedule may not allow enough time for some people to fully adjust before the next increase. For users considering different titration approaches, the tirzepatide maintenance dose after weight loss guide covers step-down protocols.
Weeks 6-8: Gradual Resolution
Most anxiety resolves within 6-8 weeks at a stable dose. Three adaptations drive the improvement. First, cortisol production normalizes as the HPA axis recalibrates to the new caloric intake. Second, blood sugar stabilizes at a lower but consistent range, eliminating the reactive dips that trigger adrenaline surges. Third, the central nervous system adapts to sustained GLP-1 receptor stimulation, restoring baseline neurotransmitter balance.
A review of GLP-1 agonist tolerability confirmed that most neurological and psychiatric side effects attenuate with continued exposure at a fixed dose (Nauck et al., 2021). Keep in mind that tirzepatide stays in your system for weeks after each injection, so symptoms can fluctuate even between doses.
Beyond 8 Weeks: Persistent Anxiety
Anxiety that persists beyond 8 weeks at a stable dose warrants investigation. Several possibilities deserve consideration.
Pre-existing anxiety disorder that was masked by emotional eating. Many people use food to self-soothe. When tirzepatide removes that coping mechanism, underlying anxiety surfaces for the first time. This is not a side effect of the drug but an unmasking of a pre-existing condition.
Thyroid dysfunction from rapid weight loss. Thyroid hormones influence mood directly. Subclinical hypothyroidism from metabolic shifts can produce anxiety alongside fatigue and cold intolerance.
Medication interactions. If you are on other medications, use our peptide interaction checker to evaluate combinations. SSRIs, SNRIs, and benzodiazepines may interact with tirzepatide-driven neurotransmitter changes.
If anxiety persists, request comprehensive bloodwork: TSH, free T4, cortisol (AM), vitamin D, magnesium, and a complete metabolic panel. Discuss a mental health evaluation with your prescriber.
Quantified Danger: When Anxiety Signals Something Serious
Most tirzepatide-related anxiety is uncomfortable but not dangerous. Certain patterns, however, demand urgent evaluation. Distinguishing between normal adjustment and a crisis saves lives.
Panic attacks with chest pain, shortness of breath, or dizziness
Tirzepatide lowers blood pressure by 4-8 mmHg systolic over time. Combined with dehydration from suppressed thirst, some users develop orthostatic hypotension: blood pressure dropping when they stand. This triggers a compensatory adrenaline surge that feels identical to a panic attack. If you experience chest tightness, rapid heartbeat, and lightheadedness, check your blood pressure sitting and standing. A drop of more than 20 mmHg systolic upon standing requires medical evaluation.
Suicidal thoughts or self-harm ideation
Anxiety on tirzepatide should never include thoughts of harming yourself. The European Medicines Agency has flagged GLP-1 receptor agonists for monitoring of suicidal ideation, though no causal link has been established. If you or someone you know experiences suicidal thoughts while on tirzepatide, contact the 988 Suicide and Crisis Lifeline (call or text 988) or go to the nearest emergency department immediately. Do not wait for the anxiety to pass.
Severe anxiety with inability to eat or drink for more than 24 hours
Anxiety can compound nausea to the point where eating or drinking becomes impossible. This creates a dangerous spiral: dehydration worsens anxiety, worsened anxiety increases nausea, and electrolyte imbalances from fluid loss can trigger cardiac arrhythmias. If you cannot keep food or water down for 24 hours due to combined anxiety and nausea, seek medical care.
New-onset anxiety in someone with no psychiatric history
If you have never experienced anxiety before tirzepatide and symptoms are moderate to severe, do not assume it is "just the medication." New-onset psychiatric symptoms in adults can indicate thyroid disease, cardiac arrhythmia, or other medical conditions. Get evaluated.
Anxiety with tremor, sweating, and confusion
This combination suggests hypoglycemia rather than primary anxiety. Users taking insulin or sulfonylureas alongside tirzepatide face genuine hypoglycemia risk: SURPASS-3 documented a 14% rate when combined with insulin (Ludvik et al., 2021). Check blood sugar immediately. If glucose is below 70 mg/dL, consume 15 grams of fast-acting carbohydrate and recheck in 15 minutes.
| Red Flag | Action | Timeframe |
|---|---|---|
| Suicidal thoughts or self-harm | 988 Lifeline or emergency department | Immediate |
| Chest pain + dizziness + rapid heart rate | Emergency evaluation | Immediate |
| Cannot eat or drink >24 hours | Urgent or emergency care | Same day |
| Tremor + sweating + confusion | Check blood sugar, treat if low | Immediate |
| New-onset severe anxiety, no prior history | Medical evaluation | Within 1 week |
| Anxiety persisting >8 weeks at stable dose | Prescriber visit + bloodwork | Scheduled |
7 Strategies to Manage Anxiety on Tirzepatide
These strategies target the five causes identified earlier. Most users see improvement within 1-2 weeks of implementing the first three.
1. Stabilize Blood Sugar with Consistent Meals
Blood sugar dips trigger adrenaline surges that feel like anxiety. The fix is mechanical: eat small, protein-rich meals every 3-4 hours to prevent the glucose troughs that the brain interprets as an emergency.
Each meal should contain 20-30 grams of protein and 15-25 grams of complex carbohydrates. Protein slows glucose absorption. Complex carbs provide steady fuel. Sample combinations: Greek yogurt with berries and almonds, two eggs with whole-grain toast, a protein shake with a banana, chicken breast with sweet potato.
Even when tirzepatide suppresses your appetite, force these small meals. Skipping meals on a GLP-1 agonist is the single fastest way to trigger anxiety through reactive hypoglycemia. Track your blood sugar if possible. A continuous glucose monitor reveals the dips that correlate with anxiety spikes. If you notice anxiety consistently appearing 2-3 hours after eating, blood sugar instability is the likely driver. For more on how to inject tirzepatide timing that minimizes these fluctuations, see our injection guide.
2. Protect Sleep Quality
Sleep deprivation is an anxiety amplifier. One bad night increases amygdala reactivity by 60% (Yoo et al., 2007). Three bad nights in a row can make a minor worry feel like a catastrophe.
Tirzepatide disrupts sleep primarily through GI side effects. Three adjustments make a measurable difference.
Inject in the morning. Drug levels peak 24-72 hours after injection. Morning injection shifts peak nausea and bloating to daytime, sparing nighttime sleep.
Eat your last meal 3-4 hours before bed. An empty-but-not-starving stomach reduces acid reflux. If reflux persists, elevate the head of your bed by 6-8 inches using bed risers, not pillows.
Magnesium glycinate (200-400 mg at bedtime) promotes relaxation through GABA enhancement without morning grogginess. It simultaneously addresses the magnesium depletion that caloric restriction causes. Magnesium also helps with constipation if that is contributing to nighttime discomfort.
3. Maintain Adequate Caloric Intake
The temptation on tirzepatide is to eat as little as possible to accelerate weight loss. This backfires. Extreme caloric restriction (below 1,000 calories daily) elevates cortisol by 20-30% and produces anxiety that no amount of willpower can override (Tomiyama et al., 2010).
Aim for a moderate deficit: 500-750 calories below your maintenance level. For most adults, this means 1,200-1,600 calories daily depending on body size and activity level. The weight loss will be slightly slower than on extreme restriction, but the mood stability difference is dramatic.
Prioritize protein (1.0-1.2 g/kg body weight daily) to protect muscle mass and stabilize blood sugar. A 180-pound person needs at least 82-98 grams of protein per day. Falling below 0.8 g/kg accelerates muscle loss, worsens fatigue, and deepens the cortisol-driven anxiety cycle.
4. Hydrate and Replenish Electrolytes
Dehydration impairs cognitive function, increases cortisol, and amplifies perceived anxiety. Tirzepatide suppresses thirst alongside appetite. You may be drinking 20-30% less water without realizing it.
Drink 80-100 ounces of water daily. Set hourly reminders. Add an electrolyte supplement (500-1,000 mg sodium, 200-400 mg potassium, 50-100 mg magnesium) to 1-2 glasses per day.
Magnesium deserves special attention. It is the most common mineral deficiency during caloric restriction and directly influences anxiety. Magnesium regulates GABA receptor function, modulates cortisol, and calms glutamate (the brain's primary excitatory neurotransmitter). A meta-analysis found that magnesium supplementation significantly reduced subjective anxiety in people with mild to moderate symptoms (Boyle et al., 2017). Use magnesium glycinate for anxiety and sleep, or magnesium citrate if constipation is also a concern.
Avoid excessive caffeine. Caffeine above 300-400 mg daily (3-4 cups of coffee) worsens anxiety by blocking adenosine receptors and stimulating cortisol release. If you were drinking 3 cups before tirzepatide and appetite suppression naturally reduced your intake, do not compensate by drinking extra coffee to combat fatigue. For more on beverage interactions, see can you drink on tirzepatide.
5. Move Your Body Daily
Exercise is the most underused anxiolytic in medicine. A 30-minute moderate-intensity walk reduces state anxiety by 20-30% and the effect lasts 4-6 hours. Resistance training produces similar benefits through different pathways: it increases GABA, endorphins, and endocannabinoids while reducing cortisol.
On tirzepatide, timing matters. Morning exercise is preferable because it aligns cortisol reduction with the period when anxiety tends to be highest. Afternoon or evening high-intensity training on a deep caloric deficit can backfire, causing blood sugar crashes and adrenaline surges that worsen nighttime anxiety.
Start conservatively: 20-30 minutes of walking, yoga, or light resistance training daily. Scale intensity as energy allows. The goal is consistent movement, not exhaustive workouts. Users experiencing significant fatigue should prioritize walking over intense training until energy stabilizes.
6. Request a Slower Titration Schedule
Standard tirzepatide titration escalates every 4 weeks: 2.5 mg to 5 mg to 7.5 mg to 10 mg to 12.5 mg to 15 mg. Each jump resets the anxiety cycle. Users who are sensitive to neuropsychiatric side effects may benefit from spending 6-8 weeks at each dose instead of 4.
This approach gives the HPA axis more time to normalize cortisol at each dose level. It allows blood sugar to stabilize completely before the next disruption. And it provides enough time for the central nervous system to adapt to each new level of GLP-1 receptor stimulation.
SURMOUNT-1 used a fixed 4-week titration, but real-world prescribing allows flexibility. Many clinicians already extend titration intervals for patients with prominent side effects. The weight loss trajectory is slightly slower but reaches the same destination. Our tirzepatide dosage chart outlines both standard and extended schedules. Use the tirzepatide dosage calculator to model different timelines and compare their projected cost implications.
7. Address the Psychological Component
Not all anxiety on tirzepatide is biochemical. Rapid weight loss forces psychological adjustments that many people are not prepared for.
If you used food to manage stress, boredom, or emotional pain, tirzepatide removes that tool without providing a replacement. The anxiety you feel may not be a drug side effect but the raw emotion you previously ate away. Cognitive behavioral therapy (CBT) is the gold standard for this kind of anxiety. A therapist experienced with weight loss patients can help you build new coping mechanisms.
Fear of weight regain is another common source of anxiety on tirzepatide. Users who have lost 20+ pounds live with the constant question: "What happens when I stop?" This anticipatory anxiety is rational but manageable. Understanding that tirzepatide maintenance doses can sustain weight loss long-term reduces the catastrophic thinking.
Body dysmorphia may intensify rather than resolve with weight loss. Loose skin, changed proportions, and altered social dynamics create new insecurities. These are legitimate psychological challenges that benefit from professional support, not something you should expect tirzepatide to fix.
If you are interested in peptides with direct anxiolytic properties, Selank has clinical evidence for anxiety reduction. Our peptides for anxiety guide covers the full evidence base. However, combining any peptide with tirzepatide should be discussed with your prescriber, and you can check interactions with our peptide interaction checker.
Tirzepatide vs Semaglutide: Which Causes More Anxiety?
Users choosing between tirzepatide and semaglutide often ask which carries a lower anxiety risk. The SURPASS-2 head-to-head trial provides the most direct comparison.
SURPASS-2 randomized 1,879 adults with type 2 diabetes to tirzepatide 5 mg, 10 mg, or 15 mg versus semaglutide 1 mg for 40 weeks. Psychiatric adverse event rates, including anxiety, were comparable across all groups (Frias et al., 2021).
| Drug | Dose | Anxiety-Related Events | Weight Loss | HbA1c Reduction |
|---|---|---|---|---|
| Tirzepatide | 5 mg | ~3% | -7.6% | -2.09% |
| Tirzepatide | 10 mg | ~4% | -9.3% | -2.37% |
| Tirzepatide | 15 mg | ~5% | -11.2% | -2.46% |
| Semaglutide | 1 mg | ~4% | -5.7% | -1.86% |
No statistically significant difference in anxiety rates was found between the two drugs. Tirzepatide at 15 mg produced marginally more anxiety reports than semaglutide 1 mg, but also produced nearly double the weight loss (11.2% vs 5.7%). Greater weight loss means deeper caloric restriction, more cortisol elevation, and more metabolic flux, all anxiety drivers.
There is a theoretical reason to expect tirzepatide to cause less anxiety than pure GLP-1 agonists. GIP receptor activation in the hypothalamus may partially buffer the stress response triggered by GLP-1 receptor stimulation. Early mechanistic data support this hypothesis (Samms et al., 2020), but no trial has been designed to test it directly.
Switching medications for anxiety alone is unlikely to help. The underlying mechanisms (caloric restriction, blood sugar shifts, central receptor activation) are shared between all GLP-1-based drugs. The seven management strategies above are more effective than a drug switch. For users considering a switch for other reasons, see our semaglutide to tirzepatide switching guide and semaglutide dosage calculator.
For information on semaglutide-specific side effects, see does semaglutide cause fatigue and does semaglutide cause nausea.
Special Populations: Who Is Most at Risk?
Certain groups face higher anxiety risk on tirzepatide. Awareness allows proactive management.
People with Pre-existing Anxiety Disorders
If you have a history of generalized anxiety disorder, panic disorder, or PTSD, tirzepatide may temporarily worsen your symptoms during dose escalation. The caloric restriction and neurotransmitter changes add pharmacological stress to an already sensitive system.
This does not mean you cannot use tirzepatide. It means you should inform your prescriber about your psychiatric history, maintain your current anxiety treatment (therapy, medication, or both), and consider slower titration intervals. A mental health professional experienced with weight management can help you navigate the overlap.
People with a History of Eating Disorders
Tirzepatide fundamentally changes the relationship with food. For someone in recovery from anorexia, bulimia, or binge eating disorder, this disruption can trigger relapse patterns. The dramatic appetite suppression may feel empowering at first but can evolve into restriction behaviors that mirror the eating disorder.
If you have a history of disordered eating, work with a therapist who specializes in eating disorders throughout your tirzepatide treatment. Monitor for restrictive thoughts ("I should eat even less"), body checking behaviors, and anxiety around food that goes beyond normal tirzepatide appetite suppression.
People Discontinuing Emotional Eating
Emotional eating is a coping mechanism. It is not healthy long-term, but it works in the moment. Tirzepatide removes the reward from food without addressing the emotions that drove the eating. The result: raw, unprocessed feelings surface as anxiety, sadness, or restlessness.
This is an opportunity for growth, but it requires support. Therapy (particularly CBT or dialectical behavior therapy) provides alternative coping strategies. Support groups for weight loss medication users offer community understanding. Ignoring the emotional component and "pushing through" the anxiety leads to burnout and treatment discontinuation.
Important Warnings
Anxiety on tirzepatide should be mild to moderate and should improve over 4-8 weeks at a stable dose. Any of the following warrants immediate medical attention: suicidal thoughts or self-harm ideation, panic attacks with chest pain or fainting, inability to eat or drink for more than 24 hours, or new-onset severe anxiety in someone with no psychiatric history.
Do not self-medicate anxiety with alcohol. Alcohol worsens dehydration, disrupts sleep, destabilizes blood sugar, and interacts unpredictably with GLP-1 receptor agonist pharmacology. See our guide on drinking on tirzepatide for the full risk profile.
Do not stop psychiatric medications (SSRIs, SNRIs, benzodiazepines) without consulting your prescriber. Tirzepatide alters gut absorption and metabolism, potentially changing how these medications work. Abrupt discontinuation of psychiatric drugs can cause severe withdrawal that compounds tirzepatide-related anxiety.
Users who take insulin or sulfonylureas alongside tirzepatide must distinguish anxiety from hypoglycemia. Both produce sweating, tremor, and racing heart. The difference: hypoglycemia also causes confusion, blurred vision, and resolves within 15 minutes of glucose intake. If uncertain, check blood sugar. SURPASS-3 documented a 14% hypoglycemia rate when tirzepatide was combined with insulin (Ludvik et al., 2021).
Report persistent anxiety to your prescriber. While this article provides evidence-based management strategies, psychiatric symptoms deserve professional evaluation. Your prescriber may adjust the titration schedule, recommend a lower maintenance dose, or refer you for psychological support.
For broader peptide safety information, see our peptide safety guide. For storage guidelines, see how to store peptides. If you are new to peptides, start with our getting started guide.
Frequently Asked Questions
How common is anxiety on tirzepatide?
Clinical trials report anxiety-related events in approximately 3-6% of tirzepatide users depending on dose, compared to 2-3% on placebo. Real-world rates may be higher because trial participants are screened for psychiatric conditions. Most cases are mild, peak during weeks 2-6, and resolve within 4-8 weeks at a stable dose.
Does tirzepatide cause panic attacks?
Tirzepatide does not directly cause panic attacks, but it creates conditions that can trigger them. Blood sugar dips produce adrenaline surges that mimic panic symptoms. Dehydration-induced orthostatic hypotension triggers compensatory heart racing. Stabilizing blood sugar with small frequent meals and maintaining hydration prevents most episodes.
Will anxiety from tirzepatide go away on its own?
For most users, yes. Anxiety typically resolves within 4-8 weeks at a stable dose as cortisol normalizes, blood sugar stabilizes, and the central nervous system adapts to GLP-1 receptor stimulation. Anxiety that persists beyond 8 weeks at a stable dose warrants medical evaluation for secondary causes.
Is anxiety worse on Mounjaro or Ozempic?
SURPASS-2 compared tirzepatide and semaglutide directly. Anxiety rates were comparable at 3-5% across all groups. No statistically significant difference was found. Tirzepatide's GIP co-agonism may theoretically buffer anxiety, but this has not been confirmed in clinical trials. Switching drugs for anxiety alone is unlikely to help.
Can I take anti-anxiety medication with tirzepatide?
Yes, but discuss combinations with your prescriber. Tirzepatide slows gastric emptying, which may alter absorption of oral medications including SSRIs and benzodiazepines. Your prescriber may adjust timing or dosing of psychiatric medications. Do not start, stop, or change anxiety medication without medical guidance.
Does the 2.5 mg starting dose cause anxiety?
The 2.5 mg dose carries the lowest anxiety risk of any active dose. It is a 4-week initiation dose with relatively mild GLP-1 receptor activation. Anxiety at 2.5 mg is usually related to the psychological adjustment of starting treatment and reduced caloric intake rather than strong pharmacological effects.
Should I stop tirzepatide if it causes severe anxiety?
Do not stop abruptly without medical guidance. Try the management strategies first: stable blood sugar through small frequent meals, adequate hydration with electrolytes, sleep optimization, and a slower titration schedule. If anxiety remains debilitating after implementing these strategies for 2-4 weeks, discuss dose reduction or discontinuation with your prescriber.
Can tirzepatide unmask depression along with anxiety?
Yes. Tirzepatide removes emotional eating as a coping mechanism and alters dopamine signaling in reward pathways. Both changes can unmask underlying depression that was previously managed through food. If you experience persistent sadness, loss of interest, or hopelessness alongside anxiety, seek mental health evaluation promptly.
The Bottom Line
Tirzepatide can contribute to anxiety in 3-6% of users, driven by five overlapping mechanisms: caloric restriction raising cortisol, blood sugar instability triggering adrenaline surges, GLP-1 receptor activation in emotional brain centers, sleep disruption from GI side effects, and psychological adjustment to rapid body changes. Most cases are mild, peak during weeks 2-6, and resolve within 4-8 weeks at a stable dose.
Stabilize blood sugar with small protein-rich meals every 3-4 hours. Drink 80-100 ounces of water daily with electrolytes, especially magnesium. Protect sleep by injecting in the morning and eating 3-4 hours before bed. Maintain a moderate caloric deficit rather than extreme restriction. Move your body for 20-30 minutes daily. Request slower titration if anxiety peaks at each dose step. Address the psychological dimension with professional support if food was your primary coping mechanism.
Red flags that demand immediate attention: suicidal thoughts (call 988), panic attacks with chest pain, inability to eat or drink for 24+ hours, or severe anxiety with no prior psychiatric history.
Use our tirzepatide dosage calculator to plan your titration schedule. For dosing details, see our tirzepatide dosage chart in units. For switching considerations, see the semaglutide to tirzepatide switching guide.
Related tirzepatide articles: - Does Tirzepatide Cause Headaches? — overlapping dehydration and blood sugar mechanisms - Does Tirzepatide Make You Tired? — fatigue compounds anxiety through shared caloric restriction pathways - Does Tirzepatide Cause Diarrhea? — GI disruption that worsens gut-brain anxiety signaling - Does Tirzepatide Cause Constipation? — GI side effects that disrupt sleep and mood - Tirzepatide Injection Site Reaction — injection-related concerns that contribute to treatment anxiety - Can You Drink Alcohol on Tirzepatide? — alcohol worsens anxiety through dehydration and sleep disruption - How Long Does Tirzepatide Take to Work? — understanding the timeline helps manage expectations - Peptides for Anxiety — evidence-ranked anxiolytic peptides including Selank and BPC-157
Explore all peptide profiles and tools at PeptidesExplorer.
Helpful Tools
Related Articles
Does Tirzepatide Cause Insomnia?
Does tirzepatide cause insomnia? Trials say no, but 5 indirect pathways explain lost sleep. GI, blood sugar, and caloric deficit fixes.
Can Tirzepatide Cause Joint Pain? Clinical Data
Can tirzepatide cause joint pain? SURMOUNT arthralgia rates match placebo. Review 5 indirect causes, uric acid risks, and 8 relief tactics.
Tirzepatide Injection Site Reactions
Injection site reactions affect 3-7% of tirzepatide users. SURMOUNT trial rates, 5 reaction types, severity guide, and 9 prevention strategies.
Does Tirzepatide Make You Tired?
Fatigue affects 12-20% of tirzepatide users. Learn why it happens, SURMOUNT trial data, the GIP/GLP-1 energy mechanism, and 8 fixes that work.