You have been injecting tirzepatide for 10 weeks. The scale dropped fast at first, then stopped. Your friend on the same dose is still losing steadily. You are wondering whether the drug quit working, whether your body adapted, or whether you drew the short straw genetically. Most people who plateau on tirzepatide have a correctable problem, not a biological dead end. The SURMOUNT-1 trial showed that 97% of participants on tirzepatide 15 mg lost at least 5% of body weight at 72 weeks, leaving only about 3% as true non-responders (Jastreboff et al., 2022). That 3% figure is roughly half the non-responder rate seen with semaglutide. The question is whether you belong to that small group or whether something fixable is standing between you and the results the drug should deliver.
| Quick Reference | Details |
|---|---|
| Expected weight loss | 22.5% of body weight at 72 weeks (SURMOUNT-1, 15 mg) |
| Non-responder rate | ~3% lose less than 5% body weight |
| Common plateau window | Weeks 8-14 |
| Most common fixable cause | Caloric intake still exceeds expenditure |
| BMR reduction with weight loss | 10-15% below predicted |
| Time to maximum effect | 20-28 weeks at maintenance dose (10 or 15 mg) |
| Mechanism advantage | Dual GIP + GLP-1 agonist (vs GLP-1 only for semaglutide) |
| When to reassess | After 16 weeks at maximum tolerated dose |
Use the tirzepatide dosage calculator to verify your current dose is correct for your vial concentration. For a visual dosing reference, see the tirzepatide dosage chart in units.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
The Weight Loss Timeline Most People Get Wrong
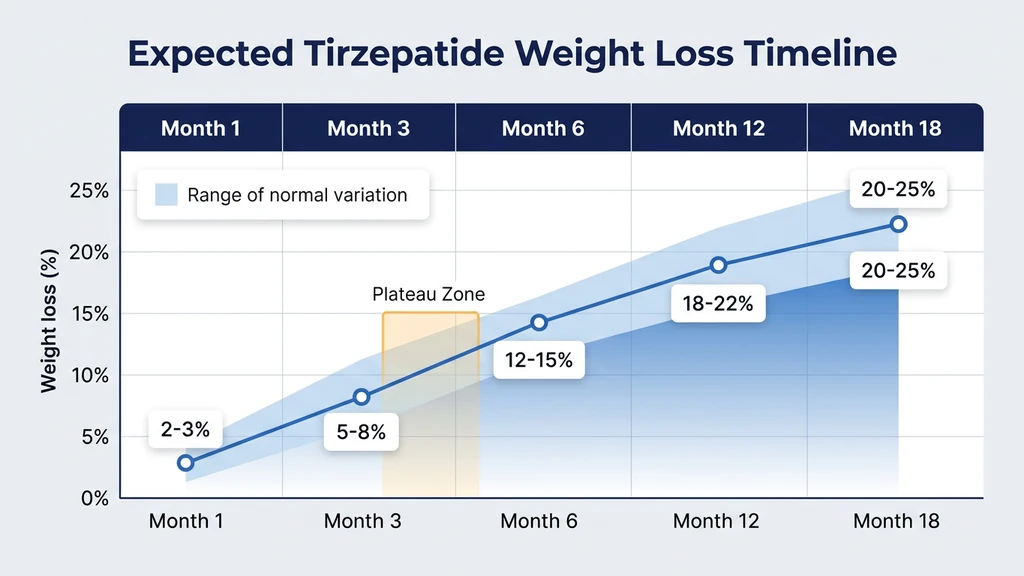
Tirzepatide does not produce linear weight loss. The trajectory looks more like a staircase: drops, pauses, drops again. The titration schedule alone takes 20 weeks to reach the maximum dose of 15 mg. Evaluating the drug at week 6 on a 2.5 mg starting dose is like rating a car's top speed while it is still in first gear.
The SURMOUNT-1 trial tracked weight loss across 72 weeks. Here is the actual trajectory:
| Timepoint | Average Weight Loss | What Is Happening |
|---|---|---|
| Week 4 | 2-3% | Starting dose (2.5 mg); mild appetite reduction |
| Week 8 | 4-6% | Dose at 5 mg; appetite suppression strengthens |
| Week 12 | 7-9% | Dose at 7.5 mg; first plateau is common |
| Week 20 | 12-15% | Reaching 10 mg or 15 mg; major fat loss phase |
| Week 40 | 18-21% | Approaching peak effect |
| Week 72 | 22.5% | Average end-of-trial result (15 mg group) |
The stall between weeks 8 and 14 is nearly universal. Weight drops steadily, then the scale freezes for 2-4 weeks. This pause is a biological recalibration. Your body detects the caloric deficit and adjusts metabolic rate, fluid balance, and hormonal output to resist further loss. The stall breaks when the next dose increase restores a stronger appetite suppression signal.
A second common misunderstanding involves rate versus total. Tirzepatide produces steeper losses in the first 12 weeks and more gradual losses from month 4 onward. Losing 3 pounds per week in month 1 and then 0.7 pounds per week in month 5 is the expected pattern, not a failure signal. The SURMOUNT-3 extension data confirmed that weight loss continues past week 72 for users who remain on the drug (Wadden et al., 2023).
If you are below 10 mg, you have not yet given tirzepatide its full chance. Check the tirzepatide dosage chart to confirm your position on the titration ladder. If you are converting from semaglutide, see the semaglutide to tirzepatide switching guide.
8 Reasons Tirzepatide Is Not Working for You
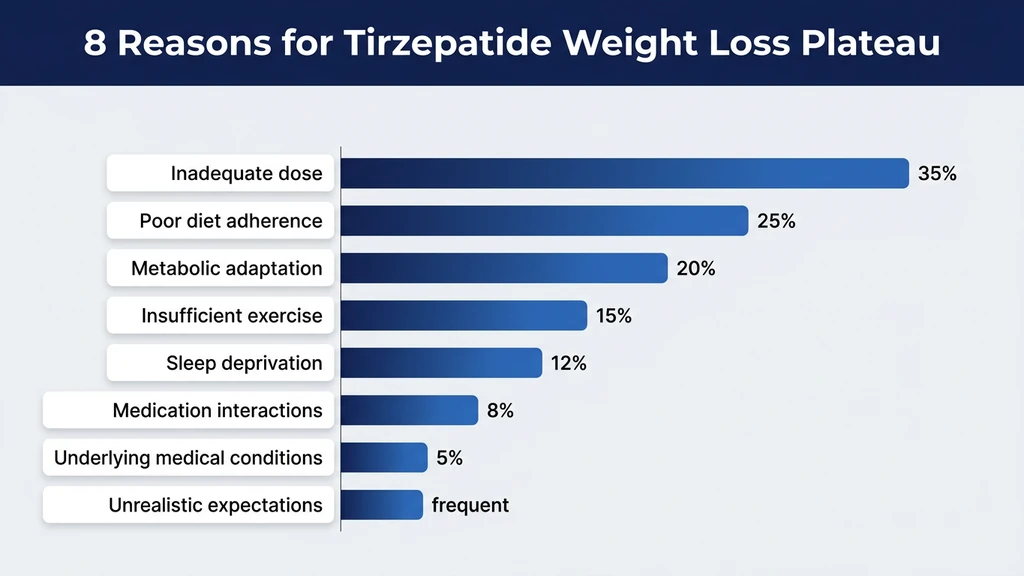
Each of these eight reasons has a defined mechanism and a targeted fix. Most users who stall on tirzepatide have two or three of these operating at the same time. Read through all eight before deciding which apply to your situation.
1. Your Dose Is Too Low or You Are Still Titrating
The standard titration for Zepbound starts at 2.5 mg and increases every 4 weeks: 2.5, 5, 7.5, 10, 12.5, then 15 mg. At the 2.5 mg starting dose, meaningful weight loss is uncommon. That dose exists to acclimate your GI tract, not to drive fat loss.
Some providers stretch each step to 6 or 8 weeks to reduce nausea. That approach is clinically safe, but it means you may not reach a therapeutic dose for 6-8 months. During that window, your results will lag behind the published trial averages because those trials followed the standard 4-week escalation.
The fix: Confirm with your provider that you are on schedule. If GI side effects are manageable at your current dose, ask about advancing to the next step without delay. The tirzepatide dosage calculator converts your milligram dose into syringe units for your vial concentration. If the unit-to-milligram conversion is unclear, our guide on how many units is 2.5 mg of tirzepatide walks through the arithmetic.
In SURMOUNT-1, the dose-response relationship was steep. Participants on 5 mg lost 15.0%, those on 10 mg lost 19.5%, and those on 15 mg lost 22.5% (Jastreboff et al., 2022). Every dose step matters.
2. You Have Not Given It Enough Time (The Week 8-14 Plateau)
A weight loss stall around weeks 8-14 is so predictable that researchers account for it in trial design. It occurs because your body's metabolic defense system triggers in response to sustained caloric deficit.
Think of it as a fuel gauge recalibrating. You burn through a quarter tank quickly, then the gauge appears to stop moving. The fuel is still burning. The gauge is adjusting its reading. Your body does something similar: it detects the deficit, reduces energy expenditure temporarily, and shifts fluid retention. The plateau breaks when the next dose increase overwhelms the compensation.
The fix: Patience. If you are still titrating, the next dose increase will push through the stall. If you are already at 10 or 15 mg, wait 4-6 more weeks. SURMOUNT-1 data shows consistent weight loss resumption after the mid-trial plateau in most participants (Jastreboff et al., 2022). Altering diet, exercise, and medication simultaneously during a plateau creates too many variables to identify what is working.
3. Your Caloric Intake Is Still Too High
Tirzepatide suppresses appetite through dual GIP and GLP-1 receptor activation. It reduces food intake by approximately 20-25% in most users. But if your starting intake was 3,200 calories and the drug cuts it to 2,500, you may still be above your maintenance level. The drug closed the gap without creating a deficit.
This is the most frequently fixable reason for stalled weight loss. Research on caloric reporting found that self-estimated intake underestimates actual consumption by 30-40% (Lichtman et al., 1992). Cooking oils, liquid calories, and between-meal snacking are the typical blind spots.
The fix: Track every calorie for 7 consecutive days. Use a food scale. Weigh everything. If your daily average exceeds your maintenance calories minus 500, that explains the stall. A 500-calorie daily deficit yields roughly 1 pound of fat loss per week. A smaller deficit produces losses so slow that daily water fluctuations mask them on the scale.
SURMOUNT-1 participants on tirzepatide 15 mg reduced caloric intake by approximately 24% compared to baseline. If you are not feeling meaningful appetite suppression, your dose may be insufficient, or you may be eating around the suppression by responding to habit and environmental cues rather than actual hunger.
4. Muscle Loss Is Reducing Your Metabolic Rate
Every pound of muscle you lose reduces your resting metabolic rate by approximately 6-7 calories per day (Wang et al., 2010). Lose 12 pounds of muscle over 6 months, and your body burns 72-84 fewer calories daily at rest. Over a year, that gap adds up to 8-9 pounds of potential fat loss that never materializes.
Weight loss from GLP-1 and GIP agonists is roughly 60-65% fat and 35-40% lean mass in participants who do not exercise. A person who drops 40 pounds on tirzepatide without resistance training may have lost 14-16 pounds of muscle alongside 24-26 pounds of fat. The metabolic rate has dropped, the caloric deficit has shrunk, and weight loss stalls.
The fix: Resistance training 2-3 times per week and protein intake of 0.7-1.0 grams per pound of body weight. A study on semaglutide combined with exercise showed significantly better body composition outcomes than semaglutide alone, and the same principle applies to tirzepatide (Lundgren et al., 2024). Three weekly sessions of compound movements (squats, deadlifts, presses, rows) for 30-40 minutes each protects muscle mass during caloric restriction.
If unusual fatigue accompanies your plateau, muscle loss may be a contributor. See our article on does tirzepatide make you tired for management strategies.
5. Medication Interactions Are Blunting the Effect
Several common medications cause weight gain that directly offsets tirzepatide's weight loss effect.
Medications that may cause weight gain: - Insulin and sulfonylureas (promote fat storage; reduced in SURPASS trials to prevent hypoglycemia) - Beta-blockers (reduce metabolic rate by 5-10%) - SSRIs and SNRIs (weight gain in 25-30% of users after 6 months) - Corticosteroids (increase appetite, promote visceral fat deposition) - Antihistamines (central appetite stimulation)
Medications that may alter tirzepatide absorption timing: - Tirzepatide slows gastric emptying, which can delay absorption of oral medications - Proton pump inhibitors (altered gastric pH may affect absorption kinetics)
The fix: Review every medication you take with your prescriber. Do not stop any medication on your own. Ask specifically whether any of your current drugs are associated with weight gain and whether safer alternatives exist. In the SURPASS-2 trial comparing tirzepatide to semaglutide in type 2 diabetes, participants on insulin required dose reductions to prevent hypoglycemia, confirming the interaction between these drug classes (Frias et al., 2021).
For a broader understanding of drug interactions with peptides, see our peptide safety guide.
6. Undiagnosed or Undertreated Thyroid Issues
Hypothyroidism reduces resting metabolic rate by 15-40%, depending on severity (Mullur et al., 2014). Subclinical hypothyroidism (elevated TSH, normal free T4) affects 4-10% of adults and frequently goes undetected. It generates enough metabolic friction to stall weight loss even on a potent dual agonist like tirzepatide.
A person with a TSH of 6.5 (normal range: 0.4-4.0) may have a resting metabolic rate 150-250 calories below normal. Over 16 weeks, that gap translates to 4-6 fewer pounds lost. That deficit is large enough to make tirzepatide feel ineffective when the drug itself is functioning correctly.
The fix: Get a thyroid panel (TSH, free T4, free T3) if you have not had one in the past year. Symptoms that mimic tirzepatide side effects include fatigue, cold intolerance, constipation, and dry skin. If your TSH is above 4.0, discuss treatment with your provider. Correcting thyroid function may unlock the weight loss that tirzepatide is designed to produce.
7. Sleep Deprivation and Cortisol Are Working Against You
Sleeping fewer than 6 hours per night increases ghrelin (the hunger hormone) by 14.9% and decreases leptin (the satiety hormone) by 15.5% (Spiegel et al., 2004). Those hormonal shifts counteract tirzepatide's appetite suppression through both its GLP-1 and GIP pathways. You are biochemically fighting the drug with your sleep schedule.
Chronic sleep deprivation also elevates cortisol, which promotes visceral fat storage, raises insulin resistance, and drives cravings for calorie-dense food. Sleep-restricted adults consumed an additional 385 calories per day compared to well-rested controls (Al Khatib et al., 2017). Those 385 extra calories can erase the entire deficit tirzepatide creates.
The fix: Target 7-9 hours of sleep per night. If tirzepatide-related nausea disrupts sleep, move your injection day so that peak GI effects (24-72 hours post-injection) fall during waking hours. For nausea-specific strategies, read does tirzepatide cause diarrhea and does tirzepatide cause headaches, which cover overlapping GI management.
Track sleep for two weeks alongside daily weigh-ins. If you consistently sleep under 6 hours and the scale is frozen, fixing sleep may matter more than adjusting the drug.
8. Insulin Resistance Is Slowing Your Initial Response
Insulin resistance creates metabolic friction that tirzepatide must overcome before fat burning accelerates. In the SURPASS-2 trial (participants with type 2 diabetes and elevated insulin resistance), tirzepatide 15 mg produced 13.1% weight loss, compared to 22.5% in the non-diabetic SURMOUNT-1 population (Frias et al., 2021). That 9.4 percentage point gap is largely attributable to baseline metabolic dysfunction.
Tirzepatide does have an advantage here. Its GIP receptor agonism enhances insulin sensitivity through a pathway that semaglutide cannot access. GIP activation improves beta-cell function and promotes more efficient glucose-dependent insulin secretion. This means tirzepatide's effectiveness against insulin resistance grows over time as the dual mechanism progressively recalibrates metabolic function.
Markers of insulin resistance include fasting insulin above 15 mIU/L, HOMA-IR above 2.5, HbA1c above 5.7%, and waist circumference above 40 inches (men) or 35 inches (women). The more elevated these values, the slower initial weight loss will be.
The fix: Resistance training and reduced refined carbohydrate intake accelerate insulin sensitization alongside tirzepatide. SURPASS-2 participants who remained on tirzepatide for 40 weeks showed continuous improvement in HbA1c and fasting glucose, confirming that the metabolic headwind weakens with time. If insulin resistance is severe and results remain poor after 16 weeks at max dose, your provider may consider adding metformin, which works through a complementary mechanism. For more on the metabolic science, see does tirzepatide burn fat.
The Dual Agonist Advantage and Metabolic Adaptation
Tirzepatide's dual GIP/GLP-1 mechanism provides two distinct pathways to overcome the metabolic adaptation that stalls weight loss on single-agonist drugs. Understanding this mechanism explains both why tirzepatide outperforms semaglutide and why plateaus still occur.
When you lose weight, your resting metabolic rate drops more than body weight alone would predict. This is metabolic adaptation, sometimes called adaptive thermogenesis. A 220-pound person with a BMR of 2,000 calories loses 35 pounds. You would expect BMR to drop to approximately 1,780 (proportional to the new weight). Instead, it may fall to 1,650. That extra 130-calorie deficit is metabolic adaptation (Rosenbaum et al., 2010).
How metabolic adaptation stalls tirzepatide weight loss:
| Factor | Before Tirzepatide | After 30 lbs Lost | Net Effect |
|---|---|---|---|
| BMR | 2,000 cal/day | 1,680 cal/day (-320 actual vs -230 predicted) | 90 fewer calories burned than expected |
| NEAT (fidgeting, walking) | 450 cal/day | 330 cal/day | 120 fewer calories burned |
| TEF (thermic effect of food) | 220 cal/day | 170 cal/day | 50 fewer calories burned |
| Exercise calories | 300 cal/day | 240 cal/day | 60 fewer calories burned |
| Total daily expenditure | 2,970 cal/day | 2,420 cal/day | 550 fewer calories burned |
That 550-calorie swing means the deficit that produced 1.5 pounds per week of fat loss now produces 0.2 pounds per week. The scale appears stuck. Tirzepatide has not stopped working. Your body has adjusted its energy output.
Tirzepatide fights this through two mechanisms that semaglutide lacks. First, GIP receptor activation improves insulin sensitivity independent of GLP-1, allowing more efficient glucose disposal and less energy stored as fat. Second, GIP agonism may enhance thermogenesis in adipose tissue, partially offsetting the BMR decline that causes metabolic adaptation (Samms et al., 2023).
The countermeasures remain the same: resistance training preserves muscle and BMR. Walking 8,000-10,000 steps daily protects NEAT. Eating 0.7-1.0g protein per pound of body weight maintains the thermic effect of food. These interventions reduce the magnitude of adaptation from 15% to 5-8%, enough to keep the scale moving.
For a full overview of weight loss peptides and how different compounds address metabolic adaptation, see our weight loss guide.
What the Clinical Trials Actually Show
Trial averages sell the drug. But averages conceal a wide spread of individual outcomes. The full data across tirzepatide's major trials tells a more complete story.
SURMOUNT-1 (Non-Diabetic Obesity) 2,539 participants. Tirzepatide at 5, 10, or 15 mg weekly for 72 weeks. Average weight loss: 15.0% (5 mg), 19.5% (10 mg), 22.5% (15 mg), versus 3.1% placebo. At 15 mg, 57% of participants lost more than 20% of body weight. Approximately 3% lost less than 5%, the standard threshold for treatment failure. The top quartile lost more than 25%. The bottom quartile lost less than 15% (Jastreboff et al., 2022).
SURMOUNT-2 (Type 2 Diabetes + Obesity) 938 participants. Tirzepatide 10 or 15 mg for 72 weeks. Average weight loss: 12.8% (10 mg) and 14.7% (15 mg) versus 3.2% placebo. The gap between SURMOUNT-1 and SURMOUNT-2 (roughly 8 percentage points at 15 mg) reflects the metabolic drag of insulin resistance and concurrent diabetes medications. Approximately 5-7% lost less than 5% (Garvey et al., 2023).
SURMOUNT-3 (Intensive Lifestyle Intervention + Tirzepatide) 579 participants who completed a 12-week intensive lifestyle program (low-calorie diet) before starting tirzepatide. Average total weight loss (lifestyle + drug): 26.6%. The lifestyle run-in added roughly 4 percentage points beyond tirzepatide alone, and the non-responder rate dropped below 2% (Wadden et al., 2023).
SURMOUNT-4 (Withdrawal Study) 670 participants who lost weight on tirzepatide for 36 weeks, then randomized to continue or switch to placebo for 52 additional weeks. Continuing produced 5.5% further loss. Switching to placebo caused 14.0% regain. This trial confirmed that tirzepatide's effect is ongoing and the drug must be continued for weight maintenance (Aronne et al., 2024).
SURPASS-2 (Tirzepatide vs Semaglutide, Head-to-Head) 1,879 participants with type 2 diabetes. Tirzepatide 15 mg produced 13.1% weight loss versus 6.7% for semaglutide 1 mg over 40 weeks. This is the only direct head-to-head trial, and it compared tirzepatide at its highest dose against semaglutide at a sub-maximal dose (1 mg, not 2.4 mg), which limits the comparison (Frias et al., 2021).
What the non-responder data means for you:
If you have been on tirzepatide 10 mg or 15 mg for at least 16 weeks with less than 5% body weight loss, verify the eight reasons listed above first. True pharmacological non-response (where the drug does not adequately activate your GLP-1 and GIP receptors) is rarer with tirzepatide than with any other approved weight loss medication. Most apparent non-response is under-dosing, insufficient time on the drug, or a correctable medical or behavioral factor.
For a comparison of tirzepatide against the next-generation triple agonist, see our retatrutide vs tirzepatide article.
Tirzepatide vs Semaglutide: What to Do If You Switched and Still Are Not Losing
Many users arrive at tirzepatide after stalling on semaglutide. The dual agonist mechanism is stronger, but switching does not guarantee results if the original problem was behavioral rather than pharmacological.
The numbers in context:
| Metric | Semaglutide 2.4 mg (STEP 1) | Tirzepatide 15 mg (SURMOUNT-1) |
|---|---|---|
| Mean weight loss | 14.9% | 22.5% |
| Participants losing >20% | ~25% | ~57% |
| Non-responder rate (<5% loss) | ~6.5% | ~3% |
| Trial duration | 68 weeks | 72 weeks |
| Mechanism | GLP-1 only | GLP-1 + GIP dual agonist |
(Jastreboff et al., 2022; Wilding et al., 2021)
If you switched from semaglutide to tirzepatide and still are not losing weight, the cause is almost certainly not the drug. At this point, you have tried the two most effective FDA-approved weight loss medications. The explanation lies elsewhere: untracked caloric surplus, medication interactions, thyroid dysfunction, or severe insulin resistance.
Troubleshooting steps for switchers: 1. Confirm your tirzepatide dose is equivalent to or higher than your previous semaglutide dose. Use the semaglutide to tirzepatide switching guide for the conversion table. 2. Allow 12-16 weeks at a stable tirzepatide dose before evaluating. The transition period involves receptor recalibration. 3. Track calories rigorously for one week. The appetite suppression profile differs between the two drugs, and eating habits may not have adjusted. 4. Request comprehensive blood work (thyroid, insulin, metabolic panel).
If semaglutide and tirzepatide both fail after adequate trials, retatrutide represents the next frontier. This triple agonist (GLP-1 + GIP + glucagon receptor) produced 24.2% weight loss at 48 weeks in Phase 2 trials (Jastreboff et al., 2023). It is not yet FDA-approved but is advancing through Phase 3 trials. Learn more in our how does retatrutide work guide.
For cost comparisons between these medications, the peptide cost calculator estimates monthly expenses based on dose and source.
A 4-Week Troubleshooting Protocol
If your weight has stalled on tirzepatide, follow this protocol for 4 weeks before concluding the drug is not working. Each week isolates a single variable. By changing one factor at a time, you can identify exactly what is blocking progress.
Week 1: Audit Your Calories and Protein
Buy a food scale. Download a tracking app. Log every item you eat and drink for 7 consecutive days. No estimating. No skipping the olive oil you cooked with or the oat milk in your latte.
Target numbers: - Daily calories: maintenance level minus 500 (use an online TDEE calculator for your current weight) - Daily protein: 0.7-1.0 grams per pound of current body weight - Daily water: half your body weight in ounces (minimum 64 oz)
At the end of week 1, calculate your daily average. If actual intake exceeds your target, you have found the problem. Adjust portions and move to week 2. If intake is already at or below target, the issue lies elsewhere.
This single step resolves the stall for more than half of tirzepatide users who report the drug has stopped working. The dual GIP/GLP-1 appetite suppression may be functioning perfectly while portion sizes remain unchanged out of habit.
Week 2: Add Resistance Training
Start a basic resistance training program. Three sessions per week, 30-40 minutes each. Focus on compound movements that recruit multiple muscle groups.
Sample schedule: - Monday: Squats, bench press, bent-over rows (3 sets of 8-12 reps each) - Wednesday: Deadlifts, overhead press, lat pulldowns (3 sets of 8-12 reps each) - Friday: Lunges, dumbbell press, cable rows (3 sets of 8-12 reps each)
If you have never lifted weights, start with body weight or light dumbbells. The goal is not to build noticeable muscle in 7 days. The goal is to send a preservation signal: muscle is in use. Do not discard it. That signal prevents further lean mass loss from the caloric deficit.
Resistance training also acutely improves insulin sensitivity. Each session opens glucose channels in muscle cells that stay active for 24-48 hours. This effect is additive to tirzepatide's own insulin-sensitizing action through both its GIP and GLP-1 pathways.
Week 3: Optimize Sleep and Stress
Track your sleep with a wearable or a simple bedtime/wake-time log. Calculate your nightly average.
Action items: - If sleeping less than 7 hours: set a fixed bedtime that allows 7.5-8 hours in bed - If injection-related GI effects disrupt sleep: shift your injection to the morning - If stress is chronic: add 10-15 minutes of walking after dinner (measurably reduces cortisol within 1 week) - Remove screens from the bedroom 30 minutes before sleep - Keep room temperature at 65-68 degrees Fahrenheit
At the end of week 3, compare your average sleep duration to the prior two weeks. If sleep improved and the scale started moving, you have identified the bottleneck. If sleep was already adequate, proceed to week 4.
For managing GI disruption during your protocol, see does tirzepatide cause constipation and does tirzepatide cause diarrhea.
Week 4: Medical Review
Request the following blood tests from your provider:
Essential panel: - TSH and free T4 (thyroid function) - Fasting insulin and fasting glucose (calculate HOMA-IR) - HbA1c (3-month blood sugar average) - Complete metabolic panel (liver, kidney function) - Iron, ferritin, B12, vitamin D
Review with your provider: - Current medication list for weight-gain-promoting drugs - Whether your tirzepatide dose can be increased (if below 15 mg) - Whether compounding pharmacy tirzepatide is safe and requires potency verification - Whether adding metformin would address residual insulin resistance
If all blood work is normal, you are eating at a 500-calorie deficit, exercising 3 times per week, sleeping 7+ hours, and have been at 10-15 mg for 16+ weeks with less than 5% weight loss, you may be a true pharmacological non-responder. This affects roughly 3% of users. The next step is a medication evaluation, not a behavior change.
For proper preparation of your medication, see our guide on how to reconstitute tirzepatide. For general peptide dosage references, check our comprehensive chart.
Side Effects That Signal a Deeper Problem
Certain side effects appearing alongside a weight loss stall point to specific underlying causes. They are diagnostic signals, not just inconveniences.
Fatigue + weight stall: Likely caloric intake too low (below 1,000/day), thyroid dysfunction, or significant muscle loss. The body conserves energy by slowing metabolic output and reducing subjective energy. This is a protective response, not drug failure. Read more in does tirzepatide make you tired.
Hair loss + weight stall: Telogen effluvium triggered by rapid initial weight loss, now followed by a plateau. The hair loss reflects what happened 2-3 months ago (the fast-loss phase), not the current stall. It resolves on its own within 6-9 months. Protein intake above 0.7g per pound of body weight accelerates recovery. See does tirzepatide cause hair loss.
Persistent nausea or GI distress + weight stall: If nausea is severe enough to prevent adequate food intake, the resulting deficit may be too extreme. Paradoxically, eating far too little stalls weight loss through severe metabolic adaptation and cortisol elevation. See does tirzepatide cause headaches for overlapping management strategies.
No appetite suppression at all: This is the strongest signal that the drug is not reaching therapeutic activity. Possible causes include degraded medication (improper storage), incorrect injection technique (injecting into muscle rather than subcutaneous fat), or genuine biological non-response to both GIP and GLP-1 agonism. Verify your reconstitution technique with the tirzepatide reconstitution guide and review storage requirements in how long does tirzepatide last in the fridge. Confirm your vial has not expired using does tirzepatide expire.
Severe constipation + weight stall: Tirzepatide slows gastric emptying, which can cause significant constipation. The retained stool and associated water retention can mask 3-5 pounds of actual fat loss on the scale. See does tirzepatide cause constipation for targeted solutions.
None of these side effects require stopping tirzepatide outright. Each has a targeted fix that addresses the root cause while preserving the medication's weight loss effect.
When to Talk to Your Doctor About Adjusting Treatment
Not every plateau requires medical intervention. But certain signals warrant a conversation with your prescriber rather than self-troubleshooting.
Schedule an appointment if: - You have been at 10-15 mg for 16+ weeks with less than 5% total weight loss - You experience zero appetite suppression at any dose - Side effects are so severe that you cannot maintain adequate nutrition - You have lost more than 15% of body weight and now experience persistent fatigue, hair loss, and cold intolerance simultaneously (possible thyroid or nutritional deficiency) - You are taking insulin or sulfonylureas and experiencing hypoglycemic episodes
Questions to bring to your appointment: 1. Can my dose be increased? (if below 15 mg) 2. Should we check thyroid function and fasting insulin? 3. Are any of my current medications known to cause weight gain? 4. Is my compounded tirzepatide from a verified source? 5. Would adding metformin improve my response?
If tirzepatide at maximum dose with all behavioral optimizations has produced inadequate results, your provider may discuss bariatric surgery referral or enrollment in a retatrutide clinical trial. Both options represent the next tier of intervention. Learn more about retatrutide in our retatrutide dosage guide and retatrutide side effects overview.
If alcohol consumption is part of your routine, review can you drink on tirzepatide. Alcohol reduces fat oxidation by up to 73% and adds untracked liquid calories that directly counteract tirzepatide's mechanism.
Frequently Asked Questions
How long does tirzepatide take to start working for weight loss?
Most users notice appetite suppression within 1-2 weeks. Measurable weight loss (5%+ of body weight) typically requires 12-16 weeks. Full titration to 15 mg takes 20 weeks. SURMOUNT-1 showed 7-9% average weight loss at week 12 and 22.5% at week 72. Judge results at your maintenance dose, not during titration.
What percentage of people do not lose weight on tirzepatide?
Approximately 3% of SURMOUNT-1 participants on tirzepatide 15 mg lost less than 5% of body weight at 72 weeks. This is roughly half the non-responder rate seen with semaglutide (6.5%). True biological non-response is rare. Most reported failures involve correctable factors: insufficient dose, inadequate time on the drug, untracked caloric surplus, or medication interactions.
Why did I stop losing weight on Mounjaro after 3 months?
A plateau between weeks 8 and 14 is biologically predictable. Your body reduces metabolic rate and adjusts hormonal output to resist further weight loss. If you are still titrating, the next dose increase will break through. If you are at maintenance dose, wait 4-6 more weeks. Persistent stalls beyond 16 weeks at max dose require medical evaluation.
Is tirzepatide better than semaglutide for weight loss?
Clinical data says yes. SURMOUNT-1 showed 22.5% weight loss with tirzepatide 15 mg versus 14.9% with semaglutide 2.4 mg in STEP 1. Tirzepatide's dual GLP-1/GIP mechanism provides stronger appetite suppression and better insulin sensitization. The non-responder rate is approximately half that of semaglutide (3% vs 6.5%). Individual response varies.
Can I lose weight on tirzepatide without exercise?
Yes. SURMOUNT-1 participants achieved 22.5% weight loss without a mandated exercise program. SURMOUNT-3 added intensive lifestyle intervention and reached 26.6%. Exercise preserves muscle mass, prevents BMR decline, and improves insulin sensitivity. Without it, roughly 35-40% of weight lost is lean mass rather than fat, which slows long-term progress.
Does tirzepatide work if you have insulin resistance or type 2 diabetes?
Yes, but more slowly. SURMOUNT-2 participants with type 2 diabetes lost 14.7% (15 mg) versus 22.5% in non-diabetic SURMOUNT-1. Tirzepatide's GIP agonism gives it an advantage over semaglutide for insulin-resistant patients. The drug improves insulin sensitivity over time, so results may accelerate the longer you take it.
How do I know if my tirzepatide is working?
Three signals confirm tirzepatide is active: reduced appetite within 1-2 weeks, feeling full faster during meals, and decreased food preoccupation. Weight loss may lag behind appetite changes by 2-4 weeks. If you experience zero appetite suppression after 4 weeks at 5 mg or higher, verify medication potency, injection technique, and storage conditions. If using compounded product, review is compound tirzepatide safe for quality verification steps.
Should I eat less than 1,200 calories a day on tirzepatide?
No. Eating below 1,200 calories daily accelerates muscle loss, triggers severe metabolic adaptation, increases fatigue, and raises gallstone risk. Aim for a 500-750 calorie deficit below your maintenance level. If tirzepatide suppresses appetite so severely that you cannot eat 1,200 calories, discuss a dose reduction with your provider.
The Bottom Line
Tirzepatide is the most effective FDA-approved weight loss medication available. SURMOUNT-1 proved that. But "most effective" does not mean automatic results for every user, and the path from injection to scale movement passes through caloric balance, muscle preservation, sleep quality, thyroid function, insulin resistance, and medication interactions.
Start with the 4-week troubleshooting protocol. Track calories honestly for one week. Add resistance training. Fix sleep. Get blood work. In that order. Most plateaus resolve at step one or two without any medication change.
If you have completed that protocol and remain below 5% weight loss after 16 weeks at 10-15 mg, a medical evaluation is the next step. Review your situation with your prescriber, bringing the blood work and calorie data from the protocol. Use the tirzepatide dosage calculator to confirm your current dose is accurate.
For users who switched from semaglutide, the semaglutide to tirzepatide switching guide and how many units is 2.5 mg of tirzepatide cover the transition. Compare costs with the peptide cost calculator.
Related articles: - How Long Does Tirzepatide Take to Work? — week-by-week timeline showing when results appear at each dose - Tirzepatide Maintenance Dose After Weight Loss — step-down protocols to sustain results long-term - How Long Does Semaglutide Take to Work? — parallel timeline for GLP-1 single agonist users - Not Losing Weight on Semaglutide? 8 Reasons + Fixes — the mirror troubleshooting guide for GLP-1 single agonist users - Does Semaglutide Need to Be Refrigerated? — storage failures can reduce potency and stall weight loss - Does Tirzepatide Burn Fat? — how the dual agonist drives fat loss versus lean mass loss - How to Inject Tirzepatide — correct injection technique to ensure full absorption - Tirzepatide Injection Site Reaction — managing site reactions that may affect adherence - Tirzepatide Cost With Insurance — 2026 coverage options and cost-saving strategies
Explore all peptide profiles and research tools at PeptidesExplorer.com.
Related Articles
Does Tirzepatide Burn Fat?
Tirzepatide produced 33.9% fat mass loss in SURMOUNT-1. Learn how GLP-1/GIP dual agonism drives fat loss, body composition data, and how to protect lean mass.
Not Losing Weight on Semaglutide?
Not losing weight on semaglutide? 5-10% of users are non-responders. Learn 8 fixable reasons, STEP trial data, and a 4-week troubleshooting plan.
Tirzepatide: How Long to Work?
Tirzepatide reduces appetite within the first week, produces measurable weight loss by week 4, and delivers significant results by weeks 12-16.
Tirzepatide Maintenance Dose Guide
Most patients maintain on 5-10 mg tirzepatide weekly after reaching goal weight. SURMOUNT-4 data shows stopping leads to 50-67% weight regain within 12 months.