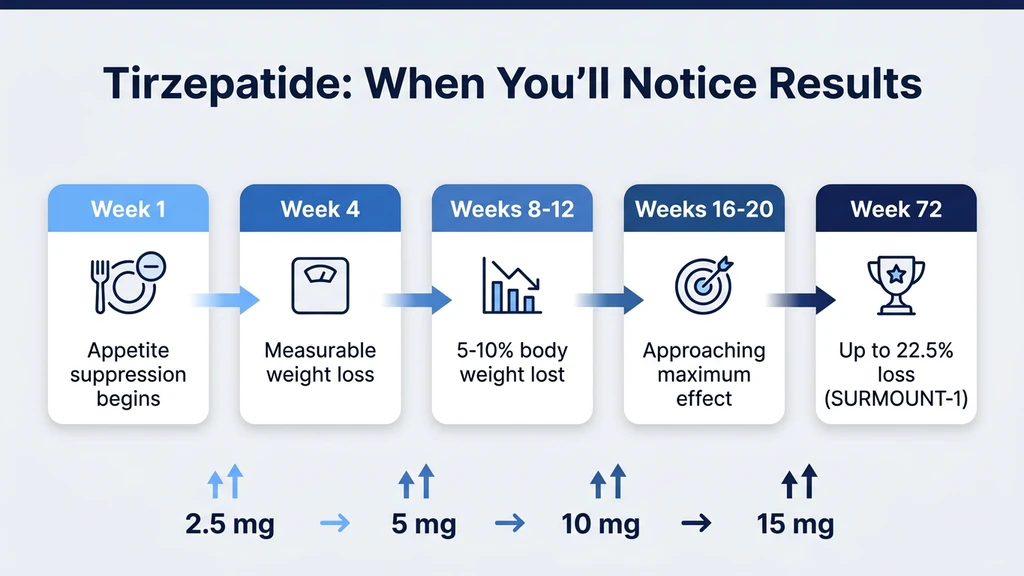
You filled your first tirzepatide prescription, and now you want to know when you will see results. Most people notice reduced appetite within the first week. Measurable weight loss appears by week 4. Significant results, defined as 10% or more of body weight lost, typically arrive between weeks 12 and 16 on the full maintenance dose (Jastreboff et al., NEJM 2022).
| Timeline | What to Expect | Typical Weight Loss |
|---|---|---|
| Week 1 | Appetite suppression, mild GI effects | 1-3 lbs (water/glycogen) |
| Weeks 2-4 | Reduced portion sizes, early fat mobilization | 3-6 lbs total |
| Weeks 4-8 | Dose escalation to 5 mg, stronger satiety | 5-10 lbs total |
| Weeks 8-12 | Dose escalation to 7.5-10 mg, steady fat loss | 8-15 lbs total |
| Weeks 12-16 | Maintenance dose (10-15 mg), significant results | 12-20+ lbs total |
| Weeks 16-72 | Continued loss, curve flattening after week 36 | 15-25% of body weight |
Use our tirzepatide dosage calculator to plan your titration schedule. For dosing in units, see the tirzepatide dosage chart.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
What Happens During the First Week on Tirzepatide
The first injection of 2.5 mg starts working within hours, not weeks. GLP-1 and GIP receptor activation begins as soon as plasma concentrations rise, which occurs within 8-12 hours of the subcutaneous injection. Peak levels are reached around 24-72 hours post-dose (Eli Lilly prescribing information, 2023).
Most people notice the first effect as a shift in appetite. Food becomes less interesting. The constant background noise of hunger quiets. Portions that felt normal on Sunday feel excessive by Wednesday. This is GLP-1 receptor activation in the hypothalamus, dampening the hunger drive before any weight loss occurs.
Gastric emptying also slows. Meals sit longer in the stomach, extending the feeling of fullness. Some people describe it as eating half a sandwich and feeling done, when they used to eat the whole thing without thinking. This effect is measurable on the first dose, though it intensifies with repeated injections. For step-by-step technique, see how to inject tirzepatide.
The scale may drop 1-3 pounds during week one. That is almost entirely water and glycogen. Improved insulin sensitivity reduces glycogen stores, and each gram of glycogen holds 3-4 grams of water. Reduced sodium intake from eating less compounds the fluid loss. Genuine fat mobilization begins around days 10-14.
Weeks 2 Through 4: The Starting Dose Window
The standard protocol holds the dose at 2.5 mg for four full weeks. This is not a therapeutic dose for weight loss. It is a tolerability phase designed to let the GI tract adapt before the dose increases.
During this window, appetite suppression is moderate. Some people feel underwhelmed. The caloric deficit at 2.5 mg is roughly 200-400 calories per day for most users, enough to produce 0.5-1 pound of true fat loss per week. The scale may show 3-6 pounds total by week 4, but roughly half of that is still water and glycogen shifting.
GI side effects peak during weeks 2-3 for most people. Nausea affects about 12-18% of users at 2.5 mg, compared to 24-31% at higher doses (Jastreboff et al., NEJM 2022). The nausea tends to be worst 24-48 hours after injection and fades over the following days. For strategies to manage nausea, see our guide on semaglutide nausea, which applies equally to tirzepatide. For constipation during this phase, see does tirzepatide cause constipation.
Some people notice improved fasting blood glucose by week 3-4. In the SURPASS-1 trial (type 2 diabetes population), tirzepatide 5 mg reduced HbA1c by 1.87% over 40 weeks, with meaningful glucose improvements visible in the first month (Rosenstock et al., NEJM 2021).
How Dose Escalation Changes the Timeline
Think of tirzepatide like adjusting the volume dial on appetite suppression. The starting 2.5 mg is volume 2 out of 10. Each dose increase turns the dial higher. Most people feel a meaningful shift at 5 mg and a strong effect at 10 mg. The full 15 mg dose is volume 10, though not everyone needs or tolerates it.
The standard titration is 2.5 mg for 4 weeks, then 5 mg for 4 weeks, then increases of 2.5 mg every 4 weeks up to a maximum of 15 mg. Here is what each dose level typically produces:
2.5 mg (Weeks 1-4): Tolerability Phase
This dose is below the threshold for significant weight loss in most adults. Its purpose is GI adaptation. The body needs time to adjust to delayed gastric emptying and altered gut motility.
Average weight loss at 2.5 mg: 2-4% of body weight over 4 weeks. For a 220-pound person, that translates to roughly 4-9 pounds, with most of the early loss being water. The caloric deficit is modest, and appetite suppression is noticeable but not dramatic.
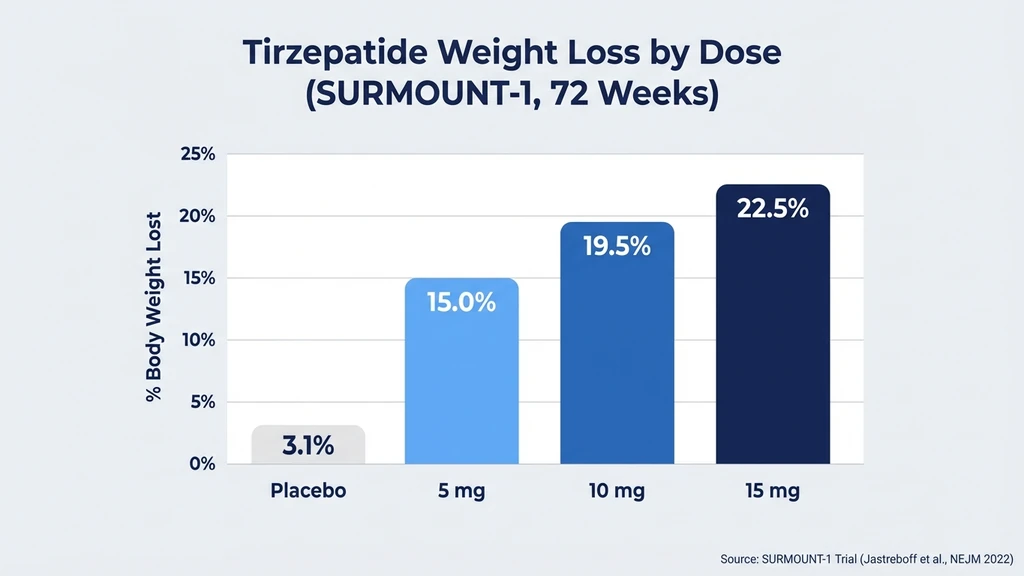
Do not judge tirzepatide's effectiveness based on this dose. SURMOUNT-1 data show the 5 mg arm (the lowest therapeutic dose studied for obesity) produced 16.0% weight loss at 72 weeks, while 15 mg produced 22.5%. The starting dose is a stepping stone, not the destination.
5 mg (Weeks 5-8): First Therapeutic Dose
The jump from 2.5 mg to 5 mg is where most people feel tirzepatide "kick in." Appetite suppression becomes more consistent throughout the week rather than fading by day 5-6 after each injection. Food noise, the persistent mental chatter about what to eat next, drops significantly.
The caloric deficit widens to approximately 400-600 calories per day. Fat loss accelerates to roughly 1-1.5 pounds per week. GI side effects may resurface for 1-2 weeks after the increase, then settle. Headaches occur in about 6% of users during dose transitions; see our guide on tirzepatide headaches.
In SURMOUNT-1, the 5 mg arm produced 16.0% total body weight loss over 72 weeks. Many clinicians keep patients at 5 mg if appetite is well-controlled and weight loss trajectory meets expectations (Jastreboff et al., NEJM 2022).
10 mg (Weeks 9-16): Strong Therapeutic Effect
At 10 mg, dual GIP/GLP-1 activation is at full force for most users. Appetite suppression is strong. Meals that once felt like reasonable portions now feel large. Some users report needing conscious effort to eat enough protein and nutrients, since the hunger drive is significantly blunted.
The caloric deficit can reach 600-800 calories per day. Weight loss at this dose runs 1.5-2 pounds per week during the active loss phase. By week 12-16 on 10 mg, most users have crossed the 10% total body weight loss threshold.
SURMOUNT-1 showed the 10 mg arm produced 21.4% weight loss at 72 weeks. The difference between 10 mg and 15 mg was only 1.1 percentage points (21.4% vs 22.5%), suggesting diminishing returns beyond 10 mg for many users. Fatigue during this phase is common; see does tirzepatide make you tired for management strategies.
15 mg (Weeks 13-20+): Maximum Dose
The 15 mg dose is reserved for patients who need additional weight loss beyond what 10 mg provides. Not everyone reaches this dose, and not everyone should. The incremental benefit is real but modest: approximately 1 additional percentage point of total weight loss compared to 10 mg, with increased GI side effect risk.
At 15 mg, nausea rates reach 24-31% and diarrhea affects about 17% of users. For diarrhea management, see does tirzepatide cause diarrhea. Some clinicians opt to keep patients at 10 mg if tolerance is poor, since the efficacy difference is small.
SURMOUNT-1 participants on 15 mg lost an average of 22.5% of body weight at 72 weeks. The top quartile of responders exceeded 30% total body weight loss. The bottom quartile lost under 15%. Individual response varies substantially.
Why the Dual GIP/GLP-1 Mechanism Affects the Timeline
Semaglutide activates one receptor (GLP-1). Tirzepatide activates two (GLP-1 and GIP). That dual mechanism changes both the speed and magnitude of results.
GLP-1 receptor activation handles appetite suppression and gastric slowing. These effects start within hours and produce the early appetite changes you feel in week one. GIP receptor activation adds a second layer: it amplifies the satiety signal, improves insulin sensitivity in adipose tissue, and may directly influence how fat cells metabolize lipids (Nauck & Muller, 2023).
The GIP component takes longer to show its full effect. GIP receptor signaling in fat tissue and the brain builds over weeks of consistent exposure. This explains why many users report a step-change in appetite suppression around weeks 3-4, even at the same dose. The GLP-1 effect is immediate; the GIP effect accumulates.
SURPASS-2 compared tirzepatide head-to-head against semaglutide 1 mg. At 40 weeks, tirzepatide 15 mg produced 13.1% weight loss versus 6.7% for semaglutide. Even tirzepatide 5 mg outperformed semaglutide 1 mg (7.6% vs 6.7%), suggesting the GIP component accelerates the timeline meaningfully (Frias et al., NEJM 2021). For dose equivalency between the two drugs, see our semaglutide to tirzepatide conversion guide.
Appetite Changes vs Weight Loss vs Metabolic Improvements
These three categories of results follow different timelines. Treating them as one leads to frustration when the scale lags behind how you feel.
Appetite Changes: Days 1-7
Appetite suppression is the fastest visible effect. Most users feel it within the first 3-5 days. Reduced hunger, smaller portions, decreased food cravings, and less interest in snacking are the hallmark early signs.
This is the GLP-1 receptor acting on the hypothalamus and brainstem to lower the appetite set point. The effect is dose-dependent: mild at 2.5 mg, moderate at 5 mg, strong at 10-15 mg. Some users describe the feeling as "food noise turning off," where the constant mental preoccupation with eating simply quiets.
Appetite changes precede weight loss by 1-2 weeks. You will eat less before the scale moves. This gap is normal and reflects the time needed to accumulate a sufficient caloric deficit for measurable fat loss.
Weight Loss: Weeks 2-4 Onward
True fat loss begins around weeks 2-3, once the initial water/glycogen shift stabilizes. The rate depends on the caloric deficit, which depends on the dose.
At 2.5 mg, expect 0.5-1 lb of fat per week. At 5 mg, 1-1.5 lbs. At 10-15 mg, 1.5-2 lbs. These rates are averages; individual variation is wide. Body weight on the scale will fluctuate day-to-day due to water retention, sodium intake, and bowel patterns. Weekly weigh-ins taken under consistent conditions (same time, same state of dress, after voiding) are more reliable than daily checks.
SURMOUNT-1 showed the steepest weight loss curve between weeks 4 and 36, with approximately 80% of total weight lost during this window. The curve flattened between weeks 36 and 72 (Jastreboff et al., NEJM 2022). For a complete analysis of the weight loss data, see does tirzepatide burn fat.
Metabolic Improvements: Weeks 4-12
Blood glucose, insulin sensitivity, triglycerides, and blood pressure improve on a timeline that trails weight loss by 2-4 weeks. These changes are clinically meaningful but not visible in the mirror.
In SURPASS-1, tirzepatide reduced HbA1c by 1.87-2.07% (depending on dose) over 40 weeks, with the steepest decline between weeks 4 and 16. Fasting glucose dropped by 43-59 mg/dL. Triglycerides fell by 19-25% (Rosenstock et al., NEJM 2021).
Blood pressure reductions of 4-7 mmHg systolic were observed in SURMOUNT-1, driven by weight loss and improved insulin sensitivity. These effects accumulated gradually over weeks 8-24 and stabilized thereafter.
If you are using tirzepatide for type 2 diabetes, metabolic improvements are often the primary treatment goal. Discuss target HbA1c and glucose ranges with your prescriber.
Tirzepatide vs Semaglutide: Which Works Faster?
Both drugs begin working within the first week, but tirzepatide produces faster and larger total results at equivalent points in the treatment timeline.
The head-to-head SURPASS-2 trial provides the clearest comparison. At 40 weeks, tirzepatide 15 mg produced 13.1% weight loss versus 6.7% for semaglutide 1 mg. Tirzepatide 10 mg produced 11.2%, and even the 5 mg dose beat semaglutide at 7.6% (Frias et al., NEJM 2021).
| Timepoint | Tirzepatide 15 mg | Semaglutide 2.4 mg* | Difference |
|---|---|---|---|
| Week 4 | ~3-4% loss | ~2-3% loss | ~1% faster |
| Week 12 | ~8-10% loss | ~6-7% loss | ~2-3% faster |
| Week 24 | ~14-16% loss | ~10-12% loss | ~4% faster |
| Week 52 | ~20-22% loss | ~13-15% loss | ~7% faster |
| Week 72 | ~22.5% loss | ~14.9% loss | ~7.6% faster |
*Cross-trial comparison: tirzepatide from SURMOUNT-1, semaglutide from STEP 1. Not a head-to-head trial at these doses.
The speed advantage comes from the GIP receptor. GLP-1-only drugs like semaglutide produce strong appetite suppression, but tirzepatide's dual activation creates a deeper sustained deficit. Tirzepatide also produces less nausea at comparable efficacy levels: 31% nausea at 15 mg versus 44% for semaglutide at 2.4 mg. Less nausea means fewer missed meals, better nutrition, and more consistent drug use.
For people switching between drugs, see our semaglutide dosage chart and conversion guide. If you are not losing weight on semaglutide, switching to tirzepatide is a common next step; see not losing weight on semaglutide.
Retatrutide, Eli Lilly's triple agonist (GLP-1/GIP/glucagon), showed 24.2% weight loss at 48 weeks in Phase 2, suggesting even faster results. It is still in Phase 3 trials. See our retatrutide vs tirzepatide comparison for more detail.
Factors That Speed Up or Slow Down Your Results
Not everyone responds to tirzepatide at the same rate. Clinical trial data and prescriber reports identify several variables that shift the timeline forward or backward.
Starting Weight and BMI
People with higher starting BMIs tend to lose weight faster in absolute pounds but slower as a percentage of body weight during the first 4-8 weeks. A 300-pound person may lose 8-10 pounds in the first month, while a 200-pound person may lose 5-7 pounds.
However, percentage-based results converge by weeks 12-16. SURMOUNT-1 enrolled participants with BMI 30 or higher, and the 22.5% average loss at 72 weeks was consistent across BMI subgroups. Starting heavier does not mean a smaller total percentage lost over the full treatment course.
Insulin Resistance and Metabolic Status
People with type 2 diabetes or significant insulin resistance tend to lose weight more slowly on tirzepatide compared to metabolically healthy obese individuals. SURPASS trials (diabetes population) showed lower percentage weight loss than SURMOUNT trials (obesity without diabetes) at comparable doses.
At 15 mg over 40 weeks, SURPASS-2 participants lost 13.1% of body weight, while SURMOUNT-1 participants on the same dose lost 22.5% over 72 weeks. Part of this difference is the longer treatment duration, but the rate per week was also slower in the diabetes population. Insulin resistance blunts the body's ability to mobilize fat stores efficiently, and improved glucose control sometimes increases appetite slightly as hypoglycemic episodes decrease.
Diet Quality and Protein Intake
Tirzepatide suppresses appetite, but it does not choose your food. Users who prioritize protein (1.2-1.6 g/kg daily) and whole foods lose more fat and less muscle than those who eat whatever fits into their reduced appetite.
A common mistake: eating 800-1,000 calories daily because the drug eliminates hunger. Extreme caloric restriction accelerates lean mass loss, slows metabolism, and increases the risk of gallstones. The drug is doing the deficit work. Aim for at least 1,200-1,500 calories with adequate protein. See our peptide safety guide for nutrition guidelines during GLP-1 treatment.
Physical Activity
Resistance training does not dramatically accelerate weight loss on the scale, but it shifts the composition of what is lost. SURMOUNT-3 combined tirzepatide with intensive lifestyle intervention (including structured exercise) and achieved a fat-to-lean loss ratio of approximately 3:1, compared to 2:1 with the drug alone (Wadden et al., 2023).
Cardio adds a modest caloric deficit (200-400 calories per session) that can speed the scale by 0.25-0.5 lbs per week. Resistance training preserves muscle, which maintains metabolic rate and improves long-term outcomes. Both matter, but if you only do one, choose resistance training.
Adherence and Injection Consistency
Missing doses slows results more than any other factor. Tirzepatide's half-life is approximately 5 days, so missing a weekly injection by 2-3 days significantly reduces plasma levels. Missing an entire dose allows appetite to rebound, often resulting in compensatory overeating that erases several days of deficit.
Inject on the same day each week, within a 2-hour window. If you miss a dose by more than 4 days, take it as soon as possible and resume the regular schedule. If you miss two consecutive doses, contact your prescriber before resuming, as GI tolerance may need to be re-established.
For proper preparation and storage of compounded tirzepatide, see how to reconstitute tirzepatide and how long does tirzepatide last in the fridge. For understanding how the drug clears your system, see how long does tirzepatide stay in your system.
When Tirzepatide Is Not Working: Red Flags and Fixes
If you have been on tirzepatide for 8 or more weeks and see less than 3-4% total body weight loss, something is off. Here are the most common causes and their solutions.
Dose is too low. The 2.5 mg starting dose is sub-therapeutic for weight loss in most adults. If your prescriber has not escalated past 2.5 mg after 4 weeks, ask about moving to 5 mg. Most non-responders at 2.5 mg become responders at 5-10 mg.
Caloric intake exceeds the deficit. Tirzepatide suppresses appetite, but liquid calories (smoothies, alcohol, sugary drinks) and calorie-dense snacks can override the deficit entirely. A single large restaurant meal can erase 3-4 days of deficit. Track intake for one week to identify leaks. Alcohol is a particular concern; see can you drink on tirzepatide.
Medication interactions. Certain medications (corticosteroids, insulin, sulfonylureas, some antipsychotics) promote weight gain and can counteract tirzepatide's deficit. Review your medication list with your prescriber if weight loss has stalled.
Unrealistic timeline expectations. Some people respond slowly during the first 8 weeks and then accelerate between weeks 12 and 24. The dose escalation schedule means most users are not on a fully therapeutic dose until week 8-12. Patience through the titration phase is essential.
Counterfeit or degraded product. Compounded tirzepatide that has been improperly stored, exposed to heat, or sourced from unreliable compounding pharmacies may have reduced potency. For safety considerations around compounded products, see is compound tirzepatide safe. If results stop abruptly, product quality should be investigated. Check does tirzepatide expire for storage guidelines.
Long-Term Results: What Happens After 6, 12, and 18 Months
The SURMOUNT clinical trial program provides the longest follow-up data for tirzepatide in obesity.
6 months (week 24): Most participants had lost 14-16% of body weight on the 15 mg dose. Fat loss accounted for approximately 60-65% of total weight lost. Visceral fat declined by an estimated 30-40% based on imaging substudies. HbA1c and fasting glucose were near their maximum improvement.
12 months (week 52): Weight loss reached approximately 20-22% on 15 mg. The rate of loss had slowed significantly compared to months 3-6. Body composition shifted further toward fat loss as lean mass stabilization occurred in users who maintained protein intake and physical activity. Waist circumference decreased by an average of 14.5 cm (5.7 inches) on 15 mg.
18 months (week 72): The SURMOUNT-1 endpoint. Average weight loss was 22.5% at 15 mg, 21.4% at 10 mg, and 16.0% at 5 mg. The curve was essentially flat between weeks 52 and 72, indicating a new equilibrium. Approximately 63% of participants on 15 mg lost 20% or more of body weight. About 36% lost 25% or more (Jastreboff et al., NEJM 2022).
After stopping: SURMOUNT-4 studied what happens when tirzepatide is discontinued. Participants who stopped after 36 weeks regained approximately 14% of lost weight over the following year. Those who continued lost an additional 5.5%. The drug must be continued to maintain results, because the appetite suppression ends when the drug clears (Aronne et al., JAMA 2024). For clearance timing, see how long tirzepatide stays in your system.
Common Mistakes That Delay Results
Weighing daily and panicking at fluctuations. Body weight varies by 2-4 pounds day-to-day based on water, sodium, food volume, and bowel habits. A single daily reading tells you nothing about fat loss trends. Weigh weekly under identical conditions, or use a 7-day moving average.
Skipping the first dose increase out of fear. Some users tolerate 2.5 mg well, feel nervous about side effects, and stay at the starting dose for 8-12 weeks. The 2.5 mg dose produces minimal weight loss in most people. Moving to 5 mg is where the drug becomes therapeutic. The GI side effects of dose escalation are usually mild and transient (1-2 weeks).
Eating too little and losing muscle. Tirzepatide can suppress appetite so effectively that some users eat under 800 calories daily. This accelerates lean mass loss, drops metabolic rate, and sets the stage for rebound weight gain. Aim for a minimum of 1,200 calories with at least 100 grams of protein daily. For body composition data on tirzepatide, see does tirzepatide burn fat.
Ignoring GI side effects instead of managing them. Nausea, constipation, and diarrhea are manageable with proper strategies: eating smaller meals, avoiding high-fat foods, staying hydrated, and using ginger or anti-nausea medication if needed. Unmanaged GI symptoms lead to poor nutrition, missed doses, and treatment abandonment. See our guides on tirzepatide constipation and tirzepatide diarrhea.
Important Safety Information
Tirzepatide is a prescription medication sold as Mounjaro (type 2 diabetes) and Zepbound (obesity). It requires a prescription and medical supervision. Do not self-prescribe or share medication.
Individuals with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2 should not use tirzepatide. The drug carries a boxed warning for thyroid C-cell tumors based on rodent studies.
Do not combine tirzepatide with other GLP-1 receptor agonists (semaglutide, liraglutide, dulaglutide). Overlapping mechanisms increase the risk of severe gastroparesis, bowel obstruction, and pancreatitis.
Report severe abdominal pain, persistent vomiting, or signs of allergic reaction to your prescriber immediately. For hair thinning during treatment, see does tirzepatide cause hair loss. For a broader look at safety, see our peptide safety guide.
This content is for educational and research purposes. Consult a qualified healthcare provider before starting, adjusting, or stopping any medication.
Frequently Asked Questions
How quickly does tirzepatide suppress appetite?
Most people notice reduced appetite within 3-5 days of the first injection. GLP-1 receptor activation in the hypothalamus begins within 8-12 hours of dosing, and peak plasma levels occur at 24-72 hours. Appetite suppression strengthens over the first 2-3 weeks as GIP receptor effects accumulate. Dose escalation from 2.5 mg to 5 mg produces a noticeable step-up in appetite control.
How much weight can you lose on tirzepatide in 3 months?
At 12 weeks, SURMOUNT-1 data show participants on the 15 mg track lost approximately 8-12% of body weight. For a 220-pound person, that translates to roughly 18-26 pounds. Most users are still titrating during this window, so results depend heavily on dose escalation speed. Users reaching 10 mg by week 8 tend to hit the higher end of this range.
Does tirzepatide work faster than semaglutide?
Yes. SURPASS-2 showed tirzepatide 15 mg produced 13.1% weight loss at 40 weeks versus 6.7% for semaglutide 1 mg. Cross-trial comparisons between SURMOUNT-1 and STEP 1 show tirzepatide producing roughly 50% more total weight loss (22.5% vs 14.9%) at similar timepoints. The GIP receptor activation accounts for the faster and greater response.
Why am I not losing weight on tirzepatide after 4 weeks?
The 2.5 mg starting dose is a tolerability phase, not a therapeutic weight loss dose. Most users see significant results only after escalating to 5 mg or higher. If you are at 5 mg or above with less than 3% loss after 8 weeks, check for liquid calorie intake, medication interactions, or product quality issues. Discuss dose adjustment with your prescriber.
What is the best dose of tirzepatide for weight loss?
SURMOUNT-1 showed 10 mg produced 21.4% weight loss and 15 mg produced 22.5% at 72 weeks. The difference is small, and 15 mg carries higher GI side effect rates (31% nausea vs 24%). Many clinicians target 10 mg as the optimal balance of efficacy and tolerability. Individual response determines whether escalating to 15 mg is worthwhile.
How long do tirzepatide side effects last?
GI side effects (nausea, diarrhea, constipation) typically peak during the first 2-3 weeks at each new dose level and then subside. Most users report significant improvement by week 4-6 of a given dose. Nausea is the most common side effect, affecting 12-31% of users depending on dose, and usually resolves within 1-2 weeks of adaptation. For detailed timelines, see our semaglutide side effects duration guide, which follows a similar pattern.
When does tirzepatide reach peak effectiveness?
Peak weight loss rate occurs between weeks 12 and 24, after the user has reached a stable maintenance dose (typically 10-15 mg). Pharmacological steady state requires approximately 4-5 half-lives (20-25 days at a consistent dose). Approximately 80% of total weight loss occurs in the first 36 weeks, with the curve flattening significantly after that point.
Will I regain weight if I stop tirzepatide?
SURMOUNT-4 showed that participants who stopped tirzepatide after 36 weeks regained approximately 14% of lost weight over the following 12 months. Those who continued lost an additional 5.5%. The drug suppresses appetite; removing it allows hunger to return to pre-treatment levels. Ongoing treatment, combined with dietary and exercise habits, is required for weight maintenance.
The Bottom Line
Tirzepatide works on three overlapping timelines. Appetite changes arrive within the first week. Measurable weight loss begins by week 4. Significant results (10% or more of body weight lost) occur between weeks 12 and 16, once the dose has been titrated to a therapeutic level. SURMOUNT-1 showed 22.5% average weight loss at the 15 mg dose over 72 weeks.
The dual GIP/GLP-1 mechanism makes tirzepatide faster and more effective than single-receptor GLP-1 drugs like semaglutide. The titration schedule determines how quickly you reach peak effect: each 4-week dose increase turns up the volume on appetite suppression and caloric deficit.
Use our tirzepatide dosage calculator to map your titration. For unit conversions, see the tirzepatide dosage chart. To compare costs across your treatment timeline, use the peptide cost calculator.
Related articles: - Why Am I Not Losing Weight on Tirzepatide? — 8 fixable reasons and a 4-week troubleshooting protocol - Tirzepatide Maintenance Dose After Weight Loss — step-down protocols for long-term weight maintenance - How Long Does Semaglutide Take to Work? — parallel timeline for semaglutide users considering switching - Does Tirzepatide Burn Fat? — body composition data and fat-to-lean ratios - Retatrutide vs Tirzepatide — comparing dual vs triple agonists - How to Reconstitute Tirzepatide — preparation guide for compounded product - How to Inject Tirzepatide — step-by-step injection guide for beginners - Tirzepatide Cost With Insurance — 2026 pricing and coverage options - Is Compound Tirzepatide Safe? — safety considerations for compounded products
Related Articles
Does Compounded Tirzepatide Work? Real Data
Does compounded tirzepatide work? Review SURMOUNT data, salt form differences (base, acetate, sodium), potency gaps, and FDA status in 2026.
Not Losing Weight on Tirzepatide?
Not losing weight on tirzepatide? About 3% of users are non-responders. Learn 8 fixable reasons, SURMOUNT trial data, and a 4-week troubleshooting protocol.
Tirzepatide Maintenance Dose Guide
Most patients maintain on 5-10 mg tirzepatide weekly after reaching goal weight. SURMOUNT-4 data shows stopping leads to 50-67% weight regain within 12 months.
Does Tirzepatide Burn Fat?
Tirzepatide produced 33.9% fat mass loss in SURMOUNT-1. Learn how GLP-1/GIP dual agonism drives fat loss, body composition data, and how to protect lean mass.