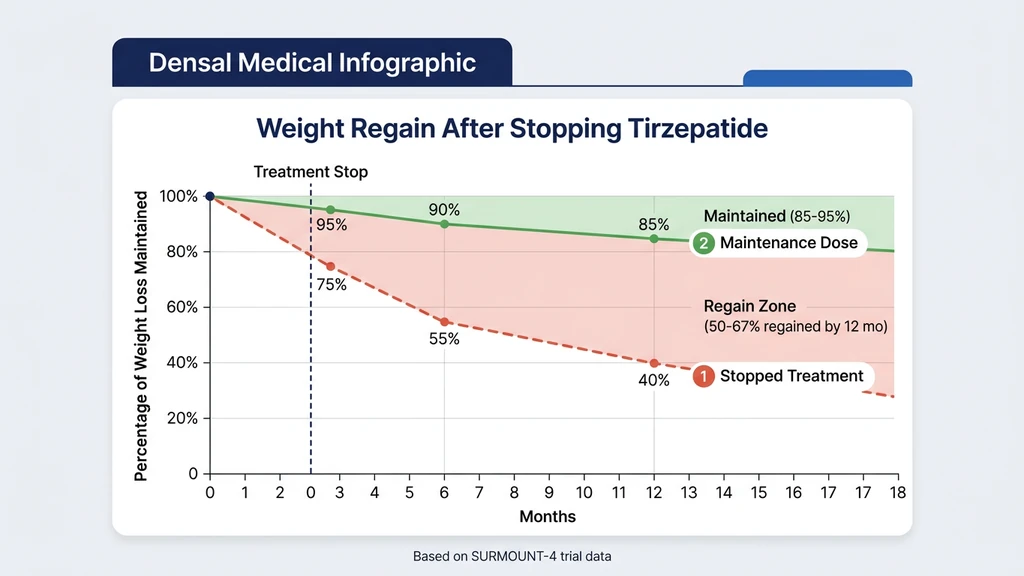
You hit your goal weight on tirzepatide. The scale reads a number you have not seen in years. Now the question that keeps you up at night: what happens next? Most patients maintain their weight loss on 5 to 10 mg of tirzepatide weekly after reaching their target. Stopping entirely leads to 50 to 67% weight regain within 12 months, according to the SURMOUNT-4 extension study (Aronne et al., JAMA 2024).
The maintenance dose is almost always lower than the dose that got you to your goal. Finding it requires a deliberate step-down, not an abrupt stop.
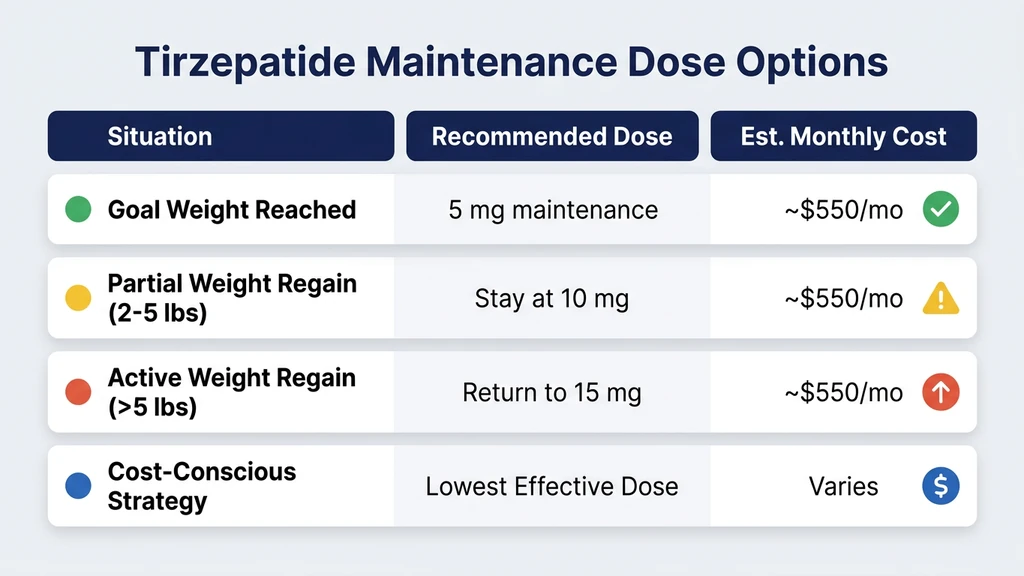
| Scenario | Recommended Maintenance Dose | Expected Outcome |
|---|---|---|
| Reached goal on 15 mg, tolerating well | 5-10 mg weekly | Maintain 85-95% of weight lost |
| Reached goal on 10 mg | 5-7.5 mg weekly | Maintain 80-90% of weight lost |
| Reached goal on 5-7.5 mg | 2.5-5 mg weekly | Maintain 75-85% of weight lost |
| Strong lifestyle habits (high protein, resistance training) | Lowest tolerated dose (2.5-5 mg) | May sustain loss with minimal pharmacological support |
| Stopping entirely | 0 mg | 50-67% of lost weight returns within 12 months |
| Switching to semaglutide maintenance | 1.0-1.7 mg semaglutide weekly | Partial maintenance; less effective than tirzepatide |
If you want help calculating your specific maintenance draw, the Tirzepatide Dosage Calculator converts any dose to units for your vial concentration.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
What SURMOUNT-4 Revealed About Stopping Tirzepatide
SURMOUNT-4 is the study that answered the question nobody wanted to ask. Eli Lilly enrolled 670 adults with obesity who had already lost an average of 20.9% of their body weight on tirzepatide over 36 weeks. Then they randomized half to continue tirzepatide and half to switch to placebo for another 52 weeks (Aronne et al., JAMA 2024).
The results were stark. Participants who stayed on tirzepatide lost an additional 5.5% body weight over the following year. Those switched to placebo regained 14.0% of their body weight from the randomization point. By week 88, the placebo group had regained roughly half of what they originally lost.
The biology explains why. Tirzepatide suppresses appetite by activating both GIP and GLP-1 receptors. When the drug clears your system (the half-life is approximately 5 days, fully cleared within 25 to 30 days), hunger hormones rebound. Ghrelin rises. Leptin sensitivity drops. The hypothalamus recalibrates toward your pre-treatment weight set point (Jastreboff et al., NEJM 2022). This is not a willpower failure. It is endocrine physiology.
The takeaway from SURMOUNT-4: some level of continued pharmacological support preserves the metabolic benefits. The question is how much.
Finding Your Lowest Effective Maintenance Dose
The goal of maintenance dosing is to find the smallest dose that holds your weight stable while minimizing side effects and cost. Think of it like a thermostat. During weight loss, you set the thermostat aggressively low to force change. During maintenance, you dial it to the temperature you want to keep. Too much and you keep losing weight you do not need to lose. Too little and the temperature drifts back up.
Your maintenance dose depends on three variables: the dose that got you to goal, how much metabolic adaptation has occurred, and how strong your lifestyle habits are.
Step-down protocol for finding maintenance dose:
- 1.Stay at your current dose for 4 weeks after reaching goal weight. Your body needs time to stabilize at the new weight. Dropping too early invites a rebound before your metabolism has adjusted.
- 2.Reduce by one dose tier (2.5 mg decrease) every 4 weeks. If you reached goal on 15 mg, step to 12.5 mg. After 4 stable weeks, step to 10 mg. Monitor your weight weekly during each step.
- 3.Hold when you find the floor. The floor is the dose where your weight holds steady (within 2 to 3 pounds) for 8 or more consecutive weeks. For most patients, this lands between 5 and 10 mg.
- 4.Never step below 2.5 mg without physician oversight. The 2.5 mg dose is the lowest manufactured tier. Going lower requires compounded formulations and careful monitoring.
If your weight starts climbing at any step, return to the previous dose immediately. A 3 to 5 pound increase over 2 weeks signals that you have gone below your maintenance threshold. For details on what each dose looks like in syringe units, see the tirzepatide dosage chart in units.
What Most Patients Land On
Clinical practice data and the SURMOUNT trial extensions suggest a pattern. Patients who reached goal on 10 or 15 mg most commonly maintain on 5 to 7.5 mg. Those who reached goal on lower doses (5 or 7.5 mg) sometimes maintain on 2.5 mg, particularly if they have adopted high-protein diets and resistance training.
A minority of patients can eventually discontinue entirely without regaining. These individuals share common traits: they have maintained goal weight for 12 or more months on a stable maintenance dose, they consume 1.2 to 1.6 g of protein per kilogram of body weight daily, they perform resistance training 3 or more times per week, and they sleep 7 or more hours consistently. Even among this group, close monitoring is essential. Weight regain can begin 8 to 12 weeks after complete discontinuation (Wilding et al., NEJM 2022).
Weight Regain Rates: What the Data Shows
The fear of regain is not irrational. It is backed by every long-term discontinuation study published to date. Understanding the numbers helps you make an informed decision about whether maintenance therapy is worth the cost and commitment.
| Timeframe After Stopping | Average Weight Regain | Source |
|---|---|---|
| 3 months | 15-20% of weight lost | SURMOUNT-4 extrapolation |
| 6 months | 30-40% of weight lost | SURMOUNT-4, Aronne et al. 2024 |
| 12 months | 50-67% of weight lost | SURMOUNT-4, STEP 1 extension (semaglutide parallel) |
| 24 months (projected) | 60-80% of weight lost | Longitudinal modeling, Rubino et al. 2021 |
The regain is not linear. Most of it happens in the first 6 months after stopping, then decelerates. By 12 months, patients in SURMOUNT-4 who switched to placebo had regained roughly 14 percentage points of body weight from their lowest point (Aronne et al., JAMA 2024).
For context, the semaglutide discontinuation data tells a similar story. In the STEP 1 extension trial, participants regained two-thirds of their lost weight within 12 months of stopping semaglutide (Wilding et al., Diabetes Obes Metab 2022). The GLP-1 receptor agonist class as a whole appears to require ongoing use for durable weight maintenance. If you are currently on semaglutide and considering a switch, see the semaglutide to tirzepatide conversion guide.
Metabolic adaptation is the core driver. After significant weight loss, your body burns 200 to 300 fewer calories per day than predicted by the new body weight alone. This "metabolic gap" persists for years, possibly permanently (Fothergill et al., Obesity 2016). Tirzepatide bridges that gap pharmacologically. Remove the bridge and the gap reasserts itself.
Lifestyle Factors That Allow Lower Maintenance Doses
Not every patient needs the same maintenance dose. The strongest predictors of successful dose reduction are behavioral, not genetic. These four habits consistently separate patients who maintain on 2.5 to 5 mg from those who need 10 mg or more.
1. Protein intake above 1.2 g per kilogram of body weight daily
Protein is the most satiating macronutrient. At 1.2 to 1.6 g/kg, it preserves lean mass during weight loss, which protects your resting metabolic rate. A 180-pound person maintaining on tirzepatide should aim for 100 to 130 g of protein per day. Each gram of lean mass preserved burns roughly 6 calories per day at rest. Over an entire body's lean mass, this adds up to hundreds of calories of daily metabolic protection (Westerterp-Plantenga et al., Annu Rev Nutr 2009). For more on how tirzepatide affects body composition, see does tirzepatide burn fat.
2. Resistance training 3 or more sessions per week
Resistance training is the only intervention proven to counteract lean mass loss during GLP-1 agonist therapy. Patients who lift weights during weight loss retain 15 to 25% more lean mass than those who do not (Cava et al., Metabolism 2017). This translates to a higher resting metabolic rate and, in practice, the ability to maintain on a lower tirzepatide dose. If tirzepatide causes fatigue that interferes with training, discuss dose timing with your provider.
3. Sleep duration of 7 or more hours per night
Sleep deprivation increases ghrelin by 15% and decreases leptin by 15%, directly opposing the appetite suppression tirzepatide provides (Spiegel et al., Ann Intern Med 2004). Chronically poor sleep can effectively negate 2.5 mg of dose reduction. If you are attempting to lower your maintenance dose, fixing sleep is non-negotiable.
4. Daily step count above 8,000
Non-exercise activity thermogenesis (NEAT) accounts for 15 to 30% of total daily energy expenditure. Walking 8,000 or more steps daily burns an additional 300 to 400 calories compared to a sedentary baseline. This energy buffer gives your maintenance dose more room to work and may allow stepping down by one tier.
When to Increase or Decrease Your Maintenance Dose
Maintenance is not a set-it-and-forget-it number. Life changes, metabolic adaptation shifts, and seasonal patterns all affect your weight trajectory. Here is when to adjust.
Signals to decrease your maintenance dose:
- You are still losing weight unintentionally after 8 weeks at goal
- You experience persistent nausea, constipation, or diarrhea that interferes with daily life
- Your BMI drops below the healthy range (under 18.5)
- You have maintained goal weight for 6 or more months and want to test a lower dose
Signals to increase your maintenance dose:
- Weight has increased by 5 or more pounds over 4 consecutive weeks
- Appetite and cravings have returned to pre-treatment levels
- You have experienced a major life stressor (job change, illness, injury) that disrupts diet and exercise routines
- Seasonal weight gain exceeds your historical pattern by 3 or more pounds
How to adjust:
Move in 2.5 mg increments. One tier at a time, 4 weeks between changes, weekly weigh-ins at the same time each morning. Log everything. If you need help converting your new dose to syringe units at your specific vial concentration, use the Tirzepatide Dosage Calculator. For those on compounded formulations, the how many mg is 20 units of tirzepatide guide walks through exact conversions.
Holiday and travel protocol:
Some patients preemptively increase by one dose tier (e.g., 5 mg to 7.5 mg) during December or vacation periods, then step back down afterward. This requires physician approval but can prevent a 5 to 10 pound rebound that takes months to reverse. Planning ahead costs far less than chasing regain.
Cost Considerations for Long-Term Maintenance
Long-term tirzepatide use means long-term costs. The math changes significantly depending on whether you use brand-name or compounded formulations.
| Formulation | Monthly Cost (Maintenance Dose) | Annual Cost |
|---|---|---|
| Brand Mounjaro/Zepbound (with insurance) | $25-150/month | $300-1,800/year |
| Brand Mounjaro/Zepbound (no insurance) | $1,000-1,200/month | $12,000-14,400/year |
| Compounded tirzepatide (5 mg/week) | $150-300/month | $1,800-3,600/year |
| Compounded tirzepatide (2.5 mg/week) | $100-200/month | $1,200-2,400/year |
Brand-name tirzepatide carries a list price of approximately $1,060 per month for Mounjaro and $1,060 per month for Zepbound (Eli Lilly, 2024). Insurance coverage varies widely. Some plans cover Mounjaro for type 2 diabetes but not Zepbound for weight management. Others require prior authorization and step therapy through semaglutide first.
Compounded tirzepatide is significantly cheaper, typically $150 to $300 per month for a maintenance dose of 5 mg weekly. However, compounding availability depends on FDA enforcement actions and the ongoing regulatory landscape. Verify with your compounding pharmacy that their formulation is current.
The cost-per-pound-maintained equation matters. If you lost 60 pounds on tirzepatide and maintenance therapy costs $200 per month, you are spending $2,400 per year to keep 60 pounds off. The metabolic, cardiovascular, and joint health benefits of maintaining that weight loss carry their own financial value in reduced healthcare costs. Use the Peptide Cost Calculator to estimate your annual expenditure based on your specific dose and source. For more on how long tirzepatide lasts once reconstituted, see our storage guide, as vial management affects total cost per dose.
Tirzepatide Maintenance vs. Semaglutide Maintenance
Some patients consider switching from tirzepatide to semaglutide for maintenance, often because of insurance coverage or cost differences. The two drugs share a GLP-1 mechanism but differ in important ways.
| Factor | Tirzepatide Maintenance | Semaglutide Maintenance |
|---|---|---|
| Mechanism | Dual GIP + GLP-1 agonist | GLP-1 agonist only |
| Average weight loss maintained | 85-95% at 5-10 mg | 70-80% at 1.0-1.7 mg |
| Typical maintenance dose | 5-10 mg weekly | 1.0-1.7 mg weekly |
| GI side effects on maintenance | Lower (dose-related reduction) | Comparable |
| Hair loss risk | Similar to semaglutide | Reported in 3-5% of users |
| Cardiovascular benefit | SELECT-like trial ongoing | Proven 20% MACE reduction (SELECT trial) |
| Cost (compounded) | $150-300/month | $100-250/month |
In head-to-head trials, tirzepatide at 15 mg produced greater weight loss than semaglutide 2.4 mg (22.5% vs. 13.7% at 72 weeks in SURMOUNT-1 vs. STEP 1). The maintenance comparison has not been directly studied, but indirect evidence suggests that patients who switch from tirzepatide to semaglutide for maintenance may experience partial regain due to the loss of the GIP receptor component (Frias et al., NEJM 2021).
If cost is the primary driver for switching, a better strategy is often to reduce the tirzepatide dose rather than switch molecules. A patient on 5 mg tirzepatide weekly pays roughly the same for compounded formulations as someone on 1.7 mg semaglutide, and retains the dual-receptor benefit. For detailed dose equivalencies, see the semaglutide to tirzepatide conversion guide. If you are currently not losing weight on semaglutide, switching to tirzepatide for the combined GIP activation may be worth discussing with your provider.
Common Mistakes When Transitioning to Maintenance
Mistake 1: Dropping from treatment dose to zero overnight.
A patient on 15 mg who stops cold has no pharmacological appetite suppression within 30 days (tirzepatide half-life is approximately 5 days; five half-lives for full clearance). Hunger returns before metabolic adaptation has occurred. In SURMOUNT-4, this produced a 14 percentage point rebound in body weight over 52 weeks (Aronne et al., JAMA 2024). The fix: step down by 2.5 mg every 4 weeks. Never skip tiers.
Mistake 2: Reducing dose and food intake simultaneously.
Some patients lower their tirzepatide dose and also cut calories further, attempting to "pre-empt" any regain. This doubles the metabolic stress. Lean mass loss accelerates, resting metabolic rate drops, and the rebound when appetite normalizes is more severe. Reduce the drug or reduce food. Not both at once.
Mistake 3: Using weight as the only metric.
Scale weight fluctuates by 2 to 5 pounds daily due to water, sodium, glycogen stores, and bowel contents. A patient who sees a 3-pound increase after stepping from 7.5 mg to 5 mg may panic and jump back up unnecessarily. Use a 7-day rolling average instead. If the 7-day average trends upward for 3 or more consecutive weeks, the dose reduction was too aggressive.
Mistake 4: Ignoring side effects during dose reduction.
Some patients experience a temporary increase in GI symptoms when they step down, possibly related to rebound gastric motility changes. Headaches and mild nausea are common during transitions. These typically resolve within 1 to 2 weeks. If they persist beyond 3 weeks, consult your prescriber. Adequate hydration and electrolyte intake minimize transition symptoms. For guidance on how long tirzepatide stays in your system, see our pharmacokinetics guide.
Step-Down Protocol: From Treatment to Maintenance
This protocol assumes you have reached your goal weight and held it stable for at least 4 weeks at your current treatment dose. If you are still losing, stay at your current dose until weight stabilizes.
1. Confirm weight stability. Weigh yourself daily for 4 weeks at your current dose. Calculate a 7-day rolling average. If the rolling average is stable (within 2 pounds), proceed to step 2.
2. Reduce by 2.5 mg. If you are on 15 mg, move to 12.5 mg. If you are on 10 mg, move to 7.5 mg. Continue weekly injections on the same day you have been using.
3. Monitor for 4 weeks. Continue daily weigh-ins and rolling averages. Track appetite, energy, and any GI changes in a simple log. If your rolling average increases by more than 3 pounds over 2 consecutive weeks, return to the previous dose.
4. If stable, reduce by another 2.5 mg. Repeat the 4-week monitoring period at each new dose.
5. Identify your maintenance floor. This is the dose where your weight holds steady for 8 or more weeks and your appetite remains manageable. Do not attempt further reductions once you find it.
6. Continue indefinitely or attempt supervised discontinuation. After 12 or more months of stable maintenance, some patients attempt complete discontinuation under physician supervision with monthly weigh-ins for the first 6 months. If weight begins to climb, restart at your last known maintenance dose.
For patients on compounded tirzepatide who need to convert their new dose into syringe units, the tirzepatide units for 2.5 mg guide covers the lowest dose tier in detail. If you are preparing your own vials, the reconstitution guide walks through safe preparation at any concentration.
Sample step-down timeline (starting from 15 mg):
| Week | Dose | Action |
|---|---|---|
| 1-4 | 15 mg | Hold at goal weight, confirm stability |
| 5-8 | 12.5 mg | First reduction, monitor rolling average |
| 9-12 | 10 mg | Second reduction, monitor |
| 13-16 | 7.5 mg | Third reduction, monitor |
| 17-20 | 5 mg | Fourth reduction, assess maintenance viability |
| 21+ | 5 mg or adjust | Hold if stable; increase if weight trends up |
Most patients reach their maintenance floor at week 13 to 20. The entire step-down takes 4 to 5 months. Do not rush it. For alcohol use during this period, see can you drink on tirzepatide, as alcohol affects both appetite regulation and GI tolerance.
When Complete Discontinuation May Work
Complete discontinuation is rare but possible. The medical literature does not yet provide a reliable biomarker for predicting who can stop successfully. However, clinical observations identify a profile of patients who have the highest probability.
Candidates for supervised discontinuation:
- Maintained goal weight on a stable dose for 12 or more months
- Lost weight primarily through combined medication and lifestyle change (not medication alone)
- Consume 1.2 to 1.6 g protein per kg body weight daily
- Perform resistance training 3 or more times per week
- Sleep 7 or more hours nightly with good sleep architecture
- Have a BMI at goal of 25 or higher (patients who drop into the low-normal range have less metabolic buffer)
- No history of binge eating disorder or significant emotional eating patterns
Even with this profile, the SURMOUNT-4 data suggests that roughly half of patients will regain meaningful weight within 12 months of stopping (Aronne et al., JAMA 2024). Supervised discontinuation means monthly weigh-ins for 6 months, then quarterly for another 12 months. A weight increase of 5 or more pounds on a rolling average triggers a return to the last effective maintenance dose.
Patients with type 2 diabetes face additional considerations. Tirzepatide provides glycemic control independent of its weight effects. Discontinuing may cause HbA1c to rise even if weight remains stable. These patients should work closely with an endocrinologist and never discontinue without ongoing metabolic monitoring.
For patients exploring alternative peptides during maintenance, the peptide safety guide and peptide stacking guide cover interaction risks and evidence-based combinations. Some clinicians explore retatrutide (a triple agonist) as a potential future maintenance option, though it remains in clinical trials. The retatrutide vs. tirzepatide comparison reviews the current evidence.
Frequently Asked Questions
What is the best maintenance dose of tirzepatide after weight loss?
Most patients maintain on 5 to 10 mg weekly after reaching goal weight. The SURMOUNT-4 trial demonstrated durable weight maintenance at the maximum tolerated dose. A step-down protocol, reducing by 2.5 mg every 4 weeks, helps identify the lowest effective dose for each individual. Patients with strong lifestyle habits sometimes maintain on 2.5 mg.
What happens if you stop taking tirzepatide after losing weight?
SURMOUNT-4 data shows patients regain 50 to 67% of lost weight within 12 months of stopping. The regain is driven by hormonal rebound: ghrelin increases, leptin sensitivity drops, and the hypothalamus recalibrates toward the pre-treatment weight set point. Most regain occurs in the first 6 months after discontinuation.
Can you reduce your tirzepatide dose after reaching goal weight?
Yes, and most providers recommend it. The standard approach is reducing by 2.5 mg every 4 weeks while monitoring weight with a 7-day rolling average. If weight increases by more than 3 pounds over 2 consecutive weeks, return to the previous dose. Most patients find their maintenance floor at 5 to 7.5 mg weekly.
How long do you need to stay on tirzepatide for weight maintenance?
Current evidence suggests indefinite use for most patients. SURMOUNT-4 showed continued benefit at 88 weeks with no clear endpoint for stopping. Some patients attempt supervised discontinuation after 12 or more months of stable maintenance, but roughly half regain significant weight within a year of stopping.
Is tirzepatide or semaglutide better for weight maintenance?
No direct head-to-head maintenance trial exists, but indirect evidence favors tirzepatide. Its dual GIP and GLP-1 mechanism maintains more weight loss than GLP-1-only semaglutide. SURMOUNT-1 showed 22.5% total weight loss vs. 13.7% in STEP 1. Maintenance doses are typically 5 to 10 mg tirzepatide vs. 1.0 to 1.7 mg semaglutide weekly.
Does insurance cover tirzepatide for weight maintenance?
Coverage varies widely. Many plans cover Mounjaro for type 2 diabetes maintenance but not Zepbound for weight management beyond an initial period. Prior authorization and step therapy through semaglutide first are common requirements. Without insurance, brand-name tirzepatide costs approximately $1,060 per month. Compounded formulations range from $100 to $300 monthly.
Can exercise replace tirzepatide for weight maintenance?
Exercise alone is unlikely to fully replace tirzepatide for most patients. The metabolic adaptation after major weight loss creates a 200 to 300 calorie daily deficit that exercise cannot reliably close. However, resistance training 3 or more times per week plus 8,000 daily steps can reduce the required maintenance dose by one to two tiers (2.5 to 5 mg less).
How much weight do you regain if you lower your tirzepatide dose?
Regain from dose reduction is smaller than from complete discontinuation. Most patients who step down by 2.5 to 5 mg from their treatment dose experience 0 to 5 pounds of regain that stabilizes within 4 to 6 weeks. If regain exceeds 5 pounds over 4 weeks, the dose reduction was too aggressive, and returning to the previous dose typically reverses the gain.
The Bottom Line
The maintenance dose for tirzepatide after weight loss falls between 5 and 10 mg weekly for most patients. SURMOUNT-4 proved that stopping entirely leads to 50 to 67% weight regain within 12 months. The step-down protocol, reducing by 2.5 mg every 4 weeks with rolling-average monitoring, identifies your personal maintenance floor without risking a rebound.
Lifestyle habits are your strongest allies. Protein above 1.2 g/kg, resistance training, adequate sleep, and daily movement can each reduce your required dose by one tier. Combined, they represent the difference between maintaining on 10 mg and maintaining on 2.5 mg.
Use the Tirzepatide Dosage Calculator to convert your maintenance dose to the correct number of syringe units at your specific vial concentration. For cost planning, the Peptide Cost Calculator estimates your annual maintenance expenditure. If you are considering switching medications, review the semaglutide to tirzepatide conversion guide before making changes.
Related articles: - How Long Does Tirzepatide Take to Work? — expected timelines from first injection to measurable results - Why Am I Not Losing Weight on Tirzepatide? — troubleshooting plateaus and stalls during treatment - How Long Does Semaglutide Take to Work? — comparison timelines if switching between GLP-1 agents - Does Semaglutide Need to Be Refrigerated? — storage rules that apply equally during a maintenance phase - Does Semaglutide Expire? — shelf-life considerations for long-term maintenance supply planning - How Long Does Bacteriostatic Water Last? — storage timelines for reconstituted peptide vials - Tirzepatide Cost With Insurance — long-term cost planning for maintenance phase - How to Inject Tirzepatide — injection technique for ongoing self-administration
Related Articles
Not Losing Weight on Tirzepatide?
Not losing weight on tirzepatide? About 3% of users are non-responders. Learn 8 fixable reasons, SURMOUNT trial data, and a 4-week troubleshooting protocol.
Tirzepatide: How Long to Work?
Tirzepatide reduces appetite within the first week, produces measurable weight loss by week 4, and delivers significant results by weeks 12-16.
Does Tirzepatide Burn Fat?
Tirzepatide produced 33.9% fat mass loss in SURMOUNT-1. Learn how GLP-1/GIP dual agonism drives fat loss, body composition data, and how to protect lean mass.
Microdosing Tirzepatide Explained
Microdosing tirzepatide means using 0.5-2.5 mg weekly instead of 5-15 mg. Protocols, clinical evidence, and side effect management.