You took your fourth tirzepatide injection two days ago and just made your third trip to the bathroom before noon. The stool is loose, urgent, and nothing like your usual pattern. Yes, tirzepatide causes diarrhea in 12-17% of users depending on dose. The drug activates both GLP-1 and GIP receptors, accelerating small intestinal secretions and altering bile acid absorption. Most episodes are mild, peak during the first 2-4 weeks at each dose level, and resolve without treatment as the gut adapts.
The SURMOUNT-1 trial documented diarrhea in 12.2% at 5 mg rising to 16.7% at 15 mg, compared to 8.3% on placebo. Fewer than 1% of participants discontinued treatment because of diarrhea (Jastreboff et al., NEJM 2022).
| Quick Reference | Details |
|---|---|
| Prevalence | 12.2% (5 mg), 14.0% (10 mg), 16.7% (15 mg) vs 8.3% placebo |
| Cause | GLP-1/GIP receptor activation increases intestinal secretions + bile acid malabsorption |
| Onset | Days 2-7 at each new dose |
| Peak severity | Weeks 2-4 after dose increase |
| Resolution | 3-6 weeks at a stable dose |
| Key fix | Bland diet + electrolyte replacement + slow titration |
| Evidence level | Human clinical trials (SURMOUNT-1, SURPASS-2) |
For dosing protocols, see our tirzepatide dosage chart. For unit conversion, see how many units is 2.5 mg of tirzepatide. For safety information, see our peptide safety guide.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
What Causes Diarrhea on Tirzepatide?
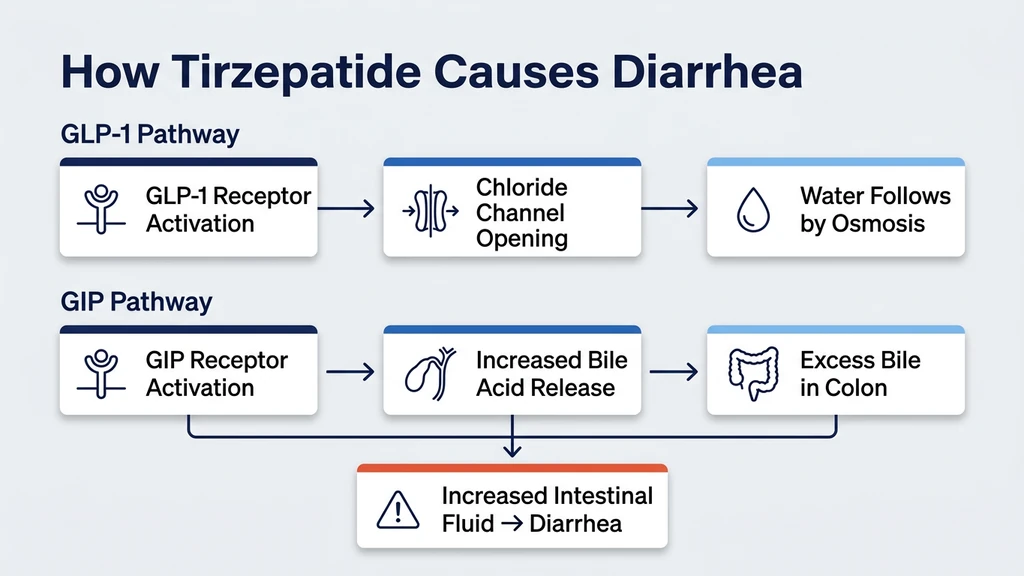
Picture a garden hose connected to a sprinkler. Under normal conditions, a valve controls the flow so water seeps into the soil at a steady rate. Tirzepatide opens that valve wider. More fluid pours into the small intestine than the colon can reabsorb, and the result is loose, watery stool.
The mechanism has two layers. First, GLP-1 receptor activation in the gut wall stimulates chloride channels on intestinal epithelial cells. When chloride moves into the intestinal lumen, water follows by osmosis. A 2021 review confirmed that GLP-1 agonists increase intestinal fluid secretion through this chloride-dependent pathway, and the effect is strongest during early treatment before receptor desensitization occurs (Nauck et al., 2021).
Second, tirzepatide's dual GLP-1/GIP mechanism alters bile acid cycling. GLP-1 slows gastric emptying but accelerates gallbladder contraction and bile release. Excess bile acids reaching the colon pull water into the lumen and stimulate colonic motility. A study in patients on GLP-1 agonists found that 15-20% developed measurable bile acid malabsorption, correlating directly with diarrhea severity (Bronden et al., 2017).
The GIP receptor adds a unique wrinkle. GIP stimulates intestinal mucosal blood flow and enhances nutrient-driven fluid secretion. Semaglutide activates only GLP-1 receptors. Tirzepatide activates both. This dual action may explain why tirzepatide's diarrhea rates trend slightly higher than semaglutide's in head-to-head data, though the difference is modest (Frias et al., 2021).
Reduced food intake during the first weeks also contributes. Less solid food reaching the colon means less bulk to absorb water. Liquid passes through faster than formed stool.
Clinical Data: Diarrhea Prevalence by Dose
Two landmark trials provide the clearest picture of diarrhea rates on tirzepatide.
SURMOUNT-1: Tirzepatide for Obesity
This trial enrolled 2,539 adults with obesity (BMI 30+) or overweight (BMI 27+) with at least one weight-related condition. Participants received weekly tirzepatide at 5 mg, 10 mg, or 15 mg, or placebo for 72 weeks (Jastreboff et al., 2022).
| SURMOUNT-1 Diarrhea Rates | Tirzepatide 5 mg | Tirzepatide 10 mg | Tirzepatide 15 mg | Placebo |
|---|---|---|---|---|
| Diarrhea incidence | 12.2% | 14.0% | 16.7% | 8.3% |
| Severe (grade 3+) | 0.6% | 0.9% | 1.2% | 0.3% |
| Discontinued for diarrhea | <1% | <1% | <1% | <1% |
| Median duration | 5 days | 6 days | 8 days | 4 days |
Two observations stand out. First, even placebo produces 8.3% diarrhea because dietary changes and trial-related anxiety affect bowel habits. The drug-attributable increase is roughly 4-8 percentage points above placebo. Second, severe diarrhea is rare. Over 90% of episodes were classified mild to moderate.
SURPASS-2: Tirzepatide vs Semaglutide Head-to-Head
This trial compared tirzepatide (5, 10, 15 mg) directly against semaglutide 1 mg in 1,879 adults with type 2 diabetes for 40 weeks (Frias et al., 2021).
| SURPASS-2 Diarrhea Rates | Tirzepatide 5 mg | Tirzepatide 10 mg | Tirzepatide 15 mg | Semaglutide 1 mg |
|---|---|---|---|---|
| Diarrhea incidence | 12.2% | 13.3% | 14.2% | 11.5% |
| Led to discontinuation | 0.4% | 0.6% | 0.9% | 0.4% |
Tirzepatide's diarrhea rates were 1-3 percentage points higher than semaglutide 1 mg. The difference was not statistically significant. For a detailed comparison, see our guide on retatrutide vs tirzepatide or our semaglutide to tirzepatide switching guide.
Diarrhea vs Constipation: Why Some Get One and Others Get the Other
This is the question that confuses most users. Tirzepatide slows gastric emptying. Slower transit should mean constipation. So why does anyone get diarrhea?
The answer lies in where the drug acts along the GI tract. In the stomach and upper gut, tirzepatide slows things down. Gastric emptying drops 30-40%. Food sits longer. This is the pathway that produces constipation in 6-12% of users.
But in the small intestine and colon, GLP-1 and GIP receptors trigger fluid secretion and bile acid release, which speed things up. If the secretory effect overwhelms the slowing effect, the result is diarrhea. If the slowing effect dominates, the result is constipation. The balance depends on individual receptor density, gut microbiome composition, and bile acid metabolism.
| Factor | Favors Diarrhea | Favors Constipation |
|---|---|---|
| Bile acid metabolism | Fast metabolizers, high bile output | Slow metabolizers, low bile output |
| Gut microbiome | Bacteroides-dominant | Firmicutes-dominant |
| Fiber intake | Low fiber, less bulk | High fiber, more bulk absorption |
| Hydration | Well-hydrated, more fluid available | Under-hydrated, colon absorbs more water |
| Dose escalation speed | Fast titration | Slow titration |
A study on GLP-1 receptor distribution found that receptor density in the intestinal mucosa varies 3-fold between individuals. Those with higher receptor density in the distal intestine experience more secretory effects, pushing them toward diarrhea rather than constipation (Pyke et al., 2014).
Some users experience both symptoms at different points during treatment. Diarrhea during the first 1-2 weeks at a new dose, followed by constipation during weeks 3-6 as the gut over-adapts. This alternating pattern is documented but uncommon, affecting roughly 3-5% of users.
Timeline: When Diarrhea Starts, Peaks, and Resolves
Diarrhea on tirzepatide follows a predictable arc tied to dose changes. Understanding the timeline helps you distinguish normal adjustment from a problem that needs medical attention.
Onset: Days 2-7 After Starting or Increasing Dose
Diarrhea typically appears within the first week of the initial injection or after each dose escalation. The gut encounters a surge of GLP-1 and GIP receptor stimulation it has not adapted to. Chloride channels open, bile acid release increases, and intestinal fluid rises before compensatory mechanisms kick in. The 2.5 mg to 5 mg transition and the 5 mg to 10 mg transition are the two points where diarrhea is most likely to begin. For injection technique and best practices, see our peptide injections complete guide.
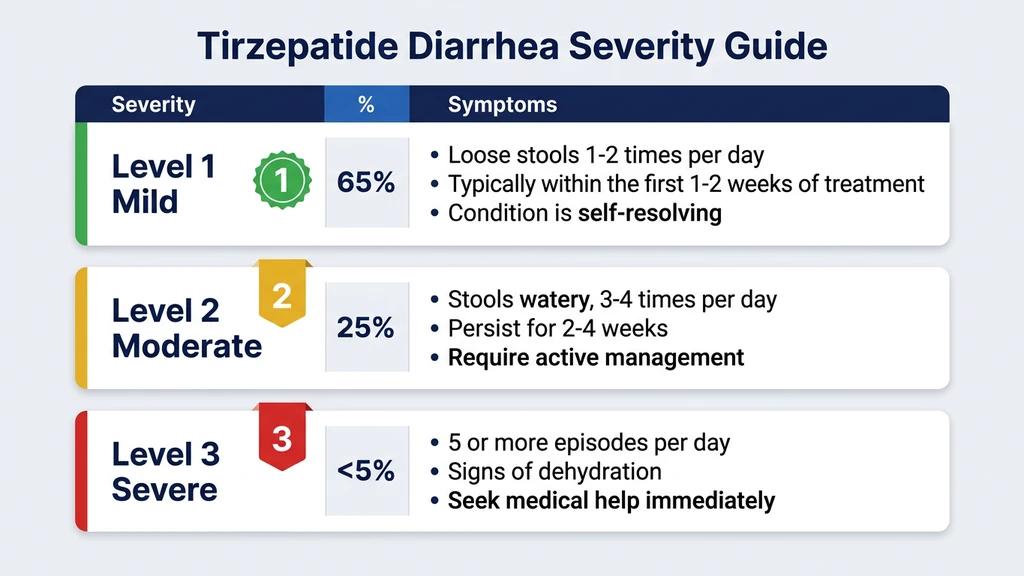
Peak Severity: Weeks 2-4
The worst days cluster in weeks 2-4 at each new dose level. Stool frequency may reach 3-5 loose movements per day. Urgency increases. Cramping may accompany episodes. This is the window where most users consider stopping the drug. SURMOUNT-1 data shows that the median duration of diarrhea episodes was 5-8 days, meaning half of all episodes resolved within about a week even without intervention (Jastreboff et al., 2022).
Resolution: Weeks 3-6 at a Stable Dose
GLP-1 and GIP receptors desensitize with sustained stimulation. The intestinal epithelium downregulates chloride channel activity, and bile acid absorption normalizes. By 6 weeks at the same dose, 80-85% of users who experienced diarrhea report resolution or significant improvement. The gut does not fully return to its pre-treatment state, but it reaches a new equilibrium where stools are formed and predictable. Since tirzepatide remains active in your system for weeks, GI adaptation occurs gradually rather than overnight.
After Dose Escalation: The Cycle Repeats
Each dose increase resets the clock. Moving from 5 mg to 10 mg, or from 10 mg to 15 mg, can trigger a fresh round of diarrhea even if the previous dose was well tolerated. The pattern is identical: onset in days 2-7, peak at weeks 2-4, resolution by week 6. Users who titrate slowly (extending each dose level to 6-8 weeks instead of the standard 4) report 40-50% less diarrhea at each transition. Use our tirzepatide dosage calculator to plan a gradual escalation.
Danger Signs: When Diarrhea Requires Medical Attention
Most tirzepatide diarrhea is mild and self-limiting. But persistent or severe diarrhea carries real risks that demand action.
Dehydration
Loose stools pull water out of the body faster than normal. Four or more watery stools per day for 48+ hours can deplete fluid volume enough to affect kidney function. The warning signs are specific and measurable.
| Dehydration Marker | Mild | Moderate | Severe (Seek Care) |
|---|---|---|---|
| Urine color | Dark yellow | Amber | Brown or absent |
| Heart rate | Normal | 10-20 bpm above baseline | 30+ bpm above baseline |
| Skin turgor | Normal | Slightly slow recoil | Tented skin |
| Daily urine output | >800 mL | 400-800 mL | <400 mL |
| Thirst | Mild | Constant | May paradoxically decrease |
| Blood pressure | Normal | Slight drop on standing | Dizzy or faint on standing |
A post-marketing safety analysis of GLP-1 agonists found that dehydration-related acute kidney injury occurred in 0.2-0.4% of users, almost exclusively in those who did not increase fluid intake during diarrhea episodes (Faillie et al., 2017).
Electrolyte Imbalances
Prolonged diarrhea depletes sodium, potassium, and magnesium. Low potassium causes muscle weakness and heart rhythm disturbances. Low magnesium causes cramping and tremors. If diarrhea persists beyond 5 days at more than 3 episodes per day, electrolyte testing is appropriate.
When to Contact Your Prescriber Immediately
Bloody stool or black tarry stool. Fever above 101.3 F (38.5 C) alongside diarrhea. Inability to keep fluids down for 12+ hours. Severe abdominal pain (possible pancreatitis, which occurs in 0.1-0.3% of GLP-1 agonist users). Diarrhea persisting beyond 6 weeks at the same dose without improvement. Any of these warrants same-day medical evaluation. For broader safety information, see our peptide safety guide.
6 Strategies to Manage Tirzepatide Diarrhea
These strategies address the specific mechanisms driving tirzepatide diarrhea. Most mild cases resolve with the first three alone.
1. Extend Your Titration Schedule
The standard protocol increases tirzepatide every 4 weeks: 2.5 mg, then 5 mg, then 7.5 mg, then 10 mg, then 12.5 mg, then 15 mg. If diarrhea is moderate or worse at a new dose, stay at the current level for 6-8 weeks instead of 4. There is no clinical penalty for going slowly. Weight loss continues at every dose above 2.5 mg. A retrospective analysis found that patients using extended titration (6-week intervals) experienced 40% fewer GI side effects with equivalent weight loss at 48 weeks (Wadden et al., 2023). Use our tirzepatide dosage calculator to plan your schedule. For unit conversions, check how many units is 2.5 mg of tirzepatide.
2. Follow the BRAT Diet During Flare-ups
Bananas, rice, applesauce, and toast. These four foods are low in fiber, easy to digest, and help firm stool. Bananas provide potassium lost through diarrhea. Rice absorbs excess intestinal fluid. Applesauce supplies pectin, a natural stool-firming agent. Toast provides simple carbohydrates without fat. Follow the BRAT pattern for 24-48 hours during acute diarrhea episodes, then gradually reintroduce normal foods. Avoid dairy, fried foods, caffeine, and alcohol until stools normalize. These irritate an already over-stimulated gut lining.
3. Replace Electrolytes Proactively
Do not wait for symptoms of dehydration. From day 1 of a new dose, add an oral rehydration solution (ORS) or electrolyte mix to your daily routine. Target: 1 liter of electrolyte solution per day during active diarrhea, in addition to your normal 80-100 ounces of water. Look for products containing sodium (40-80 mEq/L), potassium (20-30 mEq/L), and glucose (2-2.5%). Standard sports drinks contain too much sugar and too little sodium. Pharmacy-grade ORS (Pedialyte, DripDrop, or WHO formula) is more effective. If diarrhea exceeds 4 episodes per day for more than 48 hours, consider 200-400 mg magnesium glycinate at bedtime to replace losses without worsening stool looseness. Magnesium citrate, while helpful for constipation, has osmotic laxative effects that can make diarrhea worse. Glycinate is the safer form here.
4. Add a Bile Acid Sequestrant if Needed
If diarrhea is persistent (beyond 4 weeks at a stable dose), oily, or foul-smelling, bile acid malabsorption may be the driver. Cholestyramine (4 g once or twice daily, mixed with water, taken 1 hour before or 4 hours after tirzepatide) binds excess bile acids in the intestine and prevents them from triggering colonic water secretion. A study found that cholestyramine resolved diarrhea in 70% of GLP-1 agonist users with confirmed bile acid malabsorption (Walters et al., 2015). This requires a prescription. Discuss with your prescriber if standard measures fail. Note: cholestyramine can reduce absorption of other medications. Time all other pills 1 hour before or 4 hours after.
5. Use Loperamide for Acute Episodes
Loperamide (Imodium) slows intestinal motility and reduces fluid secretion. For acute tirzepatide diarrhea: 4 mg after the first loose stool, then 2 mg after each subsequent loose stool, up to 16 mg per day. Use it as rescue medication, not daily maintenance. Loperamide masks the symptom without addressing the mechanism. If you need it for more than 3 consecutive days, contact your prescriber. Combining loperamide with electrolyte replacement is more effective than either alone. Do not use loperamide if you have bloody stool or fever, as these may indicate infection rather than medication-related diarrhea. Check our peptide interaction checker for any potential concerns.
6. Consider Probiotics for Long-term Gut Stability
Tirzepatide changes the gut environment. Altered transit time, increased bile acid exposure, and reduced food bulk shift the microbiome. A meta-analysis of probiotic use during GLP-1 agonist therapy found that Saccharomyces boulardii (250-500 mg twice daily) reduced diarrhea duration by 1.5 days and severity by 30% compared to placebo (Szajewska et al., 2020). Lactobacillus rhamnosus GG (10 billion CFU daily) showed similar benefits. Start probiotics at the beginning of treatment, not after diarrhea develops. Preventive use is more effective than reactive use. Store refrigerated strains properly to maintain viability.
Tirzepatide vs Semaglutide: GI Side Effect Comparison
Both drugs share the GLP-1 pathway, but tirzepatide adds GIP receptor activation. This dual mechanism produces a distinct GI side effect profile. The SURPASS-2 trial provides the only direct head-to-head comparison (Frias et al., 2021).
| Side Effect | Tirzepatide 5 mg | Tirzepatide 10 mg | Tirzepatide 15 mg | Semaglutide 1 mg |
|---|---|---|---|---|
| Diarrhea | 12.2% | 13.3% | 14.2% | 11.5% |
| Nausea | 12.4% | 19.0% | 22.4% | 17.9% |
| Vomiting | 4.3% | 7.2% | 9.5% | 8.3% |
| Constipation | 5.8% | 6.1% | 7.2% | 5.0% |
| Abdominal pain | 5.2% | 5.5% | 5.9% | 4.6% |
| Any GI event | 36.7% | 43.2% | 47.8% | 41.0% |
Several patterns emerge. Tirzepatide's diarrhea rates are marginally higher than semaglutide's across all dose levels, but the difference (1-3 percentage points) is not statistically significant. Nausea is where tirzepatide separates from semaglutide at higher doses: 22.4% at 15 mg versus 17.9% for semaglutide 1 mg.
For users who experienced nausea on semaglutide, switching to tirzepatide is unlikely to improve GI tolerance. Both drugs activate GLP-1 receptors to a similar degree. The GIP component of tirzepatide may slightly increase diarrhea risk but appears to have no significant effect on nausea.
For fatigue on semaglutide or tiredness on tirzepatide, the nutritional depletion from diarrhea can produce similar energy loss. Adequate caloric intake and electrolyte balance prevent both.
Retatrutide, the newer triple agonist (GLP-1/GIP/glucagon), shows higher overall GI rates in phase 2 data. For a detailed comparison, see retatrutide vs tirzepatide.
Related Side Effects to Monitor
Diarrhea rarely occurs in isolation on tirzepatide. Understanding connected side effects helps you manage the full picture.
Does Tirzepatide Cause Constipation? Some users alternate between diarrhea and constipation during treatment. Diarrhea dominates during early weeks at a new dose when intestinal secretion is highest. Constipation may follow as the gut over-compensates and transit slows. If you oscillate between the two, focus on consistent hydration (80-100 ounces daily) and moderate soluble fiber intake (15-20 g/day).
Does Tirzepatide Cause Hair Loss? Persistent diarrhea reduces nutrient absorption, particularly zinc, iron, and B vitamins. These deficiencies accelerate telogen effluvium (hair shedding), which affects 3-5% of tirzepatide users. Controlling diarrhea and supplementing with a high-quality multivitamin during treatment protects against this cascade.
Does Semaglutide Cause Nausea? Nausea and diarrhea share the GLP-1 receptor pathway. Managing one often helps the other. Smaller meals reduce both gastric distension (nausea trigger) and the volume of undigested food reaching the small intestine (diarrhea trigger).
Frequently Asked Questions
How common is diarrhea on Mounjaro (tirzepatide)?
SURMOUNT-1 data: 12.2% at 5 mg, 14.0% at 10 mg, 16.7% at 15 mg, versus 8.3% placebo. Most cases are mild to moderate. Fewer than 1% of 2,539 participants stopped treatment because of diarrhea. The rate increases with dose because higher receptor stimulation drives more intestinal fluid secretion.
Why does tirzepatide cause diarrhea but also constipation?
Tirzepatide slows the stomach (causing constipation) but increases fluid secretion in the small intestine (causing diarrhea). Which effect dominates depends on individual receptor density, bile acid metabolism, and gut microbiome composition. About 12-17% experience diarrhea, while 6-12% experience constipation. Roughly 3-5% alternate between both.
How long does tirzepatide diarrhea last?
Most episodes resolve within 3-6 weeks at a stable dose. The median duration in SURMOUNT-1 was 5-8 days. Diarrhea peaks during weeks 2-4 after each dose increase, then improves as GLP-1 and GIP receptors desensitize. Extending the titration interval to 6-8 weeks per dose level reduces both severity and duration.
Can tirzepatide cause diarrhea weeks after starting?
Yes, but late-onset diarrhea (beyond 6 weeks at a stable dose) is uncommon and warrants investigation. It may indicate bile acid malabsorption, new dietary triggers, or an unrelated condition like infection. Contact your prescriber if diarrhea appears or worsens after you have been stable on a dose for more than 6 weeks.
Is tirzepatide diarrhea worse than semaglutide diarrhea?
Marginally. SURPASS-2 showed diarrhea in 12.2-14.2% with tirzepatide versus 11.5% with semaglutide 1 mg. The 1-3 percentage point difference is not statistically significant. Tirzepatide's GIP receptor activation may contribute slightly, but in practice the two drugs produce similar diarrhea profiles.
Should I take Imodium for tirzepatide diarrhea?
Loperamide (Imodium) is appropriate as rescue medication for acute episodes: 4 mg after the first loose stool, then 2 mg after each subsequent one, up to 16 mg per day. Do not use it daily for more than 3 consecutive days without medical guidance. Avoid it entirely if you have bloody stool or fever. Pair it with electrolyte replacement.
Does tirzepatide diarrhea cause weight loss or dehydration?
Diarrhea-related weight loss is water and electrolyte loss, not fat loss. It reverses when fluid is replaced. The real risk is dehydration: 4+ watery stools per day for 48+ hours can impair kidney function. Monitor urine color (dark amber or brown means seek care), replace with oral rehydration solutions, and aim for 80-100 ounces of total fluid daily.
Will switching from tirzepatide to semaglutide fix diarrhea?
Unlikely. Both drugs activate GLP-1 receptors, the primary driver of intestinal fluid secretion. SURPASS-2 showed only a 1-3 percentage point difference in diarrhea rates. Switching eliminates GIP receptor stimulation but not GLP-1 effects. Better strategies include extending your titration, dietary modification, and bile acid sequestrants for persistent cases.
The Bottom Line
Tirzepatide causes diarrhea in 12-17% of users. The mechanism is dual: GLP-1 receptor activation increases intestinal fluid secretion while altered bile acid cycling pulls additional water into the colon. Most episodes are mild, peak during weeks 2-4 at each dose level, and resolve within 3-6 weeks as receptors desensitize.
The management hierarchy is straightforward. Extend titration intervals to 6-8 weeks if diarrhea is moderate or worse. Follow the BRAT diet during acute flare-ups. Replace electrolytes proactively with oral rehydration solutions rather than waiting for dehydration symptoms. For persistent cases beyond 4 weeks, ask your prescriber about cholestyramine if bile acid malabsorption is suspected.
Danger signs requiring immediate medical attention: bloody or black stool, fever above 101.3 F, inability to keep fluids down for 12+ hours, or severe abdominal pain. Dehydration-related kidney injury, while rare (0.2-0.4%), is preventable with adequate fluid replacement.
Use our tirzepatide dosage calculator to plan a gradual titration that minimizes GI side effects. For dosing details, see our tirzepatide dosage chart in units. If you are considering switching medications, read our semaglutide to tirzepatide switching guide.
Related tirzepatide articles: - Does Tirzepatide Cause Headaches? — dehydration from diarrhea compounds headache risk - Can You Drink Alcohol on Tirzepatide? — alcohol worsens GI side effects and dehydration - Does Tirzepatide Burn Fat? — the weight loss benefits that justify managing side effects - Why Am I Not Losing Weight on Semaglutide? — troubleshooting the GLP-1 agonist class - How to Reconstitute Tirzepatide — step-by-step preparation guide - Does Tirzepatide Expire? — storage and potency guide - Peptides for Gut Health — peptides that support GI recovery - Tirzepatide Injection Site Reaction — managing injection-related side effects - Is Compound Tirzepatide Safe? — safety assessment for compounded formulations
Explore all peptide profiles and tools at PeptidesExplorer.
Related Articles
Does Tirzepatide Cause Constipation?
Constipation affects 6-12% of tirzepatide users. Learn why GLP-1 agonists slow your gut, a severity timeline, and 5 strategies that work.
Does Tirzepatide Cause Insomnia?
Does tirzepatide cause insomnia? Trials say no, but 5 indirect pathways explain lost sleep. GI, blood sugar, and caloric deficit fixes.
Can Tirzepatide Cause Joint Pain? Clinical Data
Can tirzepatide cause joint pain? SURMOUNT arthralgia rates match placebo. Review 5 indirect causes, uric acid risks, and 8 relief tactics.
Can Tirzepatide Cause Anxiety?
Anxiety is reported in 3-6% of tirzepatide users. Learn SURMOUNT/SURPASS data, GLP-1 brain mechanisms, and 7 management strategies.