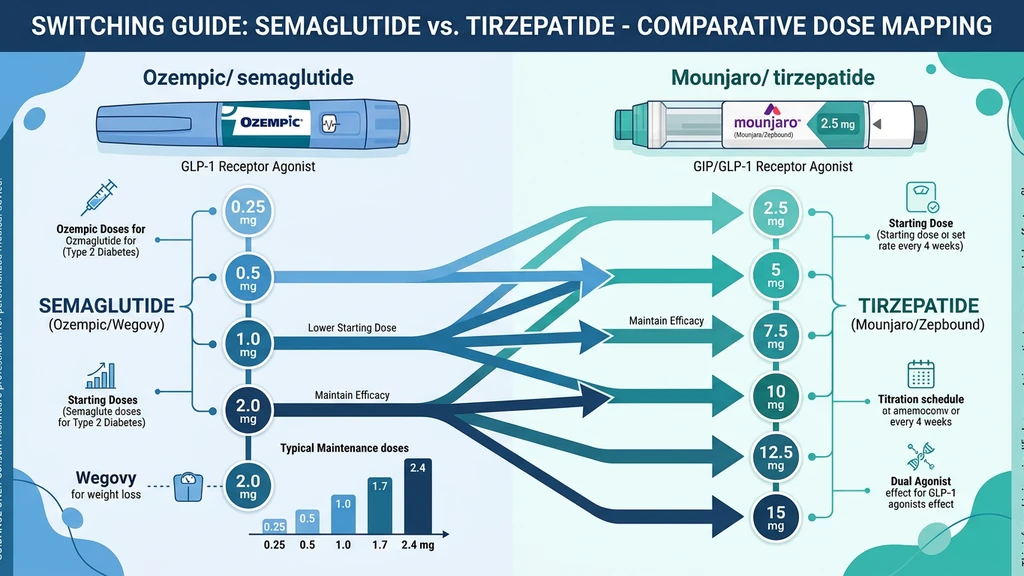
You are sitting in your provider's office. They just told you to switch from semaglutide to tirzepatide. Your first question: what tirzepatide dose equals your current semaglutide dose? No FDA-approved equivalence exists. In clinical practice, 1 mg semaglutide maps to approximately 5 mg tirzepatide, and 2.4 mg semaglutide maps to 10 to 15 mg tirzepatide.
The table below reflects clinical practice patterns, not a head-to-head conversion trial.
| Your Semaglutide Dose | Suggested Tirzepatide Starting Dose | Clinical Rationale |
|---|---|---|
| 0.25 mg | 2.5 mg | Both are the lowest titration step |
| 0.5 mg | 2.5 mg | Tirzepatide 2.5 mg provides comparable GLP-1 activity |
| 1.0 mg | 5 mg | Mid-range GLP-1 equivalence based on clinical weight loss data |
| 1.7 mg | 7.5 to 10 mg | Upper-mid range; 7.5 mg is conservative, 10 mg is aggressive |
| 2.4 mg | 10 to 15 mg | Maximum semaglutide maps to upper tirzepatide range |
These are approximate equivalences from clinical practice, not pharmacokinetic conversions. Your provider may adjust based on your tolerability and treatment response. For a broader comparison of peptide weight loss options including retatrutide, see best peptides for weight loss or the head-to-head retatrutide vs tirzepatide breakdown.
Use the Semaglutide Dosage Calculator or Tirzepatide Dosage Calculator to convert your new dose into syringe units for your specific vial concentration.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
Dose Equivalence Table: Semaglutide to Tirzepatide
No head-to-head trial has established a formal dose equivalence between semaglutide and tirzepatide. The conversions below come from clinical practice patterns, published weight loss data, and receptor binding pharmacology. Every major obesity medicine conference in 2024 and 2025 featured panels discussing these approximations.
| Semaglutide Dose | Tirzepatide Equivalent Range | Confidence Level | Notes |
|---|---|---|---|
| 0.25 mg (initiation) | 2.5 mg | High | Both are starting doses; direct mapping |
| 0.5 mg | 2.5 mg | High | Tirzepatide 2.5 mg covers this GLP-1 level |
| 1.0 mg (Ozempic maintenance) | 5 mg | Moderate | Based on SURPASS vs. STEP trial weight loss comparisons |
| 1.7 mg (Wegovy mid-tier) | 7.5 to 10 mg | Moderate | Provider preference determines whether to start at 7.5 or 10 |
| 2.4 mg (Wegovy maximum) | 10 to 15 mg | Low | Wide range; most providers start at 10 mg and titrate |
The confidence column matters. At low semaglutide doses, the mapping is straightforward because both drugs share a starting dose philosophy. At 2.4 mg semaglutide, the mapping widens because tirzepatide adds GIP receptor agonism on top of GLP-1, producing additional weight loss through a mechanism semaglutide does not have (Frias et al., N Engl J Med, 2021).
Most providers default to the conservative end of the range. Starting lower and titrating up is safer than jumping to an aggressive dose and triggering GI side effects like nausea that force a dose reduction.
Why Doses Are Not 1:1
Think of two radio stations broadcasting from the same tower. One station transmits on a single frequency (FM 101.1). The other broadcasts on two frequencies simultaneously (FM 101.1 and AM 680). Both reach your car, but the dual-frequency station carries more total signal even if each individual frequency is weaker.
Semaglutide is the single-frequency station. It activates one receptor: GLP-1. Tirzepatide is the dual-frequency station. It activates two receptors: GLP-1 and GIP. The GIP signal adds appetite suppression, improved insulin sensitivity, and enhanced fat oxidation that the GLP-1 signal alone does not provide (Willard et al., Mol Metab, 2020).
This is why 5 mg of tirzepatide produces roughly similar weight loss to 1.0 mg of semaglutide, even though the milligram numbers are five times apart. The extra receptor channel means tirzepatide can achieve equivalent clinical effect at a different dose scale.
For another comparison of dual versus triple receptor agonists, see our retatrutide vs tirzepatide guide. A milligram-to-milligram swap ignores this completely. The two drugs have different molecular weights (4,113.58 Da for semaglutide vs. 4,813.45 Da for tirzepatide), different receptor binding profiles, and different half-lives (approximately 7 days for both, but with distinct absorption kinetics). A direct numerical conversion would be like assuming 1 liter of diesel equals 1 liter of gasoline because they are both fuel.
Switching from Semaglutide to Tirzepatide: Step-by-Step Protocol
Step 1: Identify your current stable semaglutide dose. This is the dose you have been taking for at least 4 weeks without intolerable side effects. If you are still titrating up on semaglutide, finish the titration first. Switching during titration makes it impossible to isolate which drug caused which side effect.
Step 2: Find your tirzepatide starting dose in the equivalence table. If your semaglutide dose maps to a range (like 7.5 to 10 mg), start at the lower end. You can always titrate up. You cannot un-inject an overdose.
Step 3: Time the switch correctly. Both drugs are weekly injections. Take your last semaglutide dose on your normal schedule. Wait one full week. Start tirzepatide on the day your next semaglutide dose would have been due. Do not overlap the two medications. Semaglutide stays in your system for several weeks with a half-life of approximately 7 days (Ozempic prescribing information, Novo Nordisk, 2023), so residual drug will still be active during the transition week. For proper storage during the transition, see How to Store Peptides.
Step 4: Prepare for a GI adjustment period. Even at the "equivalent" dose, switching drugs resets your body's adaptation. Expect 1 to 2 weeks of mild nausea, reduced appetite, and possible loose stools or constipation. This is normal. It does not mean the dose is too high.
Step 5: Hold the starting dose for 4 weeks minimum. Do not titrate up during the first month. Your body needs time to adjust to the new receptor profile. The GIP activation is entirely new if you are coming from semaglutide, and your gut needs to calibrate.
Confirm your syringe units for the new medication using the Tirzepatide Dosage Calculator. The unit conversion is different from semaglutide because vial concentrations differ between the two drugs.
Switching from Tirzepatide to Semaglutide
The reverse switch (tirzepatide to semaglutide) follows the same logic but with an important caution: you are removing the GIP signal. Your body has been receiving dual-receptor stimulation. Dropping to single-receptor stimulation may reduce appetite suppression and glycemic control temporarily.
| Your Tirzepatide Dose | Suggested Semaglutide Starting Dose | Notes |
|---|---|---|
| 2.5 mg | 0.25 to 0.5 mg | Start at 0.5 mg if well-tolerated on tirzepatide |
| 5 mg | 1.0 mg | Direct mid-range mapping |
| 7.5 mg | 1.0 to 1.7 mg | 1.0 mg is conservative; 1.7 mg if tolerability is confirmed |
| 10 mg | 1.7 mg | Upper-mid equivalence |
| 15 mg | 2.4 mg | Maximum doses of both drugs |
Timing protocol: Take your last tirzepatide dose on schedule. Wait one full week. Start semaglutide on day 8. Hold the starting dose for at least 4 weeks before considering titration.
Some patients experience a temporary weight loss plateau or slight regain during the switch. This typically resolves within 4 to 6 weeks as the body adjusts to the single-receptor mechanism. Increasing semaglutide prematurely to compensate often causes GI side effects that set you back further.
Use the Semaglutide Dosage Calculator to convert your new milligram dose into syringe units for your specific vial concentration.
Titration Schedule After Switching
Your titration restarts when you switch medications. Even if you were at 2.4 mg semaglutide for six months, your body has never encountered tirzepatide before. The GIP receptor activation is a new variable.
Tirzepatide titration after switching from semaglutide:
| Week | Dose | Action |
|---|---|---|
| Weeks 1 to 4 | Your mapped starting dose | Hold. Assess tolerability. |
| Week 5 | Increase by one tier if tolerated | 2.5 to 5 mg, or 5 to 7.5 mg |
| Weeks 5 to 8 | Hold new dose | Assess tolerability again |
| Week 9+ | Continue titration by one tier every 4 weeks | Until target dose reached |
Semaglutide titration after switching from tirzepatide:
| Week | Dose | Action |
|---|---|---|
| Weeks 1 to 4 | Your mapped starting dose | Hold. Assess tolerability. |
| Week 5 | Increase by one tier if tolerated | 0.25 to 0.5 mg, or 0.5 to 1.0 mg |
| Weeks 5 to 8 | Hold new dose | Assess tolerability again |
| Week 9+ | Continue standard titration every 4 weeks | Until target dose reached |
The standard tirzepatide tiers are: 2.5, 5, 7.5, 10, 12.5, and 15 mg. The standard semaglutide tiers are: 0.25, 0.5, 1.0, 1.7, and 2.4 mg. Never skip a tier. Each step increase is a 50 to 100% jump in drug exposure, and skipping amplifies GI side effects disproportionately.
Two signals that your starting dose is too high: vomiting more than once per week, or inability to drink enough fluids to stay hydrated. If either occurs, drop to the next lower tier and hold for 4 weeks before trying to increase again. For a timeline of when side effects typically resolve, see how long do semaglutide side effects last.
Quantified Danger: Switching Without Dose Adjustment
These scenarios use real dose numbers to show what goes wrong when patients switch medications without proper conversion.
Scenario 1: Matching milligrams instead of using the equivalence table.
You are taking 2.4 mg semaglutide weekly. You switch to tirzepatide and tell your provider you want to start "around 2.5 mg because it is close to 2.4." Your provider agrees. Tirzepatide 2.5 mg is the lowest starting dose, designed for drug-naive patients. At your level of GLP-1 tolerance (built over months at 2.4 mg semaglutide), 2.5 mg tirzepatide provides roughly 75% less receptor activation than you are accustomed to. Within 2 to 3 weeks, appetite suppression fades. Over the next 4 to 8 weeks, you regain 3 to 5 kg before titrating up to an effective dose. The clinical practice mapping for 2.4 mg semaglutide is 10 to 15 mg tirzepatide, not 2.5.
The fix: use the equivalence table. For 2.4 mg semaglutide, start tirzepatide at 10 mg (conservative) or up to 15 mg (aggressive, with provider guidance). Never match by milligram number alone.
Scenario 2: Jumping to maximum tirzepatide without titration history.
You are taking 1.0 mg semaglutide (Ozempic standard maintenance dose). A friend says tirzepatide works better, so you ask your provider for 15 mg tirzepatide because "you want the strongest dose." The equivalence for 1.0 mg semaglutide is approximately 5 mg tirzepatide. Starting at 15 mg is three times the equivalent dose.
A 15 mg tirzepatide dose in someone whose GLP-1 tolerance was built at only 1.0 mg semaglutide delivers overwhelming receptor stimulation. Severe nausea and vomiting begin within 24 to 48 hours. In the SURPASS trials, even patients who titrated gradually to 15 mg reported nausea rates of 20 to 24% (Frias et al., N Engl J Med, 2021). A cold start at 15 mg without titration history produces rates far higher. Dehydration, electrolyte imbalance, and potential acute kidney injury from volume depletion are the downstream risks.
The fix: start at the dose mapped to your current semaglutide level. For 1.0 mg semaglutide, that is tirzepatide 5 mg. Titrate up from there in 4-week intervals.
Common Mistakes When Switching
Mistake 1: Overlapping the two medications.
You take your last semaglutide injection on Monday and start tirzepatide on Wednesday because you are "eager to switch." Both drugs have half-lives near 7 days. Tirzepatide stays in your system just as long as semaglutide. On Wednesday, roughly 80% of your semaglutide dose is still circulating. The tirzepatide stacks on top of it, producing dual-drug GLP-1 stimulation far exceeding what either drug delivers alone. The result is severe nausea, vomiting, and diarrhea lasting 5 to 7 days as the semaglutide clears. Wait a full week between your last dose of the old drug and your first dose of the new one.
Mistake 2: Using semaglutide syringe units for tirzepatide.
You were drawing 10 units of semaglutide from a 2.4 mg/mL vial. You switch to tirzepatide and draw 10 units from a 10 mg/mL vial without recalculating. Those 10 units now contain 1.0 mg of tirzepatide instead of 0.24 mg of semaglutide. The drugs have completely different vial concentrations. Every medication switch requires a fresh unit calculation from scratch. Use the Tirzepatide Dosage Calculator for your new vial. If your new vial needs reconstitution, see our bacteriostatic water mixing guide.
Mistake 3: Titrating up too fast after switching.
You start tirzepatide at 5 mg (mapped from 1.0 mg semaglutide). After one week, you feel fine and increase to 7.5 mg. After another week, you jump to 10 mg. GI side effects hit in week 3 with compounding severity because you never stabilized at any dose. The manufacturer's titration protocol requires 4 weeks at each dose before increasing. This is the minimum. After a medication switch, 4 weeks is even more important because your body is adapting to a new receptor profile.
Mistake 4: Assuming equivalent weight loss at equivalent doses.
You lost 12% body weight on 2.4 mg semaglutide. You switch to tirzepatide 10 mg and expect identical results immediately. Tirzepatide 10 mg produced a mean weight loss of 21.4% at 72 weeks in SURMOUNT-1 (Jastreboff et al., N Engl J Med, 2022), compared to semaglutide 2.4 mg producing 16.9% at 68 weeks in STEP 1 (Wilding et al., N Engl J Med, 2021). But your individual response depends on genetics, baseline weight, diet, activity level, and GIP receptor sensitivity. Some patients lose more on tirzepatide. Some lose less. Set expectations based on your own 4 to 8 week trend, not trial averages.
Frequently Asked Questions
Is there an official FDA-approved dose conversion between semaglutide and tirzepatide?
No FDA-approved conversion exists as of May 2026. The dose equivalences used in practice come from clinical observation, comparative weight loss data from the STEP and SURPASS trials, and receptor pharmacology. Your provider adjusts based on your tolerability. See the full tirzepatide dosage chart in units for syringe targets at every dose level.
Can I switch from semaglutide to tirzepatide in the same week?
No. Both drugs have half-lives near 7 days. Take your last semaglutide dose on schedule, then wait one full week before your first tirzepatide injection. Overlapping the two creates additive GLP-1 stimulation that causes severe nausea and vomiting. The tirzepatide titration schedule starts after a full one-week washout.
What tirzepatide dose equals 1 mg of semaglutide?
Approximately 5 mg of tirzepatide provides comparable GLP-1 receptor activity to 1.0 mg semaglutide based on clinical weight loss data. Tirzepatide adds GIP receptor activation that semaglutide does not have, so the comparison is inherently imprecise. Convert the 5 mg dose to syringe units with the tirzepatide dosage calculator.
Will I lose more weight on tirzepatide than semaglutide?
Clinical trial data suggests yes on average. Tirzepatide 15 mg produced 21.4% mean body weight loss in SURMOUNT-1 versus semaglutide 2.4 mg producing 16.9% in STEP 1. Individual results vary. For an even higher-potency triple-agonist comparison, see retatrutide vs tirzepatide at 28.7% mean loss.
How long do side effects last after switching from semaglutide to tirzepatide?
Most patients experience 1 to 2 weeks of mild GI symptoms (nausea, reduced appetite, loose stools) after the switch, even at an equivalent dose. This reflects your body adapting to tirzepatide's GIP receptor activation. If severe nausea persists beyond 2 weeks, see does tirzepatide cause headaches and nausea for management options.
Can I use the same syringes for both semaglutide and tirzepatide?
Yes if both are compounded formulations using standard U-100 insulin syringes. The units you draw will differ because vial concentrations differ. Recalculate from your new vial's mg/mL label using the formula: (dose in mg / concentration in mg/mL) times 100. See how to reconstitute tirzepatide for vial setup.
What happens if I switch from 2.4 mg semaglutide to 2.5 mg tirzepatide?
You will be significantly underdosed. Tirzepatide 2.5 mg is the lowest starting dose for drug-naive patients. The clinical equivalent for 2.4 mg semaglutide is 10 to 15 mg tirzepatide. Starting at 2.5 mg delivers roughly 75% less receptor activation, leading to weight regain. See how many units is 2.5 mg of tirzepatide for the math.
Do I need to restart titration from the beginning when switching medications?
Not from the absolute beginning. You start at the dose equivalent to your current medication level using the table above. Hold that starting dose for 4 weeks minimum before titrating up. The standard tirzepatide dosage chart in units shows the full 4-week-per-tier schedule from 2.5 through 15 mg.
The Bottom Line
No FDA-approved dose conversion exists between semaglutide and tirzepatide. The clinical practice pattern maps 0.25 to 0.5 mg semaglutide to 2.5 mg tirzepatide, 1.0 mg to 5 mg, 1.7 mg to 7.5 to 10 mg, and 2.4 mg to 10 to 15 mg. These are approximations based on comparative trial data and receptor pharmacology, not direct equivalence.
The three non-negotiable rules: wait one full week between your last dose of the old drug and your first dose of the new one, start at the conservative end of the equivalent range, and hold for 4 weeks before titrating up.
Convert your new dose to syringe units with the Semaglutide Dosage Calculator or Tirzepatide Dosage Calculator. For a complete tirzepatide dosing reference, see Tirzepatide Dosage Chart in Units. For semaglutide vial preparation, see Semaglutide Dosage Chart in mL.
Related Articles: - How Long Does Semaglutide Take to Work?: timeline for results at each dose - How Long Does Tirzepatide Take to Work?: what to expect after switching - Tirzepatide Maintenance Dose After Weight Loss: long-term dosing after reaching your goal - Does Semaglutide Need to Be Refrigerated?: storage during the transition - Does Tirzepatide Expire?: shelf life for your new medication - How to Inject Tirzepatide: injection technique for your new medication - Tirzepatide Cost With Insurance: cost comparison for the switch - Is Compound Tirzepatide Safe?: safety guide for compounded tirzepatide - Semaglutide Before and After: results to compare before switching
Related Articles
GLP-1 Injection Sites: The 3 Approved Spots
GLP-1 injection sites: abdomen, front thigh, back of upper arm. What the Ozempic, Wegovy, Mounjaro and Zepbound labels say, plus a rotation plan that works.
Tirzepatide Maintenance Dose Guide
Most patients maintain on 5-10 mg tirzepatide weekly after reaching goal weight. SURMOUNT-4 data shows stopping leads to 50-67% weight regain within 12 months.
Microdosing GLP-1: What It Is and the Risks
Microdosing GLP-1 means dosing below the range trials tested. What the dose-response data shows, how it differs from titration, and the cost and safety risks.
Not Losing Weight on Tirzepatide?
Not losing weight on tirzepatide? About 3% of users are non-responders. Learn 8 fixable reasons, SURMOUNT trial data, and a 4-week troubleshooting protocol.