Your doctor wrote the prescription. Now the pharmacy is quoting a number that makes your stomach drop. At list price, brand-name tirzepatide costs $1,023-$1,060 per month for Mounjaro and $550 for Zepbound's lowest dose. With commercial insurance, most patients pay $25-$150 per month after copay savings programs. The gap between sticker price and actual out-of-pocket cost is enormous, and navigating it determines whether this medication is affordable or impossible.
| Coverage Type | Monthly Cost Range | Notes |
|---|---|---|
| List price (no insurance) | $550-$1,060 | Zepbound vs Mounjaro, dose-dependent |
| Commercial insurance + copay card | $25-$150 | Eli Lilly savings program eligible |
| Commercial insurance (no copay card) | $150-$500 | Tier 3-4 formulary, plan-dependent |
| Medicare Part D | $300-$800+ | No manufacturer copay card; IRA caps apply |
| Medicaid | $0-$25 | State-dependent coverage |
| Compounded tirzepatide | $150-$450 | 503B pharmacy, no insurance needed |
| Telehealth programs | $199-$499 | Includes medication + consultations |
This guide covers every pathway to reduce your tirzepatide costs, from manufacturer coupons to Medicare workarounds to compounded alternatives. Use our peptide cost calculator to estimate your annual spend at each dose level.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
Mounjaro vs Zepbound: Understanding the Two Brand Names
Tirzepatide is the molecule. Eli Lilly sells it under two brand names for two different indications, and the distinction matters for insurance coverage.
Mounjaro received FDA approval in May 2022 for type 2 diabetes. It is prescribed as an adjunct to diet and exercise for glycemic control in adults with type 2 diabetes (Rosenstock et al., NEJM 2021). Insurance coverage for Mounjaro is generally strong because diabetes medications sit in a well-established formulary category.
Zepbound received FDA approval in November 2023 specifically for chronic weight management in adults with obesity (BMI 30+) or overweight (BMI 27+) with at least one weight-related comorbidity (Jastreboff et al., NEJM 2022). Insurance coverage for Zepbound is weaker because many plans still classify obesity medications as "lifestyle" drugs and exclude them from formularies.
The same molecule, the same manufacturer, the same injection pens. The difference is the diagnosis code your prescriber submits. A patient with type 2 diabetes and obesity could theoretically receive either product, but Mounjaro will almost always be cheaper through insurance because diabetes drug coverage is more comprehensive than obesity drug coverage.
If your prescriber diagnoses both conditions, ask which brand name and diagnosis code will produce the lowest out-of-pocket cost before filling the prescription.
List Price Breakdown by Dose Level
Eli Lilly's wholesale acquisition cost (WAC) determines the list price that uninsured patients face at the pharmacy counter. These prices apply when no insurance benefit or discount program is used.
| Dose | Mounjaro WAC (4 pens/month) | Zepbound WAC (4 pens/month) |
|---|---|---|
| 2.5 mg | $1,023.04 | $549.02 |
| 5 mg | $1,023.04 | $549.02 |
| 7.5 mg | $1,023.04 | $649.02 |
| 10 mg | $1,023.04 | $749.02 |
| 12.5 mg | $1,023.04 | $849.02 |
| 15 mg | $1,023.04 | $1,059.87 |
Mounjaro carries a flat WAC across all doses because each box contains four single-dose pens at the prescribed strength. Zepbound uses a tiered pricing model where higher doses cost more. At the 15 mg dose, the two products converge in price.
Zepbound launched at a lower price point deliberately. Eli Lilly positioned it to compete with semaglutide (Wegovy) in the obesity market, where payer resistance to coverage is high. The lower list price was designed to reduce the sticker shock that drives patients away before they explore coverage options.
These list prices rarely reflect what patients actually pay. They represent the starting point for negotiations between Eli Lilly, pharmacy benefit managers (PBMs), and insurance companies. The actual cost depends on your specific plan's formulary, tier placement, and any applicable savings programs.
For a personalized cost estimate based on your dose and coverage type, use our peptide cost calculator. To understand which dose you might need, see the tirzepatide dosage chart.
Commercial Insurance Coverage: What Most Employed Americans Pay
Commercial insurance, the plans offered through employers and the ACA marketplace, provides the best pathway to affordable tirzepatide. Coverage varies by plan, but the general framework is consistent.
Formulary Tier Placement
Insurance formularies organize drugs into tiers. Lower tiers mean lower copays. Tirzepatide typically sits on Tier 3 (preferred brand) or Tier 4 (non-preferred brand/specialty), depending on the PBM's negotiated rebate with Eli Lilly.
Tier 3 placement means a copay of $50-$100 per fill, or 25-35% coinsurance. For Mounjaro at $1,023 list price, 30% coinsurance produces a $307 copay before any savings card is applied.
Tier 4 or specialty tier placement means $150-$500 per fill, or 30-50% coinsurance. Some plans cap specialty copays at a fixed dollar amount ($150-$250), while others charge a percentage with no cap.
The difference between Tier 3 and Tier 4 often comes down to whether the PBM (Express Scripts, CVS Caremark, or OptumRx) has a preferred agreement with Eli Lilly. Check your plan's formulary online or call the number on the back of your insurance card to confirm tier placement before filling.
Prior Authorization Requirements
Most commercial plans require prior authorization (PA) for tirzepatide. This means your prescriber must submit clinical documentation proving the medication is medically necessary before insurance will cover it.
For Mounjaro (diabetes indication), PA typically requires documented type 2 diabetes diagnosis (HbA1c above 7.0%), failure of metformin (or documented intolerance), and sometimes failure of a sulfonylurea or SGLT2 inhibitor. Approval rates are high once documentation is submitted, generally above 80%.
For Zepbound (obesity indication), PA requirements are stricter. Common criteria include BMI of 30 or above (or 27+ with comorbidity), documented failure of a structured diet and exercise program, and sometimes prior trial of an older obesity medication (phentermine, orlistat). Some plans exclude obesity medications entirely, making PA impossible regardless of documentation.
If your PA is denied, your prescriber can appeal. First-level appeals succeed approximately 40-60% of the time for obesity medications, according to industry data. The appeal should include clinical trial evidence showing tirzepatide's efficacy and cost-effectiveness compared to bariatric surgery and long-term obesity complications.
Eli Lilly Copay Savings Programs
Eli Lilly offers manufacturer copay cards that dramatically reduce out-of-pocket costs for commercially insured patients. These programs change periodically, so verify current terms at the Eli Lilly website.
Mounjaro Savings Card: Eligible commercially insured patients pay as little as $25 per monthly prescription. The card covers up to $150 in copay assistance per fill, for a maximum of 12 fills. Patients not covered by insurance can pay $550 per month through a separate cash-pay program.
Zepbound Savings Card: Eligible commercially insured patients pay as little as $25 per monthly fill. Similar structure to the Mounjaro card, with copay assistance that bridges the gap between the insurance copay and the $25 target.
Eligibility exclusions: Patients with government-funded insurance (Medicare, Medicaid, Tricare, VA) cannot use manufacturer copay cards. This is a federal law restriction, not an Eli Lilly policy. Patients with commercial insurance through an employer, the ACA marketplace, or purchased individually are eligible.
The practical effect: a commercially insured patient on Tier 3 with a $100 copay uses the savings card and pays $25 per month. A Tier 4 patient with a $300 copay uses the savings card, which covers $150, and pays $150 per month. The card does not eliminate the copay entirely at higher tiers, but it reduces it substantially.
Medicare Coverage: The Most Expensive Pathway
Medicare presents the most challenging cost situation for tirzepatide patients. The combination of limited drug coverage, no access to manufacturer copay cards, and formulary restrictions means Medicare beneficiaries often pay the highest out-of-pocket costs.
Medicare Part D and Mounjaro
Medicare Part D covers prescription drugs, including diabetes medications. Mounjaro is covered by most Part D plans for the type 2 diabetes indication, but the cost-sharing can be significant.
Under the standard Part D benefit structure (2026), patients face a $590 deductible, then 25% coinsurance through the initial coverage period, then the coverage gap (formerly the "donut hole"), and finally catastrophic coverage where Medicare covers 80% and the patient pays 5%.
For Mounjaro at $1,023 per month, a Part D patient might pay $256 per month during the initial coverage period (25% of list price after PBM negotiated rate). The Inflation Reduction Act (IRA) capped total annual out-of-pocket Part D spending at $2,000 starting in 2025 (CMS.gov, 2024). Once a patient hits $2,000 in out-of-pocket costs, they pay nothing for the remainder of the year.
This means a Medicare patient on Mounjaro will likely hit the $2,000 annual cap within 3-5 months, then receive the medication at no cost for the rest of the year. The effective monthly cost averages $167 per month ($2,000 divided by 12). This is substantially better than the pre-IRA landscape.
Medicare and Zepbound (Obesity Indication)
Medicare Part D does not cover medications prescribed solely for weight loss. Zepbound prescribed for the obesity indication is excluded from Medicare Part D formularies by statute. This is not a plan-by-plan decision; it is a categorical exclusion written into Medicare law.
There is one exception. If a patient has both type 2 diabetes and obesity, the prescriber can prescribe Mounjaro (not Zepbound) for the diabetes indication, and the weight loss benefit comes as a secondary effect. The medication is covered because the primary indication is diabetes, not obesity.
Medicare patients without type 2 diabetes who want tirzepatide for weight loss have limited options. They can pay cash at list price ($550-$1,060 per month for Zepbound), use a compounded alternative ($150-$450 per month), or explore telehealth programs that include medication.
Congressional legislation to add obesity drug coverage to Medicare has been introduced repeatedly but has not passed as of early 2026. The Treat and Reduce Obesity Act would require Medicare to cover FDA-approved obesity medications, but its timeline remains uncertain.
Medicare Advantage Plans
Medicare Advantage (Part C) plans can offer supplemental drug coverage beyond standard Part D. Some Medicare Advantage plans have added limited obesity medication coverage as a supplemental benefit.
Coverage is plan-specific and changes annually during open enrollment. Patients should check their specific MA plan's formulary for both Mounjaro and Zepbound. Even when covered, cost-sharing through MA plans tends to be higher than commercial insurance because manufacturer copay cards remain unavailable.
The IRA's $2,000 out-of-pocket cap applies to Medicare Advantage plans with integrated Part D coverage, providing the same annual cost ceiling as standalone Part D.
Medicaid Coverage: State-by-State Variation
Medicaid coverage for tirzepatide varies dramatically by state. As a joint federal-state program, each state's Medicaid program makes independent formulary decisions.
Mounjaro for diabetes: Most state Medicaid programs cover Mounjaro for type 2 diabetes, though prior authorization requirements are common and sometimes more stringent than commercial insurance. Copays are minimal ($0-$3 per fill in most states) because Medicaid cost-sharing is capped by federal regulation for beneficiaries below 150% of the federal poverty level.
Zepbound for obesity: Very few state Medicaid programs cover obesity medications. As of early 2026, only a handful of states (including New York, Massachusetts, and a few others) have added GLP-1 receptor agonists for obesity to their Medicaid formularies. Most states exclude obesity drugs as a category, similar to Medicare.
Managed Medicaid: Many states administer Medicaid through managed care organizations (MCOs). Each MCO can have its own formulary within state guidelines. A patient in the same state but enrolled in different MCOs might have different tirzepatide coverage. Check with your specific MCO, not just the state Medicaid office.
For Medicaid patients without diabetes coverage, compounded tirzepatide represents the most accessible option. See the compounded pricing section below for details.
Compounded Tirzepatide: The Budget Alternative
Compounded tirzepatide became a significant market force after the FDA placed tirzepatide on the drug shortage list, which allowed 503A and 503B compounding pharmacies to produce copies of the molecule legally. The pricing, quality, and regulatory landscape of compounded tirzepatide deserves careful examination.
Pricing Comparison: Brand vs Compounded
Compounded tirzepatide costs a fraction of the brand-name product. Prices from established 503B compounding pharmacies typically range from $150-$450 per month depending on dose and supplier.
| Source | 2.5 mg/month | 5 mg/month | 10 mg/month | 15 mg/month |
|---|---|---|---|---|
| Mounjaro (list) | $1,023 | $1,023 | $1,023 | $1,023 |
| Zepbound (list) | $549 | $549 | $749 | $1,060 |
| Compounded (low) | $150 | $175 | $250 | $350 |
| Compounded (high) | $250 | $300 | $400 | $450 |
The cost savings are 60-85% compared to brand-name list price. For patients paying cash (no insurance coverage), compounded tirzepatide is often the only financially sustainable option for long-term treatment.
Insurance does not cover compounded medications. The entire cost is out-of-pocket. However, for patients whose insurance does not cover Zepbound or whose copay exceeds $300 per month, compounded tirzepatide may actually be cheaper than the insured brand-name option. Use our peptide cost calculator to compare scenarios.
Quality and Regulatory Considerations
Not all compounded tirzepatide is equal. The regulatory framework distinguishes between two types of compounding pharmacies.
503A pharmacies compound medications based on individual patient prescriptions. They are regulated by state boards of pharmacy and are not required to follow FDA current good manufacturing practices (cGMP). Quality varies significantly. Some 503A pharmacies produce excellent product; others have been cited for contamination, incorrect potency, or sterility failures.
503B outsourcing facilities operate under direct FDA oversight, follow cGMP, and can compound without individual prescriptions. They produce larger batches with more rigorous testing, including potency verification, sterility testing, and endotoxin screening. 503B compounded tirzepatide is generally considered more reliable.
The FDA's stance on compounded tirzepatide has evolved. When tirzepatide was on the shortage list, compounding was clearly permitted. As Eli Lilly increased production and the shortage status changed, the regulatory environment became more complex. See our coverage of FDA peptide regulations for the latest developments.
For handling compounded product, which typically arrives as lyophilized powder, see how to reconstitute tirzepatide. Storage matters: improperly stored reconstituted tirzepatide loses potency within days. Check how long does tirzepatide last in the fridge for detailed storage protocols.
How to Source Compounded Tirzepatide Safely
Finding a reliable compounding pharmacy requires due diligence. Start with these filters.
Verify the pharmacy holds a valid state license and, ideally, 503B outsourcing facility registration with the FDA. Check the FDA's list of registered outsourcing facilities. Request a certificate of analysis (COA) for your specific batch, showing potency (should be within 90-110% of labeled dose), sterility pass, and endotoxin results below USP limits.
Avoid pharmacies that sell tirzepatide without a prescription. Tirzepatide is a prescription medication regardless of whether it is brand-name or compounded. Any supplier offering it without a prescriber order is operating outside the law.
Be wary of prices below $100 per month at therapeutic doses. The raw material cost for tirzepatide is not trivial, and extremely low prices often indicate diluted product, untested batches, or overseas sourcing that bypasses quality controls. For guidance on evaluating peptide suppliers, see where to buy peptides in 2026.
Telehealth Programs: Medication Plus Consultation Bundled
A growing number of telehealth platforms offer tirzepatide as part of a bundled weight loss program. These programs typically include the medication (compounded), prescriber consultations, and sometimes nutritional coaching in a single monthly fee.
| Platform Type | Monthly Cost | Includes |
|---|---|---|
| Basic telehealth | $199-$299 | Compounded tirzepatide + monthly check-in |
| Mid-tier telehealth | $300-$399 | Medication + biweekly consultations + lab monitoring |
| Premium telehealth | $400-$499 | Medication + weekly coaching + labs + body composition |
These programs bypass insurance entirely. The medication is compounded, the prescriber works for the telehealth company, and billing goes directly to the patient. For people frustrated by insurance denials or prior authorization delays, telehealth offers a faster (though not cheaper) pathway to treatment.
The quality of medical oversight varies. Some telehealth programs employ board-certified endocrinologists and obesity medicine specialists who conduct thorough evaluations. Others use prescribers who rubber-stamp orders after minimal screening. Ask about the prescriber's credentials, whether labs (metabolic panel, thyroid function, lipase) are required before prescribing, and what happens if you experience adverse effects.
Telehealth tirzepatide programs are not a substitute for comprehensive medical care. Patients with complex medical histories, multiple medications, or severe obesity (BMI above 50) should work with an in-person specialist who can monitor for complications. See our peptide safety guide for a complete checklist of safety considerations.
Cost Per Month at Each Dose Level: A Complete Comparison
The monthly cost of tirzepatide depends on three variables: the dose, the product (brand vs compounded), and the coverage type. This table maps every combination.
| Dose | Mounjaro + Copay Card | Zepbound + Copay Card | Medicare Part D (avg) | Compounded |
|---|---|---|---|---|
| 2.5 mg | $25 | $25 | $167* | $150-$250 |
| 5 mg | $25 | $25 | $167* | $175-$300 |
| 7.5 mg | $25 | $25 | $167* | $200-$350 |
| 10 mg | $25 | $25 | $167* | $250-$400 |
| 12.5 mg | $25 | $25 | $167* | $300-$425 |
| 15 mg | $25 | $25 | $167* | $350-$450 |
*Medicare average assumes $2,000 annual cap spread over 12 months. Actual monthly costs are front-loaded: higher in months 1-4, then $0 for months 5-12.
For commercially insured patients with copay card eligibility, tirzepatide is remarkably affordable at $25 per month regardless of dose. This represents one of the best value propositions in the GLP-1 medication class. The cost challenge concentrates on patients without commercial insurance: Medicare beneficiaries, uninsured patients, and those whose plans exclude obesity medications.
The dose escalation schedule affects cumulative cost. Most patients start at 2.5 mg and titrate up over 12-20 weeks. See the tirzepatide dosage chart for the standard titration protocol. Your first three months will typically be at lower, less expensive doses if using compounded product.
To calculate your specific cost trajectory based on your planned titration schedule, use our tirzepatide dosage calculator alongside the peptide cost calculator.
Tirzepatide vs Semaglutide: Cost-Effectiveness Analysis
Raw monthly cost is only half the equation. The clinical outcomes per dollar spent determine true value. Tirzepatide and semaglutide, the two dominant GLP-1 medications, have different price tags and different efficacy profiles.
Head-to-Head Pricing
| Metric | Tirzepatide (Mounjaro/Zepbound) | Semaglutide (Ozempic/Wegovy) |
|---|---|---|
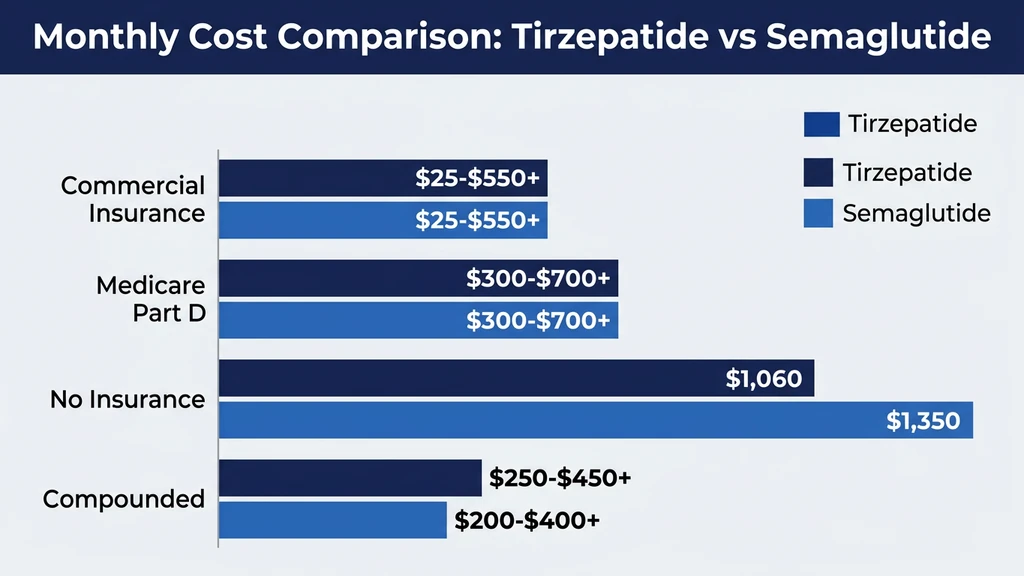
| Diabetes list price | $1,023/month | $935/month |
| Obesity list price | $549-$1,060/month | $1,349/month |
| Copay card price | $25/month | $25/month |
| Compounded price | $150-$450/month | $100-$350/month |
| Medicare avg (annual cap) | $167/month | $167/month |
At list price for the obesity indication, Zepbound is cheaper than Wegovy at every dose except 15 mg. With copay cards, both cost $25 per month for commercially insured patients. Compounded semaglutide is slightly cheaper than compounded tirzepatide because the molecule has been available longer and production is more established.
The pricing parity at the copay-card level means most commercially insured patients should choose based on clinical efficacy rather than cost.
Clinical Value Per Dollar
SURPASS-2 compared tirzepatide directly against semaglutide 1 mg in patients with type 2 diabetes. Tirzepatide 15 mg produced 13.1% weight loss versus 6.7% for semaglutide, nearly double the efficacy at similar monthly costs (Frias et al., NEJM 2021).
Cross-trial comparisons between SURMOUNT-1 (tirzepatide for obesity) and STEP 1 (semaglutide for obesity) show tirzepatide 15 mg produced 22.5% weight loss versus 14.9% for semaglutide 2.4 mg at roughly 72 weeks (Jastreboff et al., NEJM 2022; Wilding et al., NEJM 2021).
A cost-effectiveness analysis published in 2024 found tirzepatide delivered a lower cost per percentage point of weight lost compared to semaglutide across most insurance scenarios (Gomez-Lumbreras et al., 2024). At $25 per month (copay card), tirzepatide costs approximately $1.11 per percentage point of weight lost per month, versus $1.68 for semaglutide. Even at compounded prices, tirzepatide's greater efficacy offsets its higher per-milligram cost.
For patients considering a switch from semaglutide to tirzepatide, see our detailed conversion guide. If semaglutide is not producing adequate results, tirzepatide's dual mechanism offers a meaningful step up. See not losing weight on semaglutide for more context.
Long-Term Cost Considerations
Weight loss medications are not short-term treatments. SURMOUNT-4 demonstrated that discontinuing tirzepatide after 36 weeks led to regaining approximately two-thirds of lost weight over the following year (Aronne et al., JAMA 2024). Maintaining results requires ongoing treatment.
The annual cost of tirzepatide at $25 per month (copay card) is $300. At compounded prices ($200-$400 per month), the annual cost is $2,400-$4,800. At Medicare rates ($2,000 cap), the annual cost is $2,000. These costs continue indefinitely.
Compare this to the annual cost of untreated obesity: $1,861 in excess medical costs per person per year, rising to $4,000-$8,000 for individuals with obesity-related comorbidities like type 2 diabetes, cardiovascular disease, and sleep apnea (Ward et al., 2021). Bariatric surgery costs $20,000-$35,000 upfront, with its own long-term follow-up costs.
Tirzepatide at copay-card rates ($300 per year) is one of the most cost-effective medical interventions available for obesity. The challenge is that not everyone qualifies for copay-card pricing, and the people who need the medication most (Medicare beneficiaries, low-income uninsured) often face the highest costs.
Step-by-Step Guide to Minimizing Your Tirzepatide Cost
Follow this decision tree to find the lowest possible price for your situation.
Step 1: Determine your insurance type. Commercial, Medicare, Medicaid, Tricare, VA, or uninsured. This single variable determines which cost-reduction strategies are available.
Step 2: Check formulary coverage. Call the number on your insurance card or search the online formulary. Ask specifically about both Mounjaro and Zepbound. If you have both diabetes and obesity, ask which brand name and diagnosis code produces the lowest copay.
Step 3: Apply for the manufacturer copay card. If you have commercial insurance, apply at the Eli Lilly website before filling the prescription. The card is free and reduces copays to $25 per fill in most cases. Do not fill the prescription without activating the card first.
Step 4: Appeal any denial. If prior authorization is denied, file a formal appeal immediately. Include clinical documentation showing BMI, comorbidities, prior treatment failures, and references to SURMOUNT trial data showing clinical benefit. Appeals succeed 40-60% of the time.
Step 5: Explore alternatives if insurance fails. If brand-name coverage is unavailable or unaffordable, compare compounded tirzepatide from a 503B pharmacy (typically $150-$450 per month) against telehealth bundled programs ($199-$499 per month). Factor in the cost of prescriber visits and lab monitoring if using a standalone compounding pharmacy.
Step 6: Consider dose optimization. Not every patient needs the maximum 15 mg dose. SURMOUNT-1 showed 10 mg produced 21.4% weight loss versus 22.5% for 15 mg. If your results plateau at 10 mg but remain clinically significant, staying at a lower dose saves money on dose-dependent pricing (Zepbound and compounded products). See tirzepatide maintenance dose after weight loss for dose optimization strategies.
What Affects Your Insurance Coverage Decision
Insurance companies make coverage decisions based on clinical evidence, cost, and competitive pressure from alternative treatments. Understanding their logic helps you navigate the system.
The Clinical Evidence That Drives Approvals
Tirzepatide has one of the strongest clinical evidence packages of any obesity medication. The SURMOUNT trial program demonstrated 22.5% weight loss at the highest dose, superior glycemic control versus semaglutide in SURPASS-2, and cardiovascular benefit signals in secondary analyses.
The SURMOUNT-1 trial enrolled 2,539 participants and showed statistically significant weight loss across all dose arms versus placebo (Jastreboff et al., NEJM 2022). SURMOUNT-2 specifically studied tirzepatide in patients with both obesity and type 2 diabetes, demonstrating that the drug addresses both conditions simultaneously (Garvey et al., Lancet 2023).
When filing appeals, cite these specific trial results. Insurance companies respond to quantified outcomes: percentage weight loss, HbA1c reduction, cardiovascular risk reduction, and reduction in obesity-related hospitalizations.
Why Some Plans Exclude Obesity Medications
Despite strong evidence, many insurance plans exclude anti-obesity medications. The reasons are financial, not clinical.
GLP-1 medications for obesity represent a potential cost of $10,000-$15,000 per patient per year at list price. With an estimated 100 million obese adults in the United States, universal coverage would cost the healthcare system over $1 trillion annually. No payer can absorb that cost.
Plans manage this exposure through prior authorization hurdles, step therapy requirements (try cheaper drugs first), quantity limits, and outright exclusions. The exclusion strategy is blunt but effective at controlling costs. It also means many patients who would benefit clinically cannot access the medication through their insurance.
The market is shifting. As competition increases (semaglutide, tirzepatide, and emerging drugs like retatrutide), prices will likely decrease. Employer pressure is also mounting, as large self-insured employers recognize that covering obesity medications reduces downstream costs for diabetes, cardiovascular disease, and joint replacements. Coverage is improving year over year, but progress is slow.
Special Situations: Military, VA, and Employer Carve-Outs
Several coverage pathways fall outside the standard commercial/Medicare/Medicaid framework.
Tricare (military): Tricare covers Mounjaro for type 2 diabetes. Coverage for Zepbound (obesity) is limited and requires prior authorization through the managed care contractor. Copays are typically $14-$53 per fill for brand-name drugs at retail pharmacies, or $0-$29 through military treatment facility pharmacies. Manufacturer copay cards cannot be used with Tricare.
VA Healthcare: The VA formulary includes GLP-1 receptor agonists for diabetes. Obesity indication coverage varies by VA medical center and is often handled on a case-by-case basis. Veterans with type 2 diabetes and obesity have the best chance of coverage. Standard VA copays for prescription medications are $5-$11 per 30-day supply.
Employer carve-out programs: Some large employers (typically Fortune 500 companies with self-insured plans) have negotiated direct agreements with Eli Lilly for discounted tirzepatide access. These programs bypass the standard PBM formulary and offer the medication at reduced cost as part of an employer wellness initiative. Ask your HR department or benefits administrator whether your employer participates in any pharmaceutical manufacturer wellness programs.
Patient assistance programs: Eli Lilly's Lilly Cares Foundation provides free medication to uninsured patients who meet income requirements (typically below 400% of the federal poverty level). The application requires proof of income, proof of no insurance coverage, and a prescriber signature. Processing takes 4-6 weeks. This is the true safety net for low-income uninsured patients.
The Future of Tirzepatide Pricing
Several market forces will affect tirzepatide pricing over the next 2-5 years. Understanding these trends helps with long-term treatment planning.
Generic/biosimilar competition: Tirzepatide's patent protection extends into the early 2030s. Generic tirzepatide is unlikely before 2033-2035. However, biosimilar versions of semaglutide may arrive sooner, creating competitive pressure that could lead Eli Lilly to reduce tirzepatide prices preemptively.
New competitors: Eli Lilly's own pipeline includes retatrutide (triple agonist) and orforglipron (oral GLP-1). Amgen's MariTide, Pfizer's danuglipron, and other competitors are in late-stage trials. More competition generally drives prices down. See retatrutide vs tirzepatide for how next-generation drugs compare clinically.
Medicare negotiation: The Inflation Reduction Act gave Medicare the authority to negotiate prices for certain high-cost drugs. Mounjaro and Zepbound could be selected for negotiation in future cycles, which would reduce Medicare costs substantially. The first round of negotiated prices took effect in 2026, and GLP-1 medications are likely candidates for future rounds.
Compounding regulation: The FDA's approach to compounded tirzepatide will significantly affect pricing for the 30-40% of patients who currently use compounded product. If compounding is restricted after the shortage resolves, these patients will face a sharp cost increase. If compounding remains available, it will continue to provide a $150-$450 per month alternative to brand pricing. Follow our FDA regulatory updates for the latest developments.
Employer coverage expansion: The trend toward employer-sponsored obesity medication coverage is accelerating. A 2025 survey found that 44% of large employers covered GLP-1 medications for obesity, up from 25% in 2023. By 2027, projections suggest coverage will exceed 60%. If your employer does not currently cover obesity medications, it may within the next 1-2 years.
How to Talk to Your Doctor About Cost
Cost conversations with prescribers are essential but often awkward. Here is how to make them productive.
Be direct. Tell your prescriber your insurance status and budget constraints at the first visit. Prescribers cannot optimize for cost if they do not know your financial situation. Many prescribers default to brand-name prescriptions because that is what they know, not because compounded alternatives are inferior.
Ask specific questions. "Will you prescribe compounded tirzepatide if my insurance denies coverage?" is more useful than "What if I can't afford it?" Ask whether they have experience with 503B compounding pharmacies and whether they are willing to monitor patients on compounded product.
Request the diagnosis code conversation. If you have both type 2 diabetes and obesity, ask which diagnosis code will produce the best insurance outcome. A prescriber who codes for diabetes (Mounjaro) instead of obesity (Zepbound) may save you hundreds of dollars per month without changing the medication.
Discuss dose optimization. If you are responding well at 7.5 mg or 10 mg, ask whether escalating to 15 mg is clinically necessary. Staying at a lower effective dose reduces costs for dose-dependent pricing models (Zepbound, compounded). The how long does tirzepatide take to work guide covers expected timelines at each dose level.
For understanding your dosing needs in detail, check how many units is 2.5 mg of tirzepatide and how many mg is 20 units of tirzepatide.
Important Safety and Legal Information
Tirzepatide is a prescription medication regardless of source. Brand-name Mounjaro and Zepbound require a prescription from a licensed prescriber. Compounded tirzepatide also requires a valid prescription.
Do not purchase tirzepatide from sources that do not require a prescription. Products sold without prescriptions are unregulated, untested, and potentially dangerous. Reports of counterfeit GLP-1 injections containing incorrect doses, contaminants, or no active ingredient have increased alongside the medication's popularity.
Verify any compounding pharmacy through your state board of pharmacy and the FDA's outsourcing facility registry. Request certificates of analysis for each batch. If a price seems too good to be true, it probably is.
For patients new to injectable peptides, see how to inject BPC-157 for general injection technique guidance that applies to subcutaneous injections broadly. Our getting started with peptides guide covers foundational safety knowledge.
Individuals with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2 should not use tirzepatide. The drug carries a boxed warning for thyroid C-cell tumors based on rodent studies. Report severe abdominal pain, persistent vomiting, or signs of allergic reaction to your prescriber immediately.
For common side effects during treatment, see our guides on does tirzepatide make you tired and does tirzepatide cause headaches. For comprehensive safety information, visit our peptide safety guide. To understand product shelf life, see does tirzepatide expire.
This content is for educational and research purposes. Consult a qualified healthcare provider before starting, adjusting, or stopping any medication. Pricing data reflects publicly available information as of March 2026 and is subject to change.
Frequently Asked Questions
Does insurance cover tirzepatide for weight loss?
Coverage depends on your plan type. About 44% of large employer commercial plans cover GLP-1 medications for obesity as of 2025. Medicare Part D does not cover obesity medications by statute. Medicaid coverage varies by state, with only a few states including obesity drugs on their formularies. If your plan covers Zepbound, copays with the Eli Lilly savings card drop to $25 per month.
How much does tirzepatide cost per month without insurance?
Mounjaro lists at $1,023 per month across all doses. Zepbound ranges from $549 (2.5 mg) to $1,060 (15 mg). Eli Lilly offers a cash-pay program at $550 per month for eligible uninsured patients. Compounded tirzepatide from 503B pharmacies costs $150-$450 per month depending on dose and supplier. Telehealth programs bundle medication and consultations for $199-$499 per month.
Can Medicare patients get tirzepatide at a lower cost?
Medicare patients with type 2 diabetes can access Mounjaro through Part D, with annual out-of-pocket costs capped at $2,000 under the Inflation Reduction Act. This averages $167 per month across the year. Medicare does not cover Zepbound for obesity. Patients without diabetes can use compounded tirzepatide ($150-$450 per month) or apply to Eli Lilly's patient assistance program if income-eligible.
What is the Eli Lilly copay savings card and who qualifies?
The Eli Lilly savings card reduces copays to as little as $25 per monthly fill for commercially insured patients. It covers up to $150 in copay assistance per prescription. Eligibility requires commercial insurance coverage, meaning employer-sponsored or ACA marketplace plans. Patients with Medicare, Medicaid, Tricare, or VA coverage are excluded by federal law from using manufacturer copay cards.
Is compounded tirzepatide as effective as Mounjaro or Zepbound?
Compounded tirzepatide from reputable 503B outsourcing facilities contains the same molecule and should produce equivalent results when properly dosed and stored. Quality varies by pharmacy. Always request a certificate of analysis showing potency within 90-110% of the labeled dose, passing sterility tests, and endotoxin levels below USP limits. Avoid suppliers that do not provide COAs or sell without prescriptions.
How do I appeal an insurance denial for tirzepatide?
File a formal appeal through your insurance company within 30-60 days of denial. Include clinical documentation of BMI, comorbidities, prior treatment failures, and references to SURMOUNT trial data. First-level appeals succeed 40-60% of the time for obesity medications. If denied again, request an external review by an independent reviewer. Your prescriber's office can usually handle the paperwork.
Is tirzepatide cheaper than semaglutide?
At copay-card prices, both cost $25 per month. At list price, Zepbound ($549-$1,060) is cheaper than Wegovy ($1,349) for obesity. Compounded semaglutide ($100-$350 per month) is slightly cheaper than compounded tirzepatide ($150-$450). However, tirzepatide produces roughly 50% more weight loss, making it more cost-effective per percentage point of weight lost across all pricing scenarios.
Will tirzepatide get cheaper in the future?
Several factors point toward lower prices by 2028-2030. Competing GLP-1 drugs entering the market will increase pricing pressure. Medicare drug price negotiation may target tirzepatide in future cycles. Employer coverage is expanding, giving insurers more leverage. Generic tirzepatide is unlikely before 2033 due to patent protection, but biosimilar semaglutide may arrive sooner and create indirect pricing pressure.
The Bottom Line
Tirzepatide is one of the most effective weight loss medications ever developed, producing 22.5% body weight reduction in clinical trials (Jastreboff et al., NEJM 2022). Its cost ranges from $25 per month with a commercial insurance copay card to over $1,000 per month at list price without coverage. The gap between the best-case and worst-case price is wider than almost any other prescription medication.
For commercially insured patients, the path is straightforward: verify formulary coverage, activate the Eli Lilly savings card, and pay $25 per month. For Medicare patients with diabetes, the $2,000 annual Part D cap makes Mounjaro manageable at roughly $167 per month averaged across the year. For everyone else, compounded tirzepatide at $150-$450 per month or telehealth programs at $199-$499 per month represent the most accessible options.
Use our peptide cost calculator to model your specific costs based on dose, coverage type, and treatment duration. Plan your titration with the tirzepatide dosage calculator and review the tirzepatide dosage chart for unit conversions.
Related articles: - How Long Does Tirzepatide Take to Work? — week-by-week timeline with SURMOUNT trial data - Tirzepatide Maintenance Dose After Weight Loss — step-down protocols that reduce long-term costs - Why Am I Not Losing Weight on Tirzepatide? — troubleshooting before changing medications - Does Tirzepatide Burn Fat? — body composition data and fat-to-lean ratios - Semaglutide to Tirzepatide Switching Guide — dose equivalency and transition protocol - Retatrutide vs Tirzepatide — next-generation alternatives on the horizon - Where to Buy Peptides in 2026 — verified supplier directory
If you are paying out of pocket, cheapest tirzepatide lays out every self-pay route with the price of each, checked against Lilly's own published figures.
Helpful Tools
Related Articles
Cheapest Tirzepatide: Every Route Priced (2026)
The cheapest tirzepatide in 2026: manufacturer self-pay vials from $299/month, $25 insured copays, true cost per milligram, and why compounded copies ended.
Does Compounded Tirzepatide Work? Real Data
Does compounded tirzepatide work? Review SURMOUNT data, salt form differences (base, acetate, sodium), potency gaps, and FDA status in 2026.
How Much Is Semaglutide? 2026 Cost Breakdown
Semaglutide costs $149-$1,349/month depending on formulation. Compare Wegovy, Ozempic, compounded, and oral prices with savings strategies.
Does Oral Tirzepatide Work? The Facts
Oral tirzepatide is not FDA-approved. Why peptide pills face absorption barriers, sublingual drops vs injections, and oral GLP-1 alternatives in 2026.