You are holding either a Mounjaro pen with its gray cap still on, or a compounded tirzepatide vial that you just pulled from the refrigerator. Both deliver the same dual-agonist peptide, but the injection process differs between them. For the Mounjaro autoinjector pen, uncap, place flat against the skin, unlock, and press the injection button for 10 seconds. For compounded vial tirzepatide, draw your dose with an insulin syringe, pinch the skin at the abdomen, thigh, or upper arm, and inject subcutaneously at a 45-degree angle. The pen does most of the work for you. The vial requires the same technique as any subcutaneous peptide injection.
This guide covers both methods in full detail: supplies you need, choosing an injection site, step-by-step instructions for the Mounjaro autoinjector pen, step-by-step instructions for compounded tirzepatide from a vial, site rotation schedules, common mistakes, and when to seek medical help. For dosing charts and unit conversions, see the tirzepatide dosage chart and the tirzepatide dosage calculator. For the approved sites across every GLP-1 drug, see GLP-1 injection sites. If you are working with lyophilized powder that requires reconstitution, start with how to reconstitute tirzepatide before returning here.
Tirzepatide (brand name Mounjaro for type 2 diabetes, Zepbound for weight management) is FDA-approved for specific indications. Compounded tirzepatide is not FDA-approved. All injection guidance below reflects manufacturer instructions, published clinical data, and established subcutaneous injection technique. Consult a licensed healthcare provider before using tirzepatide in any form.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
Quick-Reference: Mounjaro Pen vs. Compounded Vial at a Glance
Before diving into the step-by-step process, this table summarizes the key differences between the two delivery methods. The pharmacology is identical. The injection experience is not.
| Factor | Mounjaro Autoinjector Pen | Compounded Tirzepatide Vial |
|---|---|---|
| Needle visibility | Hidden inside pen | Visible (insulin syringe) |
| Dose selection | Pre-set by pen strength (2.5mg, 5mg, 7.5mg, 10mg, 12.5mg, 15mg) | Manual: drawn by volume using syringe |
| Reconstitution needed | No (liquid pre-filled) | Sometimes (lyophilized powder requires reconstitution) |
| Needle gauge | 31 gauge, 4mm (built in) | User selects: 29 to 31 gauge recommended |
| Injection angle | 90 degrees (pen pressed flat) | 45 degrees (pinch and inject) |
| Injection sites | Abdomen, thigh, upper arm | Abdomen, thigh, upper arm |
| Injection time | 10 seconds (automatic) | 5 to 10 seconds (manual push) |
| Storage | Refrigerated or room temp up to 21 days | Refrigerated at 2 to 8 degrees Celsius |
| Cost per dose | Higher (brand pricing) | Lower (compounded pricing) |
| Skill level needed | Minimal | Moderate (same as BPC-157 injection) |
Both methods deliver tirzepatide subcutaneously. The dual GIP/GLP-1 receptor agonist reaches peak plasma concentration in 8 to 72 hours regardless of whether a pen or syringe delivers it (Coskun et al., 2018). The difference is purely mechanical.
Supplies Checklist
Gather everything before your first injection. Searching for an alcohol swab while holding a loaded syringe is how contamination and dosing errors happen.
Mounjaro Pen: What You Need
The pen arrives ready to use. Your checklist is short.
| Supply | Details |
|---|---|
| Mounjaro pen | Correct dose strength prescribed by your provider |
| Alcohol swab | 70% isopropyl, individually wrapped |
| Sharps container | FDA-cleared, puncture-resistant |
| Clean flat surface | Well-lit countertop or desk |
The pen contains a single dose. You use it once and dispose of it. No syringes, no vials, no reconstitution. Check the expiration date printed on the pen and carton. Inspect the liquid through the viewing window: it should be clear and colorless to slightly yellow. If it is cloudy, contains particles, or has changed color, do not use it.
Compounded Vial: What You Need
Compounded tirzepatide requires the same supplies as any subcutaneous peptide injection.
| Supply | Specification | Notes |
|---|---|---|
| Tirzepatide vial | Compounded, with certificate of analysis | Verify concentration on label |
| Bacteriostatic water | 30mL vial, 0.9% benzyl alcohol | Only if vial contains lyophilized powder; see bacteriostatic water sourcing |
| Insulin syringes | 29 to 31 gauge, 0.5 inch, 1mL or 0.5mL | Pharmacy purchase, no prescription needed in most US states |
| Alcohol swabs | 70% isopropyl, individually wrapped | Two per injection: one for vial stopper, one for skin |
| Sharps container | Puncture-resistant | A thick plastic detergent bottle works temporarily |
| Permanent marker | Fine-tip | Label vials with date, concentration, peptide name |
| Clean flat surface | Wiped with disinfectant | Good lighting essential for reading syringe markings |
Do not buy pre-loaded syringes from unverified sources. Tirzepatide degrades when stored in pre-loaded syringes over extended periods. Always draw fresh from a properly stored vial. For the difference between diluent types, see bacteriostatic water vs sterile water.
Choosing Your Injection Site
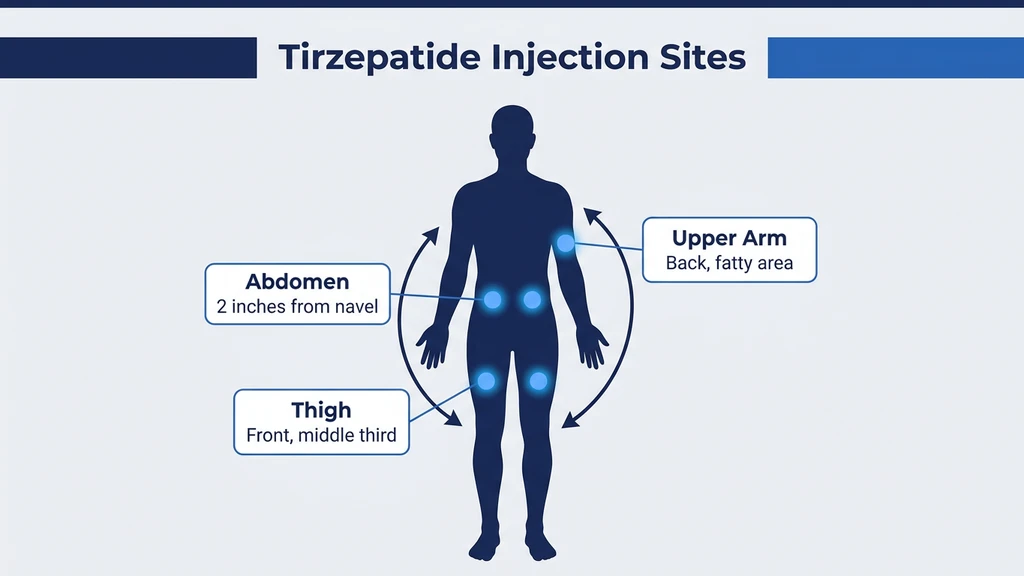
Tirzepatide is injected subcutaneously, meaning into the fat layer just beneath the skin. Three body areas are approved for tirzepatide injection based on the SURPASS and SURMOUNT clinical trials: the abdomen, the front of the thigh, and the back of the upper arm (Jastreboff et al., 2022).
| Injection Site | Location Details | Pros | Cons |
|---|---|---|---|
| Abdomen | At least 2 inches (5 cm) from navel, avoiding belt line | Largest fat pad, easiest access, most comfortable for self-injection | Avoid if abdominal skin is scarred, bruised, or has stretch marks |
| Front of thigh | Middle third of the front/outer thigh | Easy to see and reach, good fat thickness | More nerve endings than abdomen; slightly higher pain reports |
| Back of upper arm | Fleshy area on the back of the arm, between shoulder and elbow | Good absorption, useful for rotation | Difficult to self-inject; often requires help from another person |
The abdomen is the preferred site for most self-injectors. The subcutaneous fat layer is thickest here (typically 1.5 to 3 cm), making it easy to stay in the correct tissue layer. The area is simple to see, reach, and pinch.
Avoid injecting within 2 inches of the navel. The periumbilical area has denser connective tissue and more blood vessels, which increases bruising risk. Also avoid injecting into areas with visible veins, moles, scars, or skin conditions.
For the thigh, target the middle third of the front or outer aspect. The inner thigh has less subcutaneous fat and more sensitive nerve endings. Stay at least 4 inches above the knee and 4 inches below the hip crease.
The upper arm works well but is hard to reach on your own. If a partner or caregiver administers the injection, the upper arm offers excellent absorption and is comfortable for the recipient.
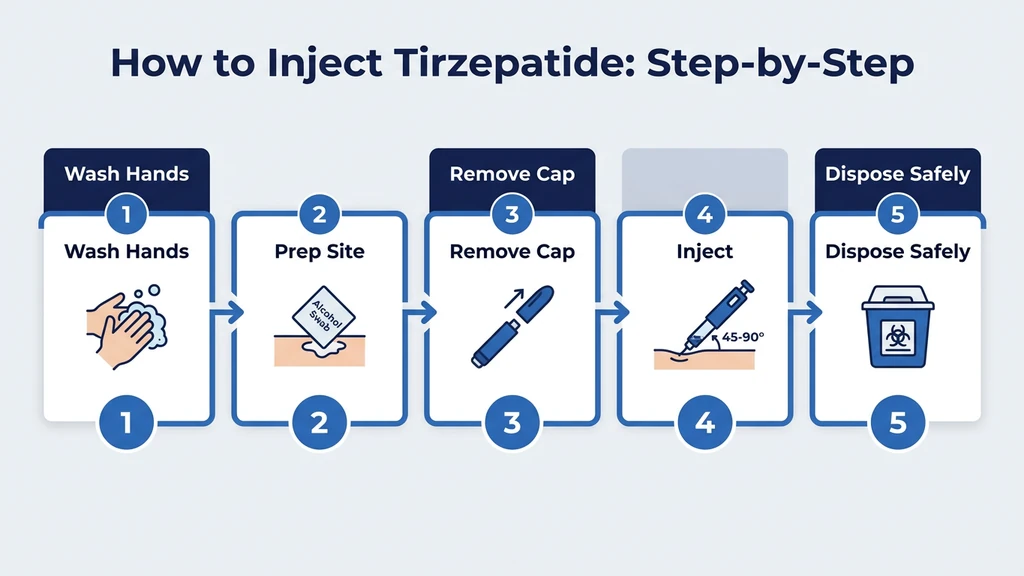
How to Inject Tirzepatide with a Mounjaro Autoinjector Pen
The Mounjaro pen is designed for people with no injection experience. The needle is hidden inside the pen body. You never see it, never handle it, never dispose of it separately. The entire pen goes into the sharps container after a single use.
Preparing the Pen
- 1.Remove the pen from the refrigerator 30 minutes before injection. Injecting cold medication increases discomfort. If the pen has been stored at room temperature (up to 30 degrees Celsius for no more than 21 cumulative days), it is ready immediately.
- 2.Check the label to confirm the correct dose strength. Mounjaro pens are color-coded: 2.5mg is plum, 5mg is brown, 7.5mg is green, 10mg is dark blue, 12.5mg is purple, and 15mg is teal.
- 3.Inspect the medication through the viewing window. The liquid should be clear and colorless to slightly yellow. Do not use if cloudy, discolored, or containing particles.
- 4.Check the expiration date. Do not use an expired pen.
- 5.Wash your hands with soap and water for at least 20 seconds. Dry with a clean towel.
Step-by-Step Pen Injection
- 1.Pull off the gray base cap. Twist it free and set it aside. This exposes the needle housing at the bottom of the pen. The needle is still retracted inside and not visible.
- 2.Swab the injection site with an alcohol pad. Wait 15 seconds for the skin to dry completely. Injecting through wet alcohol causes a stinging burn.
- 3.Place the pen flat against the skin. The clear base should sit flush against your injection site. Do not angle the pen. The built-in 31 gauge, 4mm needle is designed for 90-degree entry when the base is flat.
- 4.Unlock the pen by twisting the lock ring from the locked to the unlocked position. You will hear a click.
- 5.Press and hold the purple injection button. You will hear a first click, which means the injection has started. The needle automatically deploys into the skin.
- 6.Hold for 10 seconds. Keep the pen pressed flat against the skin. A second click occurs when the injection is complete. You do not need to count seconds precisely; the pen delivers the full dose automatically. The 10-second hold ensures complete delivery.
- 7.Lift the pen away from the skin. The needle retracts automatically into the pen body. You will not see the needle at any point.
- 8.Check the viewing window. If the gray plunger is visible in the window, the full dose was delivered. If the plunger is not visible, the injection was incomplete. Contact your healthcare provider.
- 9.Dispose of the entire pen in a sharps container. Do not recap, do not separate the needle, do not reuse.
The entire process takes under 30 seconds from cap removal to disposal. Most users report feeling only a slight pinch when the needle deploys, less noticeable than a standard blood draw.
How to Inject Compounded Tirzepatide from a Vial
Compounded tirzepatide arrives either as a pre-mixed liquid or as lyophilized powder. If you received powder, reconstitute it first following the reconstitution guide and the reconstitution calculator before proceeding with the steps below. The process mirrors any subcutaneous peptide injection, including BPC-157.
Calculating Your Dose in Syringe Units
Before drawing, you must know how many units on the syringe correspond to your prescribed dose. This depends on the concentration of your compounded solution.
| Vial Concentration | Dose (mg) | Volume to Draw (mL) | Syringe Units |
|---|---|---|---|
| 5mg/mL | 2.5mg | 0.50mL | 50 units |
| 5mg/mL | 5mg | 1.00mL | 100 units |
| 10mg/mL | 2.5mg | 0.25mL | 25 units |
| 10mg/mL | 5mg | 0.50mL | 50 units |
| 10mg/mL | 7.5mg | 0.75mL | 75 units |
| 10mg/mL | 10mg | 1.00mL | 100 units |
| 20mg/mL | 5mg | 0.25mL | 25 units |
| 20mg/mL | 10mg | 0.50mL | 50 units |
| 20mg/mL | 15mg | 0.75mL | 75 units |
The formula: dose (mg) divided by concentration (mg/mL) equals volume (mL). Multiply by 100 to convert to insulin syringe units. For exact calculations, use the tirzepatide dosage calculator. For unit conversion details, see how many units is 2.5mg of tirzepatide and how many mg is 20 units of tirzepatide.
Drawing from the Vial
- 1.Wash your hands with soap and water for at least 20 seconds. Dry with a clean towel.
- 2.Remove the vial from the refrigerator. Let it sit at room temperature for 2 to 3 minutes. Cold liquid causes more discomfort on injection. Do not microwave or heat the vial.
- 3.Swab the vial's rubber stopper with an alcohol pad. Let it dry for 10 seconds. This prevents bacteria from your fingertips from entering the vial.
- 4.Pull back the syringe plunger to the number of units you need. For example, if your dose is 50 units, pull air to the 50-unit mark.
- 5.Insert the needle through the center of the rubber stopper.
- 6.Push the air into the vial. Equalizing pressure prevents a vacuum that makes drawing difficult.
- 7.Invert the vial so the needle tip is submerged in the liquid.
- 8.Pull the plunger back slowly to your target volume. Watch for air bubbles. If they appear, flick the syringe barrel 2 to 3 times with your fingernail. Bubbles rise to the top. Push them back into the vial by advancing the plunger slightly, then redraw to your target mark.
- 9.Withdraw the needle from the vial. Return the vial to the refrigerator immediately. For storage details, see how long does tirzepatide last in the fridge.
Small air bubbles in a subcutaneous injection are not dangerous. Air embolism is a risk only with intravenous injection of large volumes (over 3 to 5mL). However, removing bubbles improves dosing accuracy because air displaces peptide solution in the syringe barrel.
Performing the Subcutaneous Injection
- 1.Choose your injection site. For your first injection, the lower abdomen (at least 2 inches from the navel) offers the easiest access and the thickest fat layer.
- 2.Swab the injection site with a fresh alcohol pad. Wait for the skin to dry completely.
- 3.Pinch a fold of skin between your thumb and index finger. Lift the fat layer gently away from the underlying muscle. Think of it like lifting the top layer of a sandwich without disturbing the filling beneath.
- 4.Hold the syringe like a pencil with the bevel (angled opening) of the needle facing up.
- 5.Insert the needle at 45 degrees in one smooth, confident motion. Hesitation drags the needle through nerve-rich skin layers and increases pain. A quick, steady push passes through the pain-sensitive dermis in a fraction of a second.
- 6.Release the skin pinch once the needle is seated.
- 7.Push the plunger slowly and steadily over 5 to 10 seconds. Tirzepatide injection volumes can be larger than other peptides (0.5 to 1.0mL is common), so slow injection prevents the stinging wheal that forms when liquid pools under the skin too quickly.
- 8.Count to 5 with the needle still in the skin. This pause lets the liquid disperse and prevents backflow through the needle track.
- 9.Withdraw the needle at the same angle you inserted it.
- 10.Press gently with a clean cotton ball or gauze if any blood appears. Do not rub. Rubbing pushes liquid out of the injection tract and causes bruising.
- 11.Dispose of the syringe in a sharps container. To avoid needlestick injuries, never push the cap onto the needle with your other hand. Use the one-handed scoop technique: lay the cap flat on a surface and slide the needle into it.
The full injection process, from hand washing to disposal, takes under 3 minutes. After 4 or 5 injections, the sequence becomes routine.
Injection Site Rotation Schedule
Tirzepatide is injected once weekly. Even at this low frequency, rotating sites prevents localized tissue damage. Repeated injections in the same spot cause lipodystrophy, where the subcutaneous fat becomes hardened or pitted. Lipodystrophy alters drug absorption, making your weekly dose unpredictable (Gentile et al., 2011).
Weekly rotation pattern across three sites:
| Week | Injection Site | Specific Location |
|---|---|---|
| 1 | Abdomen | Right side, 3 inches from navel |
| 2 | Right thigh | Middle third, outer aspect |
| 3 | Left thigh | Middle third, outer aspect |
| 4 | Abdomen | Left side, 3 inches from navel |
| 5 | Right thigh | Shift 1 inch from Week 2 spot |
| 6 | Left thigh | Shift 1 inch from Week 3 spot |
| 7 | Abdomen | Right side, 1 inch from Week 1 spot |
| 8 | Repeat cycle | Continue rotating |
If you include the upper arm (with assistance), you have four zones and an 8-week cycle before returning to the same general area. Within each zone, shift the exact injection point by at least 1 inch (2.5 cm) from the previous injection in that zone.
What not to do: inject in the same spot every week because "it does not hurt there." That painless spot may have developed early lipodystrophy, reducing nerve sensitivity along with drug absorption.
This rotation principle applies to all subcutaneous injections. The same logic governs BPC-157 injection site rotation and other peptide protocols described in the peptide safety guide.
Timing Your Weekly Injection
Tirzepatide is dosed once per week. The SURPASS-1 trial demonstrated that the half-life of tirzepatide is approximately 5 days (120 hours), supporting the 7-day interval between doses (Rosenstock et al., 2021). Choose a consistent day each week. If you inject on Monday morning, inject every Monday morning. For more on how the drug clears your system, see how long does tirzepatide stay in your system.
Best practices for injection timing:
Pick a day when you are home, unhurried, and can manage potential side effects. The first 24 to 48 hours after injection carry the highest likelihood of nausea, which is the most commonly reported adverse event at 12 to 22% of patients in the SURMOUNT-1 trial (Jastreboff et al., 2022). Many users inject on Friday evening so that any GI side effects overlap with the weekend.
There is no strict requirement for morning vs. evening injection. Absorption kinetics are the same regardless of time of day. What matters is consistency: maintaining the 7-day interval keeps plasma levels stable and minimizes breakthrough hunger between doses.
If you miss your scheduled day by 4 or fewer days, inject as soon as you remember and resume your regular schedule the following week. If you miss by more than 4 days, skip that dose entirely and inject on the next scheduled day. Do not double-dose to "catch up." For long-term dosing strategy, see the tirzepatide maintenance dose after weight loss guide.
Managing the Dose Escalation Schedule
Tirzepatide uses a mandatory dose escalation protocol. You do not start at your target dose. The FDA-approved schedule begins at 2.5mg weekly for 4 weeks, then increases by 2.5mg increments every 4 weeks until the target dose is reached. This gradual ramp gives the GI tract time to adjust to the dual GIP/GLP-1 receptor activation (Frías et al., 2021).
| Weeks | Weekly Dose | Injection Volume at 10mg/mL | Purpose |
|---|---|---|---|
| 1 to 4 | 2.5mg | 25 units (0.25mL) | Initiation; GI adaptation |
| 5 to 8 | 5mg | 50 units (0.50mL) | First therapeutic increase |
| 9 to 12 | 7.5mg | 75 units (0.75mL) | Continued escalation |
| 13 to 16 | 10mg | 100 units (1.00mL) | Escalation continues |
| 17 to 20 | 12.5mg | Use 20mg/mL concentration | Higher doses; adjust vial concentration |
| 21+ | 15mg (maximum) | 75 units at 20mg/mL (0.75mL) | Maximum approved dose |
For compounded vial users, higher doses often require switching to a more concentrated formulation. Drawing 1.5mL from a 10mg/mL vial for a 15mg dose is impractical with a 1mL insulin syringe. A 20mg/mL concentration keeps every dose under 1mL.
If side effects become intolerable at a new dose, your provider may keep you at the current dose for an additional 4 weeks rather than continuing escalation. This is a clinical decision. Do not self-adjust your dose without guidance. For detailed dosing charts, see the tirzepatide dosage chart. If you are struggling with expected weight loss, read why am I not losing weight on tirzepatide.
Common Injection Mistakes and How to Avoid Them
These errors appear repeatedly in clinical practice and patient communities. Every one is preventable.
Pen-Specific Mistakes
Mistake 1: Lifting the pen before the second click. The Mounjaro pen clicks twice. The first click means the injection started. The second click means it finished. Lifting after the first click delivers a partial dose. The remaining medication stays inside the pen, which you then discard. Fix: press and hold for the full 10 seconds. Wait for the second click. Check the viewing window for the gray plunger.
Mistake 2: Injecting through clothing. Some insulin pen guides suggest injecting through clothing. The Mounjaro pen manufacturer does not recommend this. Fabric can deflect the short 4mm needle, cause incomplete penetration, or introduce fiber fragments into the injection site. Fix: always inject on bare, cleaned skin.
Mistake 3: Storing the pen with the cap off. The gray base cap keeps the needle housing sterile. Removing it early and setting the pen down exposes the needle deployment area to bacteria on your countertop. Fix: remove the cap immediately before injection, not 10 minutes beforehand.
Mistake 4: Using an expired pen. Check the expiration date on both the pen and the outer carton. Tirzepatide stability decreases after expiration. The peptide may still be present but at reduced potency, leading to subtherapeutic dosing. For more on expiration, see does tirzepatide expire.
Vial-Specific Mistakes
Mistake 5: Confusing units with milligrams. An insulin syringe reads in units, not mg. If your concentration is 10mg/mL, then 50 units (0.5mL) equals 5mg. Misreading this as 50mg is a 10x calculation error. Fix: always calculate volume first (dose divided by concentration), then convert to syringe units. Use the tirzepatide dosage calculator to verify.
Mistake 6: Using sterile water instead of bacteriostatic water for reconstitution. Sterile water lacks the 0.9% benzyl alcohol preservative that inhibits bacterial growth. Within 48 hours, bacteria can colonize the vial. By day 7, you inject contaminated liquid. Fix: always use bacteriostatic water for multi-dose vials. See the bacteriostatic vs sterile water comparison for details.
Mistake 7: Shaking the vial during reconstitution. Aggressive shaking causes agitation-induced aggregation, denaturing the peptide through mechanical force. The result looks like a cloudy, foamy liquid instead of a clear solution. Denatured tirzepatide is biologically inactive. Fix: swirl gently in slow circles until the powder dissolves. This takes 60 to 90 seconds. Never shake. See reconstitution best practices for the full technique.
Mistake 8: Leaving the vial at room temperature. Each minute at room temperature degrades the peptide. Cumulative exposure over a multi-week use cycle reduces potency. Fix: return the vial to the refrigerator within 2 minutes of drawing your dose. For exact storage guidance, see how long does tirzepatide last in the fridge.
Technique Mistakes (Both Methods)
Mistake 9: Injecting into muscle instead of fat. On lean individuals, pushing a 0.5-inch needle at 90 degrees can penetrate through the thin subcutaneous layer into muscle. The injection hurts more, bleeds more, and produces larger bruises. Fix: for vial injections, always insert at 45 degrees with the skin pinched. The Mounjaro pen uses a short 4mm needle specifically to avoid intramuscular delivery.
Mistake 10: Not rotating injection sites. Using the same site weekly creates localized lipodystrophy within 2 to 3 months. The hardened tissue absorbs medication erratically, creating unpredictable drug levels that swing between too high and too low. Fix: follow the rotation schedule outlined above. Never inject in the same 1-inch radius within a 4-week window.
Mistake 11: Injecting too fast. Pushing 0.5 to 1.0mL of liquid rapidly into subcutaneous tissue creates a painful wheal, a raised, stinging lump that takes 10 to 15 minutes to absorb. Fix: push the plunger over 5 to 10 seconds. Slow delivery distributes the liquid gradually across a wider area.
Managing Side Effects After Injection
Injection-site reactions and systemic side effects are distinct categories. Understanding the difference prevents unnecessary alarm and ensures you seek help when it matters.
Injection-Site Reactions
Local reactions at the injection site are common and usually minor. A meta-analysis of tirzepatide clinical trials reported injection-site reactions in 3 to 5% of participants, most resolving within 48 hours (Karagiannis et al., 2024).
Normal reactions: a small red dot at the needle entry, mild itching that resolves within 1 to 2 hours, a tiny bruise (especially on the thigh), a temporary wheal if the injection was pushed too fast.
When to contact your provider: redness spreading beyond 2 cm in diameter, increasing warmth and swelling over 24 to 48 hours, pus or discharge from the site, a hard lump that grows larger rather than shrinking, or red streaking along the skin radiating from the injection point.
To reduce injection-site irritation, ensure the alcohol swab has dried completely, let the solution warm to room temperature before injecting, and inject slowly.
Systemic Side Effects in the First 24 to 48 Hours
The most common systemic side effects relate to the GI tract: nausea, diarrhea, and decreased appetite. These reflect the mechanism of action, not an injection error. Tirzepatide slows gastric emptying and modulates appetite through hypothalamic GLP-1 receptor activation (Nauck et al., 2021).
For practical management of specific side effects: - Nausea and fatigue: does tirzepatide make you tired - Headaches: does tirzepatide cause headaches - Constipation: does tirzepatide cause constipation - Diarrhea: does tirzepatide cause diarrhea - Hair thinning: does tirzepatide cause hair loss - Alcohol interactions: can you drink on tirzepatide
Most GI side effects peak during dose escalation and diminish within 2 to 4 weeks at each new dose level. The dose ramp exists specifically to minimize these effects. If nausea is severe, eat smaller meals, avoid fatty foods for 24 hours post-injection, and stay hydrated. Contact your provider if vomiting persists beyond 48 hours.
When to Seek Emergency Medical Help
Most tirzepatide side effects are manageable at home. A small number require immediate medical attention.
Seek emergency care if you experience: - Signs of anaphylaxis: swelling of face, lips, tongue, or throat; difficulty breathing; rapid heartbeat; dizziness or loss of consciousness. Anaphylactic reactions to tirzepatide are rare (less than 0.1% in clinical trials) but life-threatening. - Severe abdominal pain that does not resolve, especially if accompanied by vomiting. This may indicate pancreatitis. The SURPASS trials excluded patients with a history of pancreatitis, and cases during the trial were extremely rare, but the risk is listed in the prescribing information. - Signs of hypoglycemia if you also take insulin or sulfonylureas: shaking, sweating, confusion, rapid heartbeat, blurred vision, blood sugar below 54 mg/dL. Tirzepatide alone rarely causes hypoglycemia, but combined with other glucose-lowering medications, the risk increases (Rosenstock et al., 2021). - Signs of injection-site abscess: expanding redness, warmth, pus, fever, or red streaks radiating from the injection point. This indicates bacterial infection requiring antibiotics and possibly surgical drainage.
Do not attempt to treat these conditions at home or "wait it out." Do not inject another dose until cleared by a medical professional. For a broader overview of peptide safety principles, see the peptide safety guide.
Switching Between Mounjaro Pens and Compounded Vials
Some patients switch from Mounjaro pens to compounded tirzepatide for cost reasons. Others switch from compounded to brand-name pens for convenience or regulatory compliance. The pharmacology of the molecule is the same. What changes is the injection technique and the dose verification process.
Pen to vial transition: The biggest adjustment is learning manual syringe technique. You go from a device that hides the needle and delivers automatically to a process where you draw, measure, and inject by hand. Budget 10 minutes for your first vial injection. By the third or fourth time, the process becomes familiar.
Verify the concentration of your compounded vial carefully. A Mounjaro 5mg pen delivers exactly 5mg. A compounded vial requires you to calculate the correct volume based on the stated concentration. A 10% calculation error on a 10mg dose means you receive 9mg or 11mg, enough to affect side-effect intensity and therapeutic response. Always cross-check with the dosage calculator.
Vial to pen transition: Moving to the pen is simpler. The pre-filled pen eliminates dosing math. Your only decision is which pen strength to use, which is determined by your prescriber. There is no reconstitution, no drawing, no syringe handling.
If you are switching from semaglutide to tirzepatide (either direction), the dose equivalence is not 1:1. See the semaglutide to tirzepatide switching guide for conversion details.
Tirzepatide Injection and Fat Burning: What the Evidence Shows
Some users ask whether the injection site affects where fat is lost. It does not. Tirzepatide activates GIP and GLP-1 receptors systemically, reducing appetite, slowing gastric emptying, and improving insulin sensitivity throughout the body. Fat loss occurs globally, with individual variation driven by genetics, not injection location.
In the SURMOUNT-1 trial, participants receiving 15mg tirzepatide weekly lost an average of 22.5% of body weight over 72 weeks (Jastreboff et al., 2022). DEXA body composition analysis in SURMOUNT-2 showed that approximately 33% of total weight loss came from lean mass, with the remaining 67% from fat mass. Injecting in the abdomen does not preferentially reduce abdominal fat. The medication works through central appetite regulation and metabolic improvement, not local lipolysis.
For more on the fat loss mechanism, see does tirzepatide burn fat. For expected timelines, see how long does tirzepatide take to work.
Pain Minimization Tips for Both Injection Methods
Pain from tirzepatide injection ranges from "felt nothing" to "brief pinch." The Mounjaro pen's 31 gauge, 4mm needle is among the thinnest available, and most users report minimal sensation. Vial injection with a 29 to 31 gauge syringe is similarly comfortable when technique is correct.
Let the medication reach room temperature. Cold liquid stings. Remove the pen or vial from the refrigerator 30 minutes (pen) or 2 to 3 minutes (vial) before injecting. Do not use a microwave, hot water bath, or direct sunlight.
Wait for the alcohol swab to dry. Alcohol pushed into subcutaneous tissue by the needle causes a sharp burn lasting 10 to 20 seconds. This is the single most common cause of injection-site pain. Fifteen seconds of air drying eliminates it.
Inject slowly. Push the plunger over 5 to 10 seconds for vial injections. The pen handles this automatically. Rapid injection creates a pressurized pocket of fluid that stretches tissue and stings.
Pinch firmly (vial method). A solid pinch lifts the fat layer and numbs the area through pressure-induced analgesia. A weak pinch leaves the skin taut and makes needle entry more noticeable.
Breathe out during insertion. Exhaling relaxes the abdominal wall. Tense muscles resist the needle; relaxed tissue yields easily. This is not mysticism. It is the same principle physical therapists use during manual procedures.
Ice the site for 30 seconds beforehand. For the first few injections, holding an ice cube wrapped in a paper towel against the injection site for 20 to 30 seconds before swabbing temporarily numbs the skin. Most users drop this step after the first month once they realize the injection is nearly painless without it.
Frequently Asked Questions
Where is the best place to inject tirzepatide?
The abdomen is the preferred injection site for most self-injectors. Choose a spot at least 2 inches (5 cm) from the navel, where subcutaneous fat is typically 1.5 to 3 cm thick. The front of the thigh (middle third) and back of the upper arm are approved alternatives. Rotate among all 3 sites on a weekly schedule to prevent lipodystrophy.
Do I need to pinch the skin when using the Mounjaro pen?
No. The Mounjaro pen uses a 31 gauge, 4mm needle designed for 90-degree insertion when placed flat against the skin. Pinching is unnecessary because the short needle cannot reach muscle tissue through typical subcutaneous fat thickness. For compounded vial injections with a 0.5-inch needle, pinching is required to ensure you inject into the fat layer at a 45-degree angle.
How long do I hold the Mounjaro pen against my skin?
Hold for 10 seconds after pressing the injection button. You will hear 2 clicks: the first indicates the injection has started, the second confirms it is complete. Lifting before the second click delivers a partial dose. Check the viewing window afterward; a visible gray plunger confirms the full dose was delivered.
Can I inject tirzepatide in my arm by myself?
It is difficult to self-inject in the back of the upper arm because you cannot see or easily reach the injection site. If you inject alone, use the abdomen or thigh instead. If a partner or caregiver is available, the upper arm is an excellent option with good subcutaneous fat thickness and comfortable absorption. Rotate all 3 sites over a 6 to 8 week cycle.
What needle size should I use for compounded tirzepatide?
A 29 to 31 gauge, 0.5-inch (12.7mm) insulin syringe. This gauge is thin enough to minimize pain, short enough to remain in the subcutaneous fat layer at a 45-degree angle, and wide enough to draw liquid from the vial without excessive resistance. For doses above 50 units, use a 1mL syringe. For doses under 25 units, a 0.5mL syringe provides wider tick-mark spacing and better accuracy.
What happens if I miss my weekly tirzepatide injection?
If you are 4 or fewer days late, inject as soon as you remember and resume your regular weekly schedule. If you are more than 4 days late, skip that dose entirely and inject on the next scheduled day. Never double-dose. Tirzepatide has a half-life of approximately 5 days (120 hours), so a single missed dose does not eliminate the drug from your system.
Why does my tirzepatide injection burn or sting?
The 3 most common causes are: injecting through wet alcohol on the skin (wait 15 seconds for it to dry), injecting cold solution straight from the refrigerator (let it warm 2 to 3 minutes), and pushing the plunger too fast (inject over 5 to 10 seconds). Fix these 3 variables and most users describe the sensation as barely noticeable with a 29 to 31 gauge needle.
Can I switch from semaglutide to tirzepatide injections?
Yes, but the doses are not equivalent. Tirzepatide and semaglutide have different receptor binding profiles (dual GIP/GLP-1 vs. GLP-1 only) and different dose ranges. A provider typically starts tirzepatide at 2.5mg weekly regardless of your prior semaglutide dose, then escalates every 4 weeks. See the semaglutide to tirzepatide switching guide for detailed conversion protocols.
The Bottom Line
The injection itself takes under 30 seconds with a Mounjaro pen, under 3 minutes with a compounded vial. What determines whether the experience is smooth or painful is preparation. For the pen: check the label, let it warm, swab the skin, press flat, hold for 10 seconds, check the window. For the vial: calculate your dose, swab the stopper and skin, draw carefully, pinch, inject slowly at 45 degrees, count to 5, withdraw.
Rotate injection sites every week across abdomen, thigh, and upper arm. Maintain your dose escalation schedule: 2.5mg for 4 weeks, then increase by 2.5mg every 4 weeks until your target dose. Return vials to the refrigerator immediately. Use a fresh syringe for every injection. Dispose of pens and syringes in a sharps container.
For dose calculations, use the tirzepatide dosage calculator and the reconstitution calculator. For unit conversions, see how many units is 2.5mg of tirzepatide and the dosage chart.
Related articles: - How to Reconstitute Tirzepatide — step-by-step reconstitution for lyophilized powder - Tirzepatide Dosage Chart in Units — complete dosing reference table - Tirzepatide Maintenance Dose After Weight Loss — long-term dose strategy - How Long Does Tirzepatide Take to Work? — expected timelines by dose - Does Tirzepatide Burn Fat? — mechanism of fat loss explained - Bacteriostatic Water vs Sterile Water — why BAC water is essential for multi-dose vials - Peptide Safety Guide — comprehensive safety protocols for all peptides - How to Inject BPC-157 — companion injection guide for another common subcutaneous peptide
Related Articles
Tirzepatide Injection Site Reactions
Injection site reactions affect 3-7% of tirzepatide users. SURMOUNT trial rates, 5 reaction types, severity guide, and 9 prevention strategies.
Tirzepatide: How Long to Work?
Tirzepatide reduces appetite within the first week, produces measurable weight loss by week 4, and delivers significant results by weeks 12-16.
How to Inject BPC-157: Sites & Guide
How to inject BPC-157 subcutaneously: step-by-step technique, injection site selection by injury, needle gauge, reconstitution, and sterile protocol.
Best Place to Inject Tirzepatide: 3 Sites Ranked
Best tirzepatide injection site: the abdomen, for fat pad and access. Compare abdomen, thigh, and upper arm with rotation maps and BMI guidance.