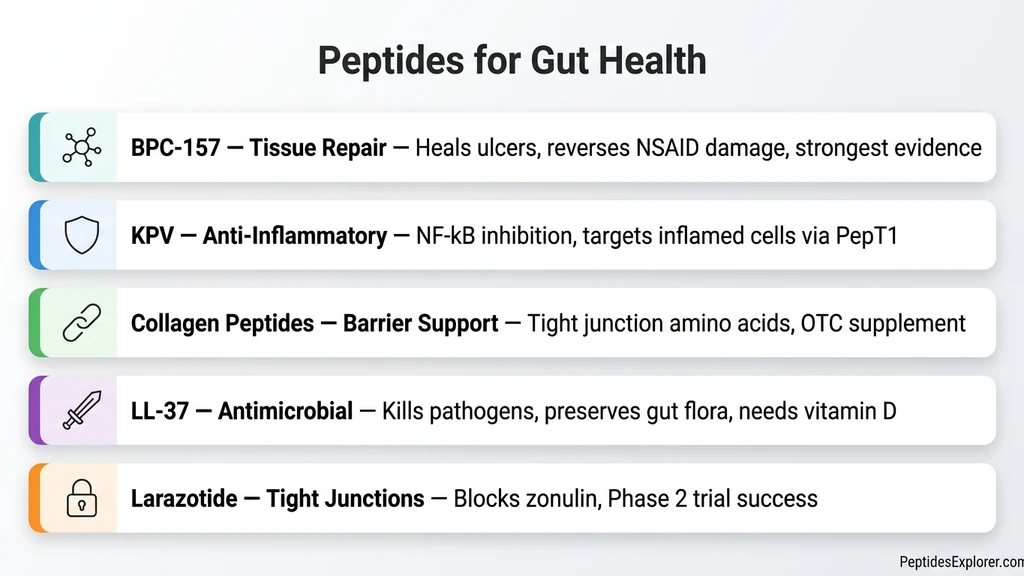
The most effective peptides for gut health are BPC-157 (tissue repair), KPV (anti-inflammatory), LL-37 (antimicrobial barrier protection), collagen peptides (tight junction support), and larazotide (permeability regulation). Each targets a different mechanism of gut damage, and the strongest results come from combining them based on your specific condition.
A 2025 American College of Gastroenterology systematic review of 36 studies confirmed BPC-157's healing effects across IBD, GI ulcers, NSAID injury, and fistula models (ACG 2025 Abstract S808). That review represents the strongest published evidence for any gut-healing peptide to date.
Search interest in peptides for gut health has grown 238% year-over-year. BPC-157 and KPV have entered early-stage clinical evaluation. Collagen peptides already sit on supplement shelves. LL-37 is the body's own antimicrobial defense, produced when vitamin D levels are adequate.
No peptide covered here is FDA-approved for gut conditions. Consult a healthcare provider before acting on any information.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
How Do Peptides Heal the Gut?
Gut healing peptides work through four distinct mechanisms. Understanding these pathways explains why different peptides suit different conditions, and why combining them produces stronger results than any single compound.
Tissue Repair and Angiogenesis
BPC-157 drives this pathway. It upregulates vascular endothelial growth factor (VEGF), nitric oxide synthesis, and the prostaglandin system to accelerate blood vessel formation in damaged tissue.
New blood vessels deliver oxygen and nutrients to injured mucosa. Fibroblast migration increases. Collagen synthesis at the wound site accelerates.
This mechanism explains why BPC-157 heals gastric ulcers, NSAID damage, and surgical anastomoses in animal studies. The peptide reconstructs the physical architecture of the gut lining (Sikiric et al. 2022, PMC10224484).
Inflammation Suppression
KPV inhibits NF-kB, the master switch of inflammatory gene expression, at nanomolar concentrations. It also suppresses the NLRP3 inflammasome, breaking the self-perpetuating inflammatory cycle that drives chronic gut conditions (Dalmasso et al. 2008, PMC2431115).
KPV shifts macrophage polarization from M1 (destructive) to M2 (reparative). This changes the immune environment from tissue destruction to tissue healing.
The result: a 50% reduction in DSS-induced colitis severity in the original Dalmasso study. Inflammation falls. Healing begins.
Barrier Function and Tight Junction Repair
Tight junctions are the seals between intestinal cells. When they open, undigested food particles and bacteria leak into the bloodstream. This is "leaky gut" at the molecular level.
Larazotide antagonizes zonulin, the protein that forces tight junctions open. Collagen peptides supply glycine and proline to strengthen junction proteins. LL-37 preserves goblet cells and upregulates mucin-2, the protective mucus layer that sits above the cell barrier (Shih et al. 2023, PubMed 36958193).
Three peptides, three layers of barrier defense.
Antimicrobial Defense
LL-37 is the body's primary antimicrobial peptide. It disrupts pathogenic bacterial membranes through direct contact while preserving beneficial gut flora.
A 2020 Frontiers in Immunology study showed that LL-37 protects gut microbiota composition during enterohemorrhagic E. coli infection (Frontiers 2020). The peptide kills pathogens without collateral damage to commensals.
Endogenous LL-37 production depends on vitamin D status. Low vitamin D means low LL-37 means a weaker antimicrobial barrier. Supplementing LL-37 directly bypasses this bottleneck.
What Are the 5 Best Peptides for Gut Health?
Ranked by strength of evidence, mechanism specificity, and practical availability. Each peptide earns its place for a different reason.
1. BPC-157: The Gold Standard for Gut Tissue Repair
BPC-157 (Body Protection Compound-157) is a 15-amino-acid peptide derived from human gastric juice. It occurs naturally in the stomach, which makes it uniquely suited for gut applications.
Evidence. The 2025 ACG systematic review analyzed 36 studies spanning 1993 to 2025 and found consistent healing in IBD, GI ulcers, NSAID injury, and fistula models. No adverse effects were reported across organ systems (ACG 2025). A 2024 review in Inflammopharmacology confirmed BPC-157's pleiotropic cytoprotective activity in the GI tract (Springer 2025).
How it works. BPC-157 upregulates VEGF, stimulates fibroblast migration, promotes collagen synthesis, and protects against NSAID-induced gastric damage. It heals ulcers from both the gastric and intestinal side (PubMed 21548867).
Dosage for gut. 250 to 500 mcg per day, oral preferred. BPC-157 is stable in gastric juice, unlike most peptides. Oral delivery puts the compound in direct contact with the GI lining. See Can You Take BPC-157 Orally? for a detailed breakdown.
Best for. Gastric ulcers, NSAID damage, IBD, surgical recovery, general gut tissue repair.
2. KPV: The Anti-Inflammatory Specialist
KPV (Lys-Pro-Val) is a tripeptide fragment of alpha-melanocyte stimulating hormone (alpha-MSH). Three amino acids. Powerful anti-inflammatory signaling.
Evidence. Dalmasso et al. (2008) demonstrated a 50% reduction in DSS-induced colitis severity with oral KPV administration. A 2024 Frontiers in Pharmacology study showed KPV nanoparticle delivery further improved colitis outcomes (Frontiers 2024). KPV also inhibits colitis-associated tumorigenesis via PepT1-mediated uptake (PMC4957955).
Unique mechanism. The intestinal PepT1 transporter absorbs KPV directly into epithelial cells. PepT1 is upregulated during inflammation, so sicker tissue absorbs more KPV. The peptide targets itself to the cells that need it most.
Dosage for gut. 200 to 500 mcg per day, oral. The PepT1 uptake mechanism makes oral delivery highly effective for gut inflammation. See the KPV Dosage Guide for complete protocols.
Best for. Active intestinal inflammation, IBD (Crohn's and ulcerative colitis), colitis prevention.
3. Collagen Peptides: The Accessible Gut Barrier Builder
Collagen peptides are hydrolyzed collagen protein, rich in glycine, proline, and glutamine. They are the most accessible option on this list: available over-the-counter, no prescription or reconstitution needed.
Evidence. A 2017 in vitro study showed collagen peptides enhance tight junction proteins in Caco-2 intestinal cells (PubMed 28174772). A 2022 randomized controlled trial found improvements in digestive symptoms among women taking collagen supplements (PMC9198822).
Honest assessment. The evidence is more indirect than for BPC-157 or KPV. Collagen peptides work by supplying amino acid building blocks to enterocytes, not through direct cell signaling. Think of them as construction materials rather than construction orders.
Dosage. 10 to 20 grams per day for at least 6 weeks. Mix into water, coffee, or smoothies. Results build gradually.
Best for. General gut barrier support, mild permeability issues, foundational use alongside therapeutic peptides.
4. LL-37: The Antimicrobial Barrier Protector
LL-37 (cathelicidin) is a 37-amino-acid peptide and the only human antimicrobial peptide of its class. The body produces it naturally as a first-line defense against pathogenic bacteria.
Evidence. Shih et al. (2023) showed LL-37 preserves goblet cells, increases mucin-2 production, and upregulates Nrf2 antioxidant pathways in intestinal tissue. A Frontiers in Immunology study confirmed LL-37 protects gut microbiota composition during E. coli infection without harming beneficial bacteria.
Vitamin D connection. LL-37 production requires adequate vitamin D. Populations with low vitamin D (northern latitudes, indoor lifestyles, darker skin) produce less LL-37 and have weaker antimicrobial gut barriers. Exogenous LL-37 supplementation bypasses this dependency.
Dosage. 100 to 200 mcg per day, subcutaneous injection. LL-37 is not typically taken orally for gut applications. See LL-37 Benefits for the full evidence profile.
Best for. Gut infections, dysbiosis, barrier protection during illness, immune-compromised patients.
5. Larazotide: The Tight Junction Regulator
Larazotide acetate is a synthetic 8-amino-acid peptide and the only compound on this list designed specifically to regulate tight junctions. It is a zonulin antagonist: it blocks the protein that forces intestinal cell junctions open.
Evidence. Larazotide holds the strongest human trial data of any peptide here. A Phase 2 randomized controlled trial in celiac disease patients showed a 26% decrease in symptomatic days (P=.017) and a 31% increase in improved symptom days (P=.034) (PMC4446229).
The honest disclosure. Phase 3 trials were discontinued due to enrollment challenges, not safety concerns (Beyond Celiac). Larazotide is not commercially available. It remains a research compound only, with no current path to market.
Why include it. Larazotide demonstrates that targeting tight junctions directly can produce measurable symptom improvement in humans. It validates the leaky gut mechanism and sets the scientific benchmark for barrier-focused peptide therapy.
Best for. Intestinal permeability (leaky gut), celiac-related gut damage. Available only through research channels.
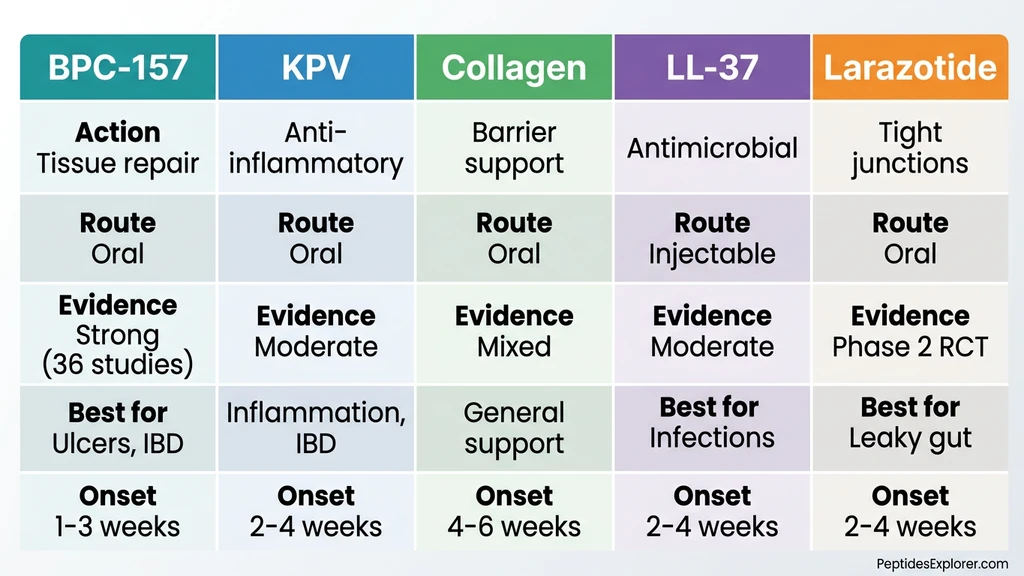
How Do These Peptides Compare Head-to-Head?
The table below maps each peptide across nine dimensions. Use it to identify which compound fits your condition, budget, and comfort level with administration routes.
| Factor | BPC-157 | KPV | Collagen Peptides | LL-37 | Larazotide |
|---|---|---|---|---|---|
| Primary action | Tissue repair, angiogenesis | Anti-inflammatory (NF-kB) | Tight junction amino acids | Antimicrobial + barrier | Tight junction regulation |
| Best for | Ulcers, NSAID damage, IBD | Active inflammation, IBD | General gut support | Infection + barrier loss | Leaky gut (celiac) |
| Evidence level | Strong preclinical + ACG 2025 | Moderate preclinical | Mixed (indirect mechanism) | Moderate preclinical | Phase 2 RCT (strongest human data) |
| Route for gut | Oral preferred | Oral (PepT1 uptake) | Oral (supplement) | Subcutaneous | Oral (capsule in trials) |
| Typical dose | 250-500 mcg/day | 200-500 mcg/day | 10-20 g/day | 100-200 mcg/day | 0.5 mg TID (trial dose) |
| Onset | 1-3 weeks | 2-4 weeks | 4-6 weeks | 2-4 weeks | 2-4 weeks |
| Availability | Research peptide | Research peptide | OTC supplement | Research peptide | Research only (not available) |
| Stackable | Yes (pairs with KPV) | Yes (pairs with BPC-157) | Yes (with any peptide) | Yes (with BPC-157) | Unknown |
| Cost | $$ | $$ | $ | $$$ | N/A |
Larazotide has the strongest human clinical data but the lowest accessibility. BPC-157 has the broadest preclinical evidence and the best practical availability. Collagen peptides offer the lowest barrier to entry.
Which Peptides Work Best for Your Gut Condition?
Different conditions require different peptides. A leaky gut protocol looks nothing like an IBD protocol. Below: condition-specific recommendations based on each peptide's mechanism of action and available evidence.
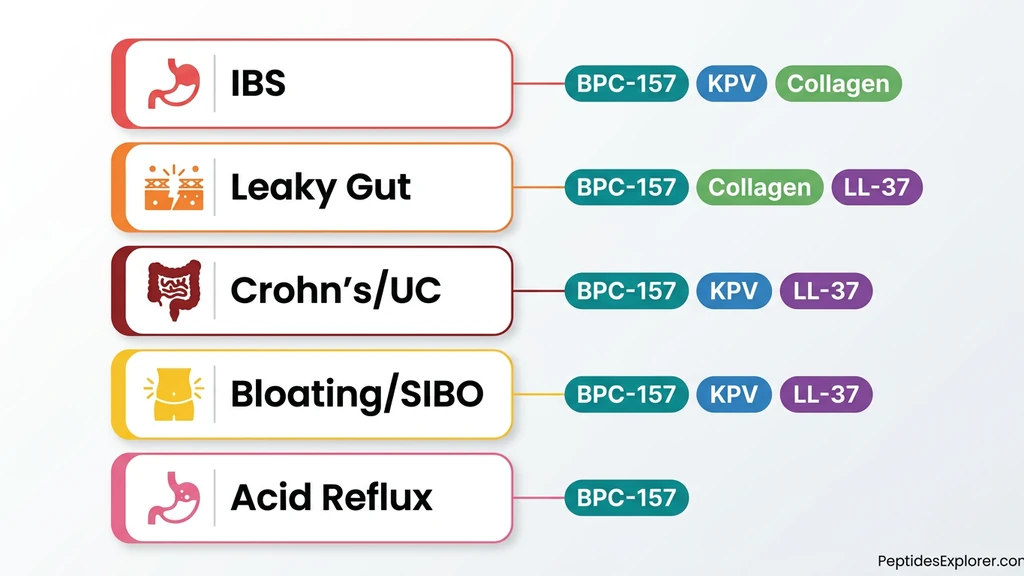
Peptides for IBS (Irritable Bowel Syndrome)
First-line: BPC-157 oral, 250 to 500 mcg per day. BPC-157 addresses mucosal hypersensitivity and promotes tissue repair in the irritated gut lining.
Add KPV (200 to 500 mcg per day oral) if inflammation dominates. Some IBS subtypes involve low-grade inflammation that standard testing misses. KPV's NF-kB suppression calms this background fire.
Collagen peptides (10 to 20 grams per day) serve as foundational support. They supply the raw materials for barrier maintenance. Results from collagen alone take 4 to 6 weeks. Combined with BPC-157, most users report improvement within 2 to 3 weeks.
Peptides for Leaky Gut (Intestinal Permeability)
First-line: BPC-157 oral, 500 mcg per day. BPC-157 stabilizes tight junctions and repairs the physical gaps where permeability occurs.
Add collagen peptides at 15 to 20 grams per day. Glycine and glutamine fuel enterocyte repair and tight junction protein synthesis. Consider LL-37 (100 to 200 mcg per day subcutaneous) if vitamin D levels are low. LL-37 production depends on vitamin D, and deficiency weakens the mucus barrier above the tight junctions.
Larazotide is the most direct tight junction regulator, but it remains unavailable outside research settings. Its Phase 2 trial confirmed the mechanism works in humans.
Peptides for Crohn's Disease and Ulcerative Colitis (IBD)
The gold standard stack: BPC-157 (250 to 500 mcg per day) plus KPV (200 to 500 mcg per day), both oral. BPC-157 handles tissue repair. KPV handles the immune overreaction driving tissue destruction.
LL-37 serves as an adjunct when infection risk is high or when antimicrobial barrier function is compromised. Thymosin Alpha-1 may benefit the immune dysregulation component. It protects against CTLA-4 intestinal immunopathology in preclinical models (PMC7441522).
Critical: IBD patients must work with a gastroenterologist. Peptides are adjuncts to medical treatment. They do not replace biologics, immunomodulators, or surgical intervention when indicated. See BPC-157 Before and After for user-reported gut healing timelines.
Peptides for Bloating and SIBO
BPC-157 oral for motility support and tissue healing. KPV for inflammation caused by bacterial overgrowth. LL-37 for direct antimicrobial action against pathogenic bacteria contributing to the overgrowth.
SIBO requires addressing the root cause: impaired motility, structural abnormalities, or immune deficiency. Peptides heal the damage SIBO causes. They do not cure SIBO itself.
A 2025 systematic review of anti-inflammatory peptides for IBD highlighted the role of peptide-based strategies in managing the inflammatory consequences of bacterial dysbiosis (Ghazvini et al. 2025).
Peptides for Acid Reflux and Gastritis
BPC-157 is the clear choice. It is derived from gastric juice, stable in stomach acid, and specifically studied for gastric protection.
The strongest evidence for BPC-157 comes from NSAID-induced gastric lesion models. The peptide prevents and reverses stomach lining damage caused by ibuprofen, aspirin, and similar drugs. Oral delivery puts the compound directly on the gastric mucosa where damage occurs (PubMed 29998800).
For acid reflux combined with alcohol use, see BPC-157 and Alcohol for specific cytoprotection data.
What Is the BPC-157 + KPV Gut Healing Stack?
The BPC-157 plus KPV combination is the most widely recommended gut healing protocol. BPC-157 functions as the construction crew: it rebuilds damaged tissue, forms new blood vessels, and lays down collagen at wound sites. KPV functions as the fire suppression system: it shuts down the inflammatory signaling that prevents healing from taking hold.
Together, they address both sides of gut damage. Inflammation and structural injury rarely occur in isolation.
The Protocol
BPC-157: 250 to 500 mcg per day, oral, on an empty stomach. KPV: 200 to 500 mcg per day, oral. Duration: 4 to 8 weeks, with reassessment at the 4-week mark.
Start both simultaneously when active inflammation is present. If symptoms improve by week 4, some users taper KPV first and continue BPC-157 alone for the remaining weeks.
Adding collagen peptides (10 to 20 grams per day) provides foundational amino acid support. Adding LL-37 (100 to 200 mcg per day subcutaneous) strengthens antimicrobial defense when infection is a concern.
Cycling and Duration
Standard cycle: 4 to 8 weeks on, 4 weeks off, then reassess. Chronic gut conditions may require multiple cycles.
The off period allows the body's endogenous repair mechanisms to take over. If symptoms return during the off period, a second cycle is warranted. Long-term continuous use of BPC-157 has not been studied in humans.
Use the Peptide Interaction Checker to verify compatibility before adding compounds to this stack. See KPV Dosage Guide for detailed KPV protocols.
Should You Take Gut Peptides Orally or by Injection?
For gut conditions specifically, oral delivery is generally preferred. The reason is direct contact: oral peptides reach the GI lining before systemic absorption dilutes their concentration.
Why Oral Works for Gut Targets
BPC-157 is stable in human gastric juice. Most peptides degrade in stomach acid within minutes. BPC-157 does not. Oral administration delivers the compound directly to the stomach and intestinal lining where damage occurs.
KPV uses the PepT1 transporter in intestinal epithelial cells for uptake. This transporter is upregulated during inflammation, creating a natural targeting mechanism. Sicker tissue absorbs more KPV. Oral KPV at doses as low as 16 mcg/kg/day protected mice from colitis in a nanoparticle delivery study (PMC5498804).
Collagen peptides are oral by nature. No injection option exists or is needed.
When Injectable Makes Sense
Injectable BPC-157 offers higher bioavailability (approximately 90% versus 30 to 50% oral). For systemic conditions that include a gut component, some practitioners combine both routes: oral for local gut effects, subcutaneous for systemic inflammation.
LL-37 is typically administered subcutaneously. Oral LL-37 for gut applications has limited data. Injectable onset is faster: 1 to 2 days for initial effects compared to 1 to 2 weeks for oral peptides.
For a deep dive on oral BPC-157 administration, see Can You Take BPC-157 Orally?.
How Does the Gut-Brain Axis Connect to Peptide Therapy?
The gut produces 90 to 95% of the body's serotonin. Enteroendocrine cells in the intestinal lining release over 30 different peptides that communicate directly with the brain through vagal afferent receptors. The vagus nerve serves as the primary highway between these two organs.
Gut inflammation disrupts vagal signaling. The result: anxiety, depression, brain fog, and mood instability that seem unrelated to digestive symptoms but share a common origin.
BPC-157 and the Brain-Gut Axis
BPC-157 modulates both dopamine and serotonin systems. Sikiric et al. (2023) demonstrated that BPC-157 recovers brain-gut axis function through multiple neurotransmitter pathways (PMC10224484).
A 2017 study mapped the theoretical and practical implications of BPC-157's dual gut-brain activity (PMC5333585). The peptide does not simply heal gut tissue. It restores the signaling cascade between the gut and the brain.
The practical implication: patients who heal their gut with BPC-157 often report improvements in mood, anxiety levels, and cognitive clarity. These are not placebo effects. They are downstream consequences of restored gut-brain communication.
Why This Matters for Treatment
If you experience both gut symptoms and mood or cognitive issues, the connection may be physiological. Treating the gut with BPC-157 and KPV may improve both domains simultaneously.
A 2022 review on the vagus nerve, gut microbiota, and brain axis confirmed that microbial metabolites modulate vagal afferent signaling to influence behavior, stress response, and emotional regulation (PMC9656367).
For readers exploring the anxiety connection specifically, see Peptides for Anxiety, which covers the BPC-157 gut-brain evidence in detail.
Are Peptides for Gut Health Safe?
Safety profiles vary by peptide. The most studied compound (BPC-157) has the strongest safety record. Collagen peptides carry the lowest risk as an established dietary supplement.
General Safety by Peptide
BPC-157. No reported toxicity in preclinical studies. The ACG 2025 systematic review found no adverse effects across organ systems in 36 studies. Half-life under 30 minutes with rapid hepatic metabolism and renal clearance.
KPV. Does not suppress the immune system; it modulates inflammatory signaling. No tanning effect (unlike full-length alpha-MSH). Well-tolerated in animal studies at therapeutic doses.
Collagen peptides. Generally recognized as safe. Widely available as an OTC supplement. Side effects are rare and mild (bloating, aftertaste).
LL-37. Theoretical risk of excessive NETosis (neutrophil extracellular trap formation) at high doses. Requires medical supervision. Not recommended for self-administration without professional guidance.
Is BPC-157 Hard on the Liver?
No. Animal studies show liver-protective effects, not liver damage. BPC-157 is metabolized by the liver with a half-life under 30 minutes and cleared by the kidneys.
The ACG 2025 review specifically assessed multi-organ safety and found no hepatotoxicity signals across 36 studies. Some studies showed BPC-157 actually improved liver function markers in models of liver damage.
See BPC-157 Side Effects for a comprehensive safety analysis.
Critical Disclaimers
Most evidence is preclinical. Animal studies, cell cultures, and early-phase trials form the evidence base. No gut-healing peptide has completed Phase 3 clinical trials in humans for GI conditions.
Larazotide came closest. Its Phase 2 RCT showed significant symptom improvement in celiac patients. Phase 3 was discontinued due to enrollment challenges, not safety signals.
Quality and sourcing matter. Third-party certificate of analysis (COA) verification is essential for any research peptide. Contaminated or underdosed products are a real risk in the peptide market. Work with a qualified healthcare provider, especially for IBD, Crohn's, or any autoimmune gut condition.
Frequently Asked Questions
What peptides repair the gut?
BPC-157 repairs gut tissue through angiogenesis and growth factor expression. KPV reduces intestinal inflammation via NF-kB inhibition. LL-37 protects the gut barrier by preserving goblet cells and mucin production. Collagen peptides supply amino acids for tight junction repair. Larazotide directly regulates tight junction permeability. These five peptides target different healing mechanisms and are often combined for broader coverage.
Is BPC-157 good for your gut?
Yes. BPC-157 is the most studied peptide for gut healing. A 2025 American College of Gastroenterology systematic review of 36 studies confirmed improved outcomes in IBD, GI ulcers, NSAID injury, and fistula models. Oral BPC-157 is preferred for gut conditions because it contacts the GI lining directly and is stable in human gastric juice.
Does BPC-157 really work?
Preclinical evidence is strong: 36 studies reviewed by the ACG show consistent GI healing in animal models. Human clinical trials remain limited, with Phase 2 data for IBD showing a safe profile. Most user reports indicate symptom improvement within 1 to 3 weeks for gut conditions. Long-term controlled human trials are still needed.
Do collagen peptides heal your gut?
Collagen peptides provide glycine, proline, and glutamine, amino acids that support gut barrier function. In vitro studies show they enhance tight junction proteins in Caco-2 intestinal cells. The evidence is more indirect than for BPC-157 or KPV. Typical dosage is 10 to 20 grams per day for at least 6 weeks.
What's the downside of taking peptides?
The main downside is limited human clinical data. Most gut peptide research comes from animal studies. Quality control varies between suppliers, making third-party COA verification essential. Side effects are generally mild (transient nausea, digestive changes) but individual responses vary. Cost is another factor: research peptides are not covered by insurance.
What's better, BPC-157 or TB-500?
For gut health specifically, BPC-157 is better. It is derived from gastric juice and acts directly on the GI lining. TB-500 is a systemic tissue repair peptide that works better for musculoskeletal injuries. For gut healing, the recommended combination is BPC-157 plus KPV rather than BPC-157 plus TB-500.
Is BPC-157 hard on the liver?
No. Animal studies show BPC-157 has liver-protective effects, not liver-damaging ones. It is metabolized by the liver with a half-life under 30 minutes and cleared by the kidneys. The ACG 2025 systematic review found no adverse effects across organ systems in preclinical safety studies spanning three decades.
Can you take BPC-157 orally for gut healing?
Yes. Oral BPC-157 is actually preferred for gut conditions because it contacts the stomach and intestinal lining directly. BPC-157 is stable in human gastric juice, unlike most peptides. Typical oral dosage for gut healing is 250 to 500 mcg once or twice daily on an empty stomach.
How long do peptides take to heal the gut?
BPC-157 users typically report initial gut symptom improvement within 1 to 3 weeks. KPV shows effects within 2 to 4 weeks. Collagen peptides require 4 to 6 weeks for noticeable results. Full mucosal healing takes 6 to 8 weeks or more depending on condition severity. Most protocols run 4 to 8 weeks with reassessment.
Can you stack BPC-157 and KPV together?
Yes. The BPC-157 plus KPV combination is the most widely recommended gut healing stack. BPC-157 drives tissue repair and blood vessel formation. KPV controls the inflammatory environment. Together they address both structural damage and immune overreaction. Typical protocol: BPC-157 250 to 500 mcg per day plus KPV 200 to 500 mcg per day, both oral, for 4 to 8 weeks.
The Bottom Line
Five peptides. Four mechanisms. One goal: rebuild a damaged gut lining and keep it intact.
BPC-157 leads the field with 36 studies and the broadest evidence base. KPV targets inflammation with precision through the PepT1 self-targeting mechanism. Collagen peptides offer the lowest barrier to entry. LL-37 defends against pathogens while preserving beneficial flora. Larazotide proved in human trials that tight junction regulation works.
For most gut conditions, the BPC-157 plus KPV oral stack is the starting point. Add collagen peptides as foundational support. Add LL-37 when antimicrobial defense is needed. Match the peptide to the condition, not the other way around.
The gut-brain axis adds another dimension. Healing the gut may improve mood, anxiety, and cognitive function through restored vagal signaling and serotonin production. The connection is biological, not theoretical.
All evidence cited here links to its source. Most of it is preclinical. Human trials are underway but incomplete. Work with a qualified healthcare provider. Verify peptide quality through third-party COA testing.
Take the Peptide Quiz to identify which peptides fit your goals, or explore individual peptide profiles for BPC-157, KPV, and LL-37. For all dosage references, see the peptide dosage chart. For reconstitution, see how to reconstitute peptides. For proper storage, see how to store peptides. For sourcing, see where to buy peptides in 2026. For overall safety, see the peptide safety guide. For stacking principles, see the peptide stacking guide. New to peptides? Start with our getting started with peptides guide.
Related Articles: - BPC-157 Side Effects - KPV Peptide Dosage - LL-37 Peptide Benefits - Thymosin Alpha-1 Benefits - Peptide Stacking Guide - BPC-157 and Alcohol
KPV is the tripeptide behind most of the gut-repair claims. KPV peptide benefits ranks what the colitis models actually support.
Related Articles
BPC-157 Oral Pills & Capsules: Do They Work?
BPC-157 oral pills deliver 250-500 mcg to the gut. Oral vs injectable vs nasal comparison, dosing protocols, and sourcing guidance.
Peptides for Healing: What the Evidence Shows
Peptides for healing by tissue: tendon, bone, wound, gut, post-surgery. Which claims rest on human trials, which rest on rat studies, and what is unsafe.
KLOW Peptide: Benefits, Dosage, and KLOW vs GLOW
KLOW peptide benefits, blend composition (GHK-Cu, BPC-157, TB-500, KPV), per-component dosing math, the copper ceiling, and how KLOW differs from GLOW.
KPV Peptide Benefits: What the Evidence Shows
KPV peptide benefits ranked by evidence: strong preclinical colitis data, plausible skin effects, weak systemic claims. No registered human trial exists.