
You just started tirzepatide (Mounjaro, Zepbound) and your medicine cabinet holds six other bottles. Tirzepatide has 427 known drug interactions, 16 classified as major. The primary mechanism: tirzepatide slows gastric emptying by 30 to 40%, altering the absorption of nearly every oral medication you take. The most clinically significant interactions involve oral contraceptives (59% reduction in ethinyl estradiol Cmax), insulin and sulfonylureas (additive hypoglycemia), warfarin (INR instability), and levothyroxine (delayed absorption). Most interactions are manageable with timing adjustments or monitoring, but a few require medication changes (FDA Prescribing Information, 2025).
| Interaction Risk | Medications | Key Concern |
|---|---|---|
| Major | Oral contraceptives | 59% Cmax reduction (ethinyl estradiol), 66% (norgestimate) |
| Major | Insulin, sulfonylureas | Additive hypoglycemia |
| Major | Warfarin | INR fluctuation during titration |
| Moderate | Levothyroxine | Delayed absorption (total uptake preserved) |
| Moderate | SSRIs/antidepressants | Overlapping nausea, no PK interaction |
| Moderate | Blood pressure medications | Hypotension from weight loss |
| Moderate | Acetaminophen | 50 to 55% Cmax reduction after first dose |
| Low | PPIs, statins, antihistamines | Minimal clinical effect |
Check your specific medications with our peptide interaction checker. For dosing guidance, see our tirzepatide dosage chart.
Not FDA-approved for use outside labeled indications. Consult a healthcare provider before combining tirzepatide with any prescription or over-the-counter medication.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
How Tirzepatide Causes Drug Interactions: The Gastric Emptying Mechanism
Tirzepatide activates both GLP-1 and GIP receptors. GLP-1 receptor activation slows gastric motility, keeping food and medications in the stomach 30 to 40% longer than normal. This delay changes how fast oral drugs reach the small intestine, where most absorption occurs.
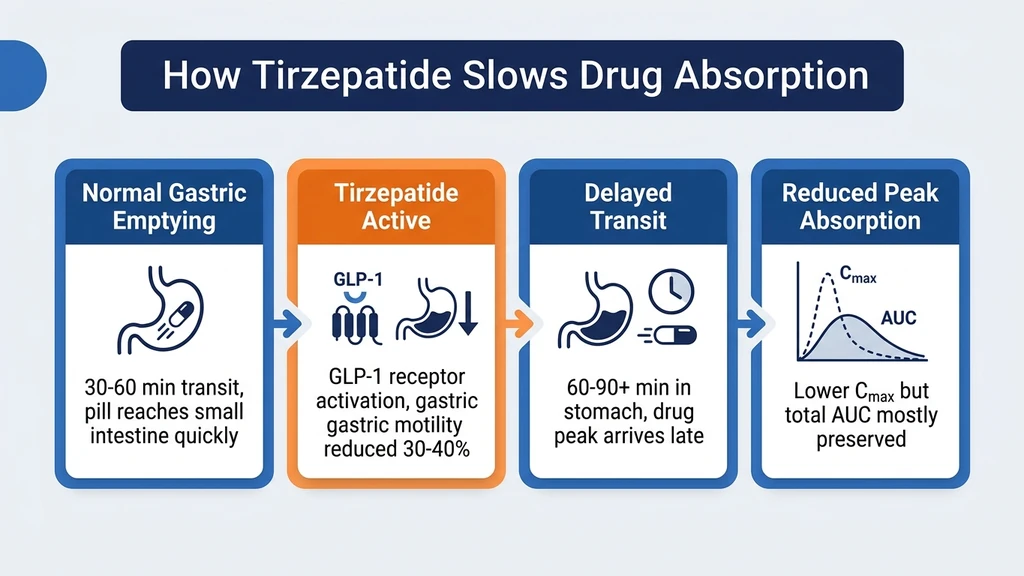
Think of your stomach as a waiting room. Normally, an oral medication passes through in 30 to 60 minutes and reaches the absorption site in the small intestine. Tirzepatide extends that wait to 60 to 90 minutes or longer. The medication still gets absorbed, but the peak concentration arrives later and lower.
The acetaminophen pharmacokinetic study in tirzepatide's FDA label quantifies this precisely. After the first tirzepatide dose, acetaminophen Cmax dropped 50 to 55% and Tmax shifted from 0.5 hours to 2.5 hours (FDA Prescribing Information, 2025). Total absorption (AUC) decreased only 15 to 20%. The drug still gets in; it just arrives late and at a lower peak.
The Tachyphylaxis Effect: First Dose Hits Hardest
Gastric emptying delay is greatest after the first dose of tirzepatide and diminishes with continued use. This tachyphylaxis effect means drug interactions are most intense during the first 4 to 8 weeks at each dose level and after each dose escalation.
At steady state (approximately 4 weeks at a stable dose), the gastric emptying delay partially normalizes. The acetaminophen Cmax reduction of 50 to 55% after the first dose drops to approximately 20% at steady state on the 5 mg dose (FDA Prescribing Information, 2025). This is why the FDA recommends extra monitoring during initiation and dose increases rather than throughout the entire treatment course.
Why Tirzepatide Does Not Interact Through CYP450 Enzymes
Most drug interactions in pharmacology occur through hepatic CYP450 enzymes. Tirzepatide does not use this pathway. It is metabolized by proteolytic cleavage (enzymes that break peptide bonds), not by liver enzymes. In vitro testing shows minimal CYP450 inhibition or induction potential at therapeutic concentrations (PMC, 2025).
This means tirzepatide does not interfere with how your liver processes other drugs. The only meaningful interaction mechanism is delayed gastric emptying. That single mechanism, however, affects every oral medication you swallow while on tirzepatide.
Major Drug Interactions (High Risk)
Three medication categories carry the highest interaction risk with tirzepatide. Each can produce clinically meaningful consequences that require monitoring or intervention.
Oral Contraceptives: Reduced Effectiveness
This is the most clinically important interaction. Tirzepatide reduces ethinyl estradiol Cmax by 59% and AUC by 20%. Norgestimate (the progestin component) Cmax drops 66%, with AUC reduced 21% (JAPh, 2023).
A 59% Cmax reduction is substantial. Oral contraceptives rely on sustained hormone levels to suppress ovulation. When peak levels drop by more than half, the contraceptive effect weakens. The FDA prescribing information recommends switching to a non-oral contraceptive method (IUD, implant, patch, or ring) or adding a barrier method during tirzepatide use.
If switching is not possible, use backup contraception for at least 4 weeks after starting tirzepatide and for 4 weeks after each dose escalation. These are the periods when gastric emptying delay, and therefore the interaction severity, is greatest.
Insulin and Sulfonylureas: Hypoglycemia Risk
Tirzepatide lowers blood glucose through GLP-1 and GIP receptor activity. Combining it with insulin or sulfonylureas (glimepiride, glipizide, glyburide) creates additive hypoglycemia risk. The SURPASS trial program documented this interaction clearly (Del Prato et al., Lancet, 2021).
Most prescribers reduce insulin doses by 20 to 30% when initiating tirzepatide. Sulfonylurea dose reduction or discontinuation is common practice. Self-monitoring of blood glucose should increase to at least twice daily during titration.
Hypoglycemia symptoms: shakiness, sweating, confusion, rapid heartbeat, and dizziness. Users on insulin or sulfonylureas should keep fast-acting glucose (tablets, juice) accessible at all times during the first 8 weeks of tirzepatide.
Warfarin and Anticoagulants: INR Monitoring Required
Warfarin has a narrow therapeutic index. Small changes in absorption timing can shift INR (International Normalized Ratio) outside the therapeutic range, increasing bleeding or clotting risk.
Tirzepatide delays warfarin absorption without reducing total exposure. The problem: INR fluctuates during dose titration as gastric emptying patterns shift. Weekly INR monitoring for the first 4 to 8 weeks of tirzepatide, and after each dose increase, is the standard recommendation.
Direct oral anticoagulants (DOACs) like apixaban and rivaroxaban face theoretical absorption delays. No published pharmacokinetic study has quantified this interaction for tirzepatide specifically. Monitor for signs of reduced anticoagulant effect (unexpected bruising patterns, clot symptoms) during initiation and discuss DOAC timing with your prescriber.
Moderate Drug Interactions
Moderate interactions are manageable with timing adjustments or monitoring. They rarely require medication changes but warrant awareness during tirzepatide initiation.
Levothyroxine: Timing Is the Solution
Levothyroxine has a narrow therapeutic window and its absorption depends on an empty stomach. Tirzepatide's gastric emptying delay can shift levothyroxine absorption timing, affecting thyroid levels during titration.
The solution is straightforward: take levothyroxine at least 60 minutes before eating and before your tirzepatide dose. Morning levothyroxine on an empty stomach, followed by a 60-minute wait before breakfast, maintains the standard absorption window. Monitor TSH every 6 to 8 weeks during tirzepatide dose escalation. Total levothyroxine absorption (AUC) is unlikely to change significantly; only the timing shifts. Most patients do not need dose adjustments.
Metformin: No Significant Interaction
Good news for the most common combination: no significant pharmacokinetic interaction exists between tirzepatide and metformin. Metformin is absorbed in the small intestine and is not hepatically metabolized. The combination is the most common pairing in type 2 diabetes management.
The SURPASS trials used metformin as background therapy in most treatment arms with no interaction signal (Del Prato et al., Lancet, 2021). No dose adjustment is needed. No special timing is required. Continue metformin on your normal schedule.
SSRIs and Antidepressants
SSRIs (sertraline, escitalopram, fluoxetine) are among the most commonly co-prescribed medications with tirzepatide. No direct pharmacokinetic interaction exists because SSRIs are metabolized through CYP450 enzymes, and tirzepatide does not affect CYP pathways.
The practical concern is overlapping nausea. SSRIs cause nausea during initiation, and tirzepatide's GI side effects peak during the same early weeks. Starting both simultaneously amplifies nausea. Stabilize one medication before starting the other when possible.
A real-world cohort study found no increased psychiatric adverse events with tirzepatide compared to non-GLP-1 controls (PMC, 2025). No SSRI dose adjustment is needed.
Blood Pressure Medications
Tirzepatide causes weight loss, and weight loss reduces blood pressure. Patients on ACE inhibitors, ARBs, or beta-blockers may experience symptomatic hypotension (dizziness, lightheadedness) as they lose weight.
A study in the Journal of the American Pharmacists Association highlighted cases of symptomatic hypotension in heart failure patients on guideline-directed medical therapy who started tirzepatide (JAPh, 2023). Blood pressure medication dose reduction may be needed after 10 to 15% body weight loss. Monitor blood pressure weekly during active weight loss phases.
NSAIDs: Delayed Onset, Preserved Total Effect
Tirzepatide delays NSAID absorption, slowing pain relief onset by 30 to 60 minutes. Total anti-inflammatory exposure is not significantly reduced. Short-term NSAID use for headaches or muscle pain is generally safe.
The GI concern matters more than the PK concern. Both tirzepatide and NSAIDs stress the gastric mucosa. Prolonged NSAID use while on tirzepatide increases the risk of nausea, stomach pain, and erosive gastritis. Use acetaminophen as a first-line pain reliever when possible, keeping in mind its own Cmax reduction of 50 to 55% after the first tirzepatide dose.
Acetaminophen: Delayed Peak, Not Reduced Overall
The FDA prescribing information includes dedicated pharmacokinetic data for acetaminophen. After the first tirzepatide dose, acetaminophen Cmax dropped 50 to 55% and Tmax shifted from 0.5 hours to 2.5 hours. At steady state on 5 mg tirzepatide, the Cmax reduction moderated to approximately 20%.
Total absorption (AUC) was only modestly reduced (15 to 20%). Pain relief from acetaminophen is delayed, not eliminated. If you take acetaminophen for a headache while on tirzepatide, expect it to work more slowly than usual. Taking it 30 minutes earlier than you normally would compensates for the absorption delay.
Statins: No Clinically Significant Interaction
Statins (atorvastatin, rosuvastatin, simvastatin) face a theoretical absorption delay from slowed gastric emptying. No clinically significant interaction has been documented in the tirzepatide clinical program or the FAERS database. No dose adjustment is needed. Continue statins on your normal schedule.
Statin metabolism occurs primarily through CYP3A4 and other hepatic enzymes, which tirzepatide does not affect (PMC, 2025). The minor absorption delay has no meaningful impact on statin efficacy.
Low-Risk Interactions
Several commonly used medication classes have minimal interaction risk with tirzepatide.
| Medication Class | Specific Agents | Risk | Notes |
|---|---|---|---|
| Proton pump inhibitors | Omeprazole, pantoprazole | Low | May help manage tirzepatide GI side effects |
| Multivitamins and supplements | Standard formulations | Low | Fat-soluble vitamins may absorb slightly slower |
| Standard antibiotics | Amoxicillin, azithromycin | Low | Minor delay not clinically significant |
| Antihistamines | Cetirizine, loratadine | Low | Wide therapeutic window, delay irrelevant |
| SGLT2 inhibitors | Empagliflozin, dapagliflozin | Low | Renal mechanism, independent of GI absorption |
| Inhaled medications | Asthma, COPD inhalers | None | Pulmonary absorption, unaffected |
| Topical medications | Creams, patches, eye drops | None | No GI component |
PPIs may actually help manage the GI side effects (nausea, acid reflux) that tirzepatide causes during dose escalation. There is no pharmacokinetic interaction to manage.
Alcohol and Tirzepatide
Alcohol does not interact with tirzepatide through a pharmacokinetic mechanism. No enzyme competition or absorption interference exists. The concerns are pharmacodynamic.
Alcohol amplifies GI side effects. Both tirzepatide and alcohol irritate the stomach lining. Combining them increases nausea, vomiting, and acid reflux risk. Users report worse hangovers and lower alcohol tolerance during tirzepatide treatment.
Alcohol causes hypoglycemia in users on insulin or sulfonylureas. The liver prioritizes alcohol metabolism over glucose production, creating a triple blood sugar suppression when combined with tirzepatide and an insulin secretagogue.
Alcohol also undermines weight loss goals. One glass of wine adds 120 to 150 calories that tirzepatide cannot offset. For a deeper dive, see our guide on alcohol and tirzepatide.
Interactions During Dose Escalation vs Steady State
The intensity of drug interactions changes as your dose increases and your body adapts.
Weeks 1 to 4 at each new dose: highest interaction risk. Gastric emptying delay peaks during this window. The acetaminophen data demonstrates this: 50 to 55% Cmax reduction after the first dose, 20% at steady state. All oral medication interactions follow this same pattern.
Steady state (4+ weeks at a stable dose): reduced interaction risk. Tachyphylaxis partially restores gastric motility. Interactions persist but at lower intensity. This is why most prescribers schedule monitoring (INR for warfarin, TSH for levothyroxine, blood glucose for insulin) most frequently during titration.
The standard tirzepatide escalation is 2.5 mg for 4 weeks, then 5 mg for 4 weeks, then 7.5, 10, 12.5, and 15 mg at 4-week intervals. Each dose increase resets the interaction clock. A patient reaching 15 mg has cycled through 5 to 6 interaction peaks over 20 to 24 weeks. See our tirzepatide dosage chart for the full escalation timeline.
Medications That Do NOT Interact with Tirzepatide
Several common medication classes have been confirmed safe to combine with tirzepatide based on clinical trial data and pharmacological analysis.
| Medication | Why No Interaction | Notes |
|---|---|---|
| Metformin | Not hepatically metabolized; small intestine absorption unaffected | Most common co-prescription in T2D |
| SGLT2 inhibitors | Renal mechanism, independent of GI absorption | Empagliflozin, dapagliflozin, canagliflozin |
| Injectable medications | Bypass GI tract entirely | Includes insulin (adjust dose, but no absorption interaction) |
| Topical medications | No GI component | Creams, patches |
| Inhaled medications | Pulmonary absorption | Asthma and COPD inhalers unaffected |
Tirzepatide shows low CYP enzyme inhibition in vitro. It does not significantly inhibit or induce CYP1A2, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6, or CYP3A4 at therapeutic concentrations. Drug transporter inhibition is also minimal (PMC, 2025). The gastric emptying delay is the sole meaningful interaction pathway for tirzepatide.
How to Manage Drug Interactions
Two strategies cover most interaction scenarios: timing adjustments and monitoring schedules.
Timing Strategies
Narrow therapeutic index drugs (warfarin, levothyroxine, phenytoin): Take these at least 1 hour before tirzepatide, ideally first thing in the morning before food. This gives the medication a head start on absorption before gastric emptying slows.
Oral contraceptives: Switch to a non-oral method (IUD, implant, ring, patch) during tirzepatide treatment. If switching is not feasible, add barrier contraception for the first 4 weeks and after each dose increase.
Pain medications: Expect delayed onset. Take acetaminophen or NSAIDs 30 minutes earlier than usual to compensate for the absorption delay.
General principle: Any oral medication requiring rapid, predictable absorption should be taken first thing in the morning, at least 1 hour before tirzepatide and food. Medications with wide therapeutic windows (statins, antihistamines, PPIs) can be taken at any time without adjustment.
Monitoring Schedule
| Co-Medication | Monitor | Frequency During Titration | Frequency at Steady State |
|---|---|---|---|
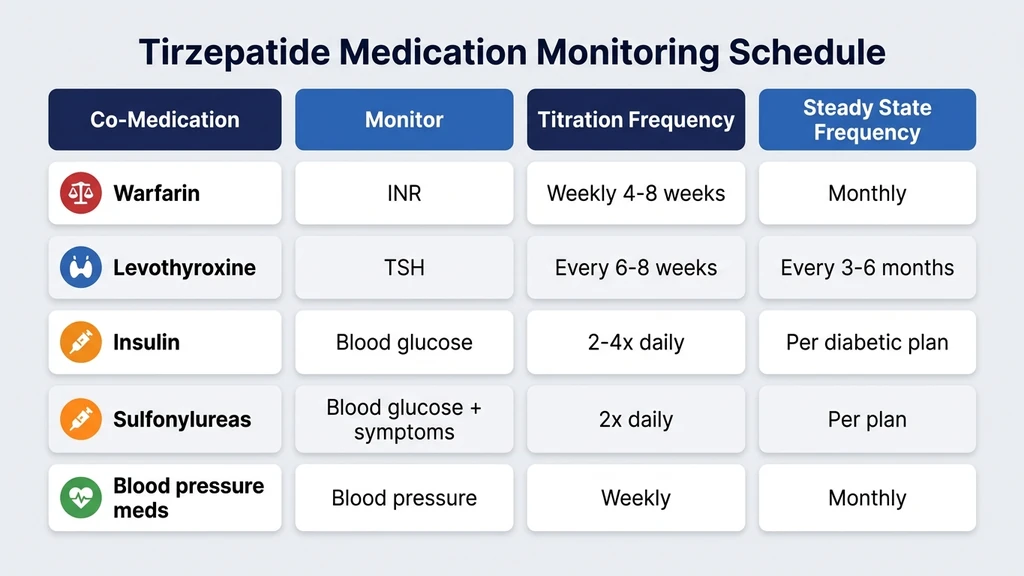
| Warfarin | INR | Weekly for 4 to 8 weeks | Monthly |
| Levothyroxine | TSH | Every 6 to 8 weeks | Every 3 to 6 months |
| Insulin | Blood glucose | 2 to 4x daily | Per diabetic management plan |
| Sulfonylureas | Blood glucose + symptoms | 2x daily | Per management plan |
| Blood pressure meds | Blood pressure | Weekly | Monthly |
| Oral contraceptives | Pregnancy test if concerned | As needed | N/A (switch method recommended) |
Use our peptide interaction checker to screen your current medications against tirzepatide. For systemic safety context, see our tirzepatide long-term side effects guide. If you are switching from semaglutide, review our semaglutide to tirzepatide switching guide for transition considerations. For complete tirzepatide safety information on compound formulations, see our dedicated guide.
Frequently Asked Questions
What medications should I avoid while taking tirzepatide?
No medication is absolutely contraindicated with tirzepatide, but oral contraceptives require backup protection (59% Cmax reduction in ethinyl estradiol). Insulin and sulfonylurea doses typically need 20 to 30% reduction to prevent hypoglycemia. Warfarin requires weekly INR monitoring during titration. Most interactions are manageable with timing adjustments. Use our peptide interaction checker to screen your full medication list.
Can I take metformin with tirzepatide?
Yes. Metformin and tirzepatide have no significant pharmacokinetic interaction. Metformin is absorbed in the small intestine and is not hepatically metabolized. The SURPASS trials used metformin as background therapy in most arms with no safety signal. No dose adjustment or special timing is needed. This is the most common tirzepatide combination in clinical practice for type 2 diabetes management.
Does tirzepatide affect birth control?
Yes. Tirzepatide reduces ethinyl estradiol Cmax by 59% and norgestimate Cmax by 66% through delayed gastric emptying (JAPh, 2023). The FDA recommends switching to non-oral contraception (IUD, implant, patch, ring) or adding barrier methods during tirzepatide use. Extra caution applies during the first 4 weeks and for 4 weeks after each dose escalation when the interaction is strongest.
Can I take ibuprofen with Mounjaro?
Yes, for short-term use. Tirzepatide delays ibuprofen absorption by 30 to 60 minutes, so pain relief arrives slower. Total anti-inflammatory exposure is preserved. The GI concern matters more: both tirzepatide and ibuprofen irritate the stomach lining, increasing nausea and erosion risk with prolonged use. Consider acetaminophen as a first-line alternative, though acetaminophen itself has a 50 to 55% Cmax reduction after the first tirzepatide dose.
Does tirzepatide interact with thyroid medication?
Tirzepatide delays levothyroxine absorption but does not reduce total uptake. Take levothyroxine at least 60 minutes before food and tirzepatide. Monitor TSH every 6 to 8 weeks during dose escalation. At steady state, levothyroxine absorption normalizes. Most patients do not need dose changes, but TSH monitoring during titration catches the exceptions. For broader tirzepatide safety data, see our long-term side effects guide.
Can I take antidepressants with tirzepatide?
Yes. SSRIs and most antidepressants are metabolized through CYP450 enzymes, and tirzepatide does not affect CYP pathways. No dose adjustment is needed. The practical concern is overlapping nausea during the early weeks of both medications. A real-world cohort study found no increased psychiatric adverse events with tirzepatide use (PMC, 2025). Stabilize one medication before starting the other when possible.
What happens if I take medications too close to my tirzepatide dose?
Oral medications taken within 1 to 2 hours of tirzepatide may experience delayed and reduced peak absorption. For most medications with wide therapeutic windows (statins, antihistamines), this has no clinical consequence. For narrow therapeutic index drugs (warfarin, levothyroxine), the timing gap matters. Take critical medications first thing in the morning, at least 60 minutes before tirzepatide and food. See the tirzepatide dosage chart for the weekly injection schedule.
The Bottom Line
Tirzepatide's 427 drug interactions stem from a single mechanism: delayed gastric emptying. This makes the interaction profile manageable. Oral contraceptives require the most attention (switch to non-oral methods or add barrier protection). Insulin and sulfonylureas need dose reductions of 20 to 30%. Warfarin demands weekly INR monitoring during titration. Levothyroxine timing should be separated from food by 60 minutes.
Most interactions peak during the first 4 weeks at each dose level and moderate at steady state. The tachyphylaxis effect means long-term tirzepatide users face less interaction intensity than new starters. Tirzepatide does not affect CYP450 enzymes, so hepatically metabolized drugs are unaffected.
Use our peptide interaction checker to screen your full medication list. For monitoring schedules at each dose, use our tirzepatide dosage calculator. For broader safety data at 72 weeks, see our tirzepatide long-term side effects guide. For information on tirzepatide with B12 supplementation, see our dedicated article.
Related Articles
Tirzepatide: How Long in Your System?
Tirzepatide has a half-life of ~5 days and takes ~25 days to fully clear your system. See the elimination timeline and factors affecting clearance.
Cheapest Tirzepatide: Every Route Priced (2026)
The cheapest tirzepatide in 2026: manufacturer self-pay vials from $299/month, $25 insured copays, true cost per milligram, and why compounded copies ended.
Does Tirzepatide Help With Inflammation?
Does tirzepatide help with inflammation? Yes: CRP drops 32.9%, IL-6 drops 17.8% in trials. SURMOUNT data and adipose tissue mechanisms.
Does Compounded Tirzepatide Work? Real Data
Does compounded tirzepatide work? Review SURMOUNT data, salt form differences (base, acetate, sodium), potency gaps, and FDA status in 2026.