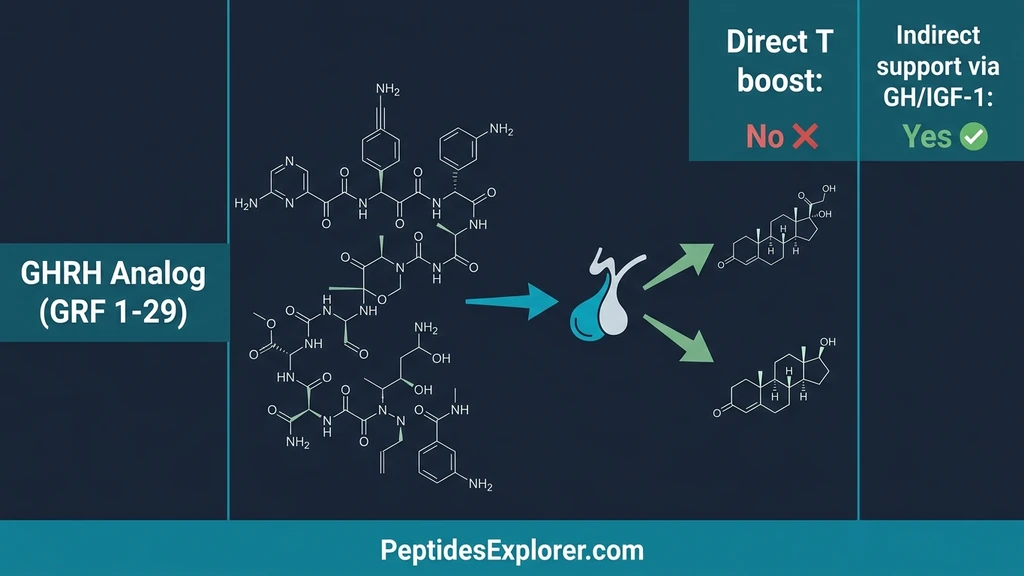
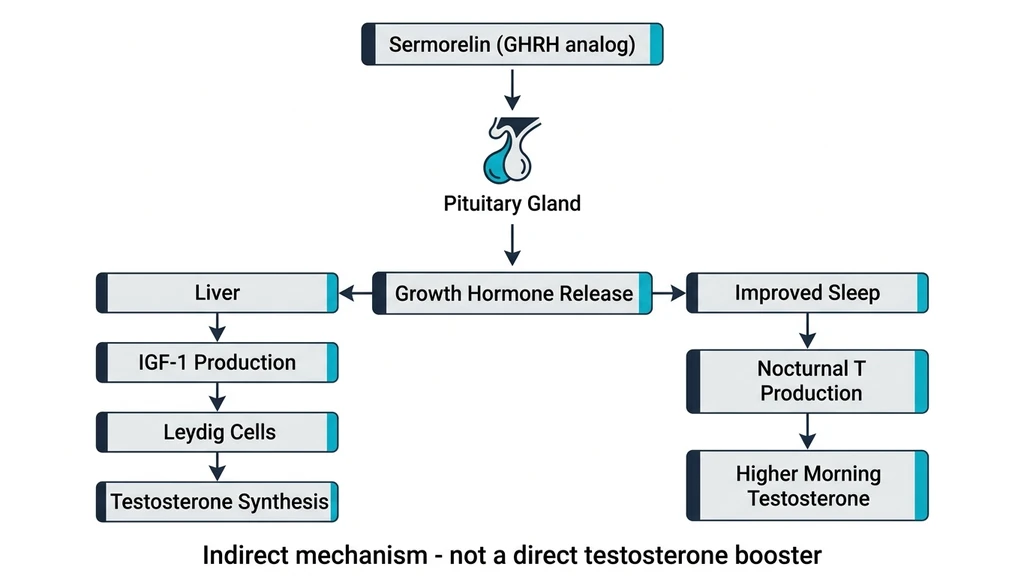
Your testosterone has been declining by roughly 1-2% per year since your early thirties, and someone suggested sermorelin might reverse the slide. Sermorelin does not directly increase testosterone. It is a growth hormone-releasing hormone (GHRH) analog that stimulates your pituitary gland to produce more growth hormone (GH), and the resulting GH and IGF-1 elevation can support testosterone production indirectly through effects on Leydig cell function and sleep architecture (Walker, Clin Interv Aging, 2006).
That distinction between "direct" and "indirect" is not semantic hair-splitting. It determines whether sermorelin alone will solve a testosterone problem, whether you need testosterone replacement therapy (TRT) instead, or whether combining the two produces results neither achieves alone. This article examines the clinical evidence for each pathway, quantifies the magnitude of any testosterone effect, and explains when sermorelin belongs in a male hormone optimization protocol.
| Quick Reference | Details |
|---|---|
| Does sermorelin directly raise testosterone? | No. It has no androgen receptor activity. |
| Does it indirectly support testosterone? | Yes, via GH/IGF-1 effects on Leydig cells and improved sleep |
| Magnitude of indirect T effect | Modest: 10-15% improvement in some studies, not statistically significant in most |
| Who benefits most? | Men with concurrent GH decline and borderline-low testosterone |
| Better option for low T? | TRT for clinically low testosterone; sermorelin for GH-related symptoms |
| Can you combine sermorelin + TRT? | Yes. Synergistic effects on body composition documented |
| FDA status | Previously approved (Geref, 1997); withdrawn 2008 for manufacturing reasons |
For sermorelin dosing specifics, read how much sermorelin per day. To understand injection technique, see our where to inject sermorelin guide.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
How Sermorelin Works: GHRH, Not Testosterone
Understanding why sermorelin cannot directly raise testosterone requires understanding what it actually does at the molecular level. Sermorelin is a synthetic version of the first 29 amino acids of growth hormone-releasing hormone (GHRH 1-29), the signaling peptide your hypothalamus secretes to tell the pituitary gland to release growth hormone. The full GHRH molecule contains 44 amino acids, but researchers at Tulane University demonstrated that only the first 29 retain full biological activity (Ling et al., Biochem Biophys Res Commun, 1984).
When injected subcutaneously, sermorelin binds exclusively to GHRH receptors on somatotroph cells in the anterior pituitary. These are G-protein coupled receptors that initiate a cAMP signaling cascade, culminating in growth hormone secretion into the bloodstream (Mayo, Mol Endocrinol, 1992). Sermorelin has zero affinity for androgen receptors, luteinizing hormone receptors, or follicle-stimulating hormone receptors. It physically cannot bind to the same targets that testosterone or testosterone-boosting compounds use.
Think of sermorelin as a factory manager who walks into the growth hormone production floor and increases output. That manager has no authority over the testosterone production floor in a different building. However, the two buildings share supply chains and delivery routes, and increased activity in one can create ripple effects in the other. Those ripple effects are the indirect pathways we will examine next.
For a deeper exploration of sermorelin's classification, see is sermorelin a steroid, which details the molecular differences between peptides and androgens.
The GH-Testosterone Axis: How Growth Hormone Supports Testosterone Indirectly
Growth hormone and testosterone are not independent systems. They share regulatory pathways, amplify each other's effects, and decline in tandem during aging. The relationship between GH and testosterone operates through at least four distinct mechanisms, each with varying levels of clinical evidence.
Pathway 1: IGF-1 and Leydig Cell Stimulation
When sermorelin stimulates GH release, the liver converts much of that GH into insulin-like growth factor 1 (IGF-1). IGF-1 receptors are present on Leydig cells, the testicular cells responsible for testosterone synthesis. Binding of IGF-1 to these receptors enhances the sensitivity of Leydig cells to luteinizing hormone (LH) and increases steroidogenic enzyme activity (Frontiers in Endocrinology, 2019).
In animal models, GH-deficient rats treated with sermorelin showed increased testosterone secretion, and IGF-1 administration directly stimulated Leydig cell testosterone output. The mechanism is clear: IGF-1 upregulates the number of LH receptors on Leydig cells, amplifying the signal that triggers testosterone production. More LH receptors means each LH pulse produces a stronger testosterone response.
The limitation: human data confirming this pathway is sparse. In elderly men, serum testosterone levels showed a positive correlation with 24-hour mean GH levels, but the improvements in testosterone were not statistically significant in most studies (Sinha et al., Transl Androl Urol, 2020). The pathway exists, but its magnitude in living humans may be clinically marginal for men whose testosterone deficit has primary testicular causes rather than secondary GH-related causes.
Pathway 2: FSH and LH Stimulation
One of the more intriguing findings in GH secretagogue research is that sermorelin uniquely stimulated both follicle-stimulating hormone (FSH) and luteinizing hormone (LH) release in clinical observations (Sinha et al., Transl Androl Urol, 2020). FSH and LH are the pituitary gonadotropins that directly regulate testicular function. LH binds Leydig cells to trigger testosterone synthesis. FSH drives spermatogenesis in Sertoli cells.
If sermorelin genuinely raises LH output, it would stimulate endogenous testosterone production through the same pathway your body already uses, without the hypothalamic-pituitary-testicular axis (HPTA) suppression that exogenous testosterone causes. This is the theoretical advantage that makes sermorelin attractive for men with borderline testosterone who want to preserve fertility.
However, the evidence supporting this pathway remains preliminary. The LH/FSH stimulation was observed in a clinical setting but has not been confirmed in large, controlled trials. Future studies are needed to determine whether this effect is robust enough to produce meaningful testosterone increases in hypogonadal men. For men exploring fertility-preserving options, read peptides for men for a broader overview.
Pathway 3: Sleep Architecture and Nocturnal Testosterone
Roughly 65-70% of daily testosterone secretion occurs during sleep, with the highest pulses during REM stages. Growth hormone also follows a sleep-dependent release pattern, with the largest GH pulse occurring within the first 90 minutes of slow-wave sleep. These two nocturnal hormone surges are not coincidental; they share overlapping regulatory mechanisms.
Sermorelin improves sleep quality, particularly deep sleep stages, through its effects on GH pulsatility. Better sleep architecture means more time in the restorative stages where testosterone production peaks. A man sleeping five hours per night produces significantly less testosterone than the same man sleeping seven to eight hours. Sermorelin does not fix poor sleep habits, but by normalizing GH pulsatility, it may restore the hormonal environment that supports robust nocturnal testosterone output.
This pathway is especially relevant for men over 40 whose GH decline has disrupted sleep quality, creating a vicious cycle: low GH leads to poor sleep, poor sleep leads to lower testosterone, and lower testosterone leads to worse sleep. Sermorelin can interrupt this cycle at the GH node. For specific age-related strategies, see our guides on peptides for men over 40 and how long sermorelin takes to work.
Pathway 4: Body Composition and Aromatase Reduction
Visceral fat contains high concentrations of aromatase, the enzyme that converts testosterone to estradiol. More belly fat means more aromatase activity, which means more testosterone converted to estrogen. This is one reason obesity and low testosterone correlate so strongly.
Sermorelin's most well-documented clinical effect is improved body composition: reduced visceral fat and increased lean mass (Vittone et al., J Gerontol A Biol Sci Med Sci, 1997). By reducing the visceral fat depot, sermorelin indirectly reduces aromatase activity, preserving more free testosterone. A man who loses 15 pounds of visceral fat through GH-driven lipolysis may see his testosterone rise 50-100 ng/dL purely from reduced aromatization.
This pathway produces the most visible testosterone-adjacent benefits for overweight men. It is also the pathway with the strongest clinical evidence, because the body composition effects of GH are well-established. Read our detailed breakdown in sermorelin for fat loss for dosing protocols specific to fat reduction.
Clinical Evidence: What the Studies Actually Show
The honest answer is that no randomized controlled trial has demonstrated that sermorelin significantly raises serum total testosterone in men. Several studies have explored related endpoints, and their findings range from suggestive to null.
The Sigalos 2017 Study: GH Secretagogues in Hypogonadal Men
The most relevant study to this question is a retrospective review by Sigalos et al. published in the American Journal of Men's Health. Researchers examined 105 hypogonadal men already on testosterone therapy who were prescribed a combination of GH secretagogues (GHRP-6, GHRP-2, and sermorelin) at 100 mcg each, injected subcutaneously three times daily (Sigalos et al., Am J Mens Health, 2017).
Key findings: - IGF-1 increased significantly in the treatment group - Lean body mass increased and body fat percentage decreased - Testosterone levels were not independently measured as a primary endpoint because all subjects were already on TRT
This study demonstrates that GH secretagogues (including sermorelin) enhance body composition in men on testosterone therapy, but it cannot tell us whether sermorelin alone would raise testosterone. The combination was synergistic for body composition, which is a clinically useful finding even if it does not answer the testosterone question directly.
The Walker 2006 Review: Sermorelin for Adult GH Insufficiency
Walker's comprehensive review in Clinical Interventions in Aging examined sermorelin as a treatment for adult-onset GH insufficiency. The review confirmed that sermorelin increases GH and IGF-1 levels while preserving physiological pulsatile secretion patterns (Walker, Clin Interv Aging, 2006).
Regarding testosterone: the review noted that in elderly men, serum testosterone correlated positively with 24-hour mean GH levels. However, sermorelin-induced improvements in testosterone were not statistically significant. The correlation exists, but the causation is not strong enough to claim sermorelin is a testosterone treatment.
This review also highlighted that sermorelin improved body composition, exercise capacity, and sleep quality, all of which are commonly attributed to testosterone when men report "feeling better" on sermorelin. The subjective experience of improved vitality may owe more to GH restoration than to any testosterone change.
The Sinha 2020 Review: GH Secretagogues and Hypogonadism
Sinha and colleagues published a narrative review in Translational Andrology and Urology examining the role of GH secretagogues in hypogonadal men. The authors noted that sermorelin uniquely stimulated both FSH and LH release, implying a potential role in hypogonadism treatment via endogenous testosterone stimulation (Sinha et al., Transl Androl Urol, 2020).
However, the review concluded that future large, longitudinal studies are needed to better characterize sermorelin's complementary role in managing hypogonadal men. The evidence base remains insufficient to recommend sermorelin as a standalone testosterone treatment. The authors positioned GH secretagogues as body composition tools that complement TRT rather than replace it.
For context on how sermorelin compares to other GH secretagogues, see tesamorelin vs. sermorelin vs. ipamorelin.
Sermorelin vs. TRT: Different Tools for Different Problems
Comparing sermorelin to TRT is like comparing a multivitamin to a targeted antibiotic. One provides broad systemic support; the other delivers a specific molecule to fix a specific deficiency. Neither is inherently superior; they solve different problems.
When TRT Is the Right Choice
Testosterone replacement therapy directly supplies exogenous testosterone to men whose testes cannot produce adequate amounts. If your total testosterone is below 300 ng/dL with symptoms (fatigue, low libido, loss of muscle mass, depression), TRT is the evidence-based first-line treatment. No peptide, supplement, or lifestyle intervention will raise severely deficient testosterone to normal levels as reliably as TRT.
TRT raises testosterone within days to weeks, not months. The tradeoffs are real: exogenous testosterone suppresses the HPTA, which means your testes stop producing testosterone and sperm naturally. This suppression is reversible for most men after discontinuation, but fertility preservation during TRT requires additional interventions like hCG or clomiphene. For a deeper look at male-specific peptide strategies that complement TRT, see peptides for men over 40.
| Parameter | TRT | Sermorelin |
|---|---|---|
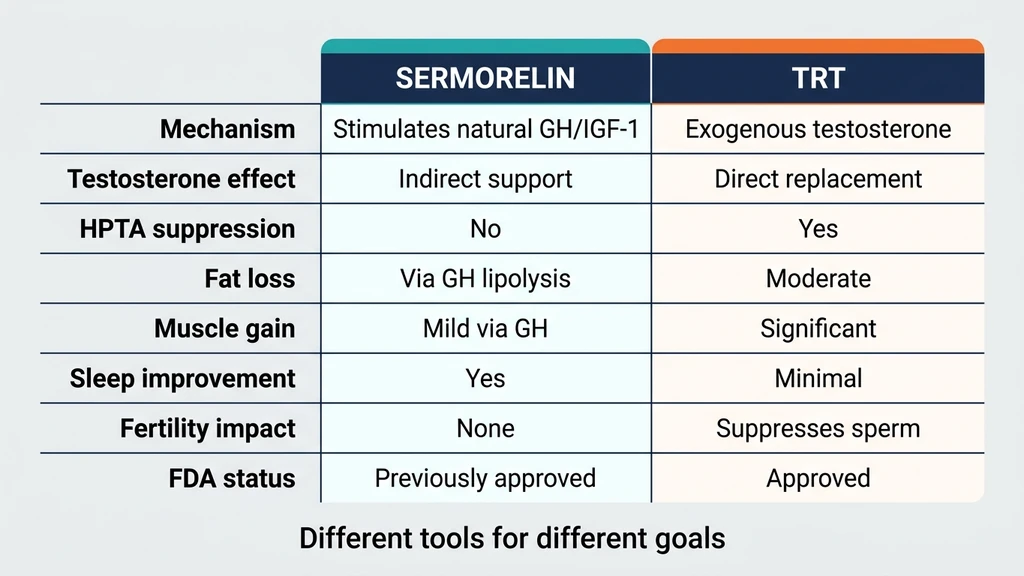
| Mechanism | Direct testosterone replacement | Stimulates natural GH release |
| Testosterone effect | Raises T to target levels within weeks | Indirect, modest, inconsistent |
| HPTA suppression | Yes, significant | No |
| Fertility impact | Suppresses spermatogenesis | None documented |
| Body composition | Increases lean mass, reduces fat | Reduces fat, modest lean mass increase |
| Sleep improvement | Minimal direct effect | Significant via GH pulsatility |
| Onset of effects | 2-4 weeks | 8-16 weeks |
| FDA status | Multiple approved formulations | Previously approved, currently off-label |
When Sermorelin Makes More Sense
Sermorelin is the better tool for men whose primary problem is growth hormone decline rather than testosterone decline, even if both hormones are suboptimal. The ideal sermorelin candidate has:
- Borderline testosterone (300-450 ng/dL) with symptoms that could stem from GH decline (poor sleep, increased visceral fat, slow recovery)
- Low IGF-1 (below 150 ng/mL for his age), suggesting GH insufficiency is the primary driver
- Desire to preserve fertility, since sermorelin does not suppress spermatogenesis
- Preference for natural hormone support over direct replacement
- Sleep disruption as a prominent symptom, since sermorelin's sleep benefits often produce the most noticeable improvement
For these men, a 3-6 month trial of sermorelin (200-300 mcg nightly) with IGF-1 monitoring at 6-8 weeks can clarify whether GH restoration resolves their symptoms without TRT. If testosterone remains symptomatic after GH normalization, adding TRT becomes a clearer clinical decision. Learn more about sermorelin safety before starting a protocol.
Combining Sermorelin and TRT: The Synergistic Approach
The Sigalos 2017 study demonstrated that adding GH secretagogues (including sermorelin) to TRT improved body composition beyond what TRT achieved alone. This makes biological sense: testosterone drives muscle protein synthesis and androgen-receptor-mediated fat metabolism, while GH drives lipolysis and collagen synthesis through different pathways. The two hormones amplify each other's body composition effects without competing for the same receptors.
A combined protocol might look like: - TRT at clinically appropriate doses (typically 100-200 mg testosterone cypionate weekly) - Sermorelin at 200-300 mcg subcutaneous nightly - Monitoring: Total T, free T, estradiol, IGF-1, and CBC every 8-12 weeks
The combination is particularly useful for men over 50 who have both testosterone and GH decline. Restoring one axis without the other leaves half the problem unsolved. The testosterone addresses libido, mood, and muscle mass; the sermorelin addresses sleep quality, visceral fat metabolism, and skin/collagen integrity.
For men interested in GH-pathway alternatives to sermorelin, CJC-1295 and ipamorelin offer similar mechanisms with different pharmacokinetic profiles. Use our CJC-1295/ipamorelin dosage calculator to compare protocols.
Body Composition Effects: Where Sermorelin and Testosterone Overlap
Men researching "does sermorelin increase testosterone" are often asking a different question underneath: "will sermorelin give me the body composition results I associate with higher testosterone?" The answer is a qualified yes, through GH-specific mechanisms rather than androgenic ones.
Fat Loss via GH-Driven Lipolysis
Growth hormone is one of the most potent lipolytic hormones in the human body. GH binds receptors on adipocytes and activates hormone-sensitive lipase, which breaks down stored triglycerides into free fatty acids for oxidation. This process is independent of testosterone.
Sermorelin-induced GH elevation produces measurable fat loss, particularly from visceral depots. The Vittone 1997 trial showed significant reductions in adiposity after six months of sermorelin treatment in GH-deficient adults. Clinically, men on sermorelin typically report losing 1-2 inches of waist circumference over 3-6 months, even without dietary changes.
This fat loss overlaps with testosterone's effects because men often attribute body composition improvements to testosterone when GH is the actual driver. A man on TRT who adds sermorelin and loses additional visceral fat may assume his testosterone "is working better" when the GH axis is doing the heavy lifting on the fat front. For specific fat-loss protocols, see sermorelin for fat loss.
Lean Mass and Muscle Recovery
Testosterone is the superior muscle-building hormone. It directly activates androgen receptors in muscle fibers, increasing myofibrillar protein synthesis and satellite cell recruitment. Growth hormone's muscle effects are more modest and operate through different pathways: increased collagen synthesis, improved nitrogen retention, and enhanced recovery between training sessions.
Men on sermorelin alone should not expect the dramatic lean mass gains that TRT produces. Expect improvements in recovery speed, reduced muscle soreness, and modest improvements in lean body mass (2-4 pounds over 6 months) rather than the 10-15 pound lean mass increases that TRT can deliver. The benefit is real but different in magnitude and mechanism.
Where GH shines is connective tissue. Tendons, ligaments, and cartilage respond to GH and IGF-1 more than to testosterone. Men with joint issues, slow-healing injuries, or training-related connective tissue wear often see more benefit from sermorelin than from additional testosterone. For a comprehensive look at growth hormone peptide stacks for recovery, read about CJC-1295/ipamorelin benefits.
Libido and Sexual Function
Testosterone is the primary hormonal driver of male libido. Men with clinically low testosterone (<300 ng/dL) consistently report reduced sexual desire, and TRT reliably restores it. Sermorelin does not have direct effects on sexual desire because it does not interact with androgen receptors in the brain regions that regulate libido.
However, sermorelin can improve sexual function indirectly through two pathways. First, improved sleep quality enhances overall energy and reduces the fatigue that suppresses libido in aging men. Second, improved body composition and the resulting confidence can have a psychological effect on sexual interest. These are secondary benefits, not primary mechanisms.
For men whose primary complaint is low libido, testosterone or PT-141 (a melanocortin receptor agonist that directly stimulates sexual arousal pathways) will produce more reliable results than sermorelin alone. Sermorelin is best understood as a supporting player in sexual health, not the lead actor.
Other GH Secretagogues and Their Testosterone Effects
Sermorelin is not the only growth hormone secretagogue. Several others have been studied for testosterone-adjacent effects, and understanding their differences helps clarify what GH-axis stimulation can and cannot do for testosterone.
CJC-1295: Extended GHRH Signaling
CJC-1295 is a modified GHRH analog with a longer half-life than sermorelin (measured in days rather than minutes). The DAC (Drug Affinity Complex) version binds albumin and provides sustained GHRH receptor stimulation. The non-DAC version (Mod GRF 1-29) is structurally similar to sermorelin but with amino acid substitutions that resist enzymatic degradation.
CJC-1295 produces higher and more sustained GH and IGF-1 elevations than sermorelin. In theory, this stronger GH stimulus might produce a larger indirect testosterone effect through the same IGF-1/Leydig cell and sleep pathways. In practice, no controlled trial has demonstrated significant testosterone increases with CJC-1295 either. The indirect pathways appear to have a ceiling effect regardless of how much GH you produce. See our CJC-1295 dosage guide for protocol details.
Ipamorelin: Ghrelin Mimetic Approach
Ipamorelin stimulates GH release through ghrelin receptors (GHS-R1a) rather than GHRH receptors. It produces a cleaner GH pulse with less cortisol and prolactin elevation compared to other ghrelin mimetics. Ipamorelin is often combined with CJC-1295 for synergistic GH release.
Like sermorelin, ipamorelin has no direct testosterone-boosting mechanism. Its advantages over sermorelin are selectivity (fewer off-target hormonal effects) and synergy with GHRH analogs. Men who combine CJC-1295 with ipamorelin report the strongest GH-related body composition improvements, but testosterone-specific effects remain indirect and modest.
MK-677 (Ibutamoren): Oral GH Secretagogue
MK-677 is an oral, non-peptide ghrelin mimetic that raises GH and IGF-1 for up to 24 hours per dose. Its convenience (oral administration, once daily) makes it popular, but it comes with side effects that sermorelin avoids: increased appetite, water retention, and potential insulin resistance with prolonged use.
Regarding testosterone: a 2-month study of MK-677 in obese males showed increased GH and IGF-1 but no significant changes in testosterone. A 2-year study in elderly adults showed sustained GH and IGF-1 elevation but, again, no significant testosterone increases. MK-677 provides the strongest test of the "more GH equals more testosterone" hypothesis, and the results consistently show that the relationship does not scale linearly. Even substantial GH elevation fails to produce clinically meaningful testosterone increases.
Who Should Consider Sermorelin for Testosterone-Related Symptoms
Given that sermorelin does not directly raise testosterone, identifying the right candidates requires distinguishing between GH-deficiency symptoms and testosterone-deficiency symptoms. There is significant overlap, which is why men conflate the two.
Symptoms That Suggest GH Decline (Sermorelin May Help)
- Poor sleep quality with difficulty reaching deep sleep stages
- Increased visceral fat despite stable diet and exercise
- Slow recovery from workouts or injuries
- Thinning skin and reduced collagen integrity
- Low IGF-1 levels on blood work (below age-adjusted reference range)
- Fatigue that worsens throughout the day
- Joint stiffness unrelated to arthritis or injury
These symptoms overlap with testosterone deficiency but respond better to GH restoration. If your blood work shows low IGF-1 (below 150 ng/mL) with borderline or normal testosterone, sermorelin is the logical first intervention. Monitor IGF-1 at 6-8 weeks and reassess symptoms at 12 weeks. Read how long does sermorelin take to work for realistic timelines.
Symptoms That Suggest Testosterone Decline (TRT Likely Needed)
- Loss of morning erections and reduced libido
- Depression or irritability unresponsive to lifestyle changes
- Significant muscle loss despite resistance training
- Total testosterone below 300 ng/dL on two separate morning blood draws
- Elevated SHBG with low free testosterone
- Gynecomastia or breast tenderness
These symptoms point to primary or secondary hypogonadism that requires direct testosterone replacement. Sermorelin will not resolve them. If your total testosterone is below 300 ng/dL, see an endocrinologist or urologist rather than starting a peptide protocol.
The Overlap Zone: When Both May Be Needed
Many men over 40 have concurrent GH and testosterone decline. Their blood work shows total testosterone of 350-450 ng/dL (borderline low), IGF-1 below the age-adjusted midrange, and symptoms from both axes. For these men, a stepwise approach works best:
Step 1 (Months 1-3): Start sermorelin at 200-300 mcg nightly. Optimize sleep, exercise, and nutrition simultaneously. Recheck IGF-1 and testosterone at 8-12 weeks.
Step 2 (Assessment at Month 3): If IGF-1 normalizes and symptoms improve substantially, continue sermorelin alone. If testosterone remains symptomatic despite IGF-1 improvement, add TRT.
Step 3 (If TRT is added): The combination of sermorelin + TRT produces superior body composition outcomes compared to either alone, as demonstrated by Sigalos et al. Monitor both axes with regular blood work.
This stepwise approach avoids premature TRT initiation in men whose symptoms are primarily GH-driven and identifies the men who genuinely need testosterone replacement. For peptides for men over 40, this combined hormonal assessment is essential.
Dosing Sermorelin for Indirect Testosterone Support
If you are using sermorelin partly for its indirect testosterone-supporting effects, the dosing protocol is the same as standard sermorelin therapy. There is no "testosterone-boosting dose" that differs from the standard GH-optimization dose.
Standard Protocol
- Dose: 200-300 mcg subcutaneous injection nightly
- Timing: 30-60 minutes before bedtime, on an empty stomach (food blunts GH release)
- Cycle: 5 days on, 2 days off; or continuous for 3-6 months
- Monitoring: IGF-1 at baseline, 6-8 weeks, and 12 weeks; total and free testosterone at the same intervals
- Adjustment: Increase to 300-500 mcg if IGF-1 response is inadequate
The bedtime timing is critical for testosterone support because it synchronizes the sermorelin-induced GH pulse with the body's natural nocturnal testosterone secretion window. Morning injections still raise GH but miss the sleep-testosterone synergy. For complete dosing details, see how much sermorelin per day.
Stacking for Enhanced Effects
Men seeking maximum GH-axis stimulation (and by extension, the strongest indirect testosterone support) often combine sermorelin with complementary peptides:
- Sermorelin + Ipamorelin: GHRH + ghrelin mimetic for synergistic GH release. The two peptides activate different receptors on somatotroph cells, producing a larger GH pulse than either alone.
- Sermorelin + CJC-1295 (no DAC): Short-acting + modified GHRH for both pulse amplitude and duration.
- Sermorelin + GHRP-6: Older combination with stronger appetite stimulation. Better for underweight men who need caloric surplus.
None of these stacks convert sermorelin into a direct testosterone booster. They amplify the GH signal, which may modestly amplify the indirect testosterone pathways. Use the CJC-1295/ipamorelin dosage calculator to compare stack protocols.
Lifestyle Factors That Amplify the GH-Testosterone Connection
Sermorelin's indirect testosterone effects are most pronounced when lifestyle factors support both axes simultaneously:
Sleep: Aim for 7-9 hours. Sermorelin improves sleep architecture, but it cannot compensate for chronic sleep restriction. Every additional hour of sleep between 5 and 8 hours raises morning testosterone measurably.
Resistance Training: Compound lifts (squats, deadlifts, presses) stimulate both GH and testosterone acutely. Training within 2-3 hours of sermorelin injection (evening training, bedtime injection) may amplify the combined hormonal response.
Body Fat Management: Keep body fat below 20% to minimize aromatase-driven testosterone-to-estrogen conversion. Sermorelin's lipolytic effects help, but dietary adherence determines the magnitude of fat loss.
Micronutrients: Zinc, magnesium, vitamin D, and boron support testosterone production. Deficiencies in any of these blunt the testosterone response regardless of GH status. Correct deficiencies before attributing low testosterone to GH decline.
Stress Management: Chronic cortisol elevation suppresses both GH and testosterone. Sermorelin cannot overcome the hormonal effects of unmanaged psychological or physical stress.
Safety Considerations: Sermorelin vs. Direct Testosterone Manipulation
One reason sermorelin appeals to men concerned about testosterone is its safety profile relative to direct hormonal manipulation. Understanding the risk differences helps frame realistic expectations.
What Sermorelin Does Not Do
- No HPTA suppression: Unlike exogenous testosterone, sermorelin does not shut down your body's natural testosterone production. Your testes continue functioning normally. This is the single biggest safety advantage for men considering sermorelin over TRT for borderline testosterone levels.
- No aromatization: Sermorelin is a peptide, not a steroid. It cannot be converted to estrogen by aromatase enzymes. Men on TRT often require aromatase inhibitors to manage estradiol; men on sermorelin do not.
- No polycythemia risk: TRT frequently elevates red blood cell counts (hematocrit), increasing thrombotic risk. Sermorelin does not affect erythropoiesis.
- No prostate stimulation: Testosterone directly stimulates prostate tissue growth. Sermorelin has no androgenic activity and does not accelerate benign prostatic hyperplasia.
For a comprehensive look at sermorelin's side effect profile, read is sermorelin safe.
What Sermorelin Can Cause
Sermorelin's side effects are generally mild and GH-related: - Injection site reactions: Redness, swelling, or itching at the subcutaneous injection site. Occurs in approximately 15-20% of users, usually resolving within 30 minutes. See where to inject sermorelin for technique tips. - Water retention: Mild fluid retention during the first 2-4 weeks as GH levels rise. Usually self-limiting. - Joint pain: Transient joint discomfort from GH-driven fluid shifts. More common at doses above 300 mcg. - Headache: Occasional headaches during the first week. Typically resolve with continued use. - Flushing or dizziness: Rare. Usually occurs within 15 minutes of injection and resolves quickly.
These side effects are dose-dependent and rarely require discontinuation. Compare this to TRT's side effect profile (acne, hair loss, testicular atrophy, potential cardiovascular risk, fertility suppression) and the safety argument for trying sermorelin first becomes clear for men with borderline testosterone.
The Bottom Line: Sermorelin Is Not a Testosterone Treatment
Sermorelin is a growth hormone secretagogue that produces real, clinically documented benefits for body composition, sleep quality, and GH/IGF-1 restoration. It is not a testosterone treatment. The indirect pathways through which GH supports testosterone (IGF-1/Leydig cell stimulation, sleep improvement, visceral fat reduction, possible FSH/LH stimulation) are biologically plausible and partially supported by evidence, but their magnitude is too modest and inconsistent to recommend sermorelin as a standalone solution for low testosterone.
The practical framework is straightforward: - Clinically low testosterone (< 300 ng/dL): See a physician for TRT evaluation. Sermorelin will not fix this. - Borderline testosterone (300-450 ng/dL) with low IGF-1: Trial sermorelin for 3 months with blood work monitoring. The GH restoration may resolve symptoms. - Normal testosterone with GH-decline symptoms: Sermorelin addresses the actual deficiency without touching testosterone. - Both axes declining (common after age 45): Consider combining sermorelin with TRT for synergistic body composition and quality-of-life improvements.
The men who benefit most from sermorelin are those who understand what it does (restores GH) rather than what they wish it did (replace testosterone). Start with accurate blood work, match the intervention to the deficiency, and monitor results with follow-up labs rather than subjective impressions.
Frequently Asked Questions
Does sermorelin directly increase testosterone levels?
No. Sermorelin is a GHRH analog that stimulates growth hormone release from the pituitary gland. It has no affinity for androgen receptors and cannot directly raise testosterone. Any testosterone-related benefits come indirectly through GH/IGF-1 pathways, improved sleep, and body composition changes. For direct testosterone evaluation, read our peptides for men guide.
How does sermorelin indirectly support testosterone production?
Sermorelin raises GH, which the liver converts to IGF-1. IGF-1 stimulates Leydig cells in the testes by upregulating LH receptor density, potentially enhancing testosterone synthesis. Sermorelin also improves deep sleep (when 65-70% of daily testosterone is produced) and reduces visceral fat (lowering aromatase-driven testosterone-to-estrogen conversion). For fat-specific protocols, see sermorelin for fat loss.
Is sermorelin better than TRT for raising testosterone?
No. TRT directly replaces testosterone and reliably raises levels within 2-4 weeks. Sermorelin's indirect testosterone effects are modest and inconsistent. However, sermorelin avoids TRT's drawbacks (HPTA suppression, fertility impact, polycythemia risk). For men with borderline testosterone and confirmed GH decline, sermorelin may resolve symptoms without TRT. Learn about sermorelin's safety profile in is sermorelin safe.
Can I take sermorelin and TRT together?
Yes. The combination produces synergistic body composition improvements. A 2017 study showed that adding GH secretagogues (including sermorelin) to TRT increased lean mass and reduced body fat beyond TRT alone. The testosterone handles muscle growth and libido; sermorelin handles sleep, fat metabolism, and connective tissue. Use our CJC-1295/ipamorelin dosage calculator for GH-side protocol planning.
How long does it take for sermorelin to affect testosterone levels?
Sermorelin's indirect testosterone effects, if they occur, take 8-16 weeks to manifest. IGF-1 elevation begins within 2-4 weeks, but the downstream effects on Leydig cell function, sleep-mediated testosterone production, and body composition take longer. Check IGF-1 at 6-8 weeks and testosterone at 12 weeks. Read how long does sermorelin take to work for a week-by-week timeline.
What is the best sermorelin dose for testosterone support?
The standard dose of 200-300 mcg subcutaneously before bedtime is optimal. There is no special "testosterone-boosting" dose. Higher doses (above 500 mcg) do not produce proportionally larger indirect testosterone effects because the GH-to-testosterone pathway has a ceiling. Bedtime timing is critical because it synchronizes with nocturnal testosterone production. See how much sermorelin per day for complete dosing tables.
Does sermorelin suppress natural testosterone production?
No. Unlike TRT, which suppresses the hypothalamic-pituitary-testicular axis (HPTA) and shuts down endogenous testosterone production, sermorelin has no effect on the HPTA. Your testes continue producing testosterone normally while on sermorelin. This is a key advantage for men who want to preserve fertility. Learn more in is sermorelin a steroid.
Which GH secretagogue has the strongest testosterone effect?
None of the GH secretagogues (sermorelin, CJC-1295, ipamorelin, MK-677) directly raise testosterone. Even MK-677, which produces the most sustained GH/IGF-1 elevation, failed to significantly raise testosterone in 2-month and 2-year clinical studies. The GH-to-testosterone relationship has a ceiling that additional GH stimulation cannot overcome.
Should I take sermorelin in the morning or at bedtime for testosterone benefits?
Bedtime, always. Approximately 65-70% of daily testosterone secretion occurs during sleep, with peaks during REM stages. Injecting sermorelin 30-60 minutes before bed synchronizes the GH pulse with the sleep-testosterone production window. Morning injection still raises GH but misses this synergy. For injection technique details, see where to inject sermorelin.
Is sermorelin safe for long-term use alongside testosterone monitoring?
Sermorelin has a favorable long-term safety profile. It works within the pituitary's natural feedback loop (somatostatin limits excessive GH release), does not suppress the HPTA, and does not cause aromatization or polycythemia. The FDA withdrew it in 2008 for manufacturing reasons, not safety concerns. Monitor IGF-1 every 3-6 months to ensure levels stay within range. Read the full safety assessment in is sermorelin safe.
The Bottom Line
Sermorelin does not increase testosterone directly. It is a growth hormone secretagogue, and growth hormone secretagogues restore GH, not testosterone. The indirect pathways linking GH to testosterone (IGF-1 effects on Leydig cells, improved sleep architecture, reduced visceral fat, possible FSH/LH stimulation) are real but produce modest, inconsistent testosterone changes that no controlled trial has found statistically significant.
This does not make sermorelin useless for men concerned about testosterone. It means the benefits sermorelin provides, better sleep, reduced body fat, improved recovery, enhanced body composition, address many of the same symptoms that drive men to seek testosterone treatment. For men with borderline testosterone and concurrent GH decline, sermorelin may resolve the underlying issue without introducing TRT's side effects and fertility concerns.
The clinical evidence supports using sermorelin as a body composition and GH-restoration tool, optionally combined with TRT for men who need both. Match the intervention to the lab-confirmed deficiency: low IGF-1 gets sermorelin, low testosterone gets TRT, and both deficiencies get both treatments. Start with blood work, not assumptions.
For related sermorelin topics, explore how much sermorelin per day, where to inject sermorelin, and sermorelin for fat loss. For peptide stacking strategies that complement a testosterone protocol, see our peptide stacking guide.
Helpful Tools
Related Articles
How Long Does Sermorelin Take to Work?
Sermorelin improves sleep in 1-2 weeks, boosts energy by week 3-4, shifts body composition at month 2-3, and delivers full results at 3-6 months.
How Much Sermorelin Per Day: Complete Dosage Guide
Sermorelin dosage: 200-500 mcg/day subcutaneous before bedtime. Starting dose, titration, gender-specific protocols, and IGF-1 monitoring.
Tesamorelin Peptide: Uses, Evidence, Risks
Tesamorelin peptide explained: a GHRH analogue FDA-approved as Egrifta for HIV lipodystrophy. What it does to visceral fat, IGF-1, and who should avoid it.
CJC-1295 With DAC: Long-Acting GHRH Analog
CJC-1295 with DAC: 6-8 day half-life, 2-10x GH increase, 1-2 mg weekly. GH bleed effect, desensitization risk, and stacking protocols.