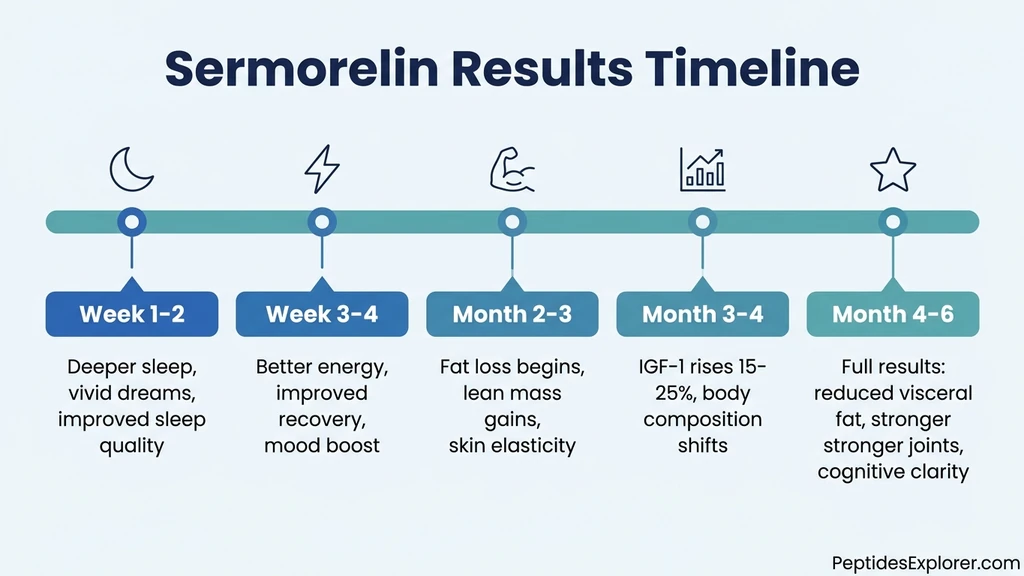
You started sermorelin injections a few nights ago. You slept well, maybe better than usual, but you are not sure if the peptide caused it or if you just had a good night. Sermorelin begins stimulating growth hormone release within minutes of injection, but noticeable results follow a predictable timeline: improved sleep at weeks 1 to 2, better energy and recovery at weeks 3 to 4, measurable body composition changes at months 2 to 3, and full therapeutic benefits at 3 to 6 months. IGF-1 levels, the most reliable blood marker of growth hormone activity, typically rise 15 to 25% above baseline within 8 to 12 weeks of consistent nightly dosing (Walker, Clin Interv Aging, 2006).
The delay between injection and visible results is not a flaw. It reflects how sermorelin works. Unlike synthetic human growth hormone (rhGH), which floods the body with exogenous hormone, sermorelin stimulates your pituitary gland to produce and release GH in its natural pulsatile pattern. Your body rebuilds its growth hormone output gradually, the way a weakened muscle regains strength through progressive training rather than a single heavy lift.
| Timeframe | What You Notice | What Is Happening Biologically |
|---|---|---|
| Days 1-3 | Nothing yet | GH pulse amplitude increases during sleep |
| Weeks 1-2 | Deeper sleep, vivid dreams | Slow-wave sleep duration extends |
| Weeks 3-4 | More energy, faster recovery | IGF-1 begins rising, cellular repair accelerates |
| Months 2-3 | Skin tightness, fat loss begins | Lipolysis increases, collagen synthesis activates |
| Months 3-4 | Body composition visibly shifts | IGF-1 reaches new steady state (15-25% above baseline) |
| Months 4-6 | Full results: reduced visceral fat, lean mass, joint health | All downstream GH pathways fully upregulated |
For dosing specifics during this timeline, see our peptide dosage chart. For a comparison of sermorelin against other growth hormone secretagogues, read our tesamorelin vs sermorelin vs ipamorelin analysis.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
How Sermorelin Works: The GHRH Mechanism
Sermorelin is a 29-amino-acid peptide that replicates the biologically active fragment of growth hormone-releasing hormone (GHRH). Your hypothalamus produces full-length GHRH (44 amino acids) to tell the pituitary gland when to secrete growth hormone. Sermorelin uses the same receptor, the GHRHR on somatotroph cells, to deliver the same signal (Walker, Clin Interv Aging, 2006).
The distinction between sermorelin and synthetic HGH matters for understanding timeline. Direct HGH injection bypasses the pituitary entirely. The hormone enters your bloodstream at whatever dose you inject, whether your body needs it or not. Sermorelin asks your pituitary to do the work. The pituitary responds by releasing GH in pulses, with the largest pulse occurring during deep sleep. This pulsatile pattern preserves the negative feedback loop: when GH and IGF-1 reach adequate levels, somatostatin signals the pituitary to pause secretion (Ishida et al., JCSM Rapid Commun, 2020).
This built-in safety brake means sermorelin rarely pushes GH or IGF-1 beyond physiological norms. It also means results build gradually because you are restoring a biological system, not overriding it. For a deeper look at whether sermorelin is safe, including side effect profiles from clinical use, see our dedicated safety article.
Pharmacokinetics: What Happens After Injection
Sermorelin has a plasma half-life of 10 to 20 minutes after subcutaneous injection. Dipeptidyl peptidase IV (DPP-IV) and other serum proteases break it down rapidly. This short half-life is intentional. Sermorelin does not need to circulate for hours because its job is to trigger a GH pulse, not sustain one. The GH pulse itself lasts 1 to 2 hours and drives downstream effects through IGF-1, which has a half-life of 12 to 15 hours.
Peak GH concentrations after a sermorelin injection occur within 30 to 60 minutes. In clinical testing, intravenous sermorelin produced a measurable GH spike within 5 to 20 minutes, confirming rapid receptor activation (Prakash & Goa, BioDrugs, 1999). Subcutaneous injection, the standard therapeutic route, follows a similar but slightly delayed curve.
The practical takeaway: sermorelin works fast at the cellular level. The weeks-to-months timeline for visible results reflects how long it takes for repeated nightly GH pulses to accumulate enough downstream effects (IGF-1 production, collagen synthesis, lipolysis, cellular repair) for you to notice them. It is not unlike how consistent exercise produces invisible muscle protein synthesis for weeks before the mirror shows anything different.
IGF-1: The Blood Marker That Confirms Sermorelin Is Working
Insulin-like growth factor 1 (IGF-1) is the best objective measure of sermorelin efficacy. The liver produces IGF-1 in response to growth hormone stimulation. Because GH itself is pulsatile and difficult to measure (a single blood draw might catch a peak or a trough), clinicians use IGF-1 as a stable proxy. IGF-1 levels reflect average GH output over days, not minutes.
Baseline IGF-1 should be drawn before starting sermorelin. A follow-up draw at 8 to 12 weeks confirms whether the pituitary is responding. A 15 to 25% increase in IGF-1 above baseline indicates the peptide is working as intended. If IGF-1 has not moved after 12 weeks, the dose may need adjustment, the injection timing may be wrong, or pituitary reserve may be insufficient (Walker, Clin Interv Aging, 2006).
IGF-1 reaches a new steady state approximately 2 to 4 weeks after any dose change. If your clinician increases your dose from 200 mcg to 300 mcg, wait at least 4 weeks before retesting to get an accurate reading. Premature testing produces misleadingly low results.
Week-by-Week Sermorelin Results Timeline
The following timeline reflects the typical experience reported in clinical practice and supported by research on GHRH analogs. Individual variation is significant. Age, baseline GH production, body composition, sleep quality, and concurrent medications all shift the curve. But the sequence of changes is consistent: sleep improves first, energy follows, body composition shifts last.
Weeks 1-2: Sleep Quality Improves
The first reliable sign that sermorelin is working is better sleep. This is not placebo. Growth hormone and slow-wave sleep (the deepest phase of non-REM sleep) are biologically linked. The largest natural GH pulse of the day occurs during the first bout of slow-wave sleep, typically 60 to 90 minutes after falling asleep. Sermorelin amplifies this pulse, and the amplified GH secretion, in turn, extends slow-wave sleep duration.
A study published in the journal Sleep found that GHRH administration increased slow-wave sleep and reduced wakefulness in older adults with age-related GH decline (Vitiello et al., Clin Interv Aging, 2006). Participants reported falling asleep faster, waking less during the night, and feeling more rested in the morning.
What you may experience during weeks 1 to 2: deeper sleep with fewer nighttime awakenings, more vivid dreams (a hallmark of increased slow-wave and REM sleep), and waking feeling genuinely rested rather than groggy. Some users report improved sleep from the very first night, though this likely reflects the acute GH pulse rather than a lasting change. By the end of week 2, the pattern should be consistent. For more on the sleep-peptide connection, see our guide on peptides for sleep.
Weeks 3-4: Energy, Recovery, and Mood
By the third week, cumulative improvements in sleep quality translate to daytime benefits. Better sleep means better cellular repair, improved glucose regulation, and more complete neurotransmitter recycling. You feel this as increased energy during the day, particularly in the afternoon when most people hit an energy trough.
Recovery from exercise accelerates. Growth hormone is a primary driver of tissue repair. The GH pulse triggered by sermorelin during sleep coincides with the body's natural repair window. Muscle soreness resolves faster. Delayed-onset muscle soreness (DOMS) that used to last 3 days may last 1 to 2. Joint stiffness after morning workouts diminishes. These changes are subtle but consistent.
Mood improvements are common at this stage. The mechanism is indirect: better sleep improves serotonin metabolism, reduces cortisol, and stabilizes blood sugar. Some users describe a "quiet optimism" that was absent before treatment. This is not euphoria. It is the absence of the low-grade fatigue and irritability that accompany chronically poor sleep and declining GH.
IGF-1 is beginning to rise at this point, but usually not enough to show a dramatic change on a blood test. The visible and subjective changes at weeks 3 to 4 are driven more by improved sleep architecture than by significant IGF-1 elevation.
Months 2-3: Body Composition Begins Shifting
This is where sermorelin's effects become measurable rather than just perceptible. IGF-1 has risen enough to activate downstream pathways that alter body composition. Three processes accelerate simultaneously.
Lipolysis increases. Growth hormone is one of the strongest natural lipolytic signals. It tells adipose tissue to break down stored triglycerides into free fatty acids for energy use. The effect is strongest against visceral fat, the metabolically dangerous fat surrounding abdominal organs. Users often notice their midsection tightening before the scale moves, because visceral fat loss does not always register as weight loss. Dense muscle may be replacing lighter fat tissue. For a detailed look at this mechanism, see our article on sermorelin for fat loss.
Lean mass preservation and modest gains. IGF-1 stimulates muscle protein synthesis and inhibits protein breakdown. In combination with resistance training, sermorelin users in this phase often notice improved muscle tone, better "pump" during workouts, and faster strength gains. This is not steroid-level muscle growth. Sermorelin operates within physiological GH ranges. The gains are modest and proportional to your training intensity. For context on whether sermorelin is a steroid (it is not), see our explainer.
Collagen synthesis activates. GH and IGF-1 stimulate fibroblasts to produce collagen. By month 2, some users report tighter skin, reduced fine wrinkles, and improved skin elasticity. Nails grow faster. Hair may feel thicker. These changes accelerate over months 3 to 6 as cumulative collagen deposition builds.
Months 3-4: IGF-1 Reaches Steady State
By month 3, IGF-1 levels have typically reached their new steady state under sermorelin therapy. This is when the 8-to-12-week follow-up blood draw provides the most accurate picture of treatment response. A 15 to 25% rise above baseline confirms the pituitary is responding well. Research on GH secretagogues in hypogonadal men demonstrated that IGF-1 increases paralleled fat loss and lean mass improvements over this timeframe (Sigalos & Pastuszak, Transl Androl Urol, 2018).
The body composition changes that started at month 2 become visible to others at month 3 to 4. If you have been consistent with training and diet, you will notice reduced abdominal girth, better muscle definition, and improved recovery between training sessions. The changes are cumulative. Sermorelin does not produce dramatic before-and-after transformations in 90 days. It produces a steady, measurable drift toward a leaner, more resilient physiology.
Joint health improvements emerge during this phase. GH and IGF-1 stimulate chondrocyte activity and synovial fluid production. People with chronic joint stiffness or mild osteoarthritis often report reduced morning stiffness and improved range of motion. For those interested in peptides specifically for joint support, our peptides for muscle growth guide covers complementary options.
Months 4-6: Full Therapeutic Benefits
The full spectrum of sermorelin benefits materializes between months 4 and 6 of consistent nightly dosing. By this point, the body has been exposed to hundreds of enhanced GH pulses. The downstream effects have accumulated across every tissue type that responds to GH and IGF-1.
Expected outcomes at the 6-month mark include: 10 to 20% reduction in visceral fat (measurable via DEXA scan), improved fasting glucose and insulin sensitivity, measurably thicker skin with better elasticity, stronger hair and nail growth, 15 to 25% improvement in IGF-1 above baseline, enhanced exercise capacity and faster recovery, and improved cognitive clarity and focus.
A key study on GHRH analog therapy in adults with age-related GH decline found that 6 months of treatment restored IGF-1 levels to those typical of adults 10 to 20 years younger, with corresponding improvements in body composition and quality of life (Walker, Clin Interv Aging, 2006). The study also noted that benefits continued to accrue beyond 6 months, suggesting that the 6-month mark is not a ceiling but a milestone.
Most clinicians recommend a minimum 3-to-6-month trial before evaluating whether sermorelin therapy is effective for a given patient. Stopping at 4 to 6 weeks because you "only" feel better sleep is premature. The body composition and metabolic benefits that make sermorelin worth the investment require the longer timeframe.
Sermorelin vs. Direct HGH: Why the Timeline Differs
If synthetic HGH produces visible results in 2 to 4 weeks, why does sermorelin take 2 to 3 months? The answer lies in mechanism. Direct HGH injection delivers supraphysiologic hormone levels immediately. The body does not need to ramp up production because production is bypassed entirely. Results come faster, but so do risks: joint pain, edema, carpal tunnel syndrome, insulin resistance, and potential contribution to tumor growth in susceptible individuals.
Sermorelin works through the pituitary's existing machinery. The pituitary must "re-learn" how to produce larger GH pulses in response to GHRH stimulation. In people with age-related GH decline (somatopause), the pituitary has not atrophied. It has simply become less responsive to GHRH because of declining hypothalamic signaling and increased somatostatin tone. Sermorelin restores the signal. The pituitary responds, but gradually, like a muscle that has been underused.
| Feature | Sermorelin | Synthetic HGH (rhGH) |
|---|---|---|
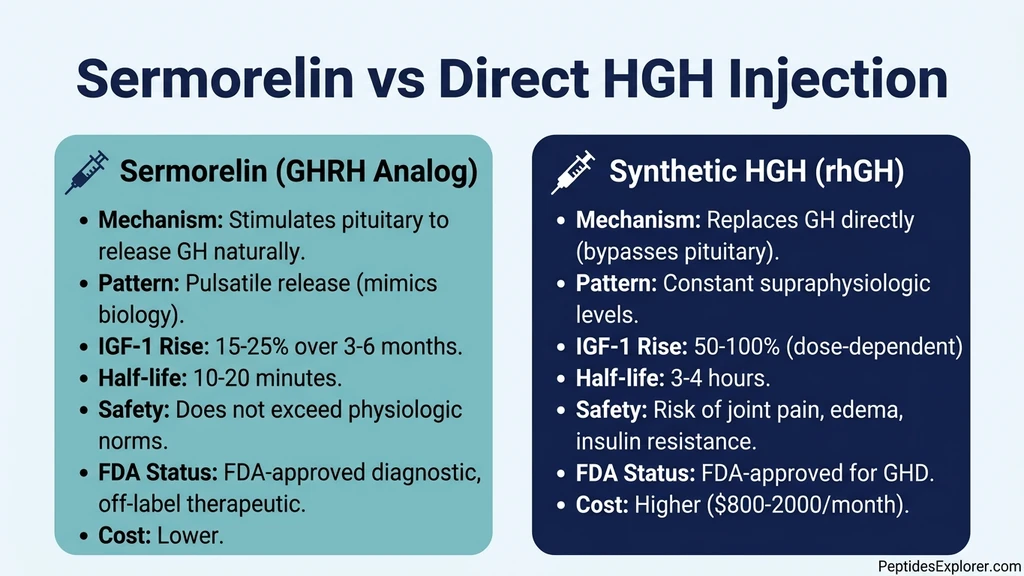
| Mechanism | Stimulates pituitary to release GH | Replaces GH directly |
| GH pattern | Pulsatile (natural) | Constant (supraphysiologic) |
| IGF-1 rise | 15-25% (physiologic) | 50-100%+ (dose-dependent) |
| Time to results | 2-6 months | 2-6 weeks |
| Safety profile | Preserves feedback loops | Overrides feedback loops |
| Joint pain/edema | Rare | Common at higher doses |
| Cost | $150-400/month | $800-2,000/month |
The tradeoff is clear: sermorelin is slower but safer. It produces results within physiological norms while maintaining the body's ability to self-regulate GH output. For people seeking anti-aging, body composition, and recovery benefits without the risks of exogenous hormone replacement, the longer timeline is the price of doing it right. For sourcing information, see where to buy sermorelin.
Factors That Speed Up or Slow Down Sermorelin Results
Not everyone follows the standard timeline. The following factors create the most variance between fast responders (noticeable changes in 2 to 3 weeks) and slow responders (needing 8 to 12 weeks for the same milestones).
Age and Pituitary Reserve
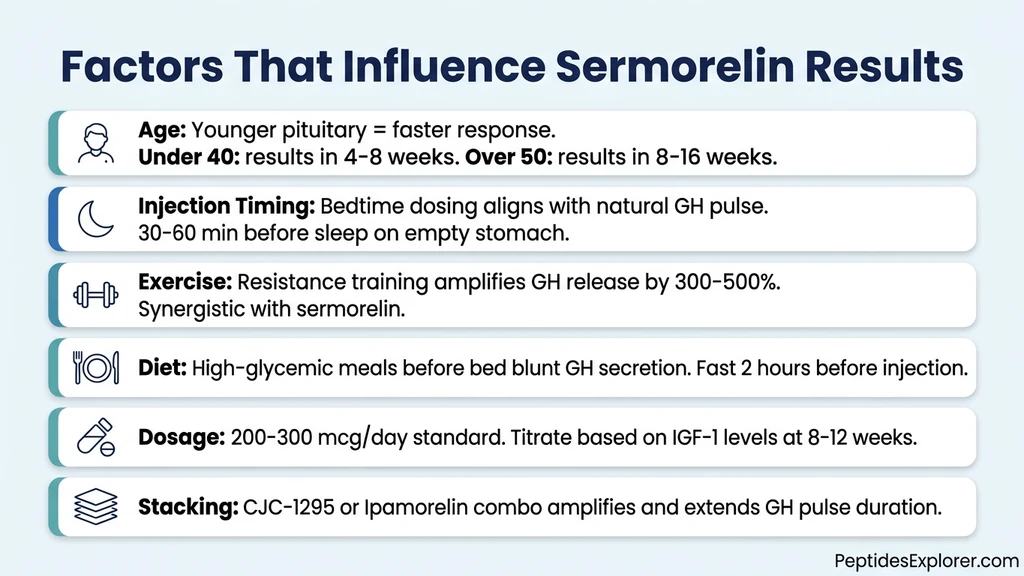
Younger adults (under 40) with mild GH decline tend to respond fastest. Their pituitary somatotroph cells are still abundant and functional; they just need a stronger signal. Sermorelin provides that signal, and GH output responds within days.
Adults over 50 may need longer. Age-related somatotroph loss means fewer cells are available to respond. The remaining cells can still increase output, but the ceiling is lower and the ramp-up is slower. A 55-year-old with 30 years of declining GH may need 10 to 16 weeks to achieve the same IGF-1 improvement a 35-year-old reaches in 6 weeks.
Pituitary damage from prior head trauma, radiation therapy, or pituitary tumors can severely limit response. If IGF-1 does not rise after 12 weeks of adequate dosing, pituitary insufficiency may be the cause, and direct GH replacement becomes the only effective option.
Injection Timing and Fasting State
Sermorelin should be injected 30 to 60 minutes before bedtime on an empty stomach. This timing matters for two reasons. First, the largest natural GH pulse coincides with sleep onset. Injecting sermorelin before bed amplifies this pulse rather than creating an off-cycle pulse during the day when somatostatin tone is higher. Second, blood glucose and insulin suppress GH release. Eating within 2 hours of injection, especially high-glycemic foods, blunts the GH response.
Clinical protocols consistently specify bedtime dosing with a 2-hour fast before injection. Patients who inject in the morning or shortly after meals report slower results, likely because they are losing 30 to 50% of each dose's effectiveness to poor timing. For a detailed protocol on how to inject peptides including site rotation and technique, see our injection guide.
Exercise: The Natural Amplifier
Resistance training is the most powerful natural GH amplifier. A single bout of heavy compound exercise (squats, deadlifts, rows) can increase GH secretion by 300 to 500% for 1 to 2 hours post-workout. When combined with sermorelin's nightly pulsatile stimulus, the cumulative GH exposure over a week is substantially higher than either intervention alone.
High-intensity interval training (HIIT) produces a similar acute GH spike. Steady-state cardio does not. If your goal is to accelerate sermorelin results, prioritize resistance training 3 to 4 days per week and include 1 to 2 HIIT sessions. The synergy between exercise-induced and sermorelin-induced GH pulses is additive, not merely redundant. For peptides specifically targeting athletic performance, see our peptides for muscle growth guide.
Sleep Hygiene
Sermorelin amplifies the GH pulse during slow-wave sleep. If your sleep architecture is disrupted (from alcohol, blue light exposure, irregular sleep schedules, or sleep apnea), the pulse it amplifies is already compromised. Optimizing sleep hygiene before or alongside sermorelin therapy improves response speed.
Key sleep factors: consistent bedtime within a 30-minute window, dark room (blackout curtains or sleep mask), no screens 60 minutes before bed, room temperature between 65 and 68 degrees Fahrenheit, and no alcohol within 3 hours of sleep. Alcohol is particularly destructive to slow-wave sleep. Even moderate intake (2 drinks) can suppress slow-wave sleep by 20 to 40%, directly undermining sermorelin's mechanism.
Dosage and Stacking
Standard sermorelin dosing ranges from 200 to 300 mcg per day, injected subcutaneously before bed. Some clinicians start at 100 mcg and titrate up based on IGF-1 response. Higher doses (up to 500 mcg) may be used in patients with very low baseline GH but carry more risk of side effects (flushing, headache, dizziness).
Stacking sermorelin with CJC-1295 or ipamorelin is common in clinical practice and can accelerate results. CJC-1295 (especially the DAC variant) has a half-life of 6 to 8 days, providing sustained GHRH receptor stimulation between sermorelin's brief pulses. Ipamorelin, a growth hormone secretagogue that works through the ghrelin receptor (GHS-R), stimulates GH release through a separate pathway. The combination produces a larger, more sustained GH pulse than either peptide alone. For a head-to-head breakdown, see our CJC-1295 vs sermorelin comparison. Use our CJC-1295/ipamorelin dosage calculator to plan stacking protocols.
How to Know If Sermorelin Is Working: Signs and Lab Markers
Tracking sermorelin's effects requires both subjective monitoring (how you feel) and objective measurement (what the blood shows). Relying on either alone gives an incomplete picture.
Subjective Markers (Weeks 1-4)
The earliest signs are experiential. Keep a brief daily log during the first 4 weeks:
Sleep quality. Rate your sleep 1 to 10 each morning. A consistent 1 to 2 point improvement by week 2 is a positive signal. Note dream vividness, nighttime awakenings, and morning alertness.
Energy. Track afternoon energy specifically. Growth hormone's metabolic effects are most noticeable during the 2 to 5 PM window when cortisol is declining and most people reach their daily low point. Sermorelin users often report that this afternoon slump becomes less severe.
Recovery. Log muscle soreness after workouts using a 1 to 5 scale. A shift from level 4 soreness lasting 3 days to level 3 soreness lasting 2 days is meaningful, even if it does not feel dramatic in the moment.
Skin and nails. These are slower signals (4 to 8 weeks) but reliable. Notice whether nail growth accelerates, whether small cuts heal faster, or whether skin on the backs of your hands feels slightly firmer.
Objective Markers (Weeks 8-12)
Blood work provides the definitive answer. The essential panel includes:
IGF-1. The primary marker. A 15 to 25% rise above baseline confirms adequate GH stimulation. Draw at baseline and again at 8 to 12 weeks. Target the age-appropriate reference range: IGF-1 naturally declines with age, and the goal is to restore levels to the upper quartile for your age group, not to exceed it.
IGFBP-3 (IGF binding protein 3). This carrier protein tracks with IGF-1 and provides a secondary confirmation. An increase in IGFBP-3 alongside IGF-1 indicates genuine GH axis activation, not measurement artifact.
Fasting glucose and insulin. GH improves insulin sensitivity over time. A decrease in fasting insulin (while glucose remains stable) indicates improved metabolic function.
Body composition (DEXA scan). If available, a DEXA scan at baseline and 6 months provides precise measurements of lean mass, fat mass, and visceral fat. This is the gold standard for documenting body composition changes.
If IGF-1 has not risen meaningfully after 12 weeks of proper dosing and timing, discuss dose adjustment with your clinician. If there is still no response after increasing the dose, pituitary reserve may be insufficient for secretagogue therapy, and direct GH replacement warrants evaluation.
Common Reasons Sermorelin Seems to Take Longer
Several correctable errors account for most reports of "sermorelin not working" or taking unusually long to produce results.
1. Injecting at the wrong time. Morning or afternoon dosing produces a suboptimal GH pulse that competes with high somatostatin tone. Switch to 30 to 60 minutes before bedtime.
2. Eating too close to injection. A meal, especially one containing carbohydrates, within 2 hours of injection suppresses GH release. The insulin spike from food directly antagonizes growth hormone secretion. Fast for at least 2 hours before your bedtime injection.
3. Alcohol before bed. Even 1 to 2 drinks suppress slow-wave sleep and blunt the nocturnal GH pulse that sermorelin amplifies. Eliminating bedtime alcohol is one of the highest-impact changes for sermorelin users.
4. Underdosing. Some compounding pharmacies provide sermorelin at concentrations that result in subtherapeutic doses. Verify that your nightly dose is at least 200 mcg. If you are injecting 100 mcg or less, the stimulus may be insufficient to overcome age-related somatostatin suppression.
5. Poor reconstitution or storage. Sermorelin is a peptide. It degrades rapidly at room temperature and is destroyed by agitation (shaking the vial). Reconstituted sermorelin should be stored refrigerated at 36 to 46 degrees Fahrenheit and used within 28 days. Rolling the vial gently to mix, never shaking, preserves the peptide structure.
6. Unrealistic timeline expectations. If you expect HGH-speed results from a GHRH analog, you will be disappointed at week 4. Sermorelin's benefits are real but gradual. The appropriate comparison is not "week 3 on HGH" but "my baseline vs. month 3 on sermorelin."
For details on proper storage and handling, see our guide on how to inject peptides.
Sermorelin Combined With Other GH Secretagogues
Many clinical protocols combine sermorelin with other peptides to produce stronger or more sustained GH release. The combination approach can accelerate the timeline for noticeable results.
Sermorelin + Ipamorelin
Ipamorelin is a selective GH secretagogue that works through the ghrelin receptor (GHS-R), a completely different receptor than the GHRHR that sermorelin targets. Combining both peptides stimulates GH release through two independent pathways simultaneously, producing a larger pulse than either peptide alone.
Clinical experience suggests the combination can shift the results timeline forward by 2 to 4 weeks compared to sermorelin alone. Sleep improvements may appear within the first week. Energy and recovery changes become noticeable by week 2 to 3. Body composition shifts may begin by week 6 rather than week 8.
The combination also provides a more sustained GH pulse. Sermorelin initiates the pulse; ipamorelin extends it. The result is a broader, higher-amplitude GH release curve that more closely resembles the GH pattern of a healthy young adult. See our detailed tesamorelin vs sermorelin vs ipamorelin comparison for dosing protocols.
Sermorelin + CJC-1295
CJC-1295 is a modified GHRH analog with a dramatically longer half-life. The DAC (drug affinity complex) variant binds to albumin in the blood, extending its half-life to 6 to 8 days. CJC-1295 without DAC (also called Modified GRF 1-29) has a half-life of approximately 30 minutes, still much longer than sermorelin's 10 to 20 minutes.
Adding CJC-1295 to a sermorelin protocol provides baseline GHRH receptor stimulation between sermorelin's bedtime pulses. This sustained stimulation keeps the pituitary primed and responsive, potentially accelerating the pituitary's re-sensitization to GHRH signaling.
Users combining sermorelin with CJC-1295 often report that the body composition phase (typically months 2 to 3 with sermorelin alone) begins at weeks 6 to 8. The IGF-1 response may also be more robust: 20 to 35% above baseline rather than the 15 to 25% typical of sermorelin monotherapy. For detailed stacking dosages, use our CJC-1295/ipamorelin dosage calculator and see our CJC-1295 vs sermorelin comparison.
Who Responds Fastest and Who Needs More Time
Clinical experience reveals clear patterns in response speed. Understanding where you fall helps calibrate expectations.
Fastest responders (results in 2-4 weeks): Adults under 40 with mild GH decline (often from poor sleep, stress, or overtraining rather than age), those who already exercise consistently, non-drinkers with good sleep hygiene, and those using sermorelin in combination with ipamorelin or CJC-1295. These individuals have abundant pituitary reserve and few lifestyle factors suppressing their GH response.
Average responders (results in 4-8 weeks): Adults 40 to 55 with moderate age-related GH decline, moderate exercisers, and those with 1 to 2 correctable lifestyle factors (e.g., occasional alcohol use, suboptimal sleep schedule). This is the majority of sermorelin users.
Slower responders (results in 8-16 weeks): Adults over 55 with significant GH decline, sedentary individuals, those with metabolic syndrome or significant insulin resistance, and those on medications that suppress GH (beta-blockers, some SSRIs, glucocorticoids). These patients benefit most from sermorelin therapy in the long run but need patience through the initial phase.
Non-responders: A small percentage of patients (estimated 5 to 10%) do not achieve meaningful IGF-1 elevation after 12 to 16 weeks of adequate dosing. The most common cause is insufficient pituitary somatotroph reserve, often from aging beyond the point where secretagogue therapy can restore adequate GH output. Direct GH replacement is the appropriate alternative for these individuals.
What Happens When You Stop Sermorelin
Sermorelin does not permanently alter your GH production. When you stop injecting, the pituitary returns to its pre-treatment secretion pattern over 2 to 4 weeks. IGF-1 levels decline toward baseline. The sleep improvements, energy gains, and body composition changes gradually reverse over 2 to 6 months, depending on how long you were on therapy and how much of the benefit was maintained by lifestyle factors (exercise, sleep, diet).
However, unlike synthetic HGH, sermorelin does not suppress your natural GH production while you are using it. There is no "rebound" period of lower-than-baseline GH after stopping. Your pituitary was working harder during therapy, not shut off. When you remove the extra GHRH signal, it simply returns to its previous output level.
Some practitioners recommend cycling sermorelin: 3 to 6 months on, 1 to 2 months off. The rationale is to prevent potential receptor desensitization, though clinical evidence for this is limited. Others maintain patients on continuous therapy for years without apparent loss of efficacy. Discuss cycling strategies with your prescribing clinician based on your IGF-1 trends and symptom response.
For procurement options, see where to buy sermorelin.
Sermorelin Timeline vs. Other Peptide Therapies
How does sermorelin's timeline compare to other popular peptide therapies? Context helps set expectations.
| Peptide | Primary Use | Time to First Noticeable Effect | Time to Full Results |
|---|---|---|---|
| Sermorelin | GH optimization, anti-aging | 1-2 weeks (sleep) | 3-6 months |
| CJC-1295 | GH optimization (long-acting) | 1-2 weeks (sleep) | 3-6 months |
| Ipamorelin | GH pulse stimulation | 1-2 weeks (sleep) | 3-6 months |
| BPC-157 | Tissue repair, gut healing | 3-7 days (pain reduction) | 4-8 weeks |
| TB-500 | Tissue repair, flexibility | 1-2 weeks (reduced inflammation) | 6-12 weeks |
| Semaglutide | Weight loss | 1-3 days (appetite) | 16-20 weeks (full dose) |
Growth hormone secretagogues share a similar timeline because they all work through the same downstream pathway: GH pulses leading to IGF-1 elevation leading to tissue-level effects. The initial changes (sleep, energy) appear quickly because they are direct effects of improved GH pulsatility. The body composition changes take months because they require sustained IGF-1 elevation to drive lipolysis, protein synthesis, and collagen production at scale.
By contrast, tissue repair peptides like BPC-157 work through entirely different mechanisms (angiogenesis, inflammation modulation) with much shorter timelines. And GLP-1 agonists like semaglutide produce rapid appetite suppression through a mechanism unrelated to growth hormone. Comparing sermorelin's timeline to these peptides is comparing different biological processes, not different speeds of the same process. For a comprehensive overview, see our peptide dosage chart.
Frequently Asked Questions
How long does sermorelin take to work for sleep?
Sleep quality improvements are typically the first benefit, appearing within 1 to 2 weeks of nightly injections. Sermorelin amplifies the growth hormone pulse during slow-wave sleep, extending deep sleep duration and reducing nighttime awakenings. Some users report better sleep from the first night, though consistent improvement usually takes 7 to 14 days. See our peptides for sleep guide for complementary strategies.
When will I see fat loss from sermorelin?
Measurable fat loss, particularly visceral abdominal fat, typically begins at months 2 to 3 of consistent therapy. Growth hormone's lipolytic effects require sustained IGF-1 elevation, which takes 8 to 12 weeks to reach optimal levels. Combining sermorelin with resistance training and proper diet accelerates this timeline. Read our detailed sermorelin for fat loss article for protocol specifics.
How long should I take sermorelin before deciding if it works?
Minimum 3 months. Most clinicians recommend a 3-to-6-month trial before evaluating effectiveness. IGF-1 should be tested at baseline and again at 8 to 12 weeks. If IGF-1 has not risen 15 to 25% above baseline after 12 weeks of proper dosing and bedtime administration, discuss dose adjustment with your prescribing clinician. Body composition changes require 3 to 6 months.
Does sermorelin work faster when stacked with ipamorelin or CJC-1295?
Yes. Combining sermorelin with ipamorelin or CJC-1295 stimulates GH release through multiple pathways, producing larger and more sustained GH pulses. Clinical experience suggests the combination shifts the results timeline forward by 2 to 4 weeks. Use our CJC-1295/ipamorelin dosage calculator for stacking protocols.
What is the best time to inject sermorelin?
Inject sermorelin 30 to 60 minutes before bedtime on an empty stomach (2-hour fast). This timing aligns with the body's largest natural GH pulse during early slow-wave sleep. Morning dosing is less effective because somatostatin tone is higher during the day. Eating, especially carbohydrates, within 2 hours of injection blunts GH release by raising insulin. See our how to inject peptides guide for technique details.
How do I know if sermorelin is working?
Track sleep quality (weeks 1-2), energy and recovery (weeks 3-4), and body composition (months 2-3). The definitive test is an IGF-1 blood draw at baseline and 8-12 weeks. A 15-25% rise confirms adequate GH stimulation. If you see sleep and energy improvements but IGF-1 has not moved, the dose may need adjustment. Our peptide dosage chart covers standard dosing ranges.
Is sermorelin the same as HGH?
No. Sermorelin stimulates your pituitary gland to produce growth hormone naturally in pulsatile bursts. HGH is synthetic growth hormone injected directly, bypassing the pituitary. Sermorelin preserves the body's feedback loops and rarely exceeds physiologic GH levels, while HGH can produce supraphysiologic levels with higher risk of side effects. Sermorelin takes longer to show results but is considered safer for long-term use. Learn more in our is sermorelin a steroid explainer.
What happens when you stop taking sermorelin?
GH production returns to pre-treatment levels over 2 to 4 weeks. IGF-1 declines toward baseline. Benefits like improved sleep, energy, and body composition gradually reverse over 2 to 6 months. Unlike HGH, sermorelin does not suppress natural GH production during use, so there is no rebound period of below-baseline GH after stopping. Some clinicians recommend cycling 3-6 months on, 1-2 months off. See where to buy sermorelin for sourcing.
The Bottom Line
Sermorelin works in a predictable sequence: sleep quality improves at weeks 1 to 2, energy and recovery follow at weeks 3 to 4, body composition shifts become measurable at months 2 to 3, and full therapeutic benefits materialize at months 3 to 6. The timeline is slower than direct HGH injection because sermorelin restores your pituitary's natural GH production rather than bypassing it. This preserves physiological feedback loops and produces results within safe, sustainable ranges.
The single most important factor for faster results is protocol compliance: inject at bedtime, fast for 2 hours beforehand, avoid alcohol before sleep, and pair therapy with resistance training. IGF-1 blood testing at baseline and 8 to 12 weeks provides the objective confirmation that the pituitary is responding. A 15 to 25% rise in IGF-1 indicates the therapy is working even before you see the body composition changes.
For stacking protocols that may accelerate the timeline, explore the CJC-1295/ipamorelin dosage calculator. For head-to-head comparisons with other GH secretagogues, read tesamorelin vs sermorelin vs ipamorelin and CJC-1295 vs sermorelin. For safety data and side effect profiles, see is sermorelin safe.
Related articles: - Sermorelin for Fat Loss — detailed mechanism and protocol for GH-driven lipolysis - Is Sermorelin Safe? — side effects, contraindications, and monitoring - Is Sermorelin a Steroid? — classification, legality, and drug testing - Where to Buy Sermorelin — sourcing guide for quality compounding pharmacies - Tesamorelin vs Sermorelin vs Ipamorelin — head-to-head GH secretagogue comparison - CJC-1295 vs Sermorelin — mechanism, half-life, and stacking differences - Peptides for Sleep — comprehensive guide to sleep-enhancing peptides - Peptides for Muscle Growth — anabolic peptide protocols for lean mass - Peptide Dosage Chart — complete reference for all peptide dosing
Helpful Tools
Related Articles
Does Sermorelin Increase Testosterone?
Does sermorelin increase testosterone? Not directly. It boosts GH, which supports testosterone via IGF-1 and improved sleep. Evidence reviewed.
How Much Sermorelin Per Day: Complete Dosage Guide
Sermorelin dosage: 200-500 mcg/day subcutaneous before bedtime. Starting dose, titration, gender-specific protocols, and IGF-1 monitoring.
Tesamorelin Peptide: Uses, Evidence, Risks
Tesamorelin peptide explained: a GHRH analogue FDA-approved as Egrifta for HIV lipodystrophy. What it does to visceral fat, IGF-1, and who should avoid it.
Is Tesamorelin FDA Approved? Status & Facts
Is tesamorelin FDA approved? Yes, as Egrifta for HIV lipodystrophy (2010). Approval timeline, off-label rules, and GH peptide comparison.