
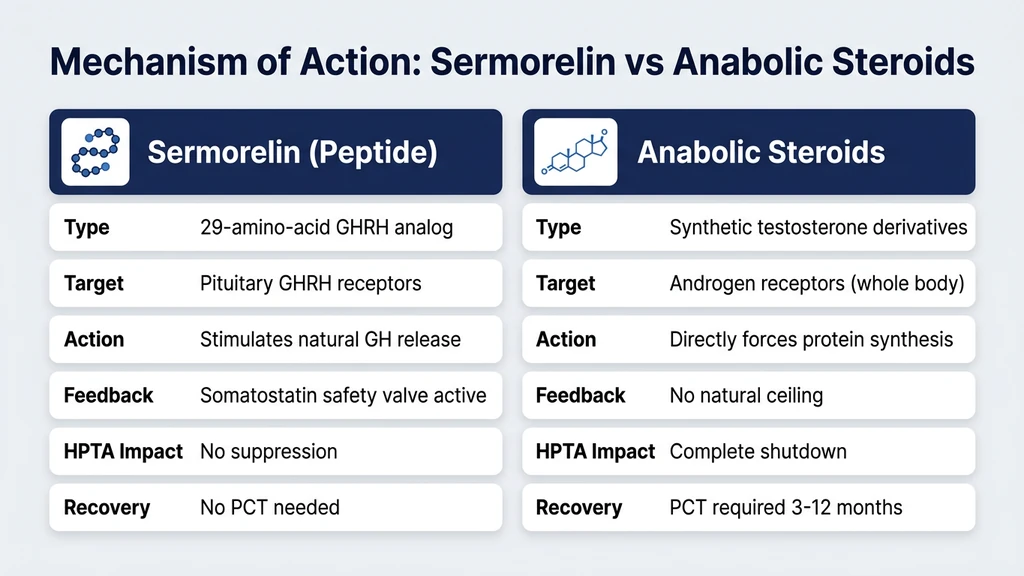
You heard someone at the gym mention sermorelin in the same breath as testosterone and trenbolone. Now you are wondering whether sermorelin belongs in the same category as anabolic steroids. Sermorelin is not a steroid. It is a 29-amino-acid peptide that mimics growth hormone-releasing hormone (GHRH), stimulating your pituitary gland to produce its own growth hormone (Walker, Endocr Pract, 2006). Steroids, by contrast, are four-ringed carbon molecules that bind androgen receptors to directly force muscle protein synthesis.
The confusion is understandable. Both sermorelin and steroids show up in conversations about body composition, performance, and anti-aging. Both involve injections. Both are regulated substances. But the similarities end there. Their molecular structures, mechanisms of action, side effect profiles, legal classifications, and drug testing outcomes differ fundamentally.
| Quick Reference | Sermorelin | Anabolic Steroids |
|---|---|---|
| Chemical class | Peptide (29 amino acids) | Synthetic derivatives of testosterone |
| Molecular weight | 3,358 Da | 288-456 Da (varies by compound) |
| Mechanism | Stimulates pituitary GH release | Binds androgen receptors directly |
| Administration | Subcutaneous injection | Injection, oral, topical |
| FDA status | Previously approved (Geref), discontinued | Schedule III controlled substances |
| Drug testing | Detectable via specific peptide assays | Detected via standard steroid panels |
| Liver toxicity | No documented hepatotoxicity | Oral steroids cause significant liver stress |
| Shutdown risk | No HPTA suppression | Suppresses natural testosterone production |
| Typical cycle | 3-6 months continuous | 8-16 week cycles with PCT |
For a broader overview of peptide safety, read our peptide safety guide. If you are new to the peptide space, start with our getting started guide. To understand sermorelin's fat loss applications specifically, see our sermorelin for fat loss guide.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
What Sermorelin Actually Is
Think of your pituitary gland as a factory that builds growth hormone. Sermorelin is the shift manager who walks in, taps the workers on the shoulder, and says "time to produce." It does not bring any growth hormone with it. It simply tells your body to make more of what it already produces naturally.
Sermorelin acetate is the synthetic version of the first 29 amino acids of human growth hormone-releasing hormone (GHRH 1-29). The full GHRH molecule contains 44 amino acids, but researchers at Tulane University discovered that only the first 29 are needed for biological activity (Ling et al., Biochem Biophys Res Commun, 1984). This truncated version retains full receptor-binding potency while being easier and cheaper to synthesize.
The FDA approved sermorelin as Geref Diagnostic in 1997 for evaluating pituitary function in children with suspected growth hormone deficiency. A therapeutic version, Geref, was approved for treating growth hormone deficiency in children but was later discontinued for commercial reasons, not safety concerns (Walker, Endocr Pract, 2006).
When injected subcutaneously, sermorelin binds to GHRH receptors on somatotroph cells in the anterior pituitary. This binding triggers a signaling cascade that culminates in growth hormone release into the bloodstream. The critical distinction: your pituitary retains its feedback mechanisms. If GH levels rise too high, somatostatin suppresses further release. This built-in safety valve does not exist with direct GH injection or steroid use.
What Anabolic Steroids Actually Are
Anabolic-androgenic steroids (AAS) are synthetic modifications of testosterone, the primary male sex hormone. Their molecular backbone is a four-ringed cyclopentanoperhydrophenanthrene structure, a carbon skeleton shared by all steroid hormones including cortisol, estrogen, and cholesterol. This structure is fundamentally different from a peptide chain.
Testosterone was first isolated in 1935 by Ernst Laqueur. By the 1950s, chemists had created dozens of modified versions designed to amplify the anabolic (muscle-building) effects while minimizing the androgenic (masculinizing) effects (Kicman, Br J Pharmacol, 2008). Common examples include nandrolone, oxandrolone, stanozolol, and trenbolone.
Steroids work by entering muscle cells, binding to androgen receptors in the cytoplasm, and traveling to the nucleus where they directly alter gene transcription. The result is increased protein synthesis, nitrogen retention, and satellite cell activation. This mechanism is forceful and dose-dependent. Double the dose, roughly double the protein synthesis, up to a saturation point.
The problem: androgen receptors exist throughout your body, not just in muscle. Steroids simultaneously affect the liver, heart, skin, prostate, brain, and reproductive organs. The hypothalamic-pituitary-testicular axis (HPTA) detects the exogenous androgens and shuts down natural testosterone production. This suppression is why steroid users require post-cycle therapy (PCT) to restart endogenous hormone production.
Molecular Differences Between Peptides and Steroids
The structural gap between sermorelin and anabolic steroids is so wide that comparing them is like comparing a paragraph of text to a single letter. They belong to entirely different classes of biological molecules.
Chemical Structure
Sermorelin is a polypeptide: a chain of 29 amino acids linked by peptide bonds. Its molecular formula is C149H246N44O42S, with a molecular weight of 3,358 Daltons. The molecule folds into a specific three-dimensional shape that fits GHRH receptors like a key in a lock.
Testosterone, the parent steroid, has the molecular formula C19H28O2 and weighs 288 Daltons. It is a single small molecule with four fused carbon rings. Modified steroids like trenbolone (C18H22O2, 270 Da) and nandrolone (C18H26O2, 274 Da) share this compact ring structure. Sermorelin is roughly 12 times heavier than testosterone at the molecular level.
Receptor Binding
Sermorelin exclusively targets GHRH receptors on pituitary somatotroph cells. These receptors are G-protein coupled receptors (GPCRs) that initiate a cAMP signaling cascade when activated (Mayo, Mol Endocrinol, 1992). The downstream effect is GH secretion. Sermorelin has no affinity for androgen receptors, estrogen receptors, or glucocorticoid receptors.
Anabolic steroids bind androgen receptors (ARs), which are nuclear hormone receptors found in nearly every tissue in the body. When a steroid binds an AR, the receptor-ligand complex translocates to the nucleus and directly alters gene expression. This mechanism is fundamentally different from the indirect, signal-relay approach that sermorelin uses.
Metabolism and Half-Life
Sermorelin has a plasma half-life of approximately 10-20 minutes. Peptidases in the blood rapidly cleave it into individual amino acids that your body recycles through normal protein metabolism (Prakash & Bhargava, IDrugs, 1999). There is no accumulation, no toxic metabolite formation, and no strain on the liver's detoxification pathways.
Anabolic steroids persist much longer. Testosterone enanthate has a half-life of 4-5 days. Nandrolone decanoate lingers for 6-12 days. Oral steroids like stanozolol pass through the liver, where first-pass metabolism creates 17-alpha-alkylated metabolites that stress hepatocytes. Some steroid metabolites remain detectable in urine for months after the last dose.
Mechanism of Action: How Each Works in Your Body
The way sermorelin and steroids produce their effects could not be more different. One asks your body to do more of what it already does. The other overrides your body's control systems entirely.
Sermorelin: The Indirect Amplifier
Sermorelin binds GHRH receptors on the anterior pituitary, triggering growth hormone release in a pulsatile pattern that mimics your body's natural rhythm. GH peaks occur approximately 15-30 minutes after injection, typically administered before bedtime to align with the largest natural GH pulse during deep sleep (Vittone et al., J Clin Endocrinol Metab, 1997).
The released GH then travels to the liver, where it stimulates production of insulin-like growth factor 1 (IGF-1). IGF-1 mediates most of the downstream effects attributed to growth hormone: fat metabolism, muscle protein synthesis, collagen production, bone density maintenance, and cellular repair.
Crucially, somatostatin provides a ceiling. When GH levels reach a certain threshold, somatostatin neurons activate and suppress further GH release regardless of how much sermorelin is present. This negative feedback loop prevents supraphysiological GH spikes. You cannot overdose your way to dangerous GH levels with sermorelin the way you can with direct GH injection or steroid abuse.
Steroids: The Direct Override
Anabolic steroids bypass every regulatory checkpoint. Injected testosterone does not ask the pituitary for permission. It floods androgen receptors throughout the body with concentrations 5-100 times above natural levels, depending on the dose (Bhasin et al., N Engl J Med, 1996).
Bhasin's landmark 1996 study demonstrated that supraphysiological testosterone (600 mg/week) increased fat-free mass by 6.1 kg in 10 weeks even without exercise. With exercise, the gain was 8.6 kg. These results are impressive but come with a cost: the hypothalamus detects the excess androgens and drastically reduces GnRH secretion. LH and FSH plummet. The testes stop producing testosterone and sperm. This shutdown begins within days and may take months to fully reverse after cessation.
Steroid effects are dose-dependent with no built-in ceiling. More compound means more receptor activation means more protein synthesis, up to the point where receptor saturation occurs. This absence of a feedback brake is precisely what makes steroids both effective and dangerous.
Side Effect Profiles Compared
The difference in side effects reflects the difference in mechanisms. Sermorelin works within your body's existing framework. Steroids bulldoze through it.
| Side Effect | Sermorelin | Anabolic Steroids |
|---|---|---|
| Injection site reactions | Mild redness, occasional itching | Pain, swelling, oil-based depot irritation |
| Liver damage | None documented | Oral steroids cause cholestasis, peliosis hepatis |
| Cardiovascular risk | Minimal | LDL increase, HDL decrease, left ventricular hypertrophy |
| Hormonal suppression | None (preserves HPTA) | Complete HPTA shutdown |
| Gynecomastia | Not reported | Common (aromatization to estrogen) |
| Hair loss | Not reported | Accelerated in genetically predisposed users |
| Acne | Not reported | Common, especially back and shoulders |
| Mood changes | Not reported | Aggression, mood swings, depression on cessation |
| Testicular atrophy | Does not occur | Occurs within weeks of use |
| Water retention | Mild (GH-mediated) | Significant (estrogen and androgen-mediated) |
| Insulin resistance | Possible with prolonged use | Possible with prolonged use |
Sermorelin Side Effects in Detail
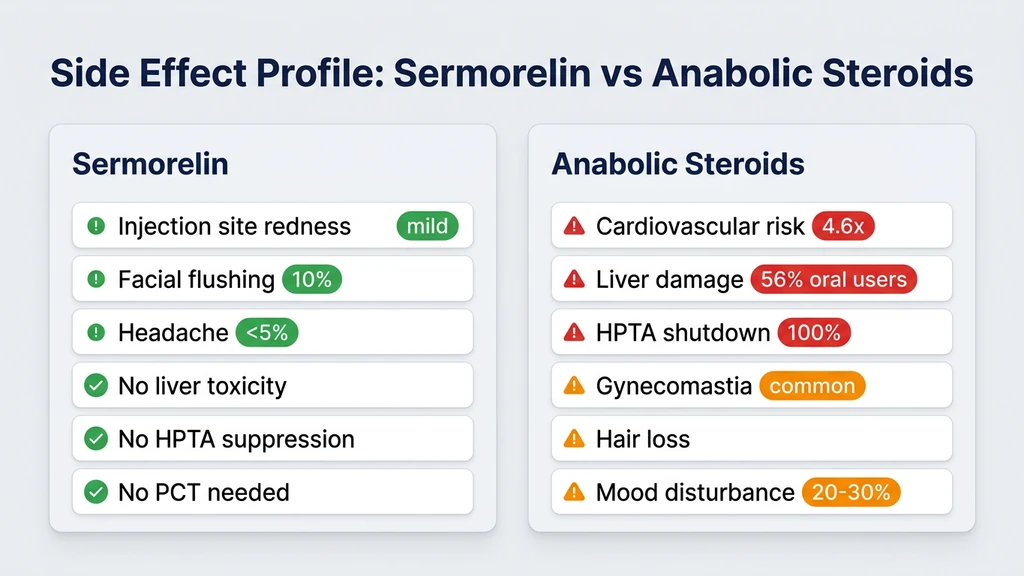
Published side effect data from sermorelin's FDA approval period and subsequent clinical studies shows a remarkably benign profile. The most common adverse events were injection site reactions (redness, swelling, pain) occurring in approximately 17% of patients. Facial flushing occurred in about 10% of subjects. Headache was reported in fewer than 5% (Walker, Endocr Pract, 2006).
Some users report increased hunger within 30-60 minutes of injection, consistent with GH's effect on ghrelin signaling. Tingling or numbness in extremities (paresthesia) occurs occasionally and typically resolves within the first two weeks. Joint stiffness has been reported, likely reflecting GH-mediated fluid retention in synovial spaces.
No cases of sermorelin-induced organ damage have appeared in the medical literature. No deaths have been attributed to sermorelin use. The peptide does not suppress natural hormone axes, meaning discontinuation requires no tapering or post-cycle therapy.
Anabolic Steroid Side Effects in Detail
The adverse effect profile of anabolic steroids fills textbook chapters. Cardiovascular damage is the most serious long-term risk. A 2017 study found that long-term AAS users had significantly reduced left ventricular ejection fraction compared to non-users, indicating impaired heart function (Baggish et al., Circ Heart Fail, 2017). AAS use increases LDL cholesterol by 20-70% while decreasing HDL by 40-70%, creating a pro-atherogenic lipid profile.
Hepatotoxicity from oral 17-alpha-alkylated steroids includes cholestatic jaundice, peliosis hepatis (blood-filled cysts), and hepatocellular carcinoma with chronic use. Injectable steroids largely bypass first-pass metabolism and are less hepatotoxic but still carry cardiovascular and endocrine risks.
HPTA suppression is universal and dose-dependent. Even "mild" steroids like oxandrolone at 20 mg/day reduce testosterone by approximately 45% within two weeks (Lovejoy et al., J Clin Endocrinol Metab, 1995). Higher doses of more potent compounds can suppress testosterone to castrate levels within days. Recovery after cessation takes 3-12 months depending on the compounds used, dosages, and duration of use.
Psychological effects include increased aggression, irritability, and anxiety during use, followed by depression and anhedonia during the post-cycle recovery period when endogenous testosterone is still suppressed.
Legal Status and Regulatory Classification
The legal frameworks governing sermorelin and anabolic steroids reflect the medical establishment's assessment of their respective risk profiles.
Sermorelin Legal Status
Sermorelin is not a controlled substance in the United States. It was FDA-approved as Geref for diagnostic use and as a therapeutic agent for pediatric growth hormone deficiency. The product was voluntarily withdrawn from the market by EMD Serono in 2008 for business reasons, not safety concerns.
Today, sermorelin is available through compounding pharmacies with a valid prescription. Physicians in anti-aging and regenerative medicine clinics commonly prescribe it off-label for adult growth hormone optimization. The 2026 FDA peptide regulatory landscape has increased scrutiny on compounding pharmacies, but sermorelin itself remains a legally prescribable medication.
Some states have additional restrictions on peptide prescribing. Always verify the legal status in your jurisdiction. For sourcing options, see our guide on where to buy peptides in 2026.
Anabolic Steroid Legal Status
Anabolic steroids are Schedule III controlled substances under the Anabolic Steroids Control Act of 1990, amended in 2004 to include prohormones. Possession without a prescription carries federal penalties of up to one year imprisonment for a first offense. Distribution carries penalties of up to five years.
Steroids are legitimately prescribed for hypogonadism, delayed puberty, muscle-wasting diseases (HIV/AIDS, cancer), and certain anemias. These prescriptions require documented medical necessity and ongoing monitoring. Using steroids purely for physique or performance enhancement falls outside approved medical indications.
The legal distinction is stark: you can walk into a telemedicine clinic and legally obtain a sermorelin prescription for age-related GH decline. Attempting the same for testosterone without documented hypogonadism (total testosterone below approximately 300 ng/dL with symptoms) is legally and medically more complex.
Drug Testing: Will Sermorelin Show Up as a Steroid?
Athletes and professionals subject to drug testing need to understand exactly how each substance is detected and classified.
Sermorelin will not trigger a positive result on any standard anabolic steroid panel. Steroid tests look for testosterone metabolites (epitestosterone ratio), nandrolone metabolites (19-norandrosterone), stanozolol metabolites, and similar steroid-specific markers. Sermorelin is a peptide and produces none of these metabolites.
However, sermorelin is detectable through specialized peptide hormone assays. The World Anti-Doping Agency (WADA) classifies growth hormone-releasing peptides and their analogs under category S2.3 (Growth Hormone Releasing Factors) of the Prohibited List. WADA-accredited laboratories use liquid chromatography-tandem mass spectrometry (LC-MS/MS) to identify sermorelin and other GHRH analogs in urine samples.
The practical implications vary by context:
Professional and Olympic sports. Sermorelin is prohibited at all times (in and out of competition) under WADA rules. Detection windows range from 24 to 72 hours after the last injection, though methods continue improving.
Workplace drug testing. Standard employment drug panels (5-panel, 10-panel) do not test for sermorelin or any peptide hormones. These panels screen for amphetamines, cannabinoids, cocaine, opiates, and PCP, with expanded panels adding benzodiazepines, barbiturates, and methadone.
Military drug testing. The Department of Defense standard panel does not include peptide hormones. However, commanders can request expanded testing that may include growth hormone markers.
Law enforcement. Testing policies vary by department. Most standard panels do not include peptide hormones.
| Testing Context | Tests for Sermorelin? | Tests for Steroids? |
|---|---|---|
| WADA/Olympic | Yes (LC-MS/MS) | Yes (GC-MS, IRMS) |
| Standard workplace (5/10 panel) | No | No |
| NCAA | Yes (peptide panel) | Yes (steroid panel) |
| Military (standard) | No | Possible |
| CrossFit Games | Yes | Yes |
Why People Confuse Sermorelin With Steroids
The peptide-steroid confusion is not limited to sermorelin. It reflects broader misunderstandings about performance-related compounds. Several factors drive this misconception.
Shared Context
Sermorelin and steroids inhabit the same conversational ecosystem. They are discussed in the same gym forums, prescribed at the same anti-aging clinics, and sold by the same compounding pharmacies. When a newcomer hears both mentioned together, they naturally assume the substances are similar. The social context creates a false equivalence that the chemistry does not support.
Injection Administration
Most people associate injections with "serious" substances, and steroids are the most culturally visible injectable performance compound. When someone learns that sermorelin requires subcutaneous injections, the visual similarity to steroid use creates a mental link. The injection site differs (subcutaneous abdominal fat for sermorelin vs intramuscular for most oil-based steroids), but the syringe looks the same from across the room. For proper technique, see our guide on how to inject BPC-157, which covers subcutaneous injection fundamentals applicable to sermorelin.
Overlapping Goals
Both sermorelin and steroids appeal to people seeking improved body composition. Sermorelin increases GH, which promotes fat oxidation and supports lean mass. Steroids directly build muscle. The desired outcomes overlap even though the mechanisms, magnitudes, and risks diverge dramatically. A person who lost 15 pounds of fat on sermorelin and a person who gained 20 pounds of muscle on testosterone are both "using something that changed their body."
For the fat loss dimension of sermorelin specifically, see our sermorelin for fat loss breakdown.
Media and Regulatory Lumping
News coverage and regulatory actions sometimes group peptides and steroids together under broad labels like "performance-enhancing drugs" or "hormone therapies." The FDA's increased scrutiny of compounding pharmacies in 2025-2026 has further blurred the line by targeting both peptide and steroid products in the same enforcement actions. This regulatory conflation reinforces public perception that peptides and steroids are two flavors of the same thing. Our FDA peptide crackdown analysis breaks down what this means for legitimate peptide users.
Sermorelin vs Other Growth Hormone Secretagogues
Sermorelin belongs to a family of compounds called growth hormone secretagogues (GHS). Understanding where it sits within this family helps clarify why it is sometimes confused not only with steroids but also with other GH-related compounds.
CJC-1295 is a modified GHRH analog with a much longer half-life (days vs minutes) due to drug affinity complex (DAC) technology. It binds the same GHRH receptor as sermorelin but provides sustained rather than pulsatile GH release. Use our CJC-1295 + Ipamorelin dosage calculator for dosing guidance.
Ipamorelin is a growth hormone-releasing peptide (GHRP) that works through the ghrelin receptor, not the GHRH receptor. It complements sermorelin by stimulating GH release through a separate pathway. The two are frequently stacked for synergistic effects. See our peptide stacking guide for combination protocols.
MK-677 (ibutamoren) is an oral growth hormone secretagogue that also acts through the ghrelin receptor. It is not technically a peptide but a non-peptide mimetic. Its oral bioavailability and 24-hour half-life make it convenient but also more likely to produce side effects like increased appetite and water retention.
GHRP-6 is another ghrelin receptor agonist with potent GH-releasing effects but significantly more appetite stimulation than ipamorelin or sermorelin. Hexarelin is the most potent GHRP but carries a higher risk of cortisol and prolactin elevation. For hexarelin-specific dosing, see our hexarelin dosage guide.
HGH Fragment 176-191 is a modified fragment of human growth hormone itself, not a secretagogue. It targets fat metabolism without the growth-promoting effects of full-length GH. Despite containing part of the GH molecule, it is still a peptide, not a steroid.
None of these compounds are steroids. None bind androgen receptors. None suppress the HPTA. They represent a pharmacologically distinct category that happens to influence some of the same endpoints (body composition, recovery, anti-aging) through entirely different pathways.
When Would a Doctor Prescribe Sermorelin Instead of Steroids?
The clinical indications for sermorelin and anabolic steroids barely overlap. They treat different deficiencies through different mechanisms.
Sermorelin Prescribing Scenarios
Physicians prescribe sermorelin for adults with declining growth hormone levels, typically presenting with increased abdominal fat, decreased muscle mass, poor sleep quality, reduced exercise capacity, and low IGF-1 on bloodwork. The typical patient is 35-65 years old with IGF-1 below 200 ng/mL. Dosing ranges from 200-500 mcg injected subcutaneously at bedtime, 5-6 days per week.
Sermorelin is preferred over direct GH injection when the pituitary is still functional. The logic is straightforward: if the factory can still produce GH, stimulating it is safer and more physiologically natural than bypassing it entirely. Sermorelin also costs significantly less than pharmaceutical GH ($150-300/month vs $800-2,000/month). Use our peptide cost calculator to estimate expenses.
For dosing reference across multiple peptides, consult our peptide dosage chart.
Anabolic Steroid Prescribing Scenarios
Testosterone replacement therapy (TRT) is prescribed for men with documented hypogonadism: total testosterone consistently below 300 ng/dL with symptoms (fatigue, low libido, depression, muscle loss). The cause may be primary (testicular failure) or secondary (pituitary/hypothalamic dysfunction).
Testosterone is also prescribed for delayed puberty, breast cancer (in specific contexts), anemia unresponsive to other treatments, and muscle wasting from HIV/AIDS or chronic illness. These are legitimate medical uses backed by extensive clinical trial evidence.
A physician would never prescribe sermorelin to treat hypogonadism, and would not prescribe testosterone to treat growth hormone deficiency. The conditions require different hormonal interventions. A patient with both deficiencies might receive both, but they address separate axes of the endocrine system.
Can You Use Sermorelin and Steroids Together?
Some users in the performance optimization space combine sermorelin with testosterone replacement therapy. This is a medically supervised practice in some anti-aging clinics, not a recommendation for self-administration.
The theoretical rationale: testosterone builds muscle directly through androgen receptor activation, while sermorelin-stimulated GH promotes fat metabolism and tissue repair. The combination addresses both the anabolic and metabolic dimensions of body composition. Some clinicians report that adding sermorelin to TRT protocols improves fat loss outcomes beyond what testosterone alone achieves.
The practical concern: stacking compounds increases the number of variables affecting your physiology. Monitoring becomes more complex. If a side effect emerges, identifying the cause requires systematic elimination. Blood panels must track not only testosterone, estradiol, and hematocrit (standard TRT markers) but also IGF-1, fasting glucose, and insulin.
Use the peptide interaction checker to evaluate potential interactions between sermorelin and other compounds in your protocol. For broader stacking principles, see the peptide stacking guide.
If you are considering this combination, work with a physician experienced in both hormone replacement therapy and peptide protocols. Self-administering testosterone without medical supervision carries legal and health risks that do not apply to sermorelin alone.
Practical Considerations for Sermorelin Users
If you have determined that sermorelin, not steroids, aligns with your goals, these practical points will help you navigate the process.
Storage and Reconstitution
Sermorelin is supplied as a lyophilized (freeze-dried) powder that requires reconstitution with bacteriostatic water before injection. Once reconstituted, store the vial at 36-46 degrees Fahrenheit (2-8 degrees Celsius). Reconstituted sermorelin remains potent for approximately 3-4 weeks when properly refrigerated.
Use our peptide reconstitution calculator to determine the correct water volume for your vial concentration. For storage best practices, read our how to store peptides guide. To understand shelf life, see how long do reconstituted peptides last.
Timing and Dosing Protocol
Inject sermorelin 30 minutes before bedtime on an empty stomach (no food for at least 90 minutes prior). Growth hormone release peaks during deep sleep, and timing your sermorelin injection to align with this window produces the strongest pulsatile response (Vittone et al., J Clin Endocrinol Metab, 1997).
Standard dosing: 200-300 mcg subcutaneously, 5 days on, 2 days off. Some protocols use daily injection for the first 4 weeks, then reduce to 5 days per week. Cycling is recommended: 3-6 months on, 1-2 months off. This prevents receptor desensitization and maintains pituitary responsiveness.
Eating before injection blunts the GH response. Carbohydrates and fats trigger insulin release, which directly opposes GH secretion. If you must eat, keep the pre-injection meal to lean protein only.
Monitoring Bloodwork
Baseline bloodwork before starting sermorelin should include IGF-1, fasting glucose, fasting insulin, a comprehensive metabolic panel, and a complete blood count. Recheck IGF-1 at weeks 4 and 12. Target IGF-1 in the upper third of the age-adjusted reference range (roughly 200-300 ng/mL for adults 30-60).
If IGF-1 rises above 350 ng/mL, reduce the dose. Chronically elevated IGF-1 is associated with increased risk of certain cancers in epidemiological studies, though a causal link from short-term peptide use has not been established. Monitor fasting glucose as well: GH is a counter-regulatory hormone that opposes insulin, and prolonged elevation can worsen insulin sensitivity.
Sourcing Quality Sermorelin
Peptide purity determines both safety and efficacy. Sermorelin from unregulated sources may contain truncated peptide fragments, bacterial endotoxins, or residual solvents. Verify third-party certificates of analysis (COA) showing HPLC purity above 98% and mass spectrometry confirmation of the correct molecular weight (3,358 Da).
Compounding pharmacies operating under a valid prescription offer the most reliable sourcing. For research-grade options, see our where to buy peptides guide and Peptide Sciences alternatives.
The Quantified Risk: Sermorelin vs Steroid Safety Data
Numbers tell the story more clearly than qualitative comparisons. The following data quantifies the actual risk differential between these two classes of compounds.
Sermorelin was used in FDA-supervised clinical trials involving over 800 pediatric patients with no serious adverse events attributed to the peptide (Walker, Endocr Pract, 2006). The most common complaint was injection site irritation. No cardiovascular events, liver damage, endocrine disruption, or deaths were reported.
Anabolic steroid adverse events are extensively documented. A systematic review by Pope et al. (2014) found that AAS users had a 4.6-fold increased risk of cardiovascular events compared to non-users (Pope et al., Endocr Rev, 2014). Baggish et al. (2017) showed that AAS users had mean left ventricular ejection fractions of 52% versus 63% in non-users, a clinically significant difference indicating cardiac dysfunction (Baggish et al., Circ Heart Fail, 2017).
Liver toxicity from oral steroids produces measurable enzyme elevations. A study of bodybuilders using oral AAS found ALT elevations exceeding 3x the upper limit of normal in 56% of participants. Peliosis hepatis, a potentially fatal condition of blood-filled liver cysts, has been reported in numerous case studies of chronic oral AAS users.
| Risk Metric | Sermorelin | Anabolic Steroids |
|---|---|---|
| Cardiovascular event risk increase | Not documented | 4.6x baseline (Pope et al., 2014) |
| Liver enzyme elevation (>3x ULN) | 0% in clinical trials | 56% of oral AAS users |
| HPTA suppression | 0% | 100% (dose-dependent severity) |
| Deaths attributed to the compound | 0 in published literature | Multiple case reports |
| Psychiatric adverse events | Not documented | 20-30% of users report mood disturbance |
For related peptide safety information, see our peptide safety guide. For understanding how other peptides compare in terms of safety, see our articles on tesamorelin dosage for fat loss and MOTS-c peptide dosage.
Related Peptide Questions
Sermorelin for Fat Loss Sermorelin's primary appeal for many users is its fat metabolism effects. GH increases lipolysis, and sermorelin's pulsatile GH stimulation targets visceral fat preferentially.
Peptides for Joint Pain If joint repair is your goal rather than muscle growth, several peptides outperform both sermorelin and steroids for connective tissue healing.
Peptides for Anxiety Some users explore peptides for cognitive and mood benefits. Sermorelin's GH-boosting effects may improve sleep quality, which indirectly supports mental health.
Peptides for Immune System Growth hormone has immunomodulatory properties. Sermorelin's GH stimulation may support immune function, particularly the thymosin-related pathway. See also thymosin alpha-1 benefits.
BPC-157 Muscle Growth For tissue repair rather than direct anabolism, BPC-157 offers a completely different approach to recovery that complements rather than replaces sermorelin.
Does BPC-157 Cause Liver Damage? Liver safety is a common concern with any injectable compound. BPC-157 has shown hepatoprotective rather than hepatotoxic effects in animal studies.
Frequently Asked Questions
Is sermorelin classified as an anabolic steroid?
No. Sermorelin is a 29-amino-acid peptide that mimics growth hormone-releasing hormone (GHRH). Anabolic steroids are synthetic derivatives of testosterone with a four-ringed carbon structure. They belong to completely different molecular classes and work through entirely separate receptor systems. Sermorelin targets GHRH receptors on the pituitary. Steroids bind androgen receptors throughout the body.
Will sermorelin show up on a steroid drug test?
Sermorelin does not trigger positive results on standard anabolic steroid panels. However, WADA-accredited labs and some sports organizations use specialized LC-MS/MS assays that detect peptide hormones including sermorelin. Standard workplace drug tests (5-panel, 10-panel) do not screen for any peptide hormones.
Does sermorelin suppress natural testosterone like steroids do?
No. Sermorelin acts exclusively on the growth hormone axis through pituitary GHRH receptors. It does not interact with the hypothalamic-pituitary-testicular axis (HPTA) that governs testosterone production. You will not experience testosterone suppression, testicular atrophy, or require post-cycle therapy after discontinuing sermorelin.
Is sermorelin safer than anabolic steroids?
Published evidence supports a substantially better safety profile. Sermorelin showed no serious adverse events in FDA clinical trials involving over 800 patients. Anabolic steroid use increases cardiovascular event risk by 4.6-fold (Pope et al., 2014), causes liver damage in 56% of oral users, and universally suppresses natural hormone production. The risk differential is significant.
Can sermorelin build muscle like steroids?
Sermorelin promotes modest lean mass gains through indirect GH stimulation, typically 2-4 pounds over 3-6 months. Supraphysiological steroid doses can add 10-20 pounds of muscle in 8-16 weeks. The magnitudes are not comparable. Sermorelin optimizes body composition gradually within physiological limits. Steroids force growth beyond natural capacity.
Do I need a prescription for sermorelin?
Yes. Sermorelin is a prescription medication available through compounding pharmacies. It is not a controlled substance like anabolic steroids (Schedule III). A physician can prescribe sermorelin for off-label use in adults with declining GH levels. Some telemedicine clinics specialize in peptide therapy prescriptions.
Is sermorelin legal for athletes?
Sermorelin is prohibited by WADA under category S2.3 (Growth Hormone Releasing Factors). It is banned in all Olympic, NCAA, and most professional sports at all times, both in and out of competition. For non-athletes, sermorelin is legal with a prescription in the United States and most countries.
What happens if I stop taking sermorelin?
GH levels return to pre-treatment baseline within days of discontinuation. There is no withdrawal syndrome, no hormonal crash, and no need for post-cycle therapy. Your pituitary resumes its normal GH secretion pattern. This contrasts sharply with steroid cessation, which can leave users with suppressed testosterone for months.
The Bottom Line
Sermorelin is not a steroid by any measure: not by molecular structure, not by mechanism, not by receptor target, not by side effect profile, not by legal classification. It is a 29-amino-acid peptide that politely asks your pituitary gland to release more growth hormone. Anabolic steroids are four-ringed carbon molecules that override your endocrine system by force.
The confusion persists because both compounds inhabit the same cultural space of performance and anti-aging medicine. Both involve injections. Both change body composition. But aspirin and morphine both relieve pain, and no one confuses the two. The mechanism, magnitude, and risk determine the category, not the outcome.
If your goal is modest, physiologically bounded improvement in body composition, sleep quality, and recovery, sermorelin operates within your body's own regulatory framework. If you are chasing dramatic muscle gains beyond natural limits, that is the domain of anabolic steroids, with commensurately greater risk.
Explore the full sermorelin peptide profile for detailed dosing and mechanism data. Use the peptide reconstitution calculator to prepare your vials correctly. For fat loss protocols, read sermorelin for fat loss. Compare sermorelin with other secretagogues using our peptide stack calculator. And for the big picture on safe peptide use, return to the peptide safety guide.
The more useful comparison is against growth hormone itself. HGH or peptides covers what each does to your own pituitary, and where the legal line sits.
Helpful Tools
Related Articles
Does Sermorelin Increase Testosterone?
Does sermorelin increase testosterone? Not directly. It boosts GH, which supports testosterone via IGF-1 and improved sleep. Evidence reviewed.
How Much Sermorelin Per Day: Complete Dosage Guide
Sermorelin dosage: 200-500 mcg/day subcutaneous before bedtime. Starting dose, titration, gender-specific protocols, and IGF-1 monitoring.
CJC-1295 vs Sermorelin: Half-Life and Dosing
CJC-1295 vs sermorelin: half-life 6-8 days vs 10-20 min, GH output 2-10x vs physiologic pulse, cost, FDA status, and who picks which.
Peptides vs Steroids: Key Differences Explained
Peptides vs steroids compared: mechanism, side effects, legal status, muscle building, fat loss, and recovery. A clear, research-backed guide for newcomers.