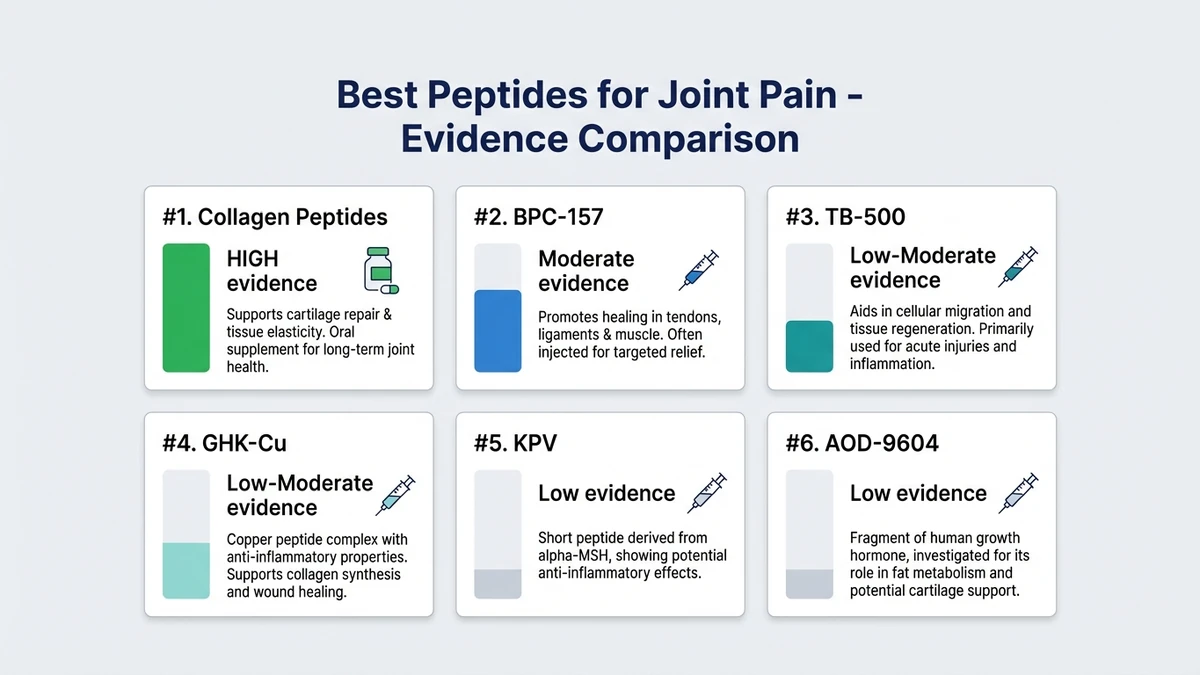
Six peptides have research supporting their use for joint pain: BPC-157, TB-500, collagen peptides, GHK-Cu, KPV, and AOD-9604. They differ sharply in evidence quality.
Collagen peptides have multiple randomized controlled trials in human patients. BPC-157 has one human joint study and 35 preclinical studies in orthopedic applications. The rest rely on preclinical data alone.
Each peptide is ranked by the strength of its evidence, with specific study data (sample sizes, p-values, WOMAC scores), dosage protocols, stacking strategies, and safety warnings. Every claim links to its source.
Most articles on peptides for joint pain are published by clinics selling peptide therapy. This is an independent research guide. We have no product to sell and no financial stake in which peptide you choose.
Quick comparison:
| Peptide | Best For | Evidence | Route | Protocol |
|---|---|---|---|---|
| Collagen Peptides | Osteoarthritis, chronic pain | HIGH (multiple RCTs) | Oral | 3-10g/day, 12-24 weeks |
| BPC-157 | Knee pain, localized injury | Moderate (1 human + 35 animal) | Injection | 250-500 mcg/day, 4-8 weeks |
| TB-500 | Systemic repair, multiple joints | Low-Moderate (animal only) | Injection | 2-2.5 mg 2x/week, 4-6 weeks |
| GHK-Cu | Cartilage remodeling, aging joints | Low-Moderate (in vitro + animal) | Injection/topical | 1-2 mg/day, 4-8 weeks |
| KPV | Inflammatory arthritis | Low (animal models) | Injection/oral | 200-500 mcg/day, 4-8 weeks |
| AOD-9604 | Cartilage protection, OA prevention | Low (animal models) | Injection | 250-300 mcg/day, 8-12 weeks |
Evidence grading: HIGH = multiple human RCTs with statistical significance. Moderate = limited human data plus strong animal evidence. Low-Moderate = robust animal data, no human RCTs. Low = promising preclinical only.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
How Peptides Work for Joint Pain
Peptides are short chains of amino acids that act as signaling molecules. Unlike NSAIDs, which block pain signals without addressing tissue damage, peptides involved in joint repair target four biological mechanisms.
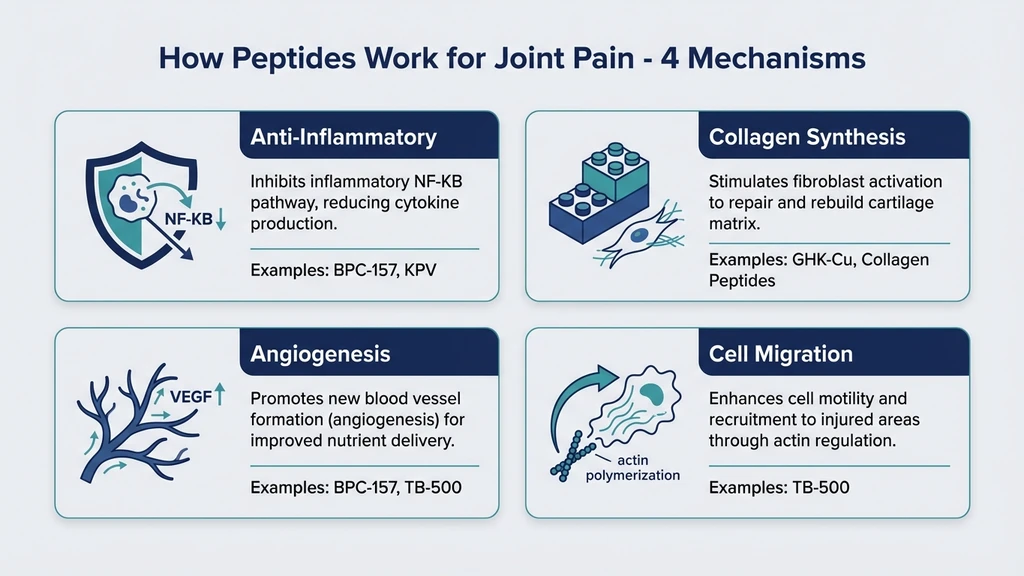
Anti-inflammatory action. Peptides like BPC-157 and KPV modulate cytokines (TNF-alpha, IL-1beta, IL-6) and inhibit the NF-kB inflammatory pathway. This is targeted inflammation reduction. NSAIDs suppress inflammation broadly, damaging the stomach lining over time. Peptides are more selective.
Collagen synthesis. Joint cartilage is primarily type II collagen. Peptides including GHK-Cu and collagen peptides stimulate fibroblast and chondrocyte activity, increasing collagen and proteoglycan production in damaged cartilage.
Angiogenesis. BPC-157 and TB-500 promote new blood vessel formation through VEGF upregulation. Cartilage and tendons are notoriously avascular. Poor blood supply is the primary reason joint injuries heal slowly.
Cell migration. TB-500 accelerates cell migration to injury sites through actin polymerization. This gets repair cells where they are needed faster.
The central distinction: traditional joint treatments manage symptoms. Peptides aim to repair the underlying tissue damage. A 2025 systematic review of BPC-157 in orthopedic applications confirmed improved structural, functional, and biomechanical outcomes across muscle, tendon, ligament, and bone injuries in 36 studies.
The 6 Best Peptides for Joint Pain (Ranked by Evidence)
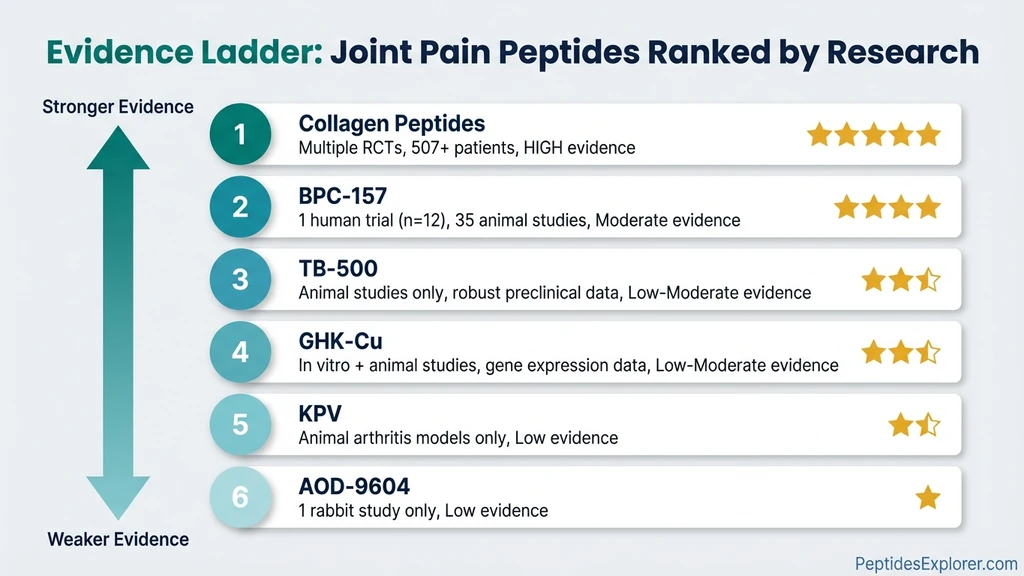
Six peptides with published research relevant to joint pain, ranked by evidence quality. Human trials and animal models are reported separately. The distinction matters.
#1 Collagen Peptides — Strongest Human Evidence for Joint Pain
Collagen peptides are hydrolyzed collagen broken into bioactive fragments, typically 2-10 kDa molecular weight. They are the only peptide on this list with multiple randomized controlled trials for joint pain in human patients.
The evidence:
A 2025 RCT published in Frontiers in Nutrition randomized 80 patients to 3,000 mg/day low-molecular-weight collagen peptides or placebo for 180 days. The collagen group showed significant WOMAC pain score improvement: -1.90 ± 4.14 versus +0.61 ± 3.97 for placebo (p=0.006). Physical function also improved significantly (p=0.035). No adverse events were reported.
A second RCT tested 4g/day low-molecular-weight collagen peptides for 12 weeks in osteoarthritis patients. WOMAC pain and VAS scores decreased significantly versus placebo.
A meta-analysis of 4 trials totaling 507 patients found statistically significant pain reduction in collagen peptide groups compared to placebo.
A bioactive collagen peptide trial reported 38% improvement in activity-related pain and 39% improvement in resting pain after 5g/day for 12 weeks.
A 24-week athlete study found collagen hydrolysate reduced activity-related joint pain in athletes with functional knee problems.
Mechanism: Collagen peptides provide building blocks for type II collagen synthesis and signal chondrocytes to produce more collagen and proteoglycans in cartilage matrix.
Dosage: 3-10g/day oral, minimum 12 weeks for significant results. Most trials used 3-5g/day.
Advantages: Oral administration, excellent safety profile, available without prescription, legal everywhere, strongest clinical evidence of any peptide for joints.
Limitations: Slow onset compared to injectable peptides. Requires consistent daily use for 3+ months. Not a fast solution for acute joint injuries.
Most articles about peptides for joint pain ignore collagen peptides entirely because they focus on injectable peptides. The gap is in media coverage, not in evidence. Collagen peptides have more human data supporting their use for joint pain than every other peptide on this list combined.
#2 BPC-157 — Best for Localized Joint Pain and Knee Injuries
BPC-157 is a 15-amino acid synthetic peptide derived from a protein found in human gastric juice. It is the most studied injectable peptide for musculoskeletal injuries.
The evidence:
Lee et al. (2021) conducted the only human study on BPC-157 for joint pain. The study included 17 patients total. In the BPC-157-only group (12 patients), 11 of 12 (91.6%) reported significant improvement. A 2025 systematic review analyzing this data reported that 7 of 12 patients maintained symptom improvement beyond 6 months.
A 2025 systematic review analyzed 36 articles (35 preclinical, 1 clinical) on BPC-157 in orthopedic applications. The review found improved structural, functional, and biomechanical outcomes across injury types. A separate narrative review titled "Regeneration or Risk?" acknowledged the promising preclinical evidence but stressed the critical need for larger human trials.
Mechanism: VEGF upregulation drives new blood vessel formation around damaged joints. BPC-157 also modulates the nitric oxide system, activates the FAK-paxillin pathway for fibroblast migration, and promotes collagen deposition at injury sites.
Dosage for joint pain: 250-500 mcg/day subcutaneous injection near the affected joint. Clinical settings use intra-articular injection for direct delivery. Protocols run 4-8 weeks. Use our BPC-157 dosage calculator for precise dosing.
Advantages: Targets specific joints. Strong preclinical evidence. Can combine with other peptides. Fast-acting (1-2 weeks for initial relief).
Limitations: FDA Category 2 substance. Cannot be legally compounded by US pharmacies. WADA banned. Only one human joint study with 12 patients. No long-term safety data beyond 6 months.
For more on this peptide, see our BPC-157 profile, BPC-157 side effects guide, BPC-157 before and after results, and BPC-157 and alcohol interactions.
By joint location: The only human trial was knee-specific. For shoulder, hip, or elbow pain, the same subcutaneous injection protocol applies; inject near the affected joint. For back or spinal pain, systemic TB-500 may be more appropriate than localized BPC-157 injection.
#3 TB-500 — Best for Systemic Joint Repair and Multiple Joints
TB-500 is a synthetic fragment of Thymosin Beta-4, a 43-amino acid protein present in nearly every human cell. Where BPC-157 targets a specific joint, TB-500 works systemically.
The evidence:
Grant et al. (2002) found a 20-fold increase in Thymosin Beta-4 mRNA expression in mechanically loaded cartilage. The study also showed increased pro-MMP-9 expression, indicating active cartilage remodeling. This study established that TB4 responds directly to joint stress.
No human clinical trials exist for TB-500 in joint pain.
Mechanism: Actin polymerization accelerates cell migration to injury sites. VEGF upregulation promotes blood vessel formation in avascular joint tissue. NF-kB suppression reduces joint inflammation. TB-500 also reorganizes collagen deposition, reducing scar tissue formation.
Why it pairs with BPC-157: BPC-157 delivers localized repair to a specific joint. TB-500 provides systemic healing. Together they address both the primary injury and compensatory damage from altered movement patterns.
Dosage: Loading phase of 2-2.5 mg twice per week for 4-6 weeks, then maintenance at 2 mg/week. See our TB-500 dosage chart for detailed protocols and our TB-500 dosage calculator for precise reconstitution.
Advantages: Systemic action treats multiple joints simultaneously. Reduces scar tissue. Long half-life allows less frequent dosing.
Limitations: No human clinical trials. All evidence from animal models. WADA banned in competitive sports.
#4 GHK-Cu — Best for Cartilage Remodeling in Aging Joints
GHK-Cu is a naturally occurring copper-binding tripeptide. Plasma levels decline significantly after age 25, which correlates with reduced tissue repair capacity.
The evidence:
Pickart et al. (2018) documented that GHK-Cu modulates over 4,000 human genes involved in tissue repair, immune function, and inflammation. Relevant to joints, GHK-Cu stimulates osteoblast activity, promotes chondrocyte function, increases type I collagen synthesis, and boosts glycosaminoglycan production.
Anti-inflammatory effects include reduced TNF-alpha and IL-6 expression and increased superoxide dismutase activity.
No joint-specific human clinical trials exist. Evidence is extrapolated from wound healing studies and in vitro chondrocyte research.
Mechanism: GHK-Cu acts as a gene expression modulator. It resets gene activity patterns in damaged tissue toward a healthier profile, upregulating repair genes and downregulating inflammatory genes.
Dosage: 1-2 mg/day subcutaneous injection. Topical application for accessible joints (fingers, wrists, knees). Protocols run 4-8 weeks.
Advantages: Dual route: injectable for deep joints, topical for superficial joints. Naturally occurring compound. Broad regenerative profile beyond joints alone.
Limitations: No joint-specific human RCTs. Evidence extrapolated from other tissue types. Copper toxicity possible at excessive doses. Contraindicated in Wilson's disease.
#5 KPV — Best for Inflammatory Arthritis and Autoimmune Joint Pain
KPV is a tripeptide (Lys-Pro-Val) derived from the C-terminal end of alpha-melanocyte-stimulating hormone (alpha-MSH). It targets inflammation at its source rather than broadly suppressing the immune system.
The evidence:
Getting et al. (2005) administered repeated IP injections of alpha-MSH fragments including KPV to rats with adjuvant-induced arthritis. The treatment significantly attenuated both clinical and histological signs of arthritis. Anti-inflammatory effects were comparable to prednisolone, without the weight gain, metabolic disruption, and bone density loss caused by chronic steroid use.
Mechanism: NF-kB pathway inhibition. NLRP3 inflammasome suppression. Macrophage polarization from pro-inflammatory M1 to anti-inflammatory M2 phenotype. Direct reduction of TNF-alpha, IL-1beta, and IL-6.
Dosage: 200-500 mcg/day. Both oral and subcutaneous injection are effective. Oral KPV survives digestion and acts on gut-associated lymphoid tissue, which modulates systemic inflammation.
Advantages: Targets autoimmune-driven joint inflammation specifically. Does not suppress immune function broadly. Effective orally. No steroid-related side effects.
Limitations: Animal models only. No human trials for joint pain or arthritis. Limited research compared to BPC-157 or collagen peptides.
For complete KPV dosing protocols and stacking strategies, see the KPV Dosage Guide.
#6 AOD-9604 — Best for Cartilage Protection and Osteoarthritis Prevention
AOD-9604 consists of amino acids 176-191 from human growth hormone with a tyrosine modification. Originally developed for fat loss, animal research suggests cartilage-protective properties.
The evidence:
Kwon et al. (2015) tested intra-articular AOD-9604 in a collagenase-induced rabbit osteoarthritis model. AOD-9604 enhanced cartilage regeneration. Combined with hyaluronic acid, it was more effective than either treatment alone. The combination group showed significantly lower cartilage degeneration scores and shorter lameness periods.
Mechanism: Increases collagen and proteoglycan production in cartilage. Promotes chondrocyte activity. May protect existing cartilage from enzymatic degradation.
Dosage: 250-300 mcg/day subcutaneous injection. Clinical research used intra-articular injection. Protocols run 8-12 weeks.
Advantages: Combination with hyaluronic acid shows synergy. Targets cartilage preservation specifically. FDA GRAS status for oral fat-loss use suggests a reasonable safety baseline.
Limitations: One rabbit study. No human joint trials. FDA GRAS status applies only to oral fat-loss use, not to injection for joint repair.
What Are the Best Peptide Stacks for Joint Pain?
Single peptides produce results. Stacking compounds them. Three protocols cover most joint pain scenarios.
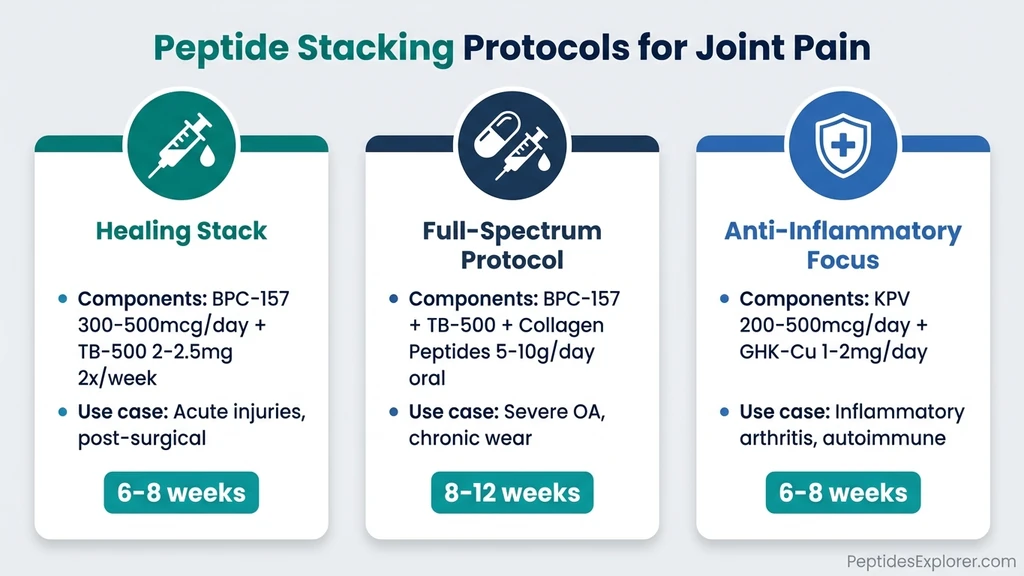
The Healing Stack (BPC-157 + TB-500)
The most widely used peptide combination for joint injuries. BPC-157 handles localized repair at the injured joint. TB-500 provides systemic healing and reduces scar tissue formation.
Protocol: - BPC-157: 300-500 mcg/day subcutaneous near the affected joint - TB-500: 2-2.5 mg twice per week subcutaneous (abdomen) - Duration: 6-8 weeks
Best for: Acute joint injuries, post-surgical recovery, chronic joint pain that has not responded to single peptides.
For detailed tendon-specific protocols using this stack, see our guide on the best peptides for tendon repair.
The Full-Spectrum Protocol (BPC-157 + TB-500 + Collagen Peptides)
Adding oral collagen peptides to the healing stack covers both acute repair and long-term structural support.
Protocol: - BPC-157: 300-500 mcg/day injection - TB-500: 2-2.5 mg twice per week injection - Collagen peptides: 5-10g/day oral - Duration: 8-12 weeks (continue collagen peptides long-term)
Best for: Moderate-to-severe osteoarthritis. Athletes with chronic joint wear across multiple sites. Post-surgical joint rehabilitation.
Injectable peptides handle acute inflammation and tissue repair. Collagen peptides provide the raw materials for sustained cartilage maintenance. The combination addresses both the acute and chronic dimensions of joint damage.
The Anti-Inflammatory Focus (KPV + GHK-Cu)
For joints where inflammation drives the pain rather than structural damage. Relevant to rheumatoid arthritis, autoimmune conditions, and aging-related inflammatory joint disease.
Protocol: - KPV: 200-500 mcg/day oral or subcutaneous - GHK-Cu: 1-2 mg/day subcutaneous or topical - Duration: 6-8 weeks
Best for: Inflammatory arthritis, autoimmune joint conditions, multi-joint inflammation in older adults. Avoids the side effects of chronic corticosteroid use.
Peptides vs. Traditional Joint Pain Treatments
Peptides are not the first line of defense for joint pain, and they are not a replacement for proven treatments. Here is how they compare.
| Treatment | Mechanism | Pros | Cons |
|---|---|---|---|
| NSAIDs | COX enzyme inhibition | Fast relief, cheap, accessible | GI bleeding risk, kidney damage with long-term use, no tissue repair |
| Corticosteroid injections | Broad immune suppression | Rapid inflammation reduction | Accelerates cartilage degradation with repeated use |
| Hyaluronic acid injections | Joint lubrication | FDA approved, well studied | Temporary relief, requires repeat injections |
| PRP therapy | Concentrated growth factors | Autologous, some RCT support | Expensive ($500-1,500/injection), variable quality |
| Glucosamine + Chondroitin | Cartilage building blocks | Widely available OTC, decades of data | Mixed evidence; Cochrane review found modest benefit at best |
| Peptide therapy | Targeted tissue repair + anti-inflammatory | Addresses root cause, multiple mechanisms | Limited human trials, regulatory gray area |
Key point: These treatments are not mutually exclusive. Many protocols use peptides alongside physical therapy, hyaluronic acid injections, or short-term NSAIDs. The AOD-9604 rabbit study specifically found that AOD-9604 combined with hyaluronic acid outperformed either treatment alone.
For a broader overview of peptide injections, including technique and site selection, see our complete beginner's guide.
How Long Do Peptides Take to Work for Joint Pain?
Expectations matter. Injectable peptides work faster than oral collagen, but neither produces overnight results.
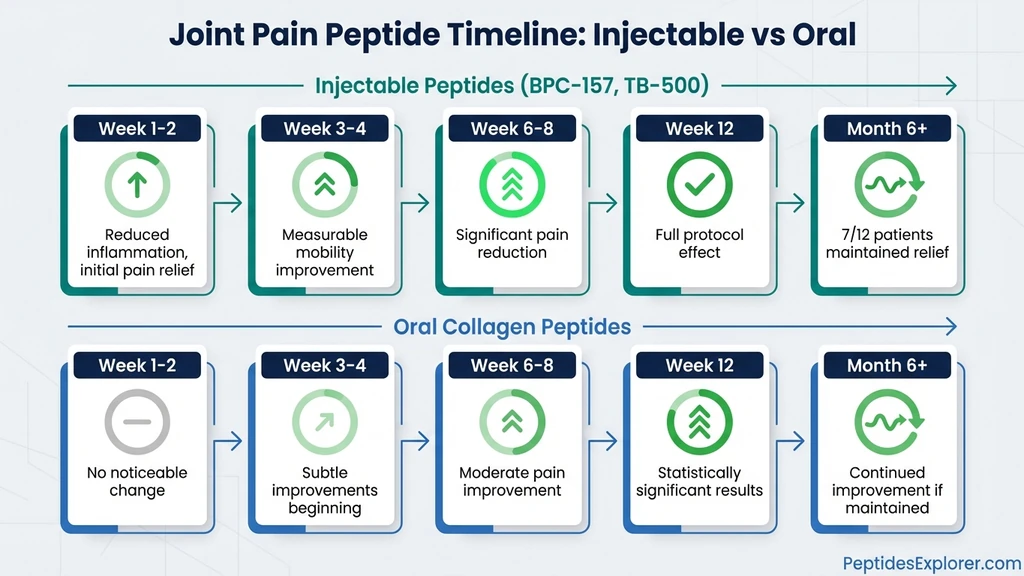
| Phase | Injectable Peptides (BPC-157, TB-500) | Oral Collagen Peptides |
|---|---|---|
| Week 1-2 | Reduced inflammation, initial pain relief | No noticeable change |
| Week 3-4 | Measurable improvement in mobility | Subtle improvements beginning |
| Week 6-8 | Significant pain reduction, tissue remodeling | Moderate pain improvement |
| Week 12+ | Full protocol effect, sustained relief | Statistically significant results per RCTs |
| Month 6+ | 7/12 maintained relief per systematic review | Continued improvement if maintained |
The BPC-157 timeline is derived from Lee et al. as analyzed by a 2025 systematic review, which reported 7 of 12 knee pain patients maintained relief beyond 6 months after intra-articular injection. The collagen timeline reflects findings from the Frontiers in Nutrition 2025 trial, where 180 days of supplementation produced statistically significant WOMAC improvements.
If you see no improvement after 6 weeks of injectable peptides or 12 weeks of collagen peptides at adequate doses, the issue may require medical evaluation rather than a longer protocol.
Are Peptides for Joint Pain Safe? Side Effects and Warnings
Peptides for joint pain carry real risks that most articles minimize. Here is what the data shows.
Common Side Effects
- Injection site redness and mild irritation (resolves in hours)
- Mild nausea with oral peptides on an empty stomach
- Temporary fatigue during the first week, particularly with TB-500
- Healing flare: old injuries may temporarily ache as repair processes activate
Serious Safety Considerations
FDA regulatory status. BPC-157 is an FDA Category 2 substance. It cannot be legally compounded by US pharmacies as of 2023. TB-500, KPV, GHK-Cu, and AOD-9604 are not FDA-approved for human use in any form. Collagen peptides are the only option on this list available as a legal dietary supplement.
Anti-doping. BPC-157 and TB-500 are prohibited by WADA and banned in NFL, NCAA, UFC, and Olympic competition.
Cancer contraindication. BPC-157, TB-500, and GHK-Cu promote angiogenesis and cell proliferation. Anyone with active cancer or a cancer history should avoid these peptides. The mechanisms that repair joint tissue can also feed tumor growth.
Product quality. Published analyses have found peptide products contaminated with arsenic and lead at 10x acceptable limits, bacterial endotoxins, wrong amino acid sequences, and purity as low as 5-75%. Source only from suppliers with third-party certificates of analysis.
No long-term safety data. The longest human study on BPC-157 for joints followed 12 patients for 6 months. Long-term effects of repeated peptide use are unknown.
Pregnancy and breastfeeding. All peptides in this article are contraindicated.
For detailed safety data on BPC-157 specifically, see our BPC-157 side effects guide.
Who Should Avoid Peptide Therapy for Joints?
- People with active cancer or cancer history
- Pregnant or breastfeeding women
- Competitive athletes subject to anti-doping testing
- Individuals on blood thinners (consult physician first)
- People with Wilson's disease (avoid GHK-Cu specifically)
- Anyone unable to verify peptide purity from their source
Frequently Asked Questions
What is the best peptide for knee joint pain?
BPC-157 has the most direct evidence for knee pain. In the only human study, 11 of 12 patients receiving intra-articular BPC-157 injections reported significant knee pain improvement, with 7 maintaining relief over 6 months (Lee et al., 2021). For long-term knee osteoarthritis, oral collagen peptides (3-5g daily) have stronger randomized controlled trial support across multiple studies totaling 507 patients.
Are peptides better than cortisone shots for joint pain?
They work differently. Cortisone provides faster pain relief by suppressing inflammation broadly, but repeated injections can accelerate cartilage degradation. Peptides like BPC-157 target tissue repair rather than symptom masking. However, cortisone injections have decades of human clinical data, while most peptide evidence comes from animal studies. They may complement each other rather than compete.
How long do peptides take to work for joint pain?
Injectable peptides like BPC-157 and TB-500 typically show initial pain relief within 1-2 weeks, with significant improvement by weeks 4-8. Oral collagen peptides require longer: clinical trials show statistically significant results at 12-24 weeks of daily use. A full injectable protocol runs 4-8 weeks.
Can you take peptides orally for joint pain?
Yes, depending on the peptide. Collagen peptides are designed for oral use and have the strongest clinical evidence for joint pain at 3-10g daily. BPC-157 can be taken orally but has less evidence for joints via this route; see our guide on taking BPC-157 orally. KPV is effective orally for systemic inflammation. TB-500, GHK-Cu, and AOD-9604 require injection.
Are peptides for joint pain legal?
Collagen peptides are legal dietary supplements worldwide. BPC-157 was classified as FDA Category 2 in 2023 and cannot be compounded by US pharmacies. It is not a controlled substance but exists in a regulatory gray area. BPC-157 and TB-500 are banned by WADA for competitive athletes. AOD-9604 has FDA GRAS status for oral fat-loss use only. Check your jurisdiction and any sport-specific regulations.
Do peptides actually repair cartilage?
Some peptides show cartilage repair potential in preclinical models. AOD-9604 enhanced cartilage regeneration in rabbit osteoarthritis models. GHK-Cu stimulates chondrocyte activity and glycosaminoglycan synthesis. Collagen peptides signal the body to produce more type II collagen. No peptide has been proven to fully regenerate damaged cartilage in human trials. The realistic expectation is slowed degeneration, reduced pain, and improved function. Full cartilage regrowth remains unproven.
Can I combine peptides with physical therapy for joint pain?
Yes, and this is the recommended approach. Peptides address biochemical repair. Physical therapy addresses biomechanical function, range of motion, and muscle support around the joint. Many clinicians recommend peptide therapy alongside structured PT for best outcomes. The combination targets both the tissue damage and the movement dysfunction that often accompanies joint pain.
How much do peptide injections cost for joint pain?
Costs vary by peptide and protocol. Oral collagen peptides run $15-40/month. BPC-157 costs $40-80 per 5mg vial (lasting 10-20 days at standard doses). TB-500 costs $50-100 per 5mg vial. A full BPC-157 + TB-500 stack runs approximately $100-200/month. These are peptide costs only and do not include clinic consultation fees, which range from $200-500 for initial evaluation.
Can growth hormone peptides like Ipamorelin help joint pain?
Indirectly, yes. Growth hormone peptides like Ipamorelin and CJC-1295 stimulate growth hormone release, which supports collagen synthesis and tissue repair throughout the body. However, their joint benefits are secondary effects, not targeted mechanisms. For direct joint pain treatment, BPC-157, collagen peptides, or TB-500 are more evidence-supported options.
The Bottom Line
The strongest evidence for peptides and joint pain belongs to oral collagen peptides: multiple RCTs, 507 patients across a meta-analysis, statistically significant pain reduction, and zero reported adverse events. That finding will surprise anyone who expected BPC-157 at the top of this list.
BPC-157 remains the best option for localized joint pain, particularly knee injuries, based on its single human trial showing 91.6% improvement and strong preclinical data across 35 studies. Stacking BPC-157 with TB-500 is the most common protocol for serious joint injuries.
Three things to remember: collagen peptides are the only option with robust human evidence, injectable peptides carry regulatory and safety considerations that oral collagen does not, and no peptide replaces proper medical evaluation for serious joint damage.
Explore individual peptide profiles for deeper research: BPC-157, TB-500, GHK-Cu, KPV, AOD-9604. Use our peptide stack calculator to plan combination protocols and our peptide interaction checker to verify compatibility. New to peptides? Start with our getting started with peptides guide. For all dosages in one place, see the peptide dosage chart. For reconstitution, see how to reconstitute peptides. For proper storage, see how to store peptides. For safety, see the peptide safety guide. For sourcing, see where to buy peptides in 2026. For stacking principles, see the peptide stacking guide.
Related Articles: - Best Peptides for Tendon Repair - BPC-157 Side Effects - TB-500 Dosage Chart - GHK-Cu Injection Dosage - KPV Peptide Dosage - Peptide Stacking Guide
Helpful Tools
Related Articles
Peptides for Inflammation: 7 Best Ranked
Top 7 anti-inflammatory peptides ranked: BPC-157, KPV, LL-37, thymosin alpha-1, GHK-Cu, TB-500, Selank. Mechanisms, dosage protocols, and 10+ PubMed citations.
Peptides for Healing: What the Evidence Shows
Peptides for healing by tissue: tendon, bone, wound, gut, post-surgery. Which claims rest on human trials, which rest on rat studies, and what is unsafe.
KLOW Peptide: Benefits, Dosage, and KLOW vs GLOW
KLOW peptide benefits, blend composition (GHK-Cu, BPC-157, TB-500, KPV), per-component dosing math, the copper ceiling, and how KLOW differs from GLOW.
Peptides for Recovery: 7 Best Ranked by Evidence
Top 7 peptides for recovery ranked: BPC-157, TB-500, GHK-Cu, ipamorelin, CJC-1295, MOTS-c, thymosin alpha-1. Post-workout and injury protocols.