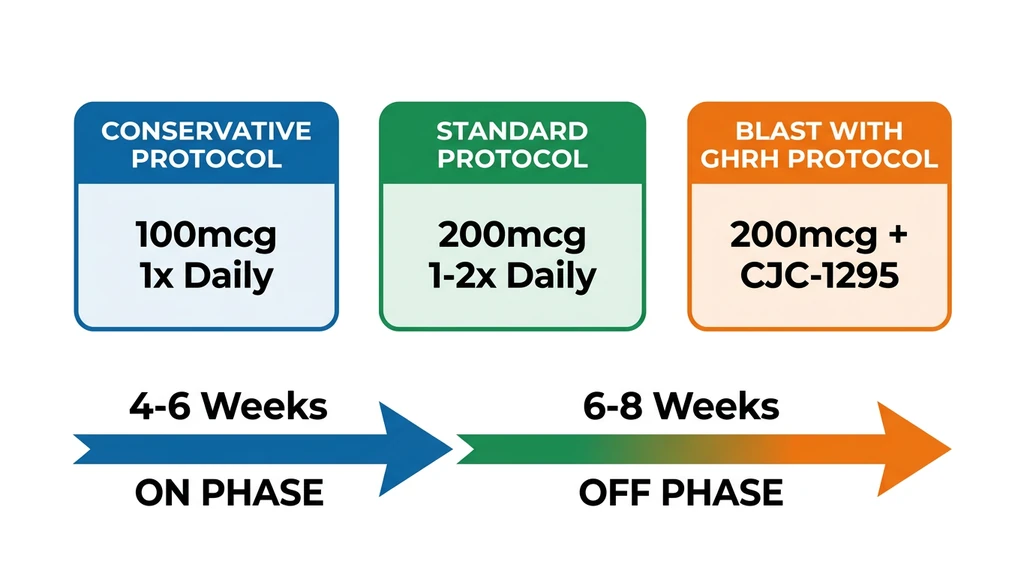
You have a vial of hexarelin on your desk, a syringe in your hand, and one question: how much do I inject? The short answer: 100 to 200 mcg subcutaneously, once or twice daily on an empty stomach, for 4 to 6 weeks on and 6 to 8 weeks off. Hexarelin (examorelin) is the most potent growth hormone releasing peptide ever tested in humans, capable of driving GH peaks above 50 ng/mL. That raw power comes with a hard expiration date. Your pituitary receptors will start going quiet within weeks if you do not cycle properly.
A Phase I dose-response study established the effective dose at 1.0 mcg/kg body weight, producing GH peaks of 52.3 ng/mL. Doubling the dose to 2.0 mcg/kg added almost no additional GH (55.0 ng/mL) but increased cortisol and prolactin (Ghigo et al. 1994, PubMed 7957536). This study defines the ceiling: going higher wastes product and amplifies side effects.
| Phase | Dose | Frequency | Duration |
|---|---|---|---|
| Conservative | 100 mcg | 1x daily | 4-6 weeks on, 6-8 off |
| Standard | 200 mcg | 1-2x daily | 4-6 weeks on, 6-8 off |
| Blast (with GHRH) | 100-200 mcg + 100 mcg CJC-1295 | 2x daily | 4 weeks max |
Hexarelin is not FDA-approved for any indication. This guide covers dosing protocols, clinical dose-response data, desensitization management, and safety. For the full peptide overview, see the hexarelin profile page.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
What Is Hexarelin and Why Does Dosage Matter So Much?
Hexarelin is a synthetic hexapeptide that locks onto the GHS-R1a receptor (the ghrelin receptor) on pituitary somatotroph cells. When it binds, those cells fire a burst of growth hormone into your bloodstream.
Among the five GHRPs studied in humans (hexarelin, GHRP-2, GHRP-6, ipamorelin, and MK-677), hexarelin produces the strongest GH release. A head-to-head comparison found hexarelin generated approximately 25% more GH than GHRP-2, the second-most potent option (Arvat et al. 1997, PubMed 9285939).
Here is the problem. The GHS-R1a receptor internalizes and downregulates under sustained, intense stimulation. Hexarelin's high binding affinity means it drives this process faster than any other GHRP. Dose too high and you accelerate desensitization without gaining more GH. Run your cycle too long and receptor downregulation cuts your response by 45% or more.
Getting your dose and cycle length right is not optional with hexarelin. It determines whether the peptide works or becomes a waste of money.
Dose-Response: What the Clinical Data Shows
The numbers below come from controlled human studies. They are the reason every protocol caps out at 200 mcg.
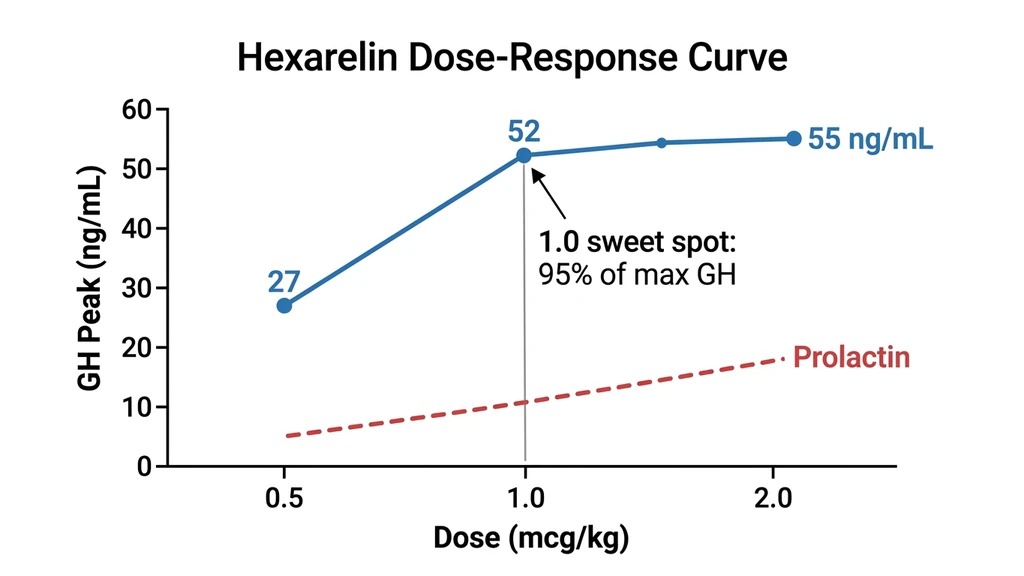
The Ghigo 1994 study administered hexarelin as IV boluses at 0.5, 1.0, and 2.0 mcg/kg to 12 healthy male volunteers and measured GH peaks (PubMed 7957536):
| Dose (mcg/kg) | GH Peak (ng/mL) | % of Maximum Response |
|---|---|---|
| Placebo | 3.9 | Baseline |
| 0.5 | 26.9 | ~49% |
| 1.0 | 52.3 | ~95% |
| 2.0 | 55.0 | ~100% |
The effective dose for half-maximal response (ED50) is 0.50 mcg/kg. At 1.0 mcg/kg, you reach 95% of the maximum GH output. Picture this: you double your dose from 100 to 200 mcg expecting double the GH. You get 5% more GH and significantly more cortisol and prolactin. The clinical data is clear: 1.0 mcg/kg captures 95% of the response. Going higher is waste.
The Arvat 1997 study expanded this picture to include cortisol and prolactin at the same dose range (PubMed 8954038):
- GH plateaus at 1.0 mcg/kg (ED50: 0.48 mcg/kg)
- Prolactin plateaus at 1.0 mcg/kg (ED50: 0.39 mcg/kg)
- Cortisol shows a step increase starting at 0.5 mcg/kg
The practical math: For an 80 kg person, 1.0 mcg/kg equals 80 mcg. Flat dosing of 100 mcg hits the optimal range for most adults. Going above 200 mcg does not produce more GH but does increase cortisol and prolactin proportionally. Higher doses are counterproductive.
Hexarelin Dosage Protocols by Goal
Four protocols tailored to different objectives. Each builds on the dose-response data above.
| Protocol | Dose | Frequency | Cycle | Best For |
|---|---|---|---|---|
| Conservative | 100 mcg | 1x daily | 4-6 wk on / 6-8 off | Beginners, anti-aging, GH optimization |
| Standard | 200 mcg | 1-2x daily | 4-6 wk on / 6-8 off | Body recomposition, recovery |
| Blast + GHRH | 100-200 mcg + 100 mcg CJC | 2x daily | 4 wk max | Experienced users, injury recovery |
| Cardio research | 100 mcg | 1x daily | Per research protocol | Cardiovascular research |
Conservative Protocol (GH Optimization)
Dose: 100 mcg per injection Frequency: Once daily, morning fasted or before bed Cycle: 4-6 weeks on, 6-8 weeks off
At 100 mcg, you get roughly 70 to 90% of the maximal GH response while keeping cortisol and prolactin at moderate levels. The lower dose also slows receptor desensitization, potentially extending your useful window by 1 to 2 weeks compared to higher doses.
This is the right starting point if you have never run hexarelin before, if you are over 40 and want general anti-aging GH support, or if you are sensitive to cortisol-related side effects like anxiety or insomnia.
Standard Protocol (Body Recomposition)
Dose: 200 mcg per injection Frequency: 1-2 times daily (morning fasted and/or before bed) Cycle: 4-6 weeks on, 6-8 weeks off
This is the near-maximal GH dose per injection. Twice-daily dosing at 200 mcg produces two large GH pulses that support fat metabolism, muscle protein synthesis, and recovery from training.
If you are actively cutting fat, building lean muscle, or training hard enough that recovery is a bottleneck, this is your protocol. This is also the ceiling: going above 200 mcg per injection adds side effects without more GH.
Blast Protocol (Short-Term Maximum GH with GHRH)
Dose: 100-200 mcg hexarelin + 100 mcg Mod GRF 1-29 (CJC-1295 no DAC) per injection Frequency: 2 times daily Cycle: 4 weeks maximum, then transition to ipamorelin + CJC-1295
Combining a GHRP (hexarelin) with a GHRH (CJC-1295) produces synergistic GH release significantly higher than either compound alone. The two mechanisms are complementary: GHRH stimulates GH synthesis and release from your pituitary, while hexarelin amplifies the release signal and suppresses somatostatin (the GH-inhibiting hormone).
Limit this stack to 4 weeks. Higher cumulative receptor exposure accelerates desensitization. After the blast, transition to ipamorelin (which does not desensitize) for sustained GH maintenance.
Build your stack: Peptide Stack Calculator | Interaction Checker
Cardioprotection Protocol (Research Context)
Dose: 100 mcg per injection Frequency: Once daily Cycle: Per research protocol
Hexarelin binds CD36 receptors on cardiomyocytes (heart muscle cells), activating anti-apoptotic and anti-fibrotic pathways through PPARgamma signaling. Preclinical studies demonstrate reduced infarct size, improved cardiac function after ischemia, and decreased atherosclerotic plaque formation (Bhatt et al. 2014, PubMed 25278975; PubMed 11988484).
The key finding: these cardiovascular effects are independent of GH release. They persist even after GH receptor desensitization occurs (PubMed 10465272). Your heart keeps benefiting even when your pituitary has stopped responding. Human clinical data remains limited.
Weight-Based vs. Flat Dosing: How to Calculate Your Dose
Clinical studies dose hexarelin in mcg/kg body weight. Community protocols use flat doses in mcg. Understanding the relationship between the two prevents you from underdosing if you are heavier or overdosing if you are lighter.
The effective range from clinical data is 1.0 to 2.0 mcg/kg. Below is a conversion table.
| Body Weight | 1.0 mcg/kg (Conservative) | 1.5 mcg/kg (Standard) | 2.0 mcg/kg (Maximum) |
|---|---|---|---|
| 60 kg / 132 lb | 60 mcg | 90 mcg | 120 mcg |
| 70 kg / 154 lb | 70 mcg | 105 mcg | 140 mcg |
| 80 kg / 176 lb | 80 mcg | 120 mcg | 160 mcg |
| 90 kg / 198 lb | 90 mcg | 135 mcg | 180 mcg |
| 100 kg / 220 lb | 100 mcg | 150 mcg | 200 mcg |
Flat dosing of 100 to 200 mcg covers the effective range for most adults weighing 60 to 100 kg. If you weigh 60 kg and take 200 mcg, you are at 3.3 mcg/kg, well above the clinical ceiling. If you weigh 100 kg and take 100 mcg, you are right at 1.0 mcg/kg, the sweet spot. Start at 100 mcg if you weigh under 70 kg. Go to 200 mcg if you are over 90 kg.
Use our reconstitution calculator for exact syringe measurements.
Reconstitution and Measuring Your Dose
Hexarelin comes as lyophilized (freeze-dried) powder, typically in 5 mg vials. You must reconstitute it with bacteriostatic water before injection.
Recommended reconstitution: - 5 mg vial + 2.5 mL bacteriostatic water = 2 mg/mL (2,000 mcg/mL) - 100 mcg dose = 0.05 mL = 5 units on a U-100 insulin syringe - 200 mcg dose = 0.10 mL = 10 units on a U-100 insulin syringe
Step-by-step: 1. Clean rubber stoppers on both vials with alcohol swabs 2. Draw 2.5 mL of bacteriostatic water 3. Inject slowly down the inside wall of the hexarelin vial (never squirt directly on the powder) 4. Gently roll between your palms until dissolved. Do not shake. 5. Label with date and concentration
Storage: Refrigerate at 2-8 degrees C after reconstitution. Use within 28 days. Unreconstituted powder stored at -20 degrees C remains stable for years.
For the full reconstitution walkthrough, see how to reconstitute peptides. For general storage guidance, see how to store peptides.
Desensitization Timeline: When Hexarelin Stops Working
Desensitization is the single biggest factor in your hexarelin protocol design. Think of it like an alarm clock. The first morning you set a new alarm, it jolts you awake instantly. After weeks of the same alarm at the same volume, you start sleeping right through it. Your pituitary receptor works the same way with hexarelin. Constant, intense stimulation causes the GHS-R1a receptor to internalize and retreat from the cell surface. Fewer receptors available means less GH released per injection, even though you are injecting the same dose.
A 16-week clinical study provides precise numbers on exactly how fast your GH response declines and how completely it recovers.
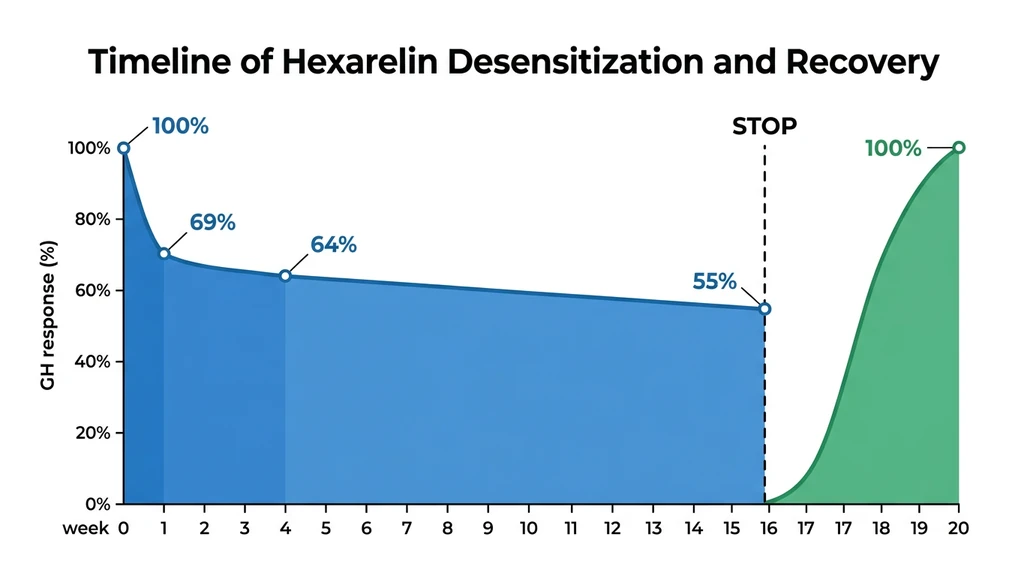
Study data (Lanfranco et al., PubMed 9589671 and PubMed 10990150):
| Timepoint | GH Response (AUCGH mcg/L/h) | % of Baseline |
|---|---|---|
| Week 0 (start) | 19.1 | 100% |
| Week 1 | 13.1 | 69% |
| Week 4 | 12.3 | 64% |
| Week 16 | 10.5 | 55% |
| 4 weeks after stopping | 19.4 | 102% (full recovery) |
Three takeaways from this data:
- 1.Desensitization hits fast but stays partial. You lose 31% of your GH response in the first week alone. By week 4, 36% is gone. But the floor is 55%, even after 16 continuous weeks.
- 1.Recovery is complete. Four weeks after stopping hexarelin, GH response returned to 102% of the original baseline. The damage is fully reversible.
- 1.The optimal window is 4 to 6 weeks. Beyond week 4, diminishing returns set in. You retain roughly 55 to 65% of your original response. The first 4 weeks capture approximately 80 to 90% of the total cumulative benefit.
Now picture the worst case. You run hexarelin for 16 straight weeks without cycling. Your GH response drops to 55% of what it was on day one. You are paying full price for half the effect. Cycling is not a suggestion; it is a requirement.
Why hexarelin desensitizes faster than other GHRPs: Higher binding affinity drives faster GHS-R1a receptor internalization and downregulation. Ipamorelin, with lower binding affinity, shows virtually no desensitization even after months of use. This is why many protocols use hexarelin for a 4 to 6 week blast, then transition to ipamorelin for long-term maintenance.
Signs your receptors are going quiet: Reduced post-injection flushing. Diminished appetite changes. Less pronounced water retention. If the side effects you felt in week one are fading, your GH response is declining with them.
Hexarelin vs. Every Other GHRP: Complete Comparison
Five GHRPs and one oral GH secretagogue have been studied in humans. This table compares them across every dimension that matters for practical use.
| Property | Hexarelin | GHRP-2 | GHRP-6 | Ipamorelin | MK-677 |
|---|---|---|---|---|---|
| GH Potency | Highest | High | Moderate | Moderate | Moderate |
| Peak GH (ng/mL) | 50-100+ | 40-80 | 30-50 | 20-40 | 15-30 |
| Cortisol Elevation | Significant | Mild | Mild | None | None |
| Prolactin Elevation | Significant | Mild | Minimal | None | None |
| Appetite Effect | Moderate | Mild | Strong | None | Strong |
| Desensitization | Fast (4-6 wk) | Moderate (8-12 wk) | Moderate (8-12 wk) | Very slow / none | None |
| Cardioprotection (CD36) | Yes | No | No | No | No |
| Administration | Injection | Injection | Injection | Injection | Oral |
| Best Use Case | Short blast cycles | Balanced GH | GH + appetite | Long-term, clean GH | Oral convenience |
Source: PubMed 10352397 (head-to-head comparison in humans)
Choosing the right GHRP for your goal: - You want maximum GH output for a short period. Hexarelin. - You want sustained GH elevation for months without cycling. Ipamorelin. - You want balanced potency with moderate side effects. GHRP-2. - You want GH plus appetite stimulation for bulking. GHRP-6. - You want oral convenience without injections. MK-677.
For overall dosage reference across all these peptides, see our peptide dosage chart.
Side Effects and How to Manage Them
Hexarelin's side effect profile reflects its non-selective potency. It drives GH hard, but it also pushes cortisol and prolactin up in a dose-dependent manner. Knowing the real numbers prevents both unnecessary panic and careless dosing.
Cortisol Elevation
Hexarelin produces a dose-dependent cortisol increase starting at 0.5 mcg/kg (PubMed 8954038). You may notice transient flushing, mild anxiety, or irritability in the 30 to 60 minutes following your injection.
Management: Keep your dosage at 100 to 200 mcg. Morning injection aligns with your natural cortisol peak (cortisol is highest upon waking), minimizing the perceived impact. Evening dosing can disrupt sleep if you are sensitive to cortisol.
The reassuring data: A 16-week chronic administration study found that cortisol and ACTH area-under-the-curve actually *decreased* compared to baseline over time. Hexarelin does not cause sustained HPA axis overstimulation (PubMed 10341859).
Prolactin Elevation
Prolactin rises in a dose-dependent manner with an ED50 of 0.39 mcg/kg. That means it reaches significant levels at a *lower* dose than the GH plateau (PubMed 8954038). Potential symptoms include nipple sensitivity and, in rare cases, gynecomastia in predisposed individuals.
Management: Stay at or below 200 mcg per injection. Monitor for symptoms. Discontinue if sensitivity develops. Prolactin elevation from hexarelin is less than from TRH (a diagnostic agent) but meaningfully more than from ipamorelin or GHRP-2.
One thing to watch for: some online sources claim hexarelin causes "no major increases in prolactin." This directly contradicts the clinical data. Be cautious with sources that downplay this effect.
Water Retention and Tingling
Mild water retention and numbness or tingling in your hands and feet are GH-mediated effects. They indicate the peptide is working. These symptoms typically resolve within the first 2 weeks as your body adjusts to elevated GH levels.
If they are severe, reduce your dose by 50 mcg and reassess after a week.
Desensitization
Not a side effect in the traditional sense, but the primary practical limitation you will face. The fix is straightforward: cycle 4 to 6 weeks on, 6 to 8 weeks off. See the desensitization timeline section for the complete data.
Timing, Administration, and Practical Tips
When to inject: On an empty stomach. Wait at least 1 hour before eating after your injection, or inject at least 3 hours after your last meal. Glucose and free fatty acids suppress GH release. Hexarelin is more resistant to this blunting effect than GHRH, but fasting still optimizes your response.
Best timing windows: - Morning fasted: Aligns with your natural cortisol peak. The GH pulse supports the transition from overnight fasting into your active day. This is the most popular timing for single-daily protocols. - Before bed: Supports the natural nocturnal GH surge. GH secretion is highest during slow-wave sleep. One study found hexarelin decreases slow-wave sleep duration while stimulating cortisol release during the night (PubMed 15177700). If your sleep quality suffers, switch to morning-only dosing. - Both (twice daily): Morning fasted plus before bed for standard and blast protocols. This produces two large GH pulses per day.
Injection method: Subcutaneous, same technique as other peptides. Abdomen (2 inches from your navel) and outer thigh are preferred sites. Rotate injection sites to prevent lipodystrophy. Use 29 to 31 gauge insulin syringes.
For the complete injection technique, see peptide injections guide.
Stacking Hexarelin with Other Peptides
Hexarelin stacks well with specific peptide categories. The core principle: pair it with compounds that use different mechanisms so you are not competing for the same receptor.
Hexarelin + CJC-1295 (no DAC) or Sermorelin
The gold standard GHRP + GHRH stack. Hexarelin stimulates GH release from your pituitary somatotrophs (GHRP pathway). CJC-1295 or sermorelin stimulates GH synthesis and release through the GHRH receptor (a completely separate pathway). Together they produce synergistic GH output substantially higher than either alone.
You can inject both compounds at the same time. They can be combined in the same syringe.
Protocol: 100 to 200 mcg hexarelin + 100 mcg CJC-1295 (no DAC), 1 to 2x daily. Limit the combined stack to 4 weeks before transitioning.
Hexarelin to Ipamorelin Transition
This is the most widely used long-term GH optimization strategy. You run hexarelin for a 4 to 6 week blast to achieve rapid GH elevation, then transition to ipamorelin for 12 to 16 weeks of sustained maintenance.
Ipamorelin produces cleaner GH release with no cortisol or prolactin elevation and virtually no desensitization. It is less potent per injection but can be used indefinitely.
Transition protocol: Complete your hexarelin cycle. Start ipamorelin (200 to 300 mcg, 1 to 2x daily) on the first day of your hexarelin off-cycle. Ipamorelin uses the same GHS-R1a receptor but with lower affinity, allowing the receptor to recover from hexarelin's intense stimulation while still producing moderate GH output.
Use our CJC-1295 + Ipamorelin calculator for the maintenance phase dosing.
Hexarelin + BPC-157 / TB-500 (Injury Recovery)
For injury recovery, hexarelin provides a systemic GH boost that supports tissue repair throughout your body. BPC-157 and TB-500 target local tissue repair: BPC-157 through angiogenesis and VEGF upregulation, TB-500 through actin regulation and scar tissue reduction.
This combination approaches healing from two directions: systemic GH elevation (hexarelin) plus localized repair (BPC-157/TB-500). They use completely different receptors and pathways, so there is no competition or interference.
See best peptides for tendon repair for detailed injury recovery protocols.
Frequently Asked Questions
What is the best hexarelin dosage for beginners?
100 mcg once daily, subcutaneously, on an empty stomach. Morning fasted is the simplest timing. At this dose you get roughly 70 to 90% of the maximal GH response while keeping cortisol and prolactin moderate. Run for 4 to 6 weeks, then take 6 to 8 weeks off before repeating. There is no reason to start higher; you capture nearly all the benefit at 100 mcg.
How long can I run hexarelin before it stops working?
Your GH response drops 31% after just 1 week and reaches a floor of 55% after 16 weeks of continuous use. The decline is partial, never total. After 4 weeks off, your response returns to 100% (PubMed 9589671). Most protocols recommend 4 to 6 week cycles because the first month captures the majority of your cumulative GH benefit. After that, you are fighting diminishing returns.
Does hexarelin raise cortisol and prolactin?
Yes, both in a dose-dependent manner. At 1.0 mcg/kg (roughly 80 mcg for an 80 kg person), cortisol shows a moderate increase and prolactin reaches near-plateau levels. The good news: chronic administration over 16 weeks does not cause sustained HPA axis overstimulation. ACTH and cortisol area-under-the-curve actually decreased compared to baseline in one long-term study (PubMed 10341859). Your body adapts.
Is hexarelin better than ipamorelin?
They solve different problems. Hexarelin produces 2 to 3 times the GH peak of ipamorelin but desensitizes within weeks and elevates cortisol and prolactin. Ipamorelin produces cleaner, more selective GH release with virtually no side effects and no desensitization, making it the better choice for long-term use. The proven strategy is to use hexarelin for a 4 to 6 week blast, then switch to ipamorelin for months of maintenance.
Can I take hexarelin orally or nasally?
Both routes have been studied. A trial in elderly subjects found that short-term intranasal and oral hexarelin did not desensitize the GH response (PubMed 8921821). Bioavailability through these routes is lower and less consistent than subcutaneous injection. If precise dosing matters to you, injection remains the standard.
How do I reconstitute a 5 mg hexarelin vial?
Add 2.5 mL of bacteriostatic water to a 5 mg vial. This gives you a concentration of 2 mg/mL (2,000 mcg/mL). For a 100 mcg dose, draw 5 units on a U-100 insulin syringe. For 200 mcg, draw 10 units. Refrigerate after reconstitution and use within 28 days. Use our reconstitution calculator for other vial sizes.
Does hexarelin protect the heart?
Preclinical evidence strongly supports cardioprotective effects. Hexarelin binds CD36 receptors on cardiac cells, activating anti-apoptotic and anti-fibrotic pathways. Studies show reduced infarct size, improved cardiac function after ischemia, and decreased atherosclerotic plaque formation. These effects operate independently of GH release and persist even when GH desensitization occurs (PubMed 25278975). Human clinical data remains limited.
What is the difference between hexarelin and GHRP-2?
Hexarelin produces approximately 25% more GH than GHRP-2 per injection but desensitizes faster (4 to 6 weeks vs. 8 to 12 weeks) and causes more cortisol and prolactin elevation. GHRP-2 offers a more balanced profile for longer cycles. Choose hexarelin when you want maximum short-term GH output. Choose GHRP-2 when you need sustained use with moderate potency and fewer hormonal side effects.
Should I use hexarelin 5 days on, 2 days off?
No clinical study tests this exact schedule, but the logic is sound: reducing your total weekly receptor exposure should slow GHS-R1a downregulation. It is a reasonable approach if you want to extend a cycle beyond 4 weeks. The hard 4 to 6 week on, 6 to 8 week off protocol has stronger published support, so default to that unless you have a specific reason to experiment.
Frequently Asked Questions
What is the best hexarelin dosage for beginners?
Start with 100 mcg once daily, subcutaneously, on an empty stomach in the morning. This captures 70 to 90% of the maximal GH response at 1.0 mcg/kg while keeping cortisol and prolactin moderate. Run for 4 to 6 weeks, then take 6 to 8 weeks off before repeating.
How long can I run hexarelin before it stops working?
Your GH response declines 31% after 1 week and bottoms out at 55% after 16 weeks. Full recovery to 100% takes just 4 weeks off. Most protocols cap cycles at 4 to 6 weeks to stay in the high-return window.
Does hexarelin raise cortisol and prolactin?
Yes, both rise dose-dependently. At 1.0 mcg/kg (about 80 mcg for an 80 kg person), cortisol increases moderately and prolactin nears its plateau. A 16-week chronic administration study showed no sustained HPA axis overstimulation; ACTH and cortisol area-under-the-curve actually decreased over time compared to baseline.
Is hexarelin better than ipamorelin?
Hexarelin produces 2 to 3 times more GH per injection but desensitizes within 4 to 6 weeks and raises cortisol and prolactin. Ipamorelin is cleaner for long-term use with no desensitization. Best approach: hexarelin blast for 4 to 6 weeks, then ipamorelin maintenance.
Can I take hexarelin orally or nasally?
Both routes have been studied with some efficacy in clinical trials. One elderly cohort showed no GH desensitization with intranasal and oral administration. Bioavailability through these routes is lower and less predictable than subcutaneous injection, which remains the standard when precise, repeatable dosing matters to your protocol.
How do I reconstitute a 5 mg hexarelin vial?
Add 2.5 mL of bacteriostatic water to the 5 mg vial for a 2 mg/mL (2,000 mcg/mL) concentration. For a 100 mcg dose, draw 5 units on a U-100 insulin syringe. For 200 mcg, draw 10 units. Refrigerate after mixing and use within 28 days.
Does hexarelin protect the heart?
Preclinical data shows cardioprotection via CD36 receptor binding on cardiomyocytes, completely independent of GH release. Effects include reduced infarct size, improved cardiac function after ischemia, and decreased atherosclerotic plaque formation in animal models. These benefits persist even after GH desensitization occurs. Human clinical data remains limited.
What is the difference between hexarelin and GHRP-2?
Hexarelin produces roughly 25% more GH per injection but desensitizes faster (4 to 6 weeks vs. 8 to 12 weeks) with more cortisol and prolactin elevation. GHRP-2 is the better choice for longer cycles where moderate, sustained GH output matters more than peak potency.
Should I cycle hexarelin 5 days on, 2 days off?
No clinical study validates this exact schedule, but reducing your total weekly receptor exposure logically slows GHS-R1a downregulation and may extend useful cycle length. The standard 4 to 6 weeks on, 6 to 8 weeks off protocol has stronger published support and remains the recommended default for most users.
The Bottom Line
Hexarelin is the most potent GHRP you can use, producing GH peaks of 50 to 100+ ng/mL in clinical studies. That potency is both its greatest advantage and its hardest constraint: powerful short-term GH elevation, limited by receptor desensitization that caps useful cycles at 4 to 6 weeks.
The dose-response data leaves no room for guessing. At 1.0 mcg/kg (roughly 100 mcg for most adults), you reach 95% of the maximal GH response. Doubling the dose adds almost nothing except more cortisol and prolactin. Your ceiling is 200 mcg per injection.
Desensitization is partial and fully reversible. Four weeks off restores your GH response to baseline. The proven strategy for sustained benefit: hexarelin blast for 4 to 6 weeks, then transition to ipamorelin for long-term maintenance. The cardioprotective effects via CD36 add a dimension no other GHRP offers.
Use our reconstitution calculator for mixing, the peptide dosage chart for cross-referencing, and the stack calculator for combination protocols. For proper handling, see how to store peptides and how long reconstituted peptides last. For sourcing, see where to buy peptides in 2026. New to peptides? Start with our getting started with peptides guide, or review the peptide safety guide.
Related Articles: - Follistatin 344 Dosage Guide - Peptides for Muscle Growth - Peptide Stacking Guide - How to Reconstitute Peptides - How to Store Peptides - Sermorelin for Fat Loss — GH-pathway fat loss alternative to hexarelin - Tesamorelin Dosage for Fat Loss — GHRH analog for targeted visceral fat reduction
Helpful Tools
Related Articles
CJC-1295 Dosage: Complete Protocol Guide
CJC-1295 dosage guide: DAC and no-DAC protocols. Dosing by goal (anti-aging, fat loss, muscle, sleep), ipamorelin stacking, and injection timing.
DSIP Peptide Dosage: Sleep Protocols
DSIP dosage guide: 100-300 mcg protocols, reconstitution steps, timing before bed, cycling schedule, cortisol modulation, and delta-wave research.
CJC-1295 & Ipamorelin Benefits Explained
CJC-1295 and ipamorelin benefits: fat loss, muscle recovery, sleep, anti-aging, bone density, cognition, and immune support. PubMed-cited guide.
CJC Peptide: Which CJC-1295 Are You Holding?
CJC peptide explained: CJC-1295 with DAC (6-8 day half-life) versus CJC-1295 no DAC, which is Mod GRF 1-29. How to identify the vial you actually hold.