You have two vials in your refrigerator, one labeled CJC-1295 and the other ipamorelin, and you want to know what combining them will actually do for your body. This stack amplifies your natural growth hormone pulse by 2 to 10-fold without raising cortisol or prolactin, delivering measurable benefits in fat loss, muscle recovery, sleep quality, and anti-aging within 4 to 12 weeks.
| Benefit | Mechanism | Timeline | Evidence Level |
|---|---|---|---|
| Fat loss and body recomposition | Increased lipolysis via GH-mediated hormone-sensitive lipase activation | 4-8 weeks | Strong (multiple human GH trials) |
| Muscle recovery and growth | Elevated IGF-1 stimulates satellite cell proliferation and protein synthesis | 6-12 weeks | Strong (GH/IGF-1 axis well-established) |
| Sleep quality improvement | GH pulse amplification during slow-wave sleep, deeper NREM cycles | 1-3 weeks | Moderate (clinical observation + GH physiology) |
| Anti-aging (skin, collagen, vitality) | Collagen synthesis upregulation via IGF-1, increased cellular turnover | 8-16 weeks | Moderate (GH replacement studies) |
| Bone density | Osteoblast stimulation via IGF-1 and direct GH receptor activation | 6-12 months | Strong (GH deficiency replacement data) |
| Cognitive function | IGF-1 crosses blood-brain barrier, supports neuronal repair and BDNF | 4-8 weeks | Preliminary (animal models + GH deficiency data) |
| Immune support | Thymic function preservation and lymphocyte proliferation via GH/IGF-1 | 4-8 weeks | Moderate (GH immunology studies) |
| Injury recovery acceleration | Increased collagen deposition, angiogenesis, and local IGF-1 at repair sites | 2-6 weeks | Moderate (GH/IGF-1 wound healing studies) |
Both peptides remain investigational and are not FDA-approved for these uses. All timelines reflect community-reported averages and should be interpreted conservatively. For dosing calculations, use the CJC-1295 and ipamorelin dosage calculator.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
Why CJC-1295 and Ipamorelin Is the Gold Standard GH Stack
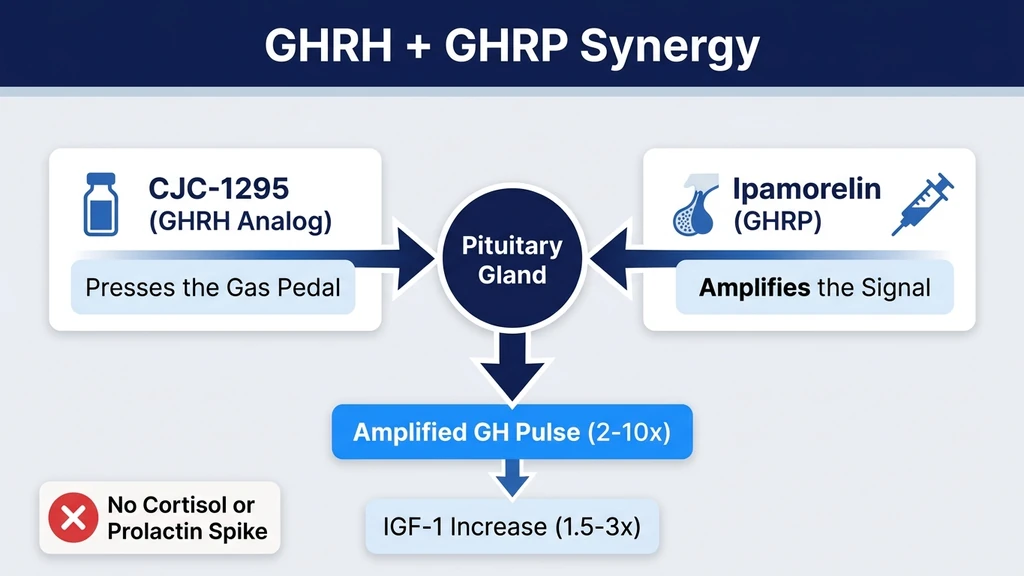
Your pituitary gland releases growth hormone in pulses, not a steady stream. Two signals control each pulse: a "go" signal from growth hormone-releasing hormone (GHRH), and an amplifier signal from growth hormone-releasing peptides (GHRPs). A third signal, somatostatin, acts as the brake. CJC-1295 and ipamorelin work on all three.
CJC-1295 is a synthetic GHRH analog. It tells the pituitary to release growth hormone. Think of it as pressing the gas pedal. Modified with a Drug Affinity Complex (DAC) or used in its no-DAC form, it extends the natural GHRH signal from minutes to hours. Teichman et al. demonstrated that a single CJC-1295 injection elevated mean GH levels 2 to 10-fold for 6 days, with IGF-1 levels increasing 1.5 to 3-fold for 9 to 11 days (Teichman et al., *Journal of Clinical Endocrinology & Metabolism*, 2006; PMID: 16670164).
The GHRH + GHRP Synergy Explained
Ipamorelin is a selective GHRP. It amplifies the signal CJC-1295 sends. Imagine CJC-1295 as a match and ipamorelin as lighter fluid. The match alone produces a small flame. Add the lighter fluid and the flame roars. Ipamorelin binds to the ghrelin receptor (GHS-R1a) on pituitary somatotrophs, priming them to respond more aggressively to the GHRH signal.
Raun et al. showed that ipamorelin produces dose-dependent GH release comparable to GHRP-6 but without the cortisol and prolactin spikes that plague other GHRPs (Raun et al., *European Journal of Endocrinology*, 1998; PMID: 9724432). This selectivity is what makes ipamorelin the preferred GHRP pairing. Hexarelin and GHRP-6 both raise cortisol and prolactin. Ipamorelin does not.
The third piece of the puzzle is somatostatin suppression. When GHRH and a GHRP fire simultaneously, they partially override the somatostatin brake that normally limits GH pulse amplitude. The result is a GH pulse that peaks higher and lasts longer than either peptide could produce alone. Bowers et al. confirmed this synergistic mechanism in controlled pituitary studies, showing combined GHRH + GHRP administration produced GH output exceeding the sum of individual responses (PMID: 1487032). For a comparison of CJC-1295 variants, see the DAC vs no-DAC guide.
Fat Loss and Body Recomposition
Growth hormone does not burn fat the way a stimulant does. It reprograms how your body fuels itself. Elevated GH activates hormone-sensitive lipase in adipocytes, the enzyme that breaks stored triglycerides into free fatty acids for oxidation. Your body shifts from burning glucose as its primary fuel to burning fat, particularly during fasting and sleep.
The practical result: users running CJC-1295 and ipamorelin report visible reduction in abdominal and visceral fat within 4 to 8 weeks, even without significant dietary changes. A meta-analysis of GH administration in obese adults demonstrated a mean reduction of 1.6 kg of fat mass over 12 weeks, with preferential loss from visceral depots (Mekala and Tritos, *Journal of Clinical Endocrinology & Metabolism*, 2009; PMID: 18854392).
The recomposition effect is the real prize. Because GH simultaneously promotes lipolysis and protein synthesis, you lose fat while preserving or gaining lean mass. This is the opposite of caloric restriction alone, which strips both fat and muscle. The peptide dosage chart has body-weight-adjusted protocols for optimizing this effect.
Muscle Recovery and Growth
CJC-1295 and ipamorelin do not build muscle the way anabolic steroids do. Steroids force protein synthesis through androgen receptor activation. This stack works upstream. Elevated GH stimulates liver production of IGF-1, which then activates satellite cells in muscle tissue. Satellite cells are the repair crews that fuse with damaged muscle fibers and donate new nuclei for growth.
Think of it like hiring more workers for a construction site. Testosterone tells each worker to lay bricks faster. IGF-1 brings additional workers to the site. The result is faster recovery between training sessions and gradual lean mass accrual over months, not weeks.
Liu et al. reviewed 44 studies involving 303 participants and found that GH supplementation increased lean body mass by an average of 2.1 kg over study periods ranging from 2 to 52 weeks (*Annals of Internal Medicine*, 2007; PMID: 17227934). The effect is most pronounced in individuals over 35, whose natural GH output has already declined 14% per decade. For stack protocols combining this with training periodization, see the peptide stacking guide.
Sleep Quality Improvement
This benefit appears first and hits hardest. Most users report deeper, more restorative sleep within the first 1 to 3 weeks. The mechanism is bidirectional: growth hormone release peaks during slow-wave (NREM stage 3) sleep, and exogenous GH pulse amplification deepens slow-wave sleep itself.
Your body performs the majority of tissue repair during deep sleep. Growth hormone is the chemical signal that initiates that repair. By amplifying GH pulses during the nighttime window, CJC-1295 and ipamorelin lengthen the time your body spends in the restorative phase of sleep. Users consistently describe waking less frequently, dreaming more vividly, and feeling more rested on the same number of hours.
Steiger et al. demonstrated that GHRH administration increased slow-wave sleep duration by 30 to 50% in healthy adults, with corresponding increases in nocturnal GH secretion (*Pharmacopsychiatry*, 2003; PMID: 14655966). Evening dosing of CJC-1295 and ipamorelin, 30 to 60 minutes before bed, capitalizes on this mechanism. For dosing timing details, see the CJC-1295 dosage guide.
Anti-Aging: Skin, Collagen, and Vitality
Growth hormone levels decline roughly 14% per decade after age 30. By 60, most people secrete less than half the GH they produced at 25. This decline correlates with thinner skin, slower wound healing, reduced collagen density, and the generalized loss of vitality that people attribute to "getting old."
CJC-1295 and ipamorelin partially reverse this decline by restoring GH pulse amplitude toward youthful levels. IGF-1 stimulates fibroblast proliferation and collagen synthesis in the dermis. The visible result is firmer, thicker skin with improved elasticity. Rudman et al. published the landmark study showing that six months of GH administration in men aged 61 to 81 increased skin thickness by 7.1% and lean body mass by 8.8% (*New England Journal of Medicine*, 1990; PMID: 2355952).
The "vitality" component is harder to measure but universally reported: improved energy, faster recovery from minor illness, better exercise tolerance, and a general sense of biological resilience. These subjective improvements align with restored GH/IGF-1 axis function in adults who were previously deficient.
Bone Density
Bone is not static. It is living tissue that remodels constantly, with osteoclasts breaking down old bone and osteoblasts building new bone. Growth hormone and IGF-1 tip this balance toward building. IGF-1 directly stimulates osteoblast proliferation and increases intestinal calcium absorption, supplying the raw material for new bone matrix.
This benefit takes the longest to manifest. Measurable changes in bone mineral density require 6 to 12 months of consistent GH elevation. Johansson et al. found that two years of GH replacement in adults with GH deficiency increased lumbar spine bone mineral density by 4 to 5%, with continued improvement through year five (*Journal of Bone and Mineral Research*, 1996; PMID: 8864909).
For individuals concerned about osteopenia or age-related bone loss, CJC-1295 and ipamorelin provide a mechanism that works alongside calcium and vitamin D supplementation rather than replacing it.
Cognitive Function
IGF-1 crosses the blood-brain barrier. Once in the central nervous system, it supports neuronal survival, promotes synaptic plasticity, and increases brain-derived neurotrophic factor (BDNF) expression. BDNF is the protein your brain uses to strengthen existing neural connections and build new ones.
Adults with growth hormone deficiency score lower on memory, attention, and processing speed tests compared to age-matched controls. GH replacement consistently improves these scores. Deijen et al. demonstrated that 18 months of GH therapy improved memory function and cognitive processing in GH-deficient adults (*Psychoneuroendocrinology*, 1998; PMID: 9621398). For a broader overview of peptides targeting brain health, see the cognitive function guide.
The cognitive benefit from CJC-1295 and ipamorelin is most noticeable in users over 40 who have experienced meaningful GH decline. Younger users with intact GH secretion may notice sharper focus and improved mental clarity, but the effect is subtler.
Immune Support
The thymus gland, responsible for T-cell maturation, shrinks with age. By 50, it is largely replaced by fatty tissue. Growth hormone slows this involution. GH receptors are expressed on lymphocytes, macrophages, and neutrophils, and GH/IGF-1 signaling enhances proliferation and cytotoxic activity across all three cell types.
Napolitano et al. showed that GH administration increased thymic mass and naive T-cell output in HIV-infected adults, suggesting direct thymic regeneration rather than peripheral expansion alone (*Journal of Clinical Investigation*, 2008; PMID: 18246204). While this study used supraphysiological GH doses, the principle applies at lower doses: restoring GH toward youthful levels supports immune surveillance.
Users of the CJC-1295 and ipamorelin stack frequently report fewer colds and faster resolution of minor infections. These reports are anecdotal but consistent with the established immunomodulatory role of the GH/IGF-1 axis.
Injury Recovery Acceleration
Growth hormone accelerates every phase of wound healing: inflammation resolution, collagen deposition, angiogenesis, and tissue remodeling. IGF-1 at the injury site stimulates fibroblast proliferation and increases type I and type III collagen synthesis, the structural proteins that rebuild tendons, ligaments, and skin.
Herndon et al. demonstrated that GH administration in severely burned patients reduced healing time by 25% and decreased hospital stay duration (*Annals of Surgery*, 2004; PMID: 15273542). In a less extreme context, users running CJC-1295 and ipamorelin report faster recovery from gym-related strains, surgical incisions, and chronic tendon injuries.
The stack pairs well with localized healing peptides like BPC-157 and TB-500 for serious injuries. CJC-1295 and ipamorelin elevate systemic GH/IGF-1 levels, creating a favorable hormonal environment, while BPC-157 drives angiogenesis directly at the injury site. See the peptide stacking guide for combination protocols.
What to Expect: Realistic Timeline
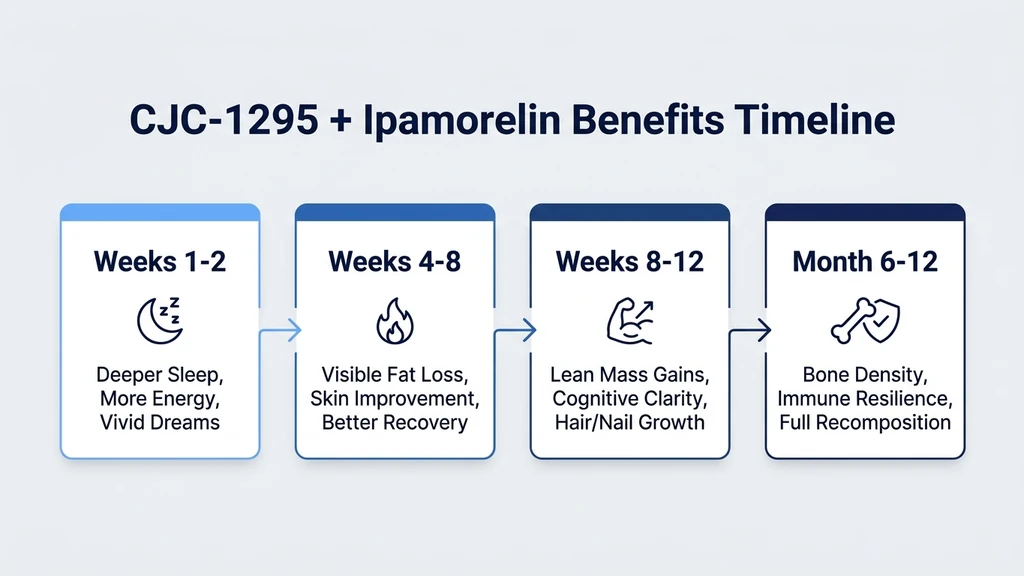
Benefits do not arrive all at once. They unfold in a predictable sequence because different tissues respond to GH/IGF-1 at different rates.
| Timeframe | Expected Changes |
|---|---|
| Week 1-2 | Deeper sleep, more vivid dreams, subtle increase in energy |
| Week 3-4 | Improved recovery between workouts, reduced joint stiffness |
| Week 5-8 | Visible fat reduction (particularly abdominal), skin appears fuller |
| Week 8-12 | Measurable lean mass gains, improved exercise capacity, hair/nail growth |
| Month 4-6 | Continued body recomposition, cognitive clarity, immune resilience |
| Month 6-12 | Bone density improvements (requires DEXA confirmation) |
These timelines assume consistent daily dosing at standard therapeutic levels (100 mcg CJC-1295 no-DAC + 100-200 mcg ipamorelin, 1-2x daily). Inconsistent dosing, poor sleep hygiene, or inadequate nutrition will delay all timelines. The CJC-1295 and ipamorelin dosage calculator can help you dial in the right protocol.
Common Mistakes That Reduce Benefits
1. Dosing too close to meals. Insulin and growth hormone oppose each other. Eating within 30 minutes before or after injection blunts the GH pulse by up to 40%. Dose on an empty stomach. The optimal windows are first thing in the morning (before breakfast) and 30-60 minutes before bed (at least 2 hours after your last meal).
2. Expecting steroid-level muscle gains. This stack is not testosterone. It will not add 15 pounds of muscle in 8 weeks. Realistic lean mass gains are 2 to 4 pounds over 3 to 6 months, combined with 3 to 6 pounds of fat loss. The recomposition effect is real, but it is gradual. Users who quit at week 4 because they do not "see results" are abandoning the protocol before the visible benefits begin.
3. Skipping weekends or cycling randomly. CJC-1295 (no-DAC) and ipamorelin work by amplifying your natural GH pulses. Consistent daily dosing maintains elevated baseline IGF-1 levels. Skipping days creates valleys where IGF-1 drops back to pre-treatment levels. Run the protocol daily for a minimum of 8 to 12 weeks before evaluating results.
4. Ignoring sleep and training. The stack amplifies your biology. If your sleep is 5 hours per night and you do not train, you are amplifying a weak signal. Eight hours of sleep gives GH more slow-wave time to work. Resistance training creates the microdamage that satellite cells repair and grow. Without these inputs, the peptides have less raw material to work with.
Safety Considerations and Side Effects
Ipamorelin's selectivity is its defining safety advantage. Raun et al. confirmed that ipamorelin does not raise cortisol or prolactin even at doses 100 times the effective GH-releasing dose (PMID: 9724432). This separates it from GHRP-6 and hexarelin, which both elevate cortisol (promoting fat storage and anxiety) and prolactin (reducing libido and disrupting hormonal balance).
Reported side effects at standard doses: - Water retention in the first 1 to 2 weeks (transient, resolves as the body adjusts) - Tingling or numbness in extremities (carpal-tunnel-like, dose-dependent, reversible) - Mild headache in the first few days - Increased hunger (GH stimulates appetite via ghrelin pathway cross-talk) - Injection site redness or irritation
Contraindications: Active cancer or a history of malignancy. GH and IGF-1 promote cell proliferation. They do not distinguish between healthy cells and tumor cells. Individuals with diabetes should monitor glucose closely, as GH impairs insulin sensitivity. Pregnant or breastfeeding women should avoid this stack entirely.
Neither CJC-1295 nor ipamorelin is FDA-approved for human use. Both are sold as research peptides. Consult a healthcare provider before beginning any peptide protocol. For a comparison between ipamorelin and other GHRPs, see the tesamorelin vs ipamorelin guide.
Frequently Asked Questions
How long does it take for CJC-1295 and ipamorelin to work?
Sleep improvements appear within 1 to 3 weeks. Fat loss becomes visible at 4 to 8 weeks. Lean mass gains require 8 to 12 weeks of consistent daily dosing. Bone density changes take 6 to 12 months to measure on a DEXA scan. The full recomposition effect requires at least 3 months at standard doses of 100 mcg CJC-1295 plus 100-200 mcg ipamorelin daily.
Does the CJC-1295 and ipamorelin stack raise cortisol or prolactin?
No. Ipamorelin is selective for GH release and does not stimulate cortisol or prolactin even at high doses (Raun et al., 1998). This separates it from GHRP-6 and hexarelin, which raise both hormones. The absence of cortisol elevation means the stack does not promote fat storage or anxiety as a side effect.
Should I use CJC-1295 with DAC or without DAC for this stack?
Most protocols use CJC-1295 without DAC (also called modified GRF 1-29) paired with ipamorelin. The no-DAC version has a 30-minute half-life, producing sharp GH pulses that mimic natural physiology. The DAC version extends the half-life to 6 to 8 days, creating sustained elevation rather than pulsatile release. See the DAC vs no-DAC comparison for details.
When is the best time to inject CJC-1295 and ipamorelin?
Inject on an empty stomach, at least 30 minutes before eating. The two most effective windows are morning (fasted, before breakfast) and evening (30 to 60 minutes before bed, at least 2 hours after dinner). Evening dosing capitalizes on the natural GH surge during slow-wave sleep. Many users dose twice daily for maximum effect.
Can I stack CJC-1295 and ipamorelin with other peptides?
Yes. Common additions include BPC-157 for localized injury healing, TB-500 for systemic recovery, and GHK-Cu for skin and collagen support. Avoid stacking with other GH secretagogues (MK-677, hexarelin) as they compete for the same receptors. The peptide stacking guide covers compatible combinations and timing protocols.
How much fat loss can I expect from CJC-1295 and ipamorelin?
Studies on GH administration show an average fat loss of 1.6 kg (3.5 lbs) over 12 weeks in obese adults (Mekala and Tritos, 2009). Community reports from the CJC-1295/ipamorelin stack range from 3 to 8 pounds of fat loss over 3 months, with preferential reduction in visceral and abdominal fat. Results depend on diet, training, and baseline body composition.
Is the CJC-1295 and ipamorelin stack safe long-term?
No long-term human safety data exists for this specific combination. Teichman et al. (2006) studied CJC-1295 for up to 12 weeks with no serious adverse events. Most practitioners recommend 3 to 6 month cycles followed by a 4 to 8 week break to prevent pituitary desensitization. Monitor IGF-1 levels via blood work every 8 to 12 weeks.
What is the standard dose for CJC-1295 and ipamorelin?
The standard protocol is 100 mcg CJC-1295 (no-DAC) combined with 100 to 200 mcg ipamorelin, injected subcutaneously 1 to 2 times daily. Both peptides are drawn into the same syringe for a single injection. Use the CJC-1295 and ipamorelin dosage calculator to determine reconstitution volumes and syringe markings for your specific vial concentrations.
The Bottom Line
CJC-1295 and ipamorelin is the most widely used GH peptide stack because it works on two complementary pathways: GHRH tells the pituitary to release growth hormone, and ipamorelin amplifies that signal without the cortisol and prolactin side effects that other GHRPs produce. The result is a cleaner, stronger GH pulse that delivers benefits across fat loss, muscle recovery, sleep, skin, bone, cognition, and immune function.
The benefits unfold gradually. Sleep improves within weeks. Body composition shifts over months. Bone density changes across a year. Patience and consistency matter more than dose escalation. Start at 100 mcg of each peptide daily, dose on an empty stomach, prioritize sleep and resistance training, and evaluate at 12 weeks.
Use the CJC-1295 and ipamorelin dosage calculator to plan your protocol. For dosing guidance, see the CJC-1295 dosage guide. For a full multi-peptide approach, consult the peptide stacking guide and the peptide dosage chart.
Helpful Tools
Related Articles
CJC-1295 Dosage: Complete Protocol Guide
CJC-1295 dosage guide: DAC and no-DAC protocols. Dosing by goal (anti-aging, fat loss, muscle, sleep), ipamorelin stacking, and injection timing.
CJC-1295 DAC vs No DAC: How to Choose
CJC-1295 DAC (6-8 day half-life, weekly injection) vs no DAC/Mod GRF 1-29 (30-min half-life, 2-3x daily). Compare dosing, GH patterns, and cost.
Tesamorelin vs Ipamorelin: Key Differences
Tesamorelin vs ipamorelin: GHRH analog vs ghrelin mimetic. Fat loss data, dosing, side effects, cost, and stacking protocols. PubMed-cited guide.
CJC Peptide: Which CJC-1295 Are You Holding?
CJC peptide explained: CJC-1295 with DAC (6-8 day half-life) versus CJC-1295 no DAC, which is Mod GRF 1-29. How to identify the vial you actually hold.