You ordered a vial labeled "CJC-1295 no DAC" and now you are staring at two dozen forum threads arguing about whether it is the same as Modified GRF 1-29, whether DAC matters, and how much to inject. The confusion is justified. Vendors mislabel these compounds constantly. Here is the straight answer: CJC-1295 without DAC is Modified GRF 1-29 (mod GRF 1-29), a synthetic GHRH analog with a half-life of approximately 30 minutes that produces sharp, pulsatile growth hormone release when injected subcutaneously at 100 mcg, 2-3 times daily on an empty stomach.
| Quick Reference | Details |
|---|---|
| Other names | Modified GRF 1-29, Mod GRF (1-29), tetrasubstituted GRF 1-29 |
| Peptide class | Growth hormone-releasing hormone (GHRH) analog |
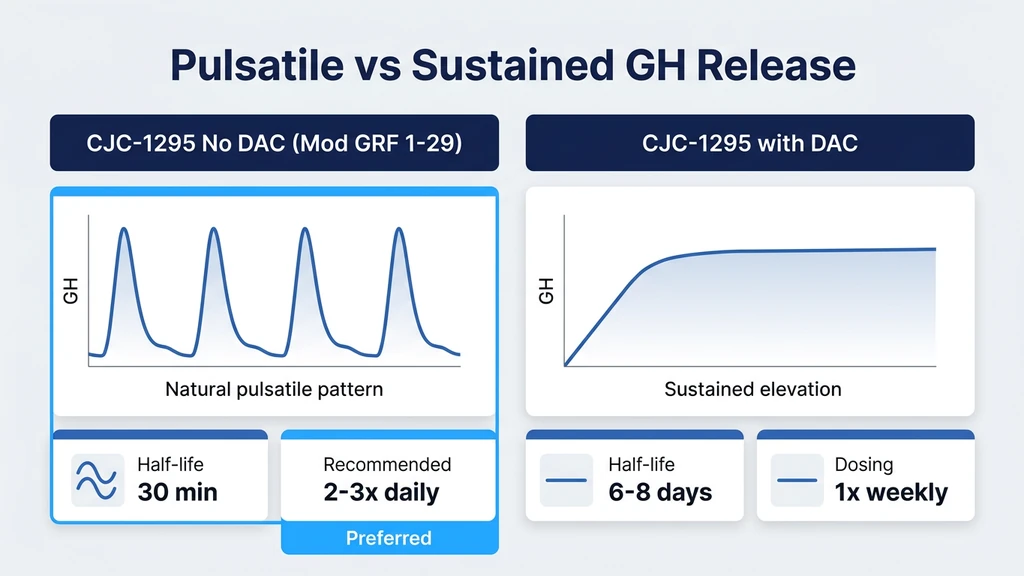
| Half-life | ~30 minutes (vs. 8 days for CJC-1295 with DAC) |
| Standard dose | 100 mcg per injection, 2-3x daily |
| Best timing | Fasted AM, post-workout, and/or before bed |
| Gold standard stack | + Ipamorelin 100-200 mcg (same syringe, same time) |
| Cycle length | 8-16 weeks on, 4 weeks off |
| Vial size | Typically 2 mg or 5 mg lyophilized powder |
| Evidence level | Human clinical trials on GRF 1-29; animal and in vitro data on modified analogs |
This compound is not FDA-approved for any indication. All protocols below reflect published research and established community practice. Consult a healthcare provider before starting any peptide regimen. For dosing calculations, use our CJC-1295 + Ipamorelin dosage calculator.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
What Is CJC-1295 Without DAC (Modified GRF 1-29)?
CJC-1295 without DAC is the first 29 amino acids of human growth hormone-releasing hormone (GHRH 1-44), with four amino acid substitutions at positions 2, 8, 15, and 27 that protect the molecule from rapid enzymatic breakdown. The original GHRH 1-29 fragment (sermorelin) has a plasma half-life of less than 10 minutes because dipeptidyl peptidase IV (DPP-IV) chews through it almost immediately after injection. The four substitutions in mod GRF 1-29 extend the half-life to approximately 30 minutes, long enough for a meaningful growth hormone pulse without the continuous elevation that DAC-conjugated versions produce (Ionescu & Bhatt, Endotext, 2022).
Think of it like a match versus a candle. Sermorelin is the match: it flares bright and dies in seconds. Mod GRF 1-29 is a short candle: it burns long enough to light the room, then goes out. CJC-1295 with DAC is an oil lamp: it stays lit for days. Your pituitary gland responds differently to each pattern, and that difference determines whether the resulting growth hormone release looks natural or artificial.
The four amino acid substitutions are: Ala at position 2 (replacing Asp), Gln at position 8 (replacing Asn), Ala at position 15 (replacing Gly), and Leu at position 27 (replacing Met). These changes block the two primary cleavage sites that degrade native GHRH without altering the peptide's binding affinity for the GHRH receptor on pituitary somatotroph cells (Tauber et al., Growth Horm IGF Res, 1999).
CJC-1295 With DAC vs. Without DAC: Why It Matters
The "DAC" stands for Drug Affinity Complex, a lysine-linked maleimidopropionic acid group that binds covalently to serum albumin after injection. This albumin binding extends the peptide's half-life from 30 minutes to approximately 6-8 days. That single chemical modification creates a fundamentally different pharmacological profile.
| Property | CJC-1295 No DAC (Mod GRF 1-29) | CJC-1295 With DAC |
|---|---|---|
| Half-life | ~30 minutes | 6-8 days |
| GH release pattern | Pulsatile (sharp peak, quick return to baseline) | Sustained, continuous elevation |
| Injection frequency | 2-3x daily | 1-2x per week |
| Mimics natural physiology | Yes (matches normal GHRH pulsatility) | No (GH stays elevated around the clock) |
| IGF-1 elevation | Moderate, cycling with GH pulses | Sustained, higher average levels |
| Somatostatin override | No (feedback loop preserved) | Partially (chronic stimulation blunts feedback) |
| Desensitization risk | Low | Moderate (continuous receptor stimulation) |
| Best for | Natural GH optimization, stacking with GHRPs | Convenience, sustained IGF-1 elevation |
The clinical study by Teichman et al. demonstrated that CJC-1295 with DAC produced dose-dependent increases in mean GH concentrations of 2-10 fold and IGF-1 increases of 1.5-3 fold after a single subcutaneous injection, with effects lasting 6-14 days (Teichman et al., J Clin Endocrinol Metab, 2006). That sustained elevation is convenient for users who dislike frequent injections. But it comes with a trade-off.
Your pituitary gland is designed to release growth hormone in sharp pulses, not steady streams. The largest natural GH pulse occurs during the first 90 minutes of deep sleep. Smaller pulses follow exercise and fasting. Between these pulses, GH drops to near-zero, which allows somatostatin (the GH-inhibiting hormone) to reset the system for the next burst. CJC-1295 with DAC disrupts this rhythm by keeping the GHRH signal active around the clock.
The no-DAC version preserves the pulsatile pattern. You inject, your pituitary fires a GH pulse, GH returns to baseline within 2 hours, and the system resets. This is why most practitioners and researchers who prioritize physiological GH signaling choose the no-DAC variant for daily protocols. For a broader comparison of GH secretagogues, see the peptide stacking guide.
Why Pulsatile GH Release Matters More Than Total GH Output
A common mistake is assuming that more growth hormone circulating for longer equals better results. The biology is more nuanced. The pattern of GH release determines which downstream effects dominate.
Pulsatile GH release activates the JAK2-STAT5 signaling pathway in liver and peripheral tissues. This pathway drives the production of IGF-1, the mediator responsible for most of GH's anabolic and lipolytic effects. Continuous GH exposure, by contrast, desensitizes the JAK2-STAT5 pathway and shifts signaling toward the STAT1 and STAT3 pathways, which are associated with inflammation and insulin resistance rather than tissue growth (Choi & Bhatt, Growth Horm IGF Res, 2007).
Picture a doorbell. Press it once and the person inside gets up to answer. Press it continuously and they stop responding. Pulsatile GH works like a doorbell: each pulse triggers a fresh downstream response. Sustained GH works like holding the button down: the initial signal is strong, but receptor internalization and downstream desensitization progressively blunt the response.
Ho et al. demonstrated this directly in humans. Pulsatile GH infusion produced significantly greater nitrogen retention (a marker of protein synthesis) and lipolysis compared to continuous GH infusion delivering the same total daily dose (Ho et al., J Clin Endocrinol Metab, 1991). The pulse pattern, not the total dose, drove the superior outcome. This finding is the pharmacological foundation for choosing CJC-1295 without DAC over the DAC-conjugated version when the goal is body composition improvement.
For users interested in the GH-fat loss connection, see sermorelin for fat loss and tesamorelin dosage for fat loss.
CJC-1295 No DAC Dosage Protocols
All dosages below assume subcutaneous injection on an empty stomach (90+ minutes after eating, 30+ minutes before eating). Food intake, particularly carbohydrates, raises insulin and suppresses the GH pulse by up to 80% (Nass et al., J Clin Endocrinol Metab, 2008).
| Protocol | Mod GRF 1-29 Dose | Frequency | Cycle | Best For |
|---|---|---|---|---|
| Beginner | 100 mcg solo | 1-2x daily | 8-12 weeks on, 4 off | First-time GH optimization |
| Standard | 100 mcg + 100 mcg ipamorelin | 2-3x daily | 12-16 weeks on, 4 off | Body recomposition, recovery |
| Aggressive | 100 mcg + 200 mcg ipamorelin | 3x daily | 12 weeks on, 4 off | Experienced users, injury recovery |
| Fat loss focus | 100 mcg + 100 mcg ipamorelin | 2x daily (AM fasted + bedtime) | 12-16 weeks on, 4 off | GH-driven lipolysis |
Beginner Protocol: 100 mcg Solo, 1-2x Daily
Start here if you have never used a GHRH peptide. Inject 100 mcg subcutaneously once or twice daily: morning fasted and/or 30 minutes before bed. This dose produces a clean GH pulse roughly equivalent to what a healthy 25-year-old generates during deep sleep.
Run this protocol for 8-12 weeks to establish your baseline response. Track sleep quality (most users notice deeper sleep within 7-14 days), recovery speed between training sessions, and skin quality. These are the earliest markers that GH pulsatility is improving.
If you respond well and want stronger effects, the next step is adding ipamorelin rather than increasing the mod GRF 1-29 dose. Doubling the GHRH dose does not double the GH pulse; it mostly increases side effects like facial flushing and lightheadedness.
Standard Protocol: 100 mcg + Ipamorelin, 2-3x Daily
This is the most widely used GH optimization protocol in the peptide community. Inject 100 mcg mod GRF 1-29 combined with 100-200 mcg ipamorelin at each administration, 2-3 times daily. The two compounds work through entirely different receptors (GHRH-R vs. GHS-R1a), and combining them produces a synergistic GH pulse 3-5 times larger than either peptide alone.
A Phase I study by Bowers et al. confirmed that co-administration of a GHRH analog with a GHRP produces supra-additive GH release in humans, meaning the combined effect exceeds the sum of each compound's individual contribution (Bowers et al., J Clin Endocrinol Metab, 1990).
Typical three-dose daily schedule:
| Time | Mod GRF 1-29 | Ipamorelin | Notes |
|---|---|---|---|
| 6:30 AM (fasted) | 100 mcg | 100-200 mcg | First GH pulse of the day |
| Post-workout | 100 mcg | 100-200 mcg | Amplifies exercise-induced GH release |
| 10:00 PM (before bed) | 100 mcg | 100-200 mcg | Synergizes with nocturnal GH surge |
Run for 12-16 weeks, then take 4 weeks off. Blood work at weeks 8 and 12 (IGF-1, fasting glucose, HbA1c) confirms the protocol is producing results without pushing IGF-1 beyond the age-adjusted normal range. Use the CJC-1295 + Ipamorelin dosage calculator to dial in your exact measurements.
Timing Protocols: When to Inject for Maximum Effect
Three injection windows produce the strongest GH pulses. Each one exploits a different physiological state.
Fasted morning (6:00-7:00 AM). After an overnight fast, insulin is at its daily low. Low insulin means no brake on GH release. This is the cleanest window for a strong pulse. Wait at least 30 minutes after injection before eating breakfast.
Post-workout (within 15 minutes of finishing). Intense exercise triggers endogenous GHRH release from the hypothalamus. Injecting mod GRF 1-29 during this window amplifies an already-active GH cascade. The post-exercise GH pulse can be 300-500% above resting levels even without peptides. Adding mod GRF 1-29 + ipamorelin during this window pushes it further. Ensure you have not eaten a pre-workout meal within the preceding 90 minutes.
Before bed (30 minutes pre-sleep). The largest natural GH pulse occurs during slow-wave sleep. Sermorelin studies showed that injecting a GHRH analog at bedtime amplifies the nocturnal GH surge synergistically, producing a fat-burning window that extends through the overnight fast when lipolysis is already favored (Kang et al., J Gerontol A Biol Sci, 2003).
If you can only inject once daily, choose bedtime. If twice, choose fasted AM and bedtime. Three times adds the post-workout window. Each additional injection adds a GH pulse, but the returns diminish after three daily doses because somatostatin builds up and progressively blunts subsequent pulses.
Stacking CJC-1295 No DAC with Ipamorelin: The Gold Standard
The mod GRF 1-29 + ipamorelin combination is the most popular GH secretagogue stack for a reason. It exploits a fundamental principle of endocrinology: GHRH and GHRPs activate two separate intracellular pathways that converge on the same outcome (GH release), and their combined effect is synergistic rather than additive.
Mod GRF 1-29 binds the GHRH receptor on pituitary somatotroph cells, activating adenylate cyclase and raising intracellular cyclic AMP. Ipamorelin binds the ghrelin receptor (GHS-R1a) on the same cells, activating phospholipase C and raising intracellular calcium. Both signals converge on the exocytosis of stored GH granules. Because the two pathways use different second messengers, stimulating both simultaneously produces a GH pulse far larger than stimulating either alone.
Bowers et al. demonstrated this synergy directly in human subjects. The GH response to combined GHRH + GHRP administration was 3-5 fold greater than the response to either compound alone, and the effect was supra-additive: 1 + 1 equaled 5, not 2 (Bowers et al., J Clin Endocrinol Metab, 1990).
Why ipamorelin specifically? Among the GHRPs (hexarelin, GHRP-2, GHRP-6, ipamorelin), ipamorelin is the only one that produces selective GH release without raising cortisol, prolactin, or aldosterone at standard doses (Raun et al., Eur J Endocrinol, 1998). It also shows minimal receptor desensitization, allowing indefinite use. This selectivity makes it the ideal pairing for a daily GHRH protocol that you plan to run for months.
The practical protocol: - Draw both peptides into the same syringe (they are chemically compatible in bacteriostatic water) - 100 mcg mod GRF 1-29 + 100-200 mcg ipamorelin per injection - 2-3 injections daily (fasted AM, post-workout, before bed) - Cycle: 12-16 weeks on, 4 weeks off
Check your planned combination with the Peptide Interaction Checker and use the Peptide Stack Calculator to build a complete protocol.
What Happens When You Get the Protocol Wrong
Two errors account for most failed mod GRF 1-29 protocols. Both are avoidable with basic knowledge.
Mistake 1: Injecting after a meal. You eat dinner at 7 PM, inject mod GRF 1-29 + ipamorelin at 7:45 PM, and wonder why your sleep quality does not improve. Here is the math. Insulin levels after a carbohydrate-containing meal suppress GH release by 50-80%. If a properly timed injection produces a GH peak of 30 ng/mL, that same injection 45 minutes after dinner produces 6-15 ng/mL. Over 12 weeks, that is the difference between visible body composition changes and nothing measurable. The fix is simple: wait 90 minutes after eating, or inject before bed after a 2-3 hour dinner gap.
Mistake 2: Confusing CJC-1295 with DAC for the no-DAC version. A user buys "CJC-1295" without reading the label, injects 100 mcg three times daily, and ends up with continuously elevated GH for days. The DAC version has a half-life of 6-8 days. Three daily injections of CJC-1295 with DAC stack on top of each other, producing sustained supraphysiological GH levels that cause water retention, joint pain, carpal tunnel symptoms, and insulin resistance. The no-DAC version clears in 2 hours. Verify the label says "Modified GRF 1-29" or "CJC-1295 no DAC" before loading your syringe.
Mistake 3: Running too high a dose of mod GRF 1-29. Some users inject 200-300 mcg per shot, reasoning that more GHRH means more GH. Above 100 mcg, the dose-response curve flattens while side effects (flushing, headache, dizziness) increase proportionally. The receptor has a saturation point. Hitting it harder does not open it wider. The correct strategy is adding a GHRP (ipamorelin) to hit a second receptor, not doubling the dose on the first one.
For a complete overview of common peptide errors, see the peptide safety guide.
How to Reconstitute CJC-1295 No DAC
Mod GRF 1-29 arrives as a white lyophilized powder, typically in 2 mg or 5 mg vials. You must dissolve it in bacteriostatic water before injection.
Recommended reconstitution for a 2 mg vial: - Add 2 mL bacteriostatic water for a concentration of 1 mg/mL (1,000 mcg/mL) - 100 mcg dose = 0.10 mL = 10 units on a U-100 insulin syringe
Recommended reconstitution for a 5 mg vial: - Add 2.5 mL bacteriostatic water for a concentration of 2 mg/mL (2,000 mcg/mL) - 100 mcg dose = 0.05 mL = 5 units on a U-100 insulin syringe
Step-by-step: 1. Clean both stoppers. Wipe the rubber tops of the peptide vial and bacteriostatic water vial with separate alcohol swabs. 2. Draw the water. Pull 2 mL (or 2.5 mL for the 5 mg vial) of bacteriostatic water into an insulin syringe or a larger syringe with a 25-27 gauge needle. 3. Inject slowly along the glass wall. Aim the stream at the inside wall of the peptide vial, not directly onto the powder. Direct pressure can denature the peptide. 4. Let it dissolve. Wait 2-3 minutes. Gently roll the vial between your palms if any powder remains. Never shake. 5. Label the vial. Write the date, concentration, and peptide name on a piece of tape. 6. Refrigerate immediately. Store at 2-8 degrees C (36-46 degrees F). Use within 28 days.
If you are also reconstituting ipamorelin, keep the vials separate. Draw from each vial into the same syringe at injection time. For exact calculations across any vial size, use our peptide reconstitution calculator. For storage guidelines, see how to store peptides and how long do reconstituted peptides last.
Half-Life Comparison: Understanding the GHRH Spectrum
Half-life determines everything about a GHRH analog's dosing schedule, GH release pattern, and clinical utility. This table maps the full spectrum from the shortest-lived to the longest.
| GHRH Analog | Half-Life | Doses Per Day | GH Pattern | Notes |
|---|---|---|---|---|
| Native GHRH (1-44) | <7 minutes | Impractical | Ultra-brief pulse | DPP-IV degrades it instantly |
| Sermorelin (GRF 1-29) | 10-20 minutes | 1-2x | Brief pulse | FDA-approved 1997 (Geref), withdrawn 2008 |
| Mod GRF 1-29 (CJC-1295 no DAC) | ~30 minutes | 2-3x | Pulsatile | 4 amino acid substitutions block DPP-IV |
| Tesamorelin (44 AA + hexenoic acid) | 26-38 minutes | 1x | Moderate pulse | FDA-approved for HIV lipodystrophy |
| CJC-1295 with DAC | 6-8 days | 1-2x/week | Sustained, continuous | Albumin-binding Drug Affinity Complex |
The 30-minute half-life of mod GRF 1-29 sits in a pharmacological sweet spot. It is long enough to produce a robust GH pulse (peak GH occurs 15-30 minutes post-injection and returns to baseline within 2 hours) but short enough that the peptide clears before the next natural GHRH pulse from your hypothalamus. This means the feedback loop stays intact. Somatostatin can reset between injections, keeping the pituitary sensitive to each subsequent dose.
Borges et al. confirmed that repeated subcutaneous injections of GHRH analogs with short half-lives maintain GH responsiveness over extended protocols without evidence of tachyphylaxis, provided injections are spaced to allow somatostatin rebound (Borges et al., Neuroendocrinology, 1999). This absence of desensitization is the primary clinical advantage over both longer-acting GHRH analogs and potent GHRPs like hexarelin.
For real-time half-life tracking across your entire peptide protocol, use the peptide half-life tracker.
Side Effects and Safety Profile
Mod GRF 1-29 has one of the mildest side effect profiles among GH-stimulating peptides. Because it works through the natural GHRH receptor and the resulting GH release is self-limited by somatostatin feedback, the risk of supraphysiological GH exposure is low when dosed correctly.
Common Side Effects
Facial flushing. The most frequently reported effect. A warm flush across the face and chest appears 1-5 minutes after injection and fades within 15-30 minutes. This is caused by transient vasodilation triggered by the GH pulse. It is harmless and tends to diminish after the first week of use.
Lightheadedness or dizziness. Occurs in approximately 5-10% of users, usually during the first 3-5 days. More common when injecting in a standing position. Sitting or lying down for 5 minutes after injection eliminates the risk. If persistent, reduce the dose by 50% for one week before returning to the standard dose.
Injection site reactions. Mild redness or itching at the subcutaneous injection site. Rotate between at least four sites (left abdomen, right abdomen, left thigh, right thigh) to minimize this. For injection technique, see how to inject peptides.
Rare Side Effects and Monitoring
Water retention. Mild fluid retention during the first 1-2 weeks is a GH-mediated effect (GH increases renal sodium reabsorption). This resolves spontaneously and does not indicate a dangerous condition. It can temporarily obscure fat loss on the scale.
Tingling or numbness in extremities. Carpal tunnel-like symptoms indicate elevated GH levels. If this occurs, reduce the dose or skip 2-3 days. It is more common when stacking with a GHRP at the higher end of the dose range.
Blood glucose changes. GH promotes gluconeogenesis and can mildly increase fasting glucose. Users with pre-diabetes or type 2 diabetes should monitor fasting glucose and HbA1c every 8-12 weeks. If fasting glucose rises above 110 mg/dL, reduce the dose or discontinue.
Mod GRF 1-29 does not raise cortisol or prolactin at standard doses, which distinguishes it from GHRPs like hexarelin and GHRP-2 (Iovino et al., J Endocrinol Invest, 1999). This clean hormonal profile is a major reason it became the preferred GHRH backbone for long-term stacking protocols.
For overall peptide safety guidance, see the peptide safety guide. For information on safe peptide sourcing and the current FDA regulatory environment, check those guides before purchasing.
Who Should Use CJC-1295 No DAC (and Who Should Not)
Mod GRF 1-29 is a versatile compound, but it is not the right tool for every goal.
Good Candidates
Adults over 30 seeking GH optimization. Growth hormone secretion declines approximately 14% per decade after age 25. Mod GRF 1-29 restores the pulsatile GHRH signal that weakens with age, and the pituitary responds well into the sixties and seventies provided no structural damage exists (Veldhuis et al., J Clin Endocrinol Metab, 1995).
Users who want body recomposition without GLP-1 side effects. GH-driven fat loss is slower than GLP-1 agonists like tirzepatide or retatrutide, but it preserves lean mass and avoids the nausea, constipation, and appetite suppression those drugs produce. See retatrutide vs tirzepatide for a comparison.
Athletes prioritizing recovery and sleep quality. The improved sleep architecture from restored nocturnal GH pulsatility is often the first benefit users notice, typically within 7-14 days. Better sleep drives better recovery, which supports higher training volume.
Users who prefer pulsatile over continuous GH elevation. If the pharmacological argument for natural GH patterns resonates with you, mod GRF 1-29 is the correct choice over CJC-1295 with DAC.
Poor Candidates
Individuals with pituitary damage. Mod GRF 1-29 requires functioning somatotroph cells. Post-surgical, post-radiation, or tumor-damaged pituitaries may not respond. These individuals need direct GH replacement, not a secretagogue.
People with active cancer. GH and IGF-1 are growth factors. Elevating them in someone with active malignancy could promote tumor proliferation. This is a hard contraindication for all GH-stimulating compounds.
Users who want once-weekly convenience. Mod GRF 1-29 requires 2-3 daily injections. If that frequency is impractical, CJC-1295 with DAC (1-2 injections per week) or MK-677 (oral, once daily) may be better options despite their pharmacological trade-offs.
Those with BMI over 35. Obesity blunts the pituitary's GH response to GHRH stimulation. Addressing caloric balance and insulin resistance first, through diet and exercise or GLP-1 therapy, will improve responsiveness to GHRH analogs later.
Common Mistakes to Avoid
Mistake 1: Buying the wrong compound. Vendors frequently mislabel CJC-1295. Some sell the DAC version labeled as "CJC-1295" without specifying which variant it is. Others sell sermorelin (GRF 1-29 without the four protective substitutions) and call it mod GRF 1-29. Always verify the peptide name includes "Modified GRF 1-29" or "tetrasubstituted GRF 1-29" on the certificate of analysis. The difference in half-life (10 minutes for sermorelin vs. 30 minutes for mod GRF vs. 8 days for DAC) means the wrong compound at the wrong dose produces a fundamentally different result.
Mistake 2: Injecting on a full stomach. This is the single most common protocol failure. Insulin is the GH brake. Eating 45 minutes before injection can suppress the GH pulse by 50-80%, turning a $200/month protocol into a $200/month placebo. The 90-minute pre-injection fast is not a suggestion. It is a pharmacological requirement (Nass et al., J Clin Endocrinol Metab, 2008).
Mistake 3: Storing improperly. Reconstituted mod GRF 1-29 left at room temperature degrades rapidly. Within 48 hours outside the refrigerator, potency drops by 20-40%. After a week, the vial is essentially bacteriostatic water. Refrigerate immediately after reconstitution and use within 28 days. For full storage protocols, see how to store peptides.
Mistake 4: Expecting GLP-1-level weight loss. Mod GRF 1-29 enhances GH-driven lipolysis. It does not suppress appetite or create a caloric deficit. Users who expect tirzepatide-like results (15-22% body weight loss) will be disappointed. Realistic expectations: improved body recomposition (simultaneous fat loss and lean mass preservation), better sleep, and faster recovery over 12-16 weeks. For GLP-1 comparison, see semaglutide before and after.
Frequently Asked Questions
Is CJC-1295 no DAC the same as Modified GRF 1-29?
Yes. CJC-1295 without DAC and Modified GRF 1-29 (mod GRF 1-29) are the same peptide: the first 29 amino acids of human GHRH with four amino acid substitutions at positions 2, 8, 15, and 27. These substitutions extend the half-life from under 10 minutes (native GHRH) to approximately 30 minutes by blocking DPP-IV enzymatic cleavage. See CJC-1295 DAC vs no DAC for the full comparison.
What is the standard CJC-1295 no DAC dosage?
The standard dose is 100 mcg per injection, administered subcutaneously 2-3 times daily on an empty stomach. Most users stack it with 100-200 mcg ipamorelin at each injection for synergistic GH release. Doses above 100 mcg show diminishing returns for GH output while increasing side effects like flushing and dizziness. See the full CJC-1295 dosage guide for protocol variants.
Can you mix CJC-1295 no DAC and ipamorelin in the same syringe?
Yes. Both peptides are chemically stable in bacteriostatic water and can be drawn into the same syringe for a single injection. Draw mod GRF 1-29 first, then draw ipamorelin into the same syringe. This reduces injection frequency from six daily shots to three when running a three-dose protocol. The CJC-1295 + Ipamorelin dosage calculator handles the combined math.
How long does CJC-1295 no DAC take to work?
Sleep quality improvements typically appear within 7-14 days. Improved recovery between training sessions follows by weeks 2-4. Visible body composition changes (reduced body fat, improved muscle tone) usually require 8-12 weeks of consistent use combined with a structured diet and exercise program. IGF-1 levels measurably increase within 4-6 weeks. For benefits breakdown, see CJC-1295 and ipamorelin benefits.
Why is CJC-1295 without DAC preferred over the DAC version?
The no-DAC version produces sharp, pulsatile GH release that mimics natural physiology. Its 30-minute half-life allows the somatostatin feedback loop to reset between injections, maintaining pituitary sensitivity. The DAC version elevates GH continuously for 6-8 days, which can desensitize GH receptors and shift downstream signaling from anabolic pathways toward inflammatory ones. The CJC-1295 with DAC guide covers the long-acting variant in depth.
Does CJC-1295 no DAC cause desensitization?
No significant desensitization occurs at standard doses when injections are spaced to allow somatostatin rebound (minimum 3-4 hours between injections). This is a key advantage over potent GHRPs like hexarelin, which desensitize pituitary receptors within 4-6 weeks. Mod GRF 1-29 can be run for 12-16 week blocks with sustained GH responsiveness throughout. See hexarelin dosage for the contrast.
What is the best time to inject CJC-1295 no DAC?
Thirty minutes before bedtime on an empty stomach is the single most effective window. It amplifies the natural nocturnal GH surge during slow-wave sleep. If adding a second dose, inject fasted in the morning upon waking. A third dose post-workout captures the exercise-induced GH cascade. All injections require a 90-minute post-meal fast for full efficacy. The peptide half-life tracker maps your daily window.
How do you reconstitute a 2 mg vial of CJC-1295 no DAC?
Add 2 mL of bacteriostatic water to the 2 mg vial for a concentration of 1 mg/mL (1,000 mcg/mL). For a 100 mcg dose, draw 10 units on a U-100 insulin syringe. Inject the water slowly along the vial wall, not directly onto the powder. Gently roll to dissolve. Refrigerate at 2-8 degrees C and use within 28 days. Use the peptide reconstitution calculator for any vial size.
The Bottom Line
CJC-1295 without DAC (Modified GRF 1-29) produces the pulsatile growth hormone release pattern that your body was designed to generate. Its 30-minute half-life creates a sharp GH pulse that clears before somatostatin feedback kicks in, preserving the rhythm that drives IGF-1 production, lipolysis, and tissue repair more effectively than sustained GH elevation.
The protocol is 100 mcg injected subcutaneously 2-3 times daily on an empty stomach, ideally stacked with 100-200 mcg ipamorelin for synergistic GH release through separate receptor pathways. That combination remains the gold standard for GH optimization in the peptide community, validated by clinical data showing supra-additive GH pulses when GHRH and GHRP pathways are stimulated simultaneously.
Start with the CJC-1295 + Ipamorelin dosage calculator to build your protocol. Use the peptide reconstitution calculator for mixing, the peptide half-life tracker for timing, and the peptide interaction checker to verify stack safety. For proper handling, see how to store peptides and how long reconstituted peptides last. New to peptides? Start with our getting started with peptides guide.
Related articles: - Peptide Stacking Guide: compatibility charts and stack protocols - Hexarelin Dosage: most potent GHRP, short-cycle blast protocols - Sermorelin for Fat Loss: GH-driven lipolysis with the original GHRH analog - Tesamorelin Dosage for Fat Loss: FDA-approved GHRH analog for visceral fat - Peptide Dosage Chart: cross-reference dosing for all major peptides - Follistatin 344 Dosage: myostatin inhibition for lean mass - Peptide Safety Guide: safety protocols for all peptide users - Where to Buy Peptides 2026: verified supplier list - CJC-1295 with DAC Guide: long-acting variant comparison - Tesamorelin vs CJC-1295: FDA-approved GHRH alternative
Helpful Tools
Related Articles
CJC Peptide: Which CJC-1295 Are You Holding?
CJC peptide explained: CJC-1295 with DAC (6-8 day half-life) versus CJC-1295 no DAC, which is Mod GRF 1-29. How to identify the vial you actually hold.
CJC-1295 With DAC: Long-Acting GHRH Analog
CJC-1295 with DAC: 6-8 day half-life, 2-10x GH increase, 1-2 mg weekly. GH bleed effect, desensitization risk, and stacking protocols.
Tesamorelin Peptide: Uses, Evidence, Risks
Tesamorelin peptide explained: a GHRH analogue FDA-approved as Egrifta for HIV lipodystrophy. What it does to visceral fat, IGF-1, and who should avoid it.
CJC-1295/Ipamorelin Side Effects: Manage Them
CJC-1295/ipamorelin side effects: injection reactions 20-30%, water retention 15-25%, flushing 15-20%. DAC comparison and management.