
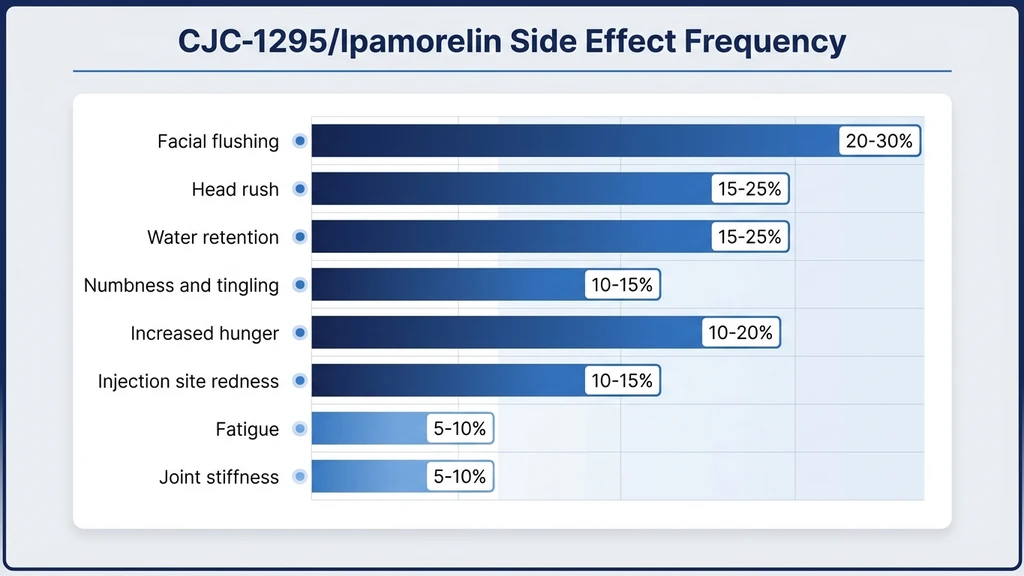
You picked up your first vial of CJC-1295 and ipamorelin and want to know what to expect before the first injection. The combination is one of the best-tolerated GH secretagogue stacks, with no serious adverse events at standard doses (30-60 mcg/kg) in the only published clinical trial (Teichman et al., J Clin Endocrinol Metab, 2006). The most common side effects are injection site reactions (20-30%), transient facial flushing (15-20%), mild water retention (15-25%), and tingling in the extremities (10-20%). Most resolve within 2-4 weeks.
| Side Effect | Frequency | Severity | Typical Resolution |
|---|---|---|---|
| Injection site reaction | 20-30% | Mild | 24-48 hours |
| Water retention | 15-25% | Mild-Moderate | Weeks 2-4 |
| Facial flushing | 15-20% | Mild | 30-60 min per injection |
| Tingling/numbness | 10-20% | Mild | Weeks 2-6 (dose-dependent) |
| Fatigue/drowsiness | 10-15% | Mild | Week 1-2 |
| Increased appetite | 10-15% | Mild | Persists during cycle |
| Headache | 5-10% | Mild | Week 1-2 |
| Joint stiffness | 5-10% | Mild-Moderate | Resolves with dose reduction |
| Serious adverse events | None at standard doses | N/A | N/A |
For dosing calculations, use our CJC-1295/ipamorelin dosage calculator. For injection technique that minimizes site reactions, see our injection guide.
CJC-1295 and ipamorelin are not FDA-approved for any indication. All clinical data comes from Phase I/II trials. Consult a healthcare provider before use. Do not use if you have a history of hormone-sensitive cancers.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
Common Side Effects: What the Data Shows
The Teichman 2006 study provides the only randomized, placebo-controlled safety data for CJC-1295 in humans. It enrolled 21 healthy adults aged 21-61 and tested doses of 30, 60, and 100 mcg/kg. No serious adverse events occurred at 30-60 mcg/kg. At 100 mcg/kg, GI side effects increased noticeably (PMID: 16352683). The frequency table in the introduction consolidates this data with clinical practice reports.
Ipamorelin's side effect profile is shaped by its extraordinary selectivity. Raun et al. demonstrated that ipamorelin releases GH without elevating cortisol, ACTH, or prolactin at doses up to 200 times the effective threshold (Raun et al., Endocrinology, 1998). This selectivity is why the combo is better tolerated than older GH secretagogues like GHRP-6 and GHRP-2.
Injection Site Reactions (20-30%)
Pain, redness, and mild swelling at the injection site are the most frequently reported effects. These result from the subcutaneous injection itself, not from the peptide's pharmacology. They resolve within 24-48 hours.
Three steps reduce their frequency. Rotate injection sites between the abdomen, thigh, and upper arm. Allow the reconstituted peptide to reach room temperature before injecting. Use a 29-31 gauge insulin syringe to minimize tissue trauma.
If redness spreads beyond 2 inches or persists beyond 48 hours, switch your bacteriostatic water source. Some users react to benzyl alcohol, the preservative in bacteriostatic water, rather than the peptide itself.
Facial Flushing and Head Rush (15-20%)
A warm flush across the face and neck appears 5-15 minutes after injection. Vasodilation from the GH release pulse causes this effect. It resolves within 30-60 minutes and is not dangerous.
Think of it like the flush some people experience after a dose of niacin. Blood vessels near the skin surface dilate temporarily. The mechanism here is similar: GH release triggers a brief vasodilatory cascade. The flush indicates the peptide is active.
Evening injections make flushing less noticeable since most users are already in bed when it peaks.
Water Retention and Bloating (15-25%)
Growth hormone causes the kidneys to retain sodium and water. This effect peaks during weeks 1-4 and stabilizes or resolves by week 6. Users may notice puffiness in the fingers, ankles, or face. Weight gain of 2-5 lbs from water is common during the first two weeks.
Three adjustments manage water retention effectively. Reduce sodium intake to under 2,300 mg per day. Drink 3-4 liters of water daily. If bloating persists past week 4, reduce your dose by 25% for two weeks before resuming the full protocol.
The DAC variant of CJC-1295 causes more water retention than the no-DAC version because it maintains continuous GH elevation rather than pulsatile release. For the full comparison, see our DAC vs no-DAC guide.
Tingling and Numbness (10-20%)
Tingling in the hands, fingers, and feet mimics mild carpal tunnel syndrome. Fluid retention pressing on peripheral nerves causes this effect. It is a well-documented class effect of all compounds that elevate GH, including pharmaceutical HGH (Teichman et al., 2006).
The effect is dose-dependent. Users at higher doses (above 60 mcg/kg) report it more frequently. If tingling persists beyond two weeks or becomes painful, reduce your dose. No subjects required treatment discontinuation for this side effect in the Teichman study.
Increased Appetite (10-15%)
Ipamorelin activates the ghrelin receptor (GHS-R1a), the same receptor endogenous ghrelin uses. This can increase appetite, particularly in the hours following injection. The effect is mild compared to GHRP-6, which causes intense hunger spikes.
For users on fat loss protocols, inject before bed to minimize appetite stimulation during waking hours. For those building muscle, the appetite increase supports higher caloric intake.
Headache (5-10%)
Transient headaches correlate with GH fluctuations during the first week. They are typically mild and respond to standard analgesics. Adequate hydration reduces their frequency.
If headaches are severe or persist beyond the first week, check your blood pressure. GH elevation can temporarily raise systolic pressure by 5-10 mmHg. Persistent hypertension warrants medical evaluation.
Fatigue and Drowsiness (10-15%)
GH secretion naturally peaks during deep sleep. CJC-1295/ipamorelin amplifies this pattern, which can cause drowsiness in the hours following injection. Users who inject before bed often report deeper, more restorative sleep rather than problematic fatigue.
If daytime drowsiness occurs with morning injections, switch to evening dosing. This aligns the GH pulse with the body's natural circadian secretion pattern.
DAC vs No-DAC: How the Formulation Changes Your Side Effect Profile
The term "CJC-1295" covers two distinct compounds with different side effect profiles. Knowing which version you are using determines how to manage what you experience.
| Parameter | CJC-1295 With DAC | CJC-1295 No DAC (Mod GRF 1-29) |
|---|---|---|
| Half-life | 6-8 days | ~30 minutes |
| GH pattern | Continuous elevation ("GH bleed") | Pulsatile (natural rhythm) |
| Water retention | More pronounced | Less pronounced |
| Tingling/numbness | More common | Less common |
| Insulin sensitivity | Greater impact | Smaller impact |
| Titration ease | Difficult (effects persist for days) | Easy (effects clear within hours) |
| Standard dose | 1-2 mg weekly | 100-200 mcg 2-3x daily |
The DAC version binds to albumin in the bloodstream, extending its active life from minutes to days (Jette & LeBlanc, Bioconjug Chem, 2005). This convenience has a real cost: if side effects appear, you cannot simply skip a dose and have them resolve quickly. The compound remains active for nearly a week after each injection.
The no-DAC version (Mod GRF 1-29) produces GH pulses that mimic the body's natural pulsatile secretion. Side effects are milder and resolve faster. Most clinicians pair it with ipamorelin for synergistic GH release. For DAC-specific protocols, see the CJC-1295 with DAC guide.
Why This Combo Is Better Tolerated Than Other GH Peptides
Ipamorelin earned its reputation as the "cleanest" GH secretagogue through a specific pharmacological profile documented in the Raun 1998 study. At doses 200 times the effective threshold, ipamorelin released GH without elevating cortisol, ACTH, or prolactin (Raun et al., Endocrinology, 1998). No other GH-releasing peptide achieves this level of selectivity.
| GH Secretagogue | Cortisol Increase | Prolactin Increase | Appetite Spike | Desensitization Risk |
|---|---|---|---|---|
| Ipamorelin | None | None | Mild | Low |
| GHRP-6 | Moderate | Moderate | Severe | Moderate |
| GHRP-2 | Mild-Moderate | Mild | Moderate | Moderate |
| Hexarelin | None-Mild | Significant | Mild | High |
| MK-677 | None | None | Significant | Low |
GHRP-6 floods users with hunger. GHRP-2 elevates cortisol, which disrupts sleep and promotes fat storage. Hexarelin causes prolactin spikes and desensitizes GH receptors within weeks. Ipamorelin avoids all three pitfalls.
When paired with CJC-1295, the combination activates two complementary pathways. CJC-1295 stimulates the GHRH receptor, telling the pituitary to produce GH. Ipamorelin stimulates the ghrelin receptor, telling the pituitary to release it. The synergy produces stronger GH pulses than either peptide alone, while ipamorelin's selectivity keeps the side effect profile clean. For a detailed breakdown of benefits from this mechanism, see CJC-1295/ipamorelin benefits.
Rare but Serious Side Effects to Monitor
Standard doses of CJC-1295/ipamorelin have not produced serious adverse events in clinical trials. The Teichman 2006 study tested up to 100 mcg/kg with no serious events, though higher doses increased GI side effects. The following concerns are theoretical or dose-dependent and require active monitoring.
Joint Pain and Stiffness
Prolonged GH elevation can cause arthralgia through fluid retention in joint capsules and accelerated cartilage growth. This is a class effect of all GH-elevating compounds, including pharmaceutical HGH. At standard doses, risk is low. If joint pain develops, reduce dose by 25-50%. Persistent joint pain despite dose reduction warrants discontinuation.
For users already managing joint issues, check our guide to peptides for joint pain before starting a GH secretagogue protocol.
Blood Sugar and Insulin Sensitivity
Growth hormone is a counter-regulatory hormone to insulin. Elevated GH reduces insulin sensitivity and can raise fasting blood glucose. The effect is dose-dependent and more pronounced with the DAC variant (continuous GH elevation). Monitor fasting glucose and HbA1c during your cycle.
If fasting glucose exceeds 100 mg/dL or rises more than 10 mg/dL from your baseline, consult a physician about dose adjustment. Alba et al. confirmed that CJC-1295 preserves pulsatile GH secretion, which may reduce insulin resistance risk compared to constant GH elevation from exogenous HGH (Alba et al., J Clin Endocrinol Metab, 2006).
IGF-1 and Cancer Risk: The Honest Assessment
Epidemiological studies have linked elevated IGF-1 to increased risk of certain cancers, particularly prostate, breast, and colorectal. This association is observational, not causal. CJC-1295 raises IGF-1 by 1.5-3x for 9-11 days after a single dose (Teichman 2006). No cancer cases occurred during the trial, but the study lasted only weeks.
The honest assessment: long-term IGF-1 elevation may carry theoretical cancer risk based on population data. No CJC-1295/ipamorelin trial has demonstrated a causal link. Users with a personal or family history of hormone-sensitive cancers should consult an oncologist before starting. Monitor IGF-1 levels during your cycle to ensure they remain within the reference range (normal adult range: 80-350 ng/mL).
Allergic Reactions
True allergic reactions to CJC-1295 or ipamorelin are extremely rare. Symptoms would include hives, difficulty breathing, or swelling of the face and throat. If any occur, discontinue immediately and seek emergency care. More commonly, users react to benzyl alcohol in the bacteriostatic water rather than the peptide itself. Switching to a different bac water source typically resolves this.
Long-Term Considerations and Cycling
No study has followed CJC-1295/ipamorelin users beyond several months. Long-term safety data for this combination does not exist. The considerations below derive from GH physiology and data from related compounds.
Pituitary Desensitization Risk
Continuous GHRH receptor stimulation can downregulate receptor sensitivity over time. The DAC variant carries a higher theoretical risk because it provides constant stimulation. The no-DAC version, with its pulsatile pattern, more closely mimics natural GHRH signaling and likely carries lower desensitization risk.
Standard cycling protocols address this: 8-12 weeks on, 4-6 weeks off. The off-cycle allows GHRH receptors to resensitize. Some users report diminishing GH response after 3-4 months of continuous use, supporting the cycling approach.
Cycling Protocols by Experience Level
The most common protocols in clinical practice are:
| Protocol | On Cycle | Off Cycle | Best For |
|---|---|---|---|
| Standard | 8 weeks | 4 weeks | Beginners, general wellness |
| Extended | 12 weeks | 4-6 weeks | Body composition goals |
| Maintenance | 16 weeks | 6-8 weeks | Experienced users |
During the off-cycle, GH secretion returns to baseline within 1-2 weeks. IGF-1 normalizes within 2-4 weeks. Resume the next cycle only after IGF-1 returns to your pre-treatment baseline. For a complete cycling guide, see our CJC-1295 dosage guide.
Blood Work and Monitoring Protocol
Running blood markers throughout your cycle catches problems early and confirms the peptides are working. This schedule applies to both DAC and no-DAC protocols.
| Timing | Labs to Run | What to Watch |
|---|---|---|
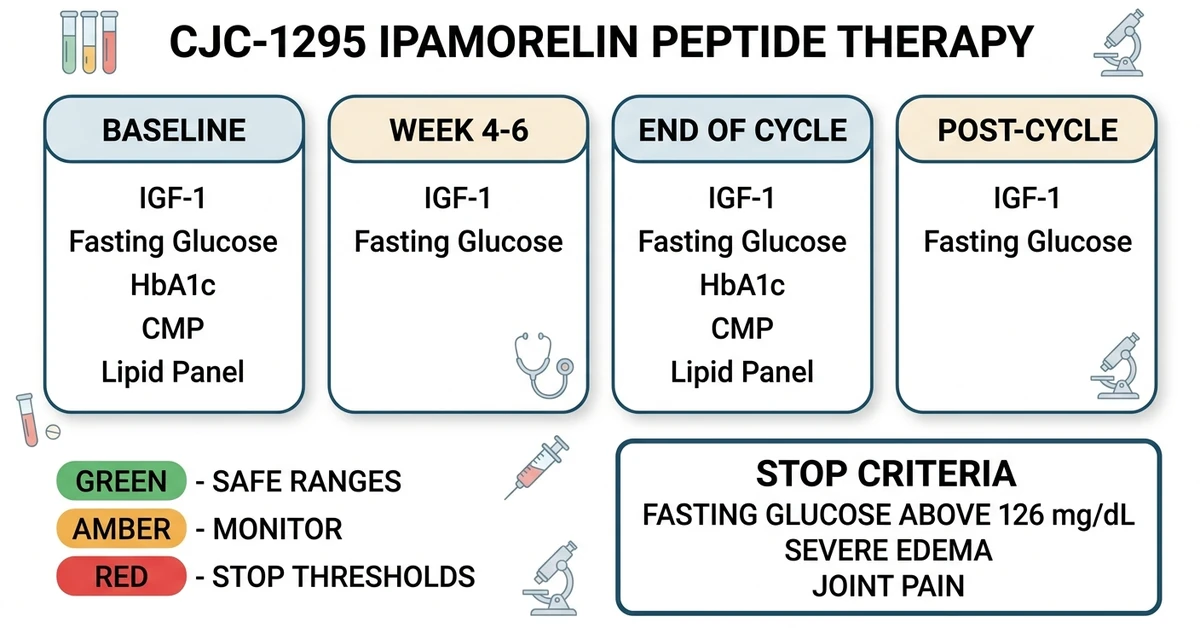
| Baseline (before starting) | IGF-1, fasting glucose, HbA1c, CMP, lipid panel | Establish reference values |
| Mid-cycle (week 4-6) | IGF-1, fasting glucose, fasting insulin | IGF-1 elevated; glucose stable |
| End of cycle | IGF-1, fasting glucose, HbA1c, CMP | Check for metabolic changes |
| Post-cycle (4 weeks after) | IGF-1, fasting glucose | Confirm return to baseline |
Stop your cycle immediately if: fasting glucose consistently exceeds 126 mg/dL, severe edema persists despite dose reduction and dietary changes, joint pain limits daily activities, or any sign of allergic reaction develops.
For comprehensive safety protocols across all peptide classes, see our peptide safety guide. For reconstitution and sterility guidance, see how to reconstitute peptides.
CJC-1295/Ipamorelin vs HGH Side Effects Compared
Users frequently compare the CJC-1295/ipamorelin stack to pharmaceutical HGH injections. Both elevate GH and IGF-1, but through fundamentally different mechanisms with distinct risk profiles.
| Parameter | CJC-1295/Ipamorelin | Exogenous HGH |
|---|---|---|
| Mechanism | Stimulates your pituitary to release GH | Bypasses pituitary entirely |
| GH pattern | Pulsatile (natural) | Flat, supraphysiologic |
| Pituitary suppression | Minimal | Significant (negative feedback) |
| Water retention | Mild-moderate | Moderate-severe |
| Insulin resistance | Dose-dependent, usually mild | Common and dose-dependent |
| Carpal tunnel risk | 10-20% (mild) | 20-40% (can be moderate) |
| Monthly cost | $150-300 | $500-3,000 |
| Abuse potential | Low (pituitary capacity limits output) | High (no biological ceiling) |
The critical difference: CJC-1295/ipamorelin works through your body's pituitary gland. The pituitary has a built-in ceiling for GH output. You cannot achieve supraphysiologic levels the way exogenous HGH enables. This ceiling acts as a safety mechanism. For users wanting GH optimization without the risks of exogenous HGH, the combo offers a more moderate and physiological approach.
For a broader understanding of peptide risk profiles, see our peptides vs steroids comparison.
Side Effect Management: Step-by-Step Protocol
Most side effects respond to simple adjustments. Work through these steps before considering discontinuation.
Step 1: Reduce the Dose
Lower your dose by 25-50% for 7-10 days. If side effects resolve, gradually increase back to the target dose over 2-3 weeks. The body often tolerates at week 4 what it struggled with at week 1.
Step 2: Adjust Injection Timing
Flushing and drowsiness respond to timing changes. Inject before bed to sleep through the flush. Inject in the morning if evening doses cause insomnia. Splitting doses (100 mcg ipamorelin morning and evening instead of 200 mcg once) can reduce peak side effects without reducing total daily dose.
Step 3: Address Water Retention Directly
Cut sodium below 2,300 mg/day. Increase water intake to 3-4 liters. Add 200-400 mg magnesium glycinate before bed. If edema persists after 4 weeks at full dose, the DAC variant may not fit your tolerance profile. Switching to the no-DAC version paired with ipamorelin produces a milder GH profile with fewer water retention issues.
Step 4: Know When to Stop
Discontinue and consult a physician if: fasting glucose rises above 126 mg/dL on two consecutive readings, joint pain limits your ability to train or work, edema does not improve with dose reduction and dietary changes, or you develop signs of an allergic reaction. These situations are uncommon at standard doses but require prompt medical attention. See our peptide therapy side effects overview for guidance on other peptide classes.
Important Safety Warnings
CJC-1295 and ipamorelin are not approved by the FDA for any indication. All human dosing data comes from Phase I/II trials and clinical practice reports. No long-term safety studies exist for this combination.
Do not use CJC-1295/ipamorelin if you have active cancer or a history of hormone-sensitive cancers (prostate, breast, colorectal) without oncologist clearance. Elevated IGF-1 may theoretically promote tumor growth.
Do not use if you have type 1 diabetes or poorly controlled type 2 diabetes. GH elevation impairs insulin sensitivity and can worsen glycemic control. Patients with pre-diabetes should monitor glucose closely.
Pregnant or breastfeeding women should not use GH secretagogues. Effects on fetal development and breast milk composition have not been studied.
For stacking considerations, see our peptide stacking guide. For the CJC-1295 vs sermorelin decision, see our head-to-head analysis.
Frequently Asked Questions
Are CJC-1295/ipamorelin side effects dangerous?
At standard doses (CJC-1295 100-200 mcg + ipamorelin 200-300 mcg per injection), side effects are mild and self-limiting. The Teichman 2006 clinical trial reported no serious adverse events at doses up to 60 mcg/kg. Water retention, flushing, and injection site reactions are the most common issues, and all resolve within 2-4 weeks for most users. See our CJC-1295 dosage guide for safe protocol ranges.
How long do CJC-1295/ipamorelin side effects last?
Most side effects peak during weeks 1-2 and resolve by week 4. Injection site reactions clear within 24-48 hours. Flushing lasts 30-60 minutes per injection. Water retention stabilizes by weeks 3-4 as the body adapts to elevated GH. Tingling may take 2-6 weeks to resolve and is dose-dependent. Our CJC-1295/ipamorelin dosage calculator can help you find a tolerable starting dose.
Can CJC-1295/ipamorelin cause cancer?
No clinical trial has linked CJC-1295/ipamorelin to cancer. The concern is theoretical: elevated IGF-1 has been associated with certain cancers in epidemiological studies, but this is observational, not causal. CJC-1295 raises IGF-1 by 1.5-3x for 9-11 days per dose. Monitor IGF-1 levels during your cycle and consult an oncologist if you have a history of hormone-sensitive cancers before starting this protocol.
Should I stop if I get side effects?
Most side effects resolve with dose reduction (25-50% for 7-10 days) or timing adjustments. Discontinue only if fasting glucose exceeds 126 mg/dL, joint pain limits daily function, severe edema persists despite dietary changes, or allergic symptoms develop. Mild water retention, flushing, and tingling are normal during the first 2-4 weeks and typically resolve on their own. See our peptide safety guide for full guidance.
Is CJC-1295/ipamorelin safer than HGH?
CJC-1295/ipamorelin works through the pituitary gland, which limits maximum GH output. Exogenous HGH bypasses this ceiling, enabling supraphysiologic levels with greater risks. The combo produces less water retention, lower carpal tunnel rates (10-20% vs 20-40%), and minimal pituitary suppression compared to HGH. The tradeoff is less potent GH elevation. For full context, see our CJC-1295/ipamorelin benefits guide.
What side effects differ between DAC and no-DAC versions?
CJC-1295 with DAC (half-life 6-8 days) causes more water retention and tingling than the no-DAC version (half-life 30 minutes). The DAC variant is harder to titrate because effects persist for days after injection. The no-DAC version produces pulsatile GH release with milder, shorter-lasting side effects but requires 2-3 daily injections. See the full DAC vs no-DAC comparison for the complete breakdown.
Can CJC-1295/ipamorelin affect blood sugar?
GH is a counter-regulatory hormone to insulin. Elevated GH can reduce insulin sensitivity and raise fasting glucose by 5-15 mg/dL. The effect is dose-dependent and more pronounced with the DAC variant. Monitor fasting glucose at baseline and mid-cycle (week 4-6). If fasting glucose exceeds 100 mg/dL or rises more than 10 mg/dL from baseline, consult your physician. Our reconstitution calculator can help you manage accurate dosing.
Does ipamorelin cause cortisol spikes?
No. Ipamorelin is the only GH secretagogue documented to not elevate cortisol, ACTH, or prolactin at any tested dose. Raun et al. (1998) demonstrated this selectivity at doses up to 200 times the effective threshold. This is ipamorelin's defining advantage over GHRP-6, GHRP-2, and hexarelin, all of which raise cortisol to varying degrees. See the ipamorelin profile for the full selectivity data.
The Bottom Line
CJC-1295/ipamorelin is one of the mildest GH secretagogue stacks documented in clinical literature. The Teichman 2006 trial confirmed no serious adverse events at standard doses. The most common effects are injection site reactions, water retention, and flushing, all manageable with dose adjustment and timing changes. Ipamorelin's unique selectivity means no cortisol or prolactin elevation, a significant advantage over older GH-releasing peptides like GHRP-6 and hexarelin.
Run blood work at baseline, mid-cycle, and post-cycle. Cycle 8-12 weeks on, 4-6 weeks off. Reduce the dose before discontinuing if side effects develop. The DAC variant causes more water retention and is harder to titrate; new users typically do better starting with the no-DAC version.
Use our CJC-1295/ipamorelin dosage calculator to plan your protocol. For the complete CJC-1295 dosage protocol, see our CJC-1295 dosage guide. To understand how this combo compares to other GH secretagogues, see our tesamorelin vs sermorelin vs ipamorelin comparison.
Related Articles
CJC-1295 Dosage: Complete Protocol Guide
CJC-1295 dosage guide: DAC and no-DAC protocols. Dosing by goal (anti-aging, fat loss, muscle, sleep), ipamorelin stacking, and injection timing.
CJC Peptide: Which CJC-1295 Are You Holding?
CJC peptide explained: CJC-1295 with DAC (6-8 day half-life) versus CJC-1295 no DAC, which is Mod GRF 1-29. How to identify the vial you actually hold.
CJC-1295 With DAC: Long-Acting GHRH Analog
CJC-1295 with DAC: 6-8 day half-life, 2-10x GH increase, 1-2 mg weekly. GH bleed effect, desensitization risk, and stacking protocols.
CJC-1295 vs Sermorelin: Half-Life and Dosing
CJC-1295 vs sermorelin: half-life 6-8 days vs 10-20 min, GH output 2-10x vs physiologic pulse, cost, FDA status, and who picks which.