
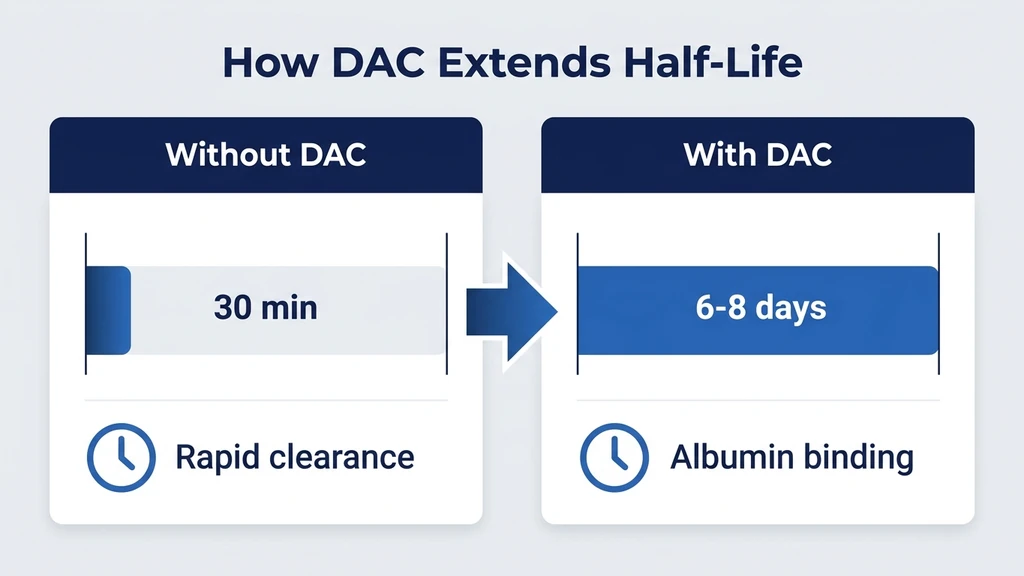
You are holding a vial labeled CJC-1295 DAC and want to understand exactly what it does before you reconstitute it. CJC-1295 with DAC (Drug Affinity Complex) is a synthetic GHRH analog that achieves a half-life of 6-8 days by covalently binding to serum albumin after injection. In a clinical trial of 21 healthy adults, a single dose produced 2-10-fold growth hormone increases for 6+ days and 1.5-3-fold IGF-1 increases for up to 11 days (Teichman et al., J Clin Endocrinol Metab, 2006). The standard protocol is 1-2 mg injected subcutaneously once or twice weekly. Unlike the no-DAC version (Mod GRF 1-29), CJC-1295 with DAC provides continuous GHRH stimulation rather than pulsatile release, creating what researchers call a "GH bleed" effect.
| Quick Reference | Details |
|---|---|
| Full name | CJC-1295 with Drug Affinity Complex |
| Class | GHRH analog (growth hormone-releasing hormone) |
| Half-life | 6-8 days (vs ~30 min for no-DAC version) |
| GH increase | 2-10-fold for 6+ days per dose |
| IGF-1 increase | 1.5-3-fold for 9-11 days |
| Standard dose | 1-2 mg subcutaneous, once weekly |
| Cycle length | 8-16 weeks on, 4-6 weeks off |
| FDA status | Not approved for any indication |
| Developer | ConjuChem Biotechnologies (dissolved) |
For dosing calculations, use our CJC-1295/ipamorelin dosage calculator. For reconstitution, see our peptide reconstitution calculator.
CJC-1295 with DAC is not FDA-approved for any indication. No long-term human safety data exists. Consult a healthcare provider before use. Do not use with active cancer or uncontrolled diabetes.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
What Is CJC-1295 With DAC?
CJC-1295 with DAC is a modified version of growth hormone-releasing hormone (GHRH). The base peptide is GRF(1-29), the first 29 amino acids of natural GHRH, with four amino acid substitutions at positions 2, 8, 15, and 27 that protect it from enzymatic breakdown. The DAC component is what makes this variant unique among all GHRH analogs.
DAC stands for Drug Affinity Complex. It consists of a maleimidoproprionic acid (MPA) group attached to a lysine residue on the peptide. After injection, this MPA group reacts with a cysteine residue on serum albumin, forming a covalent bond (Jette & LeBlanc, Bioconjug Chem, 2005). The peptide effectively hitches a ride on the most abundant protein in your blood.
Think of albumin as a cargo ship circulating through your bloodstream. Without DAC, the peptide is a small molecule that gets degraded by enzymes within minutes. With DAC, the peptide bolts itself to the hull of the cargo ship and circulates for days. Albumin has a half-life of approximately 19 days in humans, and the peptide benefits from this extended circulation for as long as the bond holds.
ConjuChem Biotechnologies in Montreal developed the DAC technology and identified CJC-1295 as their lead compound. The company progressed through Phase I/II clinical trials before dissolving. The compound was never submitted for FDA approval.
How CJC-1295 DAC Works: The GH Bleed Effect
Normal GH secretion is pulsatile. Your pituitary releases 6-12 GH pulses per day, with the largest occurring during stage 3-4 deep sleep. Between pulses, GH levels drop to near zero. This pulsatile pattern is how the body regulates GH signaling: receptor sensitivity is preserved through intermittent stimulation.
CJC-1295 with DAC disrupts this pattern by providing continuous GHRH receptor stimulation. The peptide circulates for 6-8 days, delivering a constant "release GH" signal to the pituitary. The result is sustained elevation of baseline GH levels rather than distinct peaks and troughs. Researchers call this the "GH bleed" effect.
Alba et al. studied this phenomenon and found an important nuance: pulsatile GH secretion persists on top of the elevated baseline (Alba et al., J Clin Endocrinol Metab, 2006). The pituitary still produces GH pulses; they simply start from a higher floor. This is partially reassuring because pulsatile GH signaling activates different gene pathways than continuous exposure.
The GH bleed creates a real tradeoff. Sustained elevation drives continuous IGF-1 production in the liver, supporting fat metabolism and tissue repair around the clock. The cost: continuous GH elevation impacts insulin sensitivity more than pulsatile release, and side effects are harder to manage because the compound remains active for days after each injection.
Clinical Evidence
Two key clinical studies inform our understanding of CJC-1295 with DAC.
The Teichman 2006 Study (Primary Evidence)
This randomized, placebo-controlled, double-blind trial enrolled 21 healthy adults aged 21-61. Subjects received single or multiple subcutaneous doses of CJC-1295 at 30, 60, or 100 mcg/kg. The findings form the foundation of all current CJC-1295 dosing protocols.
Key results: GH levels increased 2-10-fold within 2 hours and remained elevated for 6+ days after a single dose. IGF-1 rose 1.5-3-fold and stayed elevated for 9-11 days. After multiple weekly doses, mean IGF-1 remained elevated for 28 days. The dose-response was clear: higher doses produced greater and longer GH elevation (PMID: 16352683).
Safety data: No serious adverse events occurred at 30-60 mcg/kg. At 100 mcg/kg, GI side effects increased significantly. The study authors concluded that 30-60 mcg/kg was the optimal range, balancing efficacy with tolerability. For a 75 kg (165 lb) person, that translates to approximately 2.25-4.5 mg per dose.
The GHRH Knockout Mouse Study
Ionescu and Bhatt demonstrated that once-daily CJC-1295 normalized growth in mice genetically engineered to lack GHRH production (Ionescu & Bhatt, Endocrinology, 2006). These mice, which cannot produce their own GHRH, grew normally when treated with CJC-1295.
The clinical implication: CJC-1295 is potent enough to replace endogenous GHRH function entirely. For users with intact GHRH systems, the compound adds to existing signaling rather than replacing it, making outcomes harder to predict and individual variation higher.
Benefits of CJC-1295 With DAC
The following benefits are supported by clinical data on GH/IGF-1 elevation and extrapolated from the established physiology of growth hormone. Body composition endpoints specific to CJC-1295 have not been studied in Phase III trials.
Sustained GH and IGF-1 Elevation
The defining benefit. A single weekly injection produces continuous GH and IGF-1 elevation. No other peptide provides this duration of effect from a single dose. Your body processes GH and its downstream signals 24 hours a day throughout the cycle, rather than in brief daily pulses that clear within hours.
Fat Loss and Body Composition
GH promotes lipolysis through hormone-sensitive lipase activation. IGF-1 shifts nutrient partitioning toward muscle protein synthesis and away from fat storage. Sustained GH/IGF-1 elevation supports more consistent fat oxidation than pulsatile alternatives. For proven visceral fat reduction with Phase III clinical data, tesamorelin is the better-documented option. For a comprehensive review of GH peptides for weight loss, see best peptides for weight loss.
Muscle Recovery and Growth
IGF-1 drives satellite cell activation and muscle protein synthesis. Sustained elevation supports recovery between training sessions. Users typically report improved recovery within the first 2-3 weeks. Measurable strength and lean mass changes appear at 6-12 weeks. CJC-1295 DAC supports the recovery infrastructure; it does not replace training stimulus or adequate nutrition.
Sleep Quality Improvement
GH secretion peaks during deep sleep. Many users report deeper, more restorative sleep beginning in weeks 1-2. Vivid dreams are a commonly reported early signal that the compound is active. The sleep benefit partially reflects improved GH-mediated tissue repair during overnight recovery. For a comparison of sleep-focused peptides, see our peptides for sleep guide.
Convenient Weekly Dosing
One to two injections per week versus the 7-21 injections required by sermorelin or CJC-1295 no-DAC. For users who travel frequently or have low injection tolerance, the DAC version eliminates a significant practical barrier. This convenience advantage is why many users choose the DAC variant despite its less physiological GH release pattern.
CJC-1295 DAC Dosing Protocol
The Teichman study established 30-60 mcg/kg as the optimal dose range. Clinical practice uses fixed doses rather than weight-based calculations for convenience.
| Protocol Level | Dose | Frequency | Cycle Length | Best For |
|---|---|---|---|---|
| Beginner | 1 mg | Once weekly | 8-12 weeks | First-time users; assessing tolerance |
| Standard | 2 mg | Once weekly | 12-16 weeks | Body composition; recovery |
| Advanced | 2 mg | Twice weekly (Mon/Thu) | 12-16 weeks | Maximum GH/IGF-1 elevation |
Starting protocol: Begin at 1 mg weekly for the first 2-3 weeks. CJC-1295 DAC has a long washout period: steady-state levels take 2-3 weeks to achieve and 2-3 weeks to clear after stopping. Assess tolerance before increasing to 2 mg.
Stacking with ipamorelin: The most common clinical protocol combines CJC-1295 DAC at 1-2 mg weekly with ipamorelin at 200-300 mcg daily. CJC-1295 DAC provides continuous GHRH receptor stimulation; ipamorelin adds targeted GH pulses through the ghrelin receptor. Two pathways produce greater GH output than either compound alone. For full stack data, see CJC-1295/ipamorelin benefits.
Injection timing: CJC-1295 DAC can be injected at any time of day because effects persist for 6-8 days regardless of timing. A fixed weekly schedule (e.g., every Monday morning) improves consistency.
For detailed protocols, see our CJC-1295 dosage guide.
Reconstitution and Storage
CJC-1295 DAC arrives as a lyophilized (freeze-dried) powder requiring reconstitution before injection.
Reconstitution: Add 2 mL of bacteriostatic water to a 5 mg vial. This yields a concentration of 2.5 mg/mL. Draw 0.4 mL (40 units on an insulin syringe calibrated to 100 units/mL) for a 1 mg dose. Draw 0.8 mL (80 units) for a 2 mg dose. Direct the water stream against the glass wall, not directly onto the powder. Swirl gently; do not shake or vortex.
Storage: Store lyophilized powder at -15°C (5°F) or below for long-term storage, or at 2-8°C (refrigerator) for up to 6 months. Once reconstituted, store at 2-8°C and use within 3-4 weeks. Never freeze reconstituted peptide.
Use our peptide reconstitution calculator for exact draw volumes for any vial size. For step-by-step reconstitution technique, see how to reconstitute peptides. For shelf life details, see how long reconstituted peptides last.
Side Effects of CJC-1295 With DAC
The DAC variant produces more pronounced side effects than the no-DAC version because sustained GH elevation drives stronger fluid retention and metabolic effects.
Common Side Effects
Water retention affects 15-25% of users and is the most frequently reported side effect. It peaks during weeks 1-4 and typically stabilizes by week 6. Injection site reactions (20-30%) are brief and resolve within 24-48 hours. Facial flushing (15-20%) appears 5-15 minutes post-injection and resolves within 30-60 minutes. Tingling or numbness in extremities (10-20%) results from fluid pressure on peripheral nerves and is dose-dependent. Increased appetite (10-15%) stems from ghrelin pathway interactions.
For complete management protocols covering all GH-class side effects, see our CJC-1295/ipamorelin side effects guide.
DAC-Specific Concerns
The long half-life creates a management challenge: if side effects develop, you cannot clear the compound quickly. A dose injected Monday remains active through Sunday. Full dose reduction takes 2-3 weeks to reflect in your symptom profile.
Pituitary desensitization is a real concern with continuous GHRH receptor stimulation. The body may downregulate receptor sensitivity with extended use. Cycling (8-16 weeks on, 4-6 weeks off) is standard to mitigate this.
Insulin sensitivity impact is greater with continuous GH elevation versus pulsatile release. Monitor fasting glucose and HbA1c during your cycle. If fasting glucose exceeds 100 mg/dL or rises more than 10 mg/dL from your baseline, consult your physician.
The Safety Incident: Transparent Disclosure
One death was reported during clinical development of CJC-1295. The Wikipedia entry on CJC-1295 references this event. The circumstances and causal relationship have not been clarified in peer-reviewed literature, so no definitive conclusion about causality can be drawn.
This event underscores the importance of medical supervision when using any research compound. CJC-1295 has not completed the safety review required for FDA approval. Users accept an inherent level of uncertainty about long-term safety. This is not a reason to avoid the compound, but it is information that belongs in any honest guide.
CJC-1295 DAC vs No-DAC: Which Is Better?
This is the most common question from new users. The answer depends on your priorities.
| Parameter | CJC-1295 With DAC | CJC-1295 No DAC (Mod GRF 1-29) |
|---|---|---|
| Half-life | 6-8 days | ~30 minutes |
| GH release pattern | Continuous (GH bleed) | Pulsatile (natural) |
| Injection frequency | 1-2x weekly | 2-3x daily |
| Water retention | More pronounced | Less pronounced |
| Titration ease | Difficult (long washout) | Easy (clears in hours) |
| Pituitary desensitization risk | Higher (continuous stimulation) | Lower (intermittent stimulation) |
| Insulin sensitivity impact | Greater | Milder |
| Convenience | High | Low |
Choose DAC for weekly dosing convenience, maximum sustained IGF-1 elevation, and if you are comfortable with the more pronounced side effect profile.
Choose no-DAC for natural pulsatile GH release, easier dose titration, and stack compatibility with ipamorelin for targeted daily GH pulses.
For the full comparison, see our DAC vs no-DAC guide. For no-DAC protocols, see our CJC-1295 no-DAC guide.
Results Timeline: Week by Week
Individual responses vary significantly. The following reflects commonly reported experiences from clinical practice.
| Timeframe | Expected Changes |
|---|---|
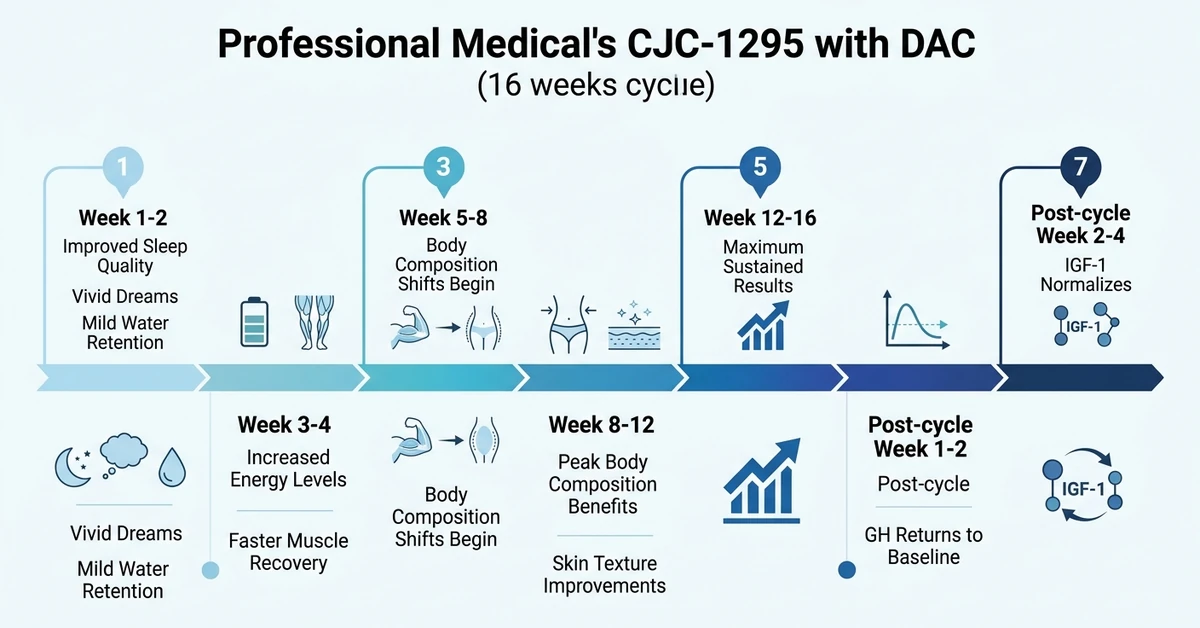
| Week 1-2 | Improved sleep depth, vivid dreams, mild water retention begins |
| Week 3-4 | Increased energy, faster workout recovery, appetite changes |
| Week 5-8 | Body composition shifts begin (fat loss, lean tissue gains) |
| Week 8-12 | Peak body composition benefits; skin and hair quality improvements |
| Week 12-16 | Maximum sustained results for extended cycles |
| Post-cycle week 1-2 | GH returns to baseline; water retention resolves |
| Post-cycle week 2-4 | IGF-1 normalizes; benefit retention depends on training |
CJC-1295 DAC is not a substitute for training and nutrition. Users who do not exercise and eat appropriately will see minimal body composition changes regardless of GH elevation. The peptide supports recovery infrastructure; it does not create results in the absence of stimulus.
For how this compound compares to alternatives, see CJC-1295 vs sermorelin. For the FDA-approved GHRH analog comparison, see tesamorelin vs CJC-1295.
Blood Work and Monitoring Protocol
Monitoring blood markers throughout your cycle catches problems early and documents whether the compound is working.
| Timing | Labs to Run | What to Watch |
|---|---|---|
| Baseline | IGF-1, fasting glucose, HbA1c, CMP, lipid panel | Establish reference values |
| Week 4-6 | IGF-1, fasting glucose, fasting insulin | IGF-1 elevated; glucose stable |
| End of cycle | IGF-1, fasting glucose, HbA1c, CMP | Check for metabolic changes |
| Post-cycle (4 weeks after) | IGF-1, fasting glucose | Confirm return to baseline |
Target IGF-1 range: remain within the upper-normal reference range for your age (generally 80-350 ng/mL for adults). Levels substantially above this may increase side effect risk. If fasting glucose exceeds 126 mg/dL on two consecutive readings, consult your physician and consider stopping.
For comprehensive safety guidance, see our peptide safety guide. For CJC-1295/ipamorelin side effects and monitoring, see our dedicated side effects guide.
Important Safety Warnings
CJC-1295 with DAC is not FDA-approved for any indication. All human dosing data comes from a single Phase I/II trial of 21 subjects. No long-term safety data exists.
Do not use if you have active cancer or a history of hormone-sensitive cancers (prostate, breast, colorectal) without oncologist clearance. GH and IGF-1 elevation may theoretically promote tumor growth.
Do not use with type 1 diabetes or poorly controlled type 2 diabetes. Continuous GH elevation impairs insulin sensitivity.
Discontinue if IGF-1 exceeds the upper reference range for your age, fasting glucose rises above 126 mg/dL, or severe persistent edema develops.
For stacking guidance, see our peptide stacking guide. For a broader GH peptide comparison including FDA-approved options, see tesamorelin vs sermorelin vs ipamorelin.
Frequently Asked Questions
What does DAC stand for in CJC-1295?
DAC stands for Drug Affinity Complex. It is a maleimidoproprionic acid (MPA) moiety attached to the CJC-1295 peptide that covalently binds to serum albumin after injection. This albumin binding extends the peptide's half-life from approximately 30 minutes (without DAC) to 6-8 days, enabling weekly dosing instead of multiple daily injections. See our DAC vs no-DAC guide for the full comparison.
How often do you inject CJC-1295 with DAC?
The standard protocol is 1-2 mg subcutaneously once per week. Advanced users may split into two weekly doses (e.g., 1 mg Monday and 1 mg Thursday). Injection can occur at any time of day because the 6-8 day half-life provides continuous activity regardless of timing. Beginners should start at 1 mg weekly for 2-3 weeks before adjusting. Use our dosage calculator for guidance.
What is the half-life of CJC-1295 with DAC?
CJC-1295 with DAC has a measured half-life of 5.8-8.1 days in the Teichman 2006 clinical trial. This is approximately 500 times longer than CJC-1295 without DAC (30 minutes) and 350 times longer than sermorelin (10-20 minutes). The extended half-life results from covalent binding to serum albumin after subcutaneous injection.
Can you stack CJC-1295 DAC with ipamorelin?
Yes. CJC-1295 DAC (1-2 mg weekly) plus ipamorelin (200-300 mcg daily) is the most common clinical stack. CJC-1295 DAC provides continuous GHRH receptor stimulation while ipamorelin adds targeted GH pulses through the ghrelin receptor. The two pathways are synergistic, producing greater GH output than either peptide alone. See our CJC-1295/ipamorelin benefits guide for full data.
Is CJC-1295 with DAC FDA approved?
No. CJC-1295 with DAC has never been FDA-approved for any indication. It progressed through Phase I/II clinical trials under ConjuChem Biotechnologies but was never submitted for FDA approval. The company has dissolved. CJC-1295 is available through compounding pharmacies as a research compound with a valid prescription from a licensed physician.
What is the GH bleed effect?
GH bleed refers to the continuous elevation of baseline GH caused by CJC-1295 DAC's persistent GHRH receptor stimulation. Normal GH secretion is pulsatile (6-12 pulses per day with near-zero baseline between pulses). CJC-1295 DAC raises the baseline so GH never drops to zero. Alba et al. (2006) showed that pulsatile secretion persists on top of this elevated baseline, partially preserving the natural GH signaling pattern.
How long should you cycle CJC-1295 DAC?
Standard cycles run 8-16 weeks on, followed by 4-6 weeks off. The off-cycle allows GHRH receptors to resensitize and IGF-1 to return to baseline before the next cycle. Beginners should start with 8-week cycles. Do not resume until IGF-1 returns to your pre-treatment values at post-cycle testing. Monitor fasting glucose and HbA1c throughout.
How does CJC-1295 DAC compare to HGH?
CJC-1295 DAC stimulates your pituitary to release GH naturally, with a biological ceiling on output. Exogenous HGH bypasses the pituitary entirely, enabling supraphysiologic doses. HGH is more potent but carries higher risks: pituitary suppression, more severe water retention, and costs $500-3,000 per month versus $150-300 for CJC-1295 DAC. For the comparison with FDA-approved GHRH alternatives, see tesamorelin vs CJC-1295.
The Bottom Line
CJC-1295 with DAC is the longest-acting GHRH analog available. The Teichman 2006 trial confirmed 2-10-fold GH increases and 1.5-3-fold IGF-1 increases from a single dose, with effects lasting 6+ days. Weekly dosing at 1-2 mg is the standard protocol, typically combined with daily ipamorelin for dual-pathway synergy.
The tradeoffs are real and worth understanding before you inject. The GH bleed effect impacts insulin sensitivity more than pulsatile alternatives. Side effects are harder to manage because the compound remains active for nearly a week after each injection. One safety incident occurred during clinical development. No long-term human safety data exists. Cycle 8-16 weeks on, 4-6 weeks off, and monitor blood work throughout.
Use our CJC-1295/ipamorelin dosage calculator to plan your protocol. For reconstitution, see our peptide reconstitution calculator. For how this compound compares to alternatives, see CJC-1295 vs sermorelin and tesamorelin vs CJC-1295.
Related Articles
CJC Peptide: Which CJC-1295 Are You Holding?
CJC peptide explained: CJC-1295 with DAC (6-8 day half-life) versus CJC-1295 no DAC, which is Mod GRF 1-29. How to identify the vial you actually hold.
Tesamorelin Peptide: Uses, Evidence, Risks
Tesamorelin peptide explained: a GHRH analogue FDA-approved as Egrifta for HIV lipodystrophy. What it does to visceral fat, IGF-1, and who should avoid it.
CJC-1295/Ipamorelin Side Effects: Manage Them
CJC-1295/ipamorelin side effects: injection reactions 20-30%, water retention 15-25%, flushing 15-20%. DAC comparison and management.
CJC-1295 vs Sermorelin: Half-Life and Dosing
CJC-1295 vs sermorelin: half-life 6-8 days vs 10-20 min, GH output 2-10x vs physiologic pulse, cost, FDA status, and who picks which.