You are holding a vial labeled CJC-1295 and a second vial labeled ipamorelin. Your protocol sheet says "100 mcg CJC / 200 mcg ipamorelin, subcutaneous, before bed." The syringe is ready. But the vial does not say whether it contains CJC-1295 with DAC or without DAC, and that distinction changes everything about how you dose it.
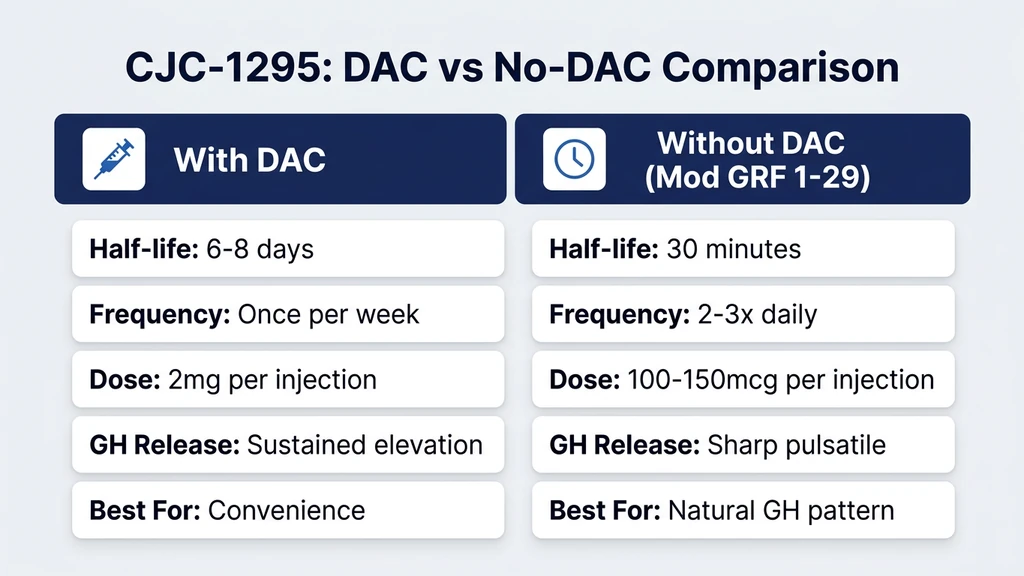
CJC-1295 with DAC (Drug Affinity Complex) is injected once or twice per week at 1,000 to 2,000 mcg per dose. CJC-1295 without DAC (also called Modified GRF 1-29) is injected one to three times daily at 100 to 300 mcg per dose. Same name, radically different protocols.
Quick reference: CJC-1295 dosage by variant
| Parameter | CJC-1295 with DAC | CJC-1295 without DAC (Mod GRF 1-29) |
|---|---|---|
| Dose per injection | 1,000-2,000 mcg | 100-300 mcg |
| Frequency | 1-2x per week | 1-3x per day |
| Half-life | 5-8 days | 25-30 minutes |
| GH release pattern | Sustained elevation | Pulsatile burst |
| Best paired with | Standalone or GHRP | Ipamorelin (most common) |
| Typical cycle | 8-12 weeks | 8-16 weeks |
Use our CJC-1295 + Ipamorelin dosage calculator to build your exact protocol based on vial size and target dose. For dosage reference across all peptides, see the complete peptide dosage chart.
CJC-1295 is not FDA-approved for any indication. All dosage information below comes from published clinical and preclinical data plus established community protocols. This is an educational resource. Consult a qualified healthcare provider before acting on any information. For broader peptide safety context, see the peptide safety guide.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
What Is CJC-1295 and How Does It Work?
CJC-1295 is a synthetic analog of growth hormone-releasing hormone (GHRH). Your hypothalamus naturally secretes GHRH in pulses to tell your pituitary gland to release growth hormone. CJC-1295 mimics that signal, but with a dramatically extended duration of action compared to the natural hormone.
Natural GHRH survives in the bloodstream for fewer than 7 minutes before enzymes break it apart. That is too short for a single injection to produce meaningful clinical effect. CJC-1295 solves this problem through structural modifications that resist enzymatic degradation (Teichman et al., J Clin Endocrinol Metab 2006).
Think of it like a slow-release fertilizer versus a liquid spray. The liquid spray (natural GHRH) feeds the plant for minutes. The slow-release pellet (CJC-1295 with DAC) feeds it for days. Both deliver the same nutrient. The delivery timeline is what changes.
Two versions exist, and they behave very differently in the body.
CJC-1295 with DAC (Drug Affinity Complex)
The DAC modification attaches CJC-1295 to albumin in the bloodstream through a reactive chemical group. Albumin is a large protein with a half-life of approximately 20 days, and once CJC-1295 binds to it, the peptide inherits that slow clearance rate. The result: a single injection elevates GH levels for 5 to 8 days (Teichman et al., J Clin Endocrinol Metab 2006).
In the key human trial, a single 60 mcg/kg dose of CJC-1295-DAC increased mean GH levels 2 to 10-fold above baseline for up to 6 days. IGF-1 levels rose by 1.5 to 3-fold and remained elevated for 9 to 11 days after a single injection.
The tradeoff is specificity. Because DAC keeps CJC-1295 active for days, GH elevation is sustained rather than pulsatile. Your pituitary normally releases GH in sharp bursts, especially during deep sleep. DAC creates a constant, low-grade stimulus instead. Some researchers consider this less physiological than the pulsatile pattern. Others argue the sustained IGF-1 elevation is the primary therapeutic benefit regardless of the GH release pattern.
CJC-1295 without DAC (Modified GRF 1-29)
Without the DAC modification, CJC-1295 has a half-life of approximately 25 to 30 minutes. This is dramatically longer than natural GHRH (under 7 minutes) but far shorter than the DAC version. The result is a sharp, pulsatile GH release that peaks within 15 to 30 minutes and returns to baseline within 2 to 3 hours.
Modified GRF 1-29 (also sold as "CJC-1295 no DAC" or simply "Mod GRF") contains amino acid substitutions at positions 2, 8, 15, and 27 of the original GHRH(1-29) fragment. These substitutions protect against dipeptidyl peptidase-IV (DPP-IV) cleavage, the enzyme that destroys natural GHRH within minutes (Alba et al., J Med Chem 2006).
The short half-life is actually the advantage for many users. It produces GH release that mimics the body's natural pulsatile rhythm. When injected before bed, it amplifies the largest natural GH surge of the day (the one that occurs during slow-wave sleep). This pulsatile pattern preserves the negative feedback loop: somatostatin still regulates the system normally between pulses.
CJC-1295 Dosage Protocols: DAC vs No-DAC
The two variants require entirely different dosing strategies. Confusing them is the most common mistake in GH peptide dosing. Injecting a DAC dose on a no-DAC schedule (or vice versa) either wastes product or overwhelms the pituitary with continuous stimulation.
CJC-1295 with DAC: Weekly Dosing Protocol
The DAC version is dosed infrequently because of its long half-life. One injection sustains GH elevation for nearly a week.
| Phase | Dose | Frequency | Duration |
|---|---|---|---|
| Loading (optional) | 2,000 mcg | Twice per week | Weeks 1-2 |
| Standard | 1,000-2,000 mcg | Once per week | 8-12 weeks |
| Conservative | 1,000 mcg | Once per week | 8-12 weeks |
| Aggressive | 2,000 mcg | Twice per week | 8-12 weeks |
In the Teichman et al. trial, subjects receiving weekly doses of 30 to 60 mcg/kg (roughly 2,000 to 4,000 mcg for an 80 kg adult) showed sustained IGF-1 elevation with no serious adverse events over the study period (Teichman et al., J Clin Endocrinol Metab 2006).
Most community protocols settle on 2,000 mcg once weekly, injected subcutaneously. Some users prefer splitting to 1,000 mcg twice weekly (e.g., Monday and Thursday) for more stable blood levels. Both approaches produce comparable IGF-1 elevation.
CJC-1295 with DAC is typically used standalone, without ipamorelin. The sustained GH elevation from DAC already provides continuous stimulation. Adding a GHRP on top of that can lead to excessive GH exposure and increased side effects like water retention and numbness.
CJC-1295 without DAC (Mod GRF 1-29): Daily Dosing Protocol
Without DAC, the peptide clears within hours. Daily (or multiple daily) injections are required.
| Protocol | Dose per Injection | Frequency | Best For |
|---|---|---|---|
| Minimal | 100 mcg | Once daily (before bed) | Anti-aging, sleep |
| Standard | 100-200 mcg | 2x daily (morning + before bed) | General GH optimization |
| Aggressive | 200-300 mcg | 3x daily (morning, post-workout, before bed) | Muscle growth, fat loss |
| With ipamorelin | 100 mcg CJC + 200 mcg ipamorelin | 1-3x daily | Most popular protocol |
The saturation dose for Mod GRF 1-29 is approximately 100 mcg (or 1 mcg/kg body weight). Above this threshold, the pituitary's GHRH receptors are fully occupied, and additional CJC-1295 produces diminishing returns. Going from 100 mcg to 300 mcg does not triple GH output. It may increase it by 20 to 30% at best (Ionescu & Ghigo, Endocrine 2005).
This is why stacking with ipamorelin is standard practice. Rather than increasing CJC-1295 above its saturation dose, adding a second peptide that activates a completely different receptor (the ghrelin/GHS receptor) amplifies total GH release more efficiently. The two peptides work through separate pathways and produce a synergistic pulse.
Dosage by Goal: Anti-Aging, Fat Loss, Muscle Growth, Sleep
The same peptide serves different purposes depending on dose, timing, and combination strategy. Your goal determines which protocol fits best.
Anti-Aging and General Wellness
Growth hormone declines approximately 14% per decade after age 30. By age 60, many adults produce less than half the GH they did at 25. This decline contributes to thinner skin, reduced bone density, increased visceral fat, and slower recovery from injury (Rudman et al., N Engl J Med 1990).
The anti-aging protocol aims to restore GH levels toward youthful ranges without pushing into supraphysiological territory. Conservative dosing is the priority. More is not better when the goal is longevity.
| Parameter | Recommended |
|---|---|
| Variant | CJC-1295 no DAC + ipamorelin |
| Dose | 100 mcg CJC + 100 mcg ipamorelin |
| Frequency | Once daily, before bed |
| Cycle | 12-16 weeks on, 4-8 weeks off |
| Monitoring | IGF-1 at baseline, 6 weeks, 12 weeks |
The before-bed timing amplifies the natural nocturnal GH surge, the largest pulse of the day. This protocol produces the most physiological GH pattern: a strong nighttime burst followed by daytime clearance. IGF-1 typically rises 30 to 50% above baseline on this regimen, placing most users in the upper quartile of their age-adjusted reference range. For peptides that target other aspects of aging, see our GHK-Cu injection dosage guide.
Fat Loss
Growth hormone is a powerful lipolytic hormone. It mobilizes fatty acids from adipose tissue, particularly visceral fat, and shifts metabolism toward fat oxidation. Elevating GH through CJC-1295 and ipamorelin increases resting energy expenditure and preferentially targets the deep abdominal fat that wraps around organs (Møller & Jørgensen, Endocr Rev 2009).
The fat loss protocol adds a fasted morning injection to the standard before-bed dose. GH mobilizes fatty acids; the fasted state prevents insulin from re-storing them.
| Parameter | Recommended |
|---|---|
| Variant | CJC-1295 no DAC + ipamorelin |
| Dose | 100-200 mcg CJC + 200-300 mcg ipamorelin |
| Frequency | 2x daily: fasted AM + before bed |
| Cycle | 8-12 weeks on, 4 weeks off |
| Diet | Moderate caloric deficit (300-500 cal below maintenance) |
| Cardio | 30-45 min low-intensity after morning injection |
The morning injection on an empty stomach is critical. Insulin opposes GH-mediated lipolysis. Eating before or immediately after the injection blunts the fat-burning cascade. Wait at least 20 to 30 minutes after injection before eating. Light fasted cardio during that window oxidizes the mobilized fatty acids. See our tesamorelin dosage for fat loss guide for how CJC-1295 compares to FDA-approved GH-releasing peptides for visceral fat.
Muscle Growth and Recovery
GH does not build muscle the way testosterone does. It does not directly activate the androgen receptor. Instead, GH acts indirectly through IGF-1 to stimulate protein synthesis, promote satellite cell proliferation, and accelerate recovery between training sessions (Velloso, Br J Pharmacol 2008).
The practical benefit for athletes and lifters: faster recovery, better sleep quality, and improved body composition over months of consistent use. The muscle growth protocol maximizes daily GH exposure through three injection windows.
| Parameter | Recommended |
|---|---|
| Variant | CJC-1295 no DAC + ipamorelin |
| Dose | 200 mcg CJC + 200-300 mcg ipamorelin |
| Frequency | 3x daily: fasted AM, post-workout, before bed |
| Cycle | 12-16 weeks on, 4-8 weeks off |
| Training | Resistance training 4-6x/week |
| Protein | 1.6-2.2 g/kg bodyweight daily |
The post-workout window takes advantage of the exercise-induced GH surge. Resistance training itself stimulates GH release; adding CJC-1295 and ipamorelin within 30 minutes of finishing amplifies that response. Wait to eat your post-workout meal until 20 to 30 minutes after the injection.
This three-times-daily schedule demands commitment. For those who find it impractical, two daily injections (morning and night) capture roughly 80% of the benefit. For broader muscle-building peptide strategies, see our peptides for bodybuilding guide and peptide stacking guide.
Sleep Quality
Growth hormone and sleep exist in a bidirectional relationship. Deep sleep triggers GH release, and GH itself promotes the transition into slow-wave sleep stages. Users consistently report that GH peptides are among the most noticeable sleep-quality interventions they have tried.
The sleep protocol is the simplest. One injection, one time of day, low dose.
| Parameter | Recommended |
|---|---|
| Variant | CJC-1295 no DAC + ipamorelin |
| Dose | 100 mcg CJC + 100-200 mcg ipamorelin |
| Frequency | Once daily, 30 min before bed |
| Cycle | 8-16 weeks on, 4 weeks off |
| Notes | Empty stomach; last meal 2+ hours before |
A small study of 8 healthy older adults found that GHRH administration before sleep increased slow-wave sleep duration by 25% and decreased REM sleep latency (Steiger et al., Neuroendocrinology 1992). The effect was most pronounced during the first half of the night, when endogenous GH secretion is naturally highest.
Inject on an empty stomach. A meal within the preceding 2 hours raises insulin and blunts GH release. Many users combine this with magnesium glycinate (400 mg) and glycine (3 g) for additive sleep support, though no trial has tested this specific combination with GH peptides.
CJC-1295 and Ipamorelin Stack: The Standard Protocol
The CJC-1295 (no DAC) plus ipamorelin combination is the most widely used GH peptide stack in clinical and research settings. It appears in the protocols of nearly every anti-aging and optimization clinic that prescribes GH secretagogues. The reason is pharmacological synergy.
CJC-1295 activates the GHRH receptor on pituitary somatotrophs. Ipamorelin activates the growth hormone secretagogue receptor (GHS-R, also called the ghrelin receptor). These are two distinct receptor systems. Stimulating both simultaneously produces a GH pulse that exceeds the sum of either peptide alone. Anderson et al. demonstrated that combined GHRH + GHRP administration produced 2 to 3 times more GH release than either compound individually in healthy subjects (Anderson et al., J Clin Endocrinol Metab 2001).
There is a second advantage to ipamorelin specifically. Unlike older GHRPs (GHRP-6, GHRP-2, hexarelin), ipamorelin does not significantly increase cortisol, prolactin, or appetite at standard doses (Raun et al., Eur J Endocrinol 1998). This makes it the cleanest GHRP to pair with CJC-1295, and explains why clinics favor it over the alternatives.
Standard CJC-1295/Ipamorelin Stack Dosing
| Timing | CJC-1295 (no DAC) | Ipamorelin | Notes |
|---|---|---|---|
| Morning (fasted) | 100 mcg | 200 mcg | Optional: for fat loss and muscle goals |
| Post-workout | 100 mcg | 200 mcg | Optional: within 30 min of training |
| Before bed | 100 mcg | 200 mcg | Primary injection for all goals |
Minimum protocol: Once daily (before bed), 100 mcg CJC + 200 mcg ipamorelin.
Maximum protocol: Three times daily, 100-200 mcg CJC + 200-300 mcg ipamorelin per injection.
Both peptides can be drawn into the same syringe and injected together. They are chemically compatible and do not degrade each other in solution. Draw the CJC-1295 first, then the ipamorelin, from separate vials. Some compounding pharmacies sell pre-mixed CJC-1295/ipamorelin vials, which simplifies the process to a single draw.
Cycle length: 8 to 16 weeks on, followed by 4 to 8 weeks off. The off period prevents GHRH receptor desensitization and allows the pituitary to reset. Users who run continuous cycles without breaks often report diminishing returns after 4 to 5 months.
Use the CJC-1295 + Ipamorelin dosage calculator to determine your exact injection volume based on vial concentration. Check your stack for interactions with the peptide interaction checker.
Why Ipamorelin Over Other GHRPs?
Four GHRPs are commonly available: ipamorelin, GHRP-2, GHRP-6, and hexarelin. Each activates the GHS receptor, but their side effect profiles differ substantially.
| GHRP | GH Release | Cortisol Increase | Prolactin Increase | Hunger Increase | Best For |
|---|---|---|---|---|---|
| Ipamorelin | Moderate | None/minimal | None/minimal | None/minimal | Clean GH elevation, fewest sides |
| GHRP-2 | Strong | Mild | Mild-moderate | Moderate | Stronger GH release, tolerable sides |
| GHRP-6 | Strong | Moderate | Moderate | Severe | Budget option; hunger is a feature for bulking |
| Hexarelin | Strongest | Moderate | Moderate | Moderate | Short-term GH blast; desensitizes fastest |
GHRP-6 causes intense hunger within 20 minutes of injection. For someone in a caloric deficit targeting fat loss, that hunger response undermines the entire protocol. GHRP-2 is a reasonable middle ground: stronger GH release than ipamorelin, moderate side effects. Hexarelin produces the largest GH pulse but desensitizes the GHS receptor within 4 to 8 weeks, making it unsuitable for long cycles (Rahim et al., Clin Endocrinol 1998).
Ipamorelin is the default choice because it works well enough, long enough, with the fewest disruptions to cortisol, prolactin, and appetite.
What Happens When You Get CJC-1295 Dosing Wrong
Two mistakes account for most problems with CJC-1295 protocols. Both are preventable with basic knowledge.
Mistake 1: Using DAC Doses on a No-DAC Schedule
A user reads "CJC-1295 dose: 2,000 mcg" from a DAC protocol and injects 2,000 mcg of Mod GRF 1-29 three times daily. That is 6,000 mcg per day of a peptide that saturates receptors at 100 mcg. The excess floods the pituitary with GHRH signal, leading to receptor desensitization within days rather than months.
The result: severe water retention, numbness and tingling in the hands (carpal tunnel symptoms from excessive GH), facial flushing, and paradoxically reduced GH output as the pituitary downregulates its response. After 2 to 3 weeks, the user notices the peptide "stopped working." It did not stop working. The receptors stopped responding because they were overwhelmed.
The fix: verify which variant you have before your first injection. CJC-1295 with DAC is dosed in milligrams (1-2 mg) once or twice weekly. CJC-1295 without DAC is dosed in micrograms (100-300 mcg) one to three times daily. If your vendor label says "CJC-1295" without specifying DAC, assume it is the no-DAC version (Mod GRF 1-29) unless confirmed otherwise. The no-DAC version is far more commonly sold.
Mistake 2: Injecting After a Meal
A user injects 100 mcg CJC-1295 plus 200 mcg ipamorelin 20 minutes after a carbohydrate-heavy dinner. Blood glucose is elevated. Insulin is elevated. The pituitary receives the GHRH signal but the downstream GH response is blunted by 60 to 80%.
This is not a theoretical concern. Insulin is one of the strongest inhibitors of GH secretion. A study in healthy adults showed that oral glucose loading reduced GH response to GHRH by 75% compared to fasted conditions (Giustina & Veldhuis, Endocr Rev 1998). Eating before injection does not make CJC-1295 dangerous. It makes it ineffective. You are paying for a peptide and then blocking its mechanism with food.
The fix: inject on an empty stomach. Fast for at least 2 hours before injection. After injection, wait 20 to 30 minutes before eating. The GH pulse peaks within 15 to 30 minutes of a no-DAC injection and clears within 2 hours. That fasting window is when the peptide does its work.
How to Reconstitute CJC-1295
CJC-1295 (both variants) typically arrives as a lyophilized (freeze-dried) powder in vials of 2 mg or 5 mg. The powder must be reconstituted with bacteriostatic water before injection. For a detailed comparison of diluents, see bacteriostatic water vs sterile water.
Supplies Needed
| Supply | Specification |
|---|---|
| CJC-1295 vial | Lyophilized powder (2 mg or 5 mg) |
| Bacteriostatic water | 0.9% benzyl alcohol preserved |
| Insulin syringes | 29-31 gauge, 0.5 mL or 1 mL |
| Alcohol swabs | For cleaning vial stoppers and injection sites |
Always use bacteriostatic water for multi-dose vials. The benzyl alcohol preservative prevents bacterial growth and allows the reconstituted solution to last 28 to 30 days when refrigerated. Sterile water has no preservative and must be used within 24 to 48 hours. For sourcing, see where to buy bacteriostatic water for injection.
Step-by-Step Reconstitution
- 1.Clean both vial stoppers with alcohol swabs. Let dry for 10 seconds.
- 2.Draw bacteriostatic water into the syringe. For a 2 mg vial, use 1 mL (gives 2 mg/mL or 2,000 mcg/mL). For a 5 mg vial, use 2.5 mL (gives 2 mg/mL).
- 3.Insert the needle into the CJC-1295 vial at a slight angle. Let the water flow slowly down the inside wall of the glass. Never spray directly onto the lyophilized powder.
- 4.Swirl gently in a circular motion. Never shake. Shaking creates foam and denatures the peptide.
- 5.Wait until fully dissolved. The solution should be clear and colorless. If cloudy, refrigerate for 15 minutes and swirl again.
- 6.Label the vial with the date and concentration (e.g., "CJC no DAC, 2 mg/mL, reconstituted 03/17").
- 7.Refrigerate immediately at 2 to 8 degrees Celsius.
Use the reconstitution calculator to determine exact volumes for your vial size and desired concentration. For comprehensive reconstitution guidance, see how to reconstitute peptides.
Dosing After Reconstitution: Volume Reference Table
With a 2 mg vial reconstituted in 1 mL bacteriostatic water (2,000 mcg/mL concentration):
| Target Dose | Volume to Draw | Insulin Syringe Units |
|---|---|---|
| 100 mcg | 0.05 mL | 5 units |
| 200 mcg | 0.10 mL | 10 units |
| 300 mcg | 0.15 mL | 15 units |
| 1,000 mcg (DAC) | 0.50 mL | 50 units |
| 2,000 mcg (DAC) | 1.00 mL | 100 units (full syringe) |
With a 5 mg vial reconstituted in 2.5 mL bacteriostatic water (2,000 mcg/mL concentration):
| Target Dose | Volume to Draw | Insulin Syringe Units | Doses per Vial |
|---|---|---|---|
| 100 mcg | 0.05 mL | 5 units | 50 doses |
| 200 mcg | 0.10 mL | 10 units | 25 doses |
| 300 mcg | 0.15 mL | 15 units | ~16 doses |
| 1,000 mcg (DAC) | 0.50 mL | 50 units | 5 doses |
At the standard no-DAC protocol of 100 mcg before bed, a single 5 mg vial provides 50 doses: nearly two months of daily injections. That makes CJC-1295 one of the most cost-effective GH peptides available. Compare costs with the peptide cost calculator. For storage guidelines, see how to store peptides and how long do reconstituted peptides last.
Injection Timing, Sites, and Frequency
CJC-1295 is administered subcutaneously. The injection technique is the same as any other peptide. If you are new to self-injection, our how to inject peptides guide covers the complete process.
Best Time to Inject CJC-1295
Timing depends on the variant and your goal.
CJC-1295 with DAC: Timing is flexible. The 5 to 8-day half-life means the injection time barely matters. Most users inject in the morning on their chosen day(s) for consistency. There is no meaningful advantage to fasted versus fed injection with the DAC variant because the GH elevation is sustained over days, not minutes.
CJC-1295 without DAC: Timing matters significantly. The GH pulse peaks within 15 to 30 minutes and clears within 2 hours. For maximum effect:
| Injection Window | Timing Rule | Rationale |
|---|---|---|
| Before bed | 30 min before sleep, fasted 2+ hours | Amplifies natural nocturnal GH surge |
| Morning (fasted) | Immediately upon waking, before food | Maximizes fat mobilization |
| Post-workout | Within 30 min of finishing | Amplifies exercise-induced GH surge |
The before-bed injection is the highest-priority window. If you inject only once daily, this is the one to choose. The natural GH surge during slow-wave sleep is the largest of the day, and GHRH amplifies it substantially.
Injection Sites and Rotation
Subcutaneous injection sites for CJC-1295:
- Abdomen: Most common. Pinch a fold of skin 2 or more inches from the navel. Inject at a 45-degree angle.
- Front of thigh: Middle third of the upper leg. A good alternative for daily rotation.
- Upper arm (back): Viable but harder to self-inject.
For daily injections, rotate between at least three sites to prevent injection site reactions and lipohypertrophy. A simple rotation: abdomen (right), abdomen (left), right thigh, left thigh, repeat. Mark the injection site and date in a notebook or phone note. At the volumes used for no-DAC CJC-1295 (0.05 to 0.15 mL per injection), injection site reactions are rare because the fluid volume is so small.
CJC-1295 Side Effects and Safety
CJC-1295 has a favorable safety profile at standard doses. The Teichman et al. Phase 1/2 trial reported no serious adverse events at doses up to 60 mcg/kg (Teichman et al., J Clin Endocrinol Metab 2006). Side effects are dose-dependent and related to GH elevation rather than the peptide itself.
Common Side Effects
| Side Effect | Incidence | Mechanism | Management |
|---|---|---|---|
| Water retention | Common (20-30%) | GH increases sodium reabsorption | Reduce sodium intake; resolves in 2-4 weeks |
| Numbness/tingling in hands | Moderate (10-15%) | GH-mediated carpal tunnel | Reduce dose; usually transient |
| Facial flushing | Common with DAC (15-25%) | Vasodilation from sustained GHRH | Transient; resolves within 30 min |
| Injection site redness | Mild (5-10%) | Local irritation | Rotate sites; clean technique |
| Fatigue/drowsiness | Mild (5-10%) | GH-mediated (especially with nighttime dose) | Inject before bed; this is a feature for sleep |
| Headache | Occasional (5%) | IGF-1 elevation | Hydrate; resolves as body adapts |
Water retention is the most frequently reported side effect and is directly proportional to dose and GH elevation. It typically manifests as slightly puffy fingers or ankles. Reducing sodium intake and increasing water consumption helps the body adapt within 2 to 4 weeks. If numbness or tingling in the hands persists beyond 2 weeks, reduce the dose by 50% and reassess. Persistent carpal tunnel symptoms indicate IGF-1 levels may be too high.
IGF-1 Monitoring
Monitor IGF-1 levels to ensure GH elevation stays within the physiological range. Excessive IGF-1 carries long-term risks including potential promotion of existing cancerous cells. This is a theoretical concern from epidemiological data, not a demonstrated side effect of CJC-1295, but it warrants monitoring (Renehan et al., Lancet 2004).
Recommended testing schedule:
- Baseline: Before starting CJC-1295
- 6 weeks: Assess initial response
- 12 weeks: Confirm levels before continuing
Target: IGF-1 in the upper third of the age-adjusted reference range. For most adults under 50, this means 200 to 300 ng/mL. If IGF-1 exceeds 3 standard deviations above the age-adjusted mean, reduce dose or discontinue. For overall peptide safety protocols, see the peptide safety guide.
CJC-1295 vs Other GH-Releasing Peptides
Several peptides stimulate growth hormone release through different mechanisms. Choosing the right one depends on your goal, budget, and tolerance for injection frequency.
| Peptide | Mechanism | Half-Life | Dose | Frequency | Evidence Level | Monthly Cost |
|---|---|---|---|---|---|---|
| CJC-1295 with DAC | GHRH + albumin binding | 5-8 days | 1-2 mg | 1-2x/week | Phase 1/2 trial | $80-150 |
| CJC-1295 no DAC | Modified GHRH | 25-30 min | 100-300 mcg | 1-3x/day | Preclinical + community | $40-100 |
| Sermorelin | GHRH (1-29) | ~11 min | 200-500 mcg | 1x/day | FDA-approved (discontinued) | $60-120 |
| Tesamorelin | Modified GHRH (1-44) | ~26 min | 2 mg | 1x/day | Phase 3 trials | $200-500 |
| Ipamorelin | Ghrelin receptor | ~2 hours | 200-300 mcg | 1-3x/day | Phase 2 trial | $40-80 |
| MK-677 | Oral ghrelin mimetic | ~24 hours | 10-25 mg oral | 1x/day | Phase 2 trials | $30-60 |
CJC-1295 without DAC occupies the sweet spot: longer-acting than sermorelin (which degrades too fast for reliable clinical effect), shorter-acting than DAC (which sacrifices pulsatility), and considerably cheaper than tesamorelin (the only FDA-approved option in this class).
MK-677 is the convenience option: oral dosing, once daily, no injections. The tradeoff is that it elevates cortisol and appetite more than ipamorelin, and its 24-hour half-life creates continuous rather than pulsatile GH elevation. For users who cannot commit to daily injections, MK-677 is the practical alternative. For those willing to inject, CJC-1295 no DAC plus ipamorelin remains the standard.
Cycling and Long-Term Use
GH peptides are not meant for continuous indefinite use. The pituitary adapts to sustained stimulation, and receptor desensitization reduces efficacy over time. Cycling preserves the peptide's effectiveness and gives the hypothalamic-pituitary axis time to reset.
Recommended Cycling Protocols
| Protocol | On Period | Off Period | Best For |
|---|---|---|---|
| Standard | 8-12 weeks | 4 weeks | Most users |
| Extended | 12-16 weeks | 6-8 weeks | Anti-aging, conservative dosing |
| 5 days on, 2 off | Monday-Friday | Saturday-Sunday | Convenience; less effective |
The standard 8 to 12 weeks on, 4 weeks off protocol balances efficacy with recovery. During the off period, GH levels return to baseline within 1 to 2 weeks (for no-DAC) or 2 to 3 weeks (for DAC). IGF-1 follows with a slight delay, normalizing within 3 to 4 weeks after the last injection.
Do not stack multiple GH secretagogues during the off period as a "bridge." The point of the off period is pituitary recovery. Using MK-677 during the CJC-1295 off period defeats the purpose.
Track your peptide clearance with the peptide half-life tracker.
Signs You Need an Off Period
Three signals indicate the pituitary is fatiguing:
- 1.Diminishing sleep quality. The sleep improvement from nighttime GH peptides is one of the first benefits to appear and one of the first to fade when desensitization begins.
- 2.Water retention that no longer resolves. Early-cycle water retention typically subsides within 2 to 4 weeks. If it returns or worsens at month 3, the body is struggling to process continuous GH stimulation.
- 3.Stable or rising IGF-1 with reduced subjective benefits. If bloodwork shows IGF-1 remains elevated but you no longer feel the recovery and sleep benefits, the receptor response is downregulating despite adequate GH production.
When any of these appear, begin your off period regardless of where you are in the planned cycle. Pushing through desensitization wastes peptide and delays recovery.
Common CJC-1295 Dosing Mistakes
Beyond the two critical mistakes covered earlier (confusing DAC and no-DAC dosing, and injecting after meals), three additional errors frequently undermine results.
1. Exceeding the saturation dose. Injecting 300 mcg of Mod GRF 1-29 does not release three times the GH of 100 mcg. The GHRH receptor saturates at approximately 100 mcg. Higher doses produce marginally more GH release (perhaps 20 to 30% more) at three times the cost. The efficient strategy is 100 mcg CJC plus 200 mcg ipamorelin rather than 300 mcg CJC alone. Two pathways beat one overloaded pathway.
2. Skipping the off period. Running CJC-1295 for 6 or more months without a break leads to GHRH receptor desensitization. The pituitary becomes less responsive to each injection. Users report "it stopped working" around month 4 to 5. A 4-week off period after every 8 to 12 weeks of use prevents this.
3. Storing reconstituted vials at room temperature. CJC-1295 in solution degrades rapidly above 8 degrees Celsius. A vial left on a countertop for 48 hours loses significant potency. Reconstituted vials must stay refrigerated at all times. Store them in the back of the refrigerator where temperature is most stable, not in the door. For detailed storage guidance, see how to store peptides.
CJC-1295 Dosage FAQ
Frequently Asked Questions
What is the standard CJC-1295 dosage with ipamorelin?
The standard protocol is 100 mcg CJC-1295 (no DAC) plus 200 mcg ipamorelin, injected subcutaneously 1 to 3 times daily. The before-bed injection is the highest priority. Both peptides can be drawn into the same syringe. Cycle 8 to 12 weeks on, 4 weeks off.
What is the difference between CJC-1295 with DAC and without DAC?
CJC-1295 with DAC binds albumin, extending its half-life to 5 to 8 days. It is dosed at 1,000 to 2,000 mcg once or twice weekly. CJC-1295 without DAC (Mod GRF 1-29) has a 25 to 30-minute half-life and is dosed at 100 to 300 mcg one to three times daily. The no-DAC version produces pulsatile GH release; the DAC version produces sustained elevation.
When is the best time to inject CJC-1295?
For the no-DAC version, inject 30 minutes before bed on an empty stomach (fasted at least 2 hours). This amplifies the natural nocturnal GH surge. For fat loss, add a fasted morning injection. For the DAC version, timing is flexible because the half-life spans days.
Can you mix CJC-1295 and ipamorelin in the same syringe?
Yes. Both peptides are chemically compatible in the same syringe and do not degrade each other. Draw CJC-1295 first, then ipamorelin, from their separate vials into one syringe. Some compounding pharmacies sell pre-mixed vials containing both peptides at standard ratios.
How long does it take for CJC-1295 to work?
Sleep quality improvements typically appear within the first 3 to 7 days. Body composition changes (fat loss, improved recovery) become noticeable at weeks 4 to 8. IGF-1 levels measurably increase within 1 to 2 weeks of consistent dosing. Full benefits accumulate over an 8 to 12-week cycle.
How long should you cycle CJC-1295?
Run CJC-1295 for 8 to 12 weeks, then take 4 weeks off. The off period prevents GHRH receptor desensitization and allows the pituitary to reset. Without cycling, most users report diminishing returns by month 4 to 5. Anti-aging protocols may extend to 12 to 16 weeks with a 6 to 8-week break.
Does CJC-1295 cause weight gain?
CJC-1295 can cause transient water retention of 1 to 3 pounds, especially in the first 2 to 4 weeks. This is not fat gain. GH promotes lipolysis (fat breakdown) and lean mass preservation. Most users experience a net improvement in body composition over an 8 to 12-week cycle, particularly when combined with exercise and a moderate caloric deficit.
Is CJC-1295 safe to use?
In the published Phase 1/2 trial, CJC-1295 with DAC showed no serious adverse events at doses up to 60 mcg/kg. Common side effects include water retention, facial flushing, and tingling in the hands. Long-term safety data beyond 12 weeks is limited. Monitor IGF-1 levels and consult a healthcare provider.
The Bottom Line
CJC-1295 dosing comes down to one critical decision: DAC or no DAC. The DAC version requires 1,000 to 2,000 mcg once or twice weekly. The no-DAC version (Mod GRF 1-29) requires 100 to 300 mcg one to three times daily. Confusing the two is the single most consequential dosing error with this peptide.
For most users, the optimal protocol is 100 mcg CJC-1295 (no DAC) plus 200 mcg ipamorelin, injected subcutaneously 30 minutes before bed on an empty stomach. This combination amplifies the natural nocturnal GH surge through two distinct receptor systems, producing more GH release than either peptide alone. Cycle 8 to 12 weeks on, 4 weeks off.
Inject fasted. Always. Insulin blunts GH release by up to 75%. Eating before or immediately after injection wastes the peptide's primary mechanism. Wait 20 to 30 minutes after injection before food.
For exact injection volumes, use the CJC-1295 + Ipamorelin dosage calculator. For reconstitution math, use the reconstitution calculator. For clearance tracking between cycles, use the peptide half-life tracker. For cost planning, use the peptide cost calculator.
Related Articles: - Complete Peptide Dosage Chart - Peptide Stacking Guide - Peptide Safety Guide - Tesamorelin Dosage for Fat Loss - Hexarelin Dosage - Getting Started with Peptides - How to Inject Peptides - How to Store Peptides - Peptides for Bodybuilding - How Long Do Reconstituted Peptides Last
If you are not certain which version you hold, CJC peptide shows how to identify DAC from no-DAC by molecular weight, vial size, and price.
Helpful Tools
Related Articles
CJC-1295 DAC vs No DAC: How to Choose
CJC-1295 DAC (6-8 day half-life, weekly injection) vs no DAC/Mod GRF 1-29 (30-min half-life, 2-3x daily). Compare dosing, GH patterns, and cost.
Tesamorelin vs Ipamorelin: Key Differences
Tesamorelin vs ipamorelin: GHRH analog vs ghrelin mimetic. Fat loss data, dosing, side effects, cost, and stacking protocols. PubMed-cited guide.
How Much Sermorelin Per Day: Complete Dosage Guide
Sermorelin dosage: 200-500 mcg/day subcutaneous before bedtime. Starting dose, titration, gender-specific protocols, and IGF-1 monitoring.
Tesamorelin Dosage for Fat Loss
Tesamorelin dosage guide for fat loss. FDA-approved 2 mg/day protocol, visceral fat reduction data, cycling strategies, and GH peptide comparisons.