You have a specific goal. Maybe it is building muscle after 35, dropping stubborn belly fat, or fixing a libido that quietly disappeared. Peptides can help, but the right one depends on what you are trying to accomplish. The best peptides for men are CJC-1295 + ipamorelin for muscle and recovery, semaglutide for fat loss, PT-141 for sexual health, and GHK-Cu for hair loss.
Peptides are not testosterone replacement therapy. They target specific biological pathways: growth hormone release, appetite regulation, melanocortin receptor activation, collagen synthesis. No peptide here is FDA-approved for the listed indication unless noted. Consult a healthcare provider before starting any protocol.
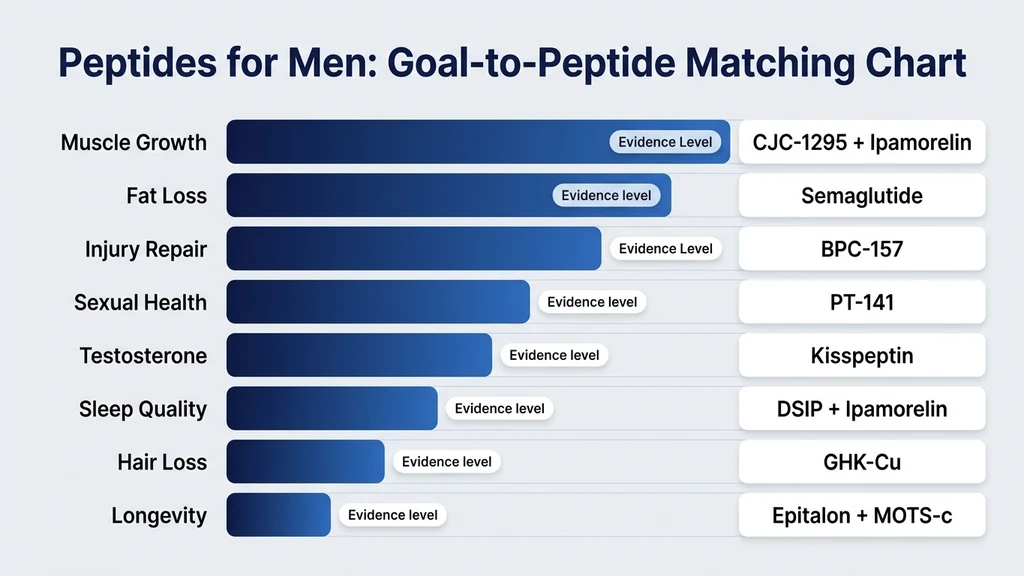
Quick-reference: best peptides for men by goal
| Goal | Best Peptide | Typical Dose | Evidence Level |
|---|---|---|---|
| Muscle growth & recovery | CJC-1295 + Ipamorelin | 100-200 mcg + 200-300 mcg before bed | Moderate (human GH data) |
| Injury repair | BPC-157 | 250-500 mcg/day | Strong (animal data) |
| Fat loss | Semaglutide | 0.25-2.4 mg/week | Strong (FDA-approved) |
| Body recomposition | 5-Amino-1MQ | 50-100 mg/day oral | Emerging (preclinical) |
| Sexual health & libido | PT-141 | 1.75 mg subcutaneous PRN | Strong (FDA-approved as Vyleesi) |
| Testosterone support | CJC-1295 + Kisspeptin | 1-2 mg/week + 10-20 mcg/day | Moderate (human endocrine data) |
| Sleep & recovery | DSIP + Ipamorelin | 100-200 mcg + 200-300 mcg before bed | Limited (small human trials) |
| Hair loss prevention | GHK-Cu | 1-2 mg/day or topical | Moderate (human skin data) |
| Longevity & anti-aging | Epitalon + MOTS-c | 5-10 mg/day + 5-10 mg/week | Moderate (human + animal data) |
For dosing protocols, see the peptide dosage chart. For combination strategies, use the peptide stack calculator.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
Why Men Turn to Peptides
Starting around age 30, a man's growth hormone output drops by roughly 14% per decade (Iranmanesh et al., J Clin Endocrinol Metab, 1991). Testosterone declines by about 1-2% per year after 30 (Travison et al., J Clin Endocrinol Metab, 2007). Recovery slows. Body fat accumulates around the midsection even when diet stays the same.
Think of these hormonal shifts like a slowly dimming thermostat. The furnace still works, but the signal telling it to fire gets weaker each year. Peptides do not replace the furnace. They turn the thermostat back up by sending stronger signals to the glands that produce growth hormone, regulate appetite, or drive sexual function. Each molecule has a narrow target, which means fewer side effects than broad-spectrum hormones.
Muscle Growth and Recovery
Muscle is the goal most men chase first. Two peptides dominate here: the CJC-1295 + ipamorelin combination for growth hormone support, and BPC-157 for injury repair that keeps training consistent.
CJC-1295 + Ipamorelin: The GH Stack
The most widely used peptide combination for men over 30. Ipamorelin triggers a GH pulse from the pituitary. CJC-1295 amplifies and extends that pulse. Together, they produce higher and longer growth hormone peaks than either alone.
CJC-1295 with DAC increased mean GH levels by 2-10 fold and IGF-1 by 1.5-3 fold over 7-14 days in a human trial (Teichman et al., J Clin Endocrinol Metab, 2006). Ipamorelin raised GH in a dose-dependent manner without spiking cortisol or prolactin (Raun et al., Eur J Endocrinol, 2005). Elevated GH drives muscle protein synthesis, tendon collagen turnover, and lipolysis.
Protocol: - Ipamorelin: 200-300 mcg subcutaneous before bed - CJC-1295 (no DAC / Mod GRF 1-29): 100-200 mcg before bed (same injection) - Duration: 8-12 weeks on, 4 weeks off. Inject fasted.
Use the CJC-1295 + ipamorelin calculator for weight-adjusted dosing. See the CJC-1295 dosage guide for a full breakdown. Expect deeper sleep within the first week, faster recovery by week 2-3, and visible body composition changes by week 6-8 (community-reported timelines, not clinical endpoints).
BPC-157: The Repair Molecule
Training consistency builds more muscle than any single supplement. Injuries kill consistency. BPC-157 is the most studied peptide for tissue repair, with positive results across tendon, muscle, ligament, and nerve models. A rat Achilles tendon study showed BPC-157 restored biomechanical strength to near-normal levels within 72 days (Chang et al., J Appl Physiol, 2011).
Protocol: - Tendon or joint injury: 250-500 mcg/day subcutaneous near the injury site, 4-8 weeks - General muscle recovery: 250 mcg/day during heavy training blocks
No completed human trial exists. See BPC-157 and muscle growth for a deeper look and use the BPC-157 dosage calculator for dosing.
Fat Loss and Body Recomposition
Belly fat that resists diet and exercise is the second most common reason men explore peptides. Three compounds address it through different mechanisms.
Semaglutide: The Appetite Reset
Semaglutide is the only FDA-approved peptide for weight management on this list. The STEP 1 trial showed a mean body weight reduction of 14.9% over 68 weeks (Wilding et al., N Engl J Med, 2021). It mimics GLP-1, a gut hormone that signals fullness, slows gastric emptying, and improves insulin sensitivity.
Protocol: - Start: 0.25 mg subcutaneous once weekly for 4 weeks - Titrate up every 4 weeks: 0.5 mg, 1.0 mg, 1.7 mg, 2.4 mg - Duration: 12+ months for sustained results
Semaglutide requires a prescription. Nausea during dose escalation is common but resolves within 2-4 weeks. Maintain resistance training and 1.6 g protein/kg/day minimum to preserve lean mass.
5-Amino-1MQ and AOD-9604: Emerging Options
5-Amino-1MQ inhibits NNMT, an enzyme elevated in visceral fat tissue. Blocking NNMT increased energy expenditure and reduced fat mass in preclinical models (Neelakantan et al., Biochem Pharmacol, 2018). Dose: 50-100 mg/day oral.
AOD-9604 is a modified fragment of human growth hormone that stimulates lipolysis without GH-related insulin resistance. A 12-week human trial showed significant fat loss versus placebo (Heffernan et al., Obes Res, 2001). Dose: 300 mcg/day subcutaneous.
Both have thinner evidence than semaglutide. They are options for men who cannot access or tolerate GLP-1 agonists, not first-line choices.
Sexual Health and Libido
Low libido affects 15-25% of men, and the percentage climbs with age (Corona et al., J Sex Med, 2010). When testosterone is normal but desire is absent, the problem often sits in the brain, not the bloodstream.
PT-141 (Bremelanotide): Central Arousal Activation
PT-141 is FDA-approved for hypoactive sexual desire disorder in women (marketed as Vyleesi) and used off-label for male sexual dysfunction. It activates melanocortin-4 receptors in the hypothalamus, producing arousal through a central nervous system pathway rather than a vascular one like PDE5 inhibitors (Viagra, Cialis).
A phase II trial in men with erectile dysfunction showed PT-141 produced erections in 67% of participants who had not responded to sildenafil (Diamond et al., Int J Impot Res, 2004). PT-141 addresses desire and arousal. PDE5 inhibitors address blood flow alone.
Protocol: - Dose: 1.75 mg subcutaneous, 45 minutes before anticipated activity - Frequency: No more than once in 24 hours, no more than 8 doses per month - Common side effects: nausea (40% of users, usually mild), flushing, headache
For men already on TRT with persistent libido issues, PT-141 addresses the neurological component that testosterone alone may not reach. For detailed protocols, see peptides for libido.
Testosterone Support
Peptides do not replace TRT. If your total testosterone is below 300 ng/dL with symptoms, testosterone replacement prescribed by a physician is the evidence-based treatment. Peptides occupy a different space: supporting endogenous production in men with borderline levels.
CJC-1295 and GH-Mediated Testosterone Support
GH and testosterone have a bidirectional relationship. GH stimulates Leydig cell function in the testes. A study in GH-deficient men showed GH replacement increased testosterone by 12-18% as a secondary effect (Giavoli et al., Eur J Endocrinol, 2012). CJC-1295 + ipamorelin raises GH, which may provide modest downstream testosterone support.
This is not a substitute for TRT. The increase is small and inconsistent. It is relevant for men in the 400-550 ng/dL range who want to optimize without committing to exogenous testosterone.
Kisspeptin: The HPG Axis Signal
Kisspeptin is the master upstream regulator of the HPG axis. It triggers GnRH release from the hypothalamus, which stimulates LH and FSH, which drives testosterone production in the testes. A single injection of kisspeptin-54 in healthy men increased LH by 3-fold and testosterone by approximately 50% within 90 minutes (Dhillo et al., J Clin Endocrinol Metab, 2005).
Protocol (investigational): - Kisspeptin-10: 10-20 mcg subcutaneous daily - Duration: 4-8 weeks, cycling with off periods
The acute testosterone spike is well-documented, but long-term data in men is limited. Kisspeptin preserves fertility (unlike exogenous testosterone), making it theoretically attractive for younger men. No commercially standardized protocol exists yet.
Sleep and Recovery
Poor sleep is the silent saboteur. Growth hormone secretion peaks during slow-wave sleep. Testosterone production follows the same pattern, with 60-70% of daily testosterone release occurring during sleep (Leproult & Van Cauter, JAMA, 2011). Fix sleep, and both hormones improve without any additional intervention.
DSIP: The Sleep Peptide
Delta sleep-inducing peptide (DSIP) modulates sleep architecture by increasing slow-wave (delta) sleep duration. A human trial showed DSIP normalized sleep patterns in patients with chronic insomnia, increasing slow-wave sleep by 20-30% (Schneider-Helmert & Schoenenberger, Eur Neurol, 1983).
Protocol: - Dose: 100-200 mcg subcutaneous or intranasal, 30 minutes before bed - Duration: 2-4 weeks, then assess
DSIP does not produce sedation like a sleeping pill. It shifts sleep architecture toward deeper phases. The evidence base is limited to small, older studies. Tolerance has not been well-characterized.
Ipamorelin for Sleep-Phase GH Release
Ipamorelin at 200-300 mcg before bed amplifies the natural GH pulse during slow-wave sleep. This single-purpose use does not require pairing with CJC-1295. The GH pulse drives overnight muscle protein synthesis, tendon repair, and fat metabolism.
Men who add bedtime ipamorelin commonly report deeper sleep and faster recovery within 1-2 weeks. These reports are anecdotal but consistent. For comprehensive recovery protocols, see peptides for recovery.
Hair Loss Prevention
Male pattern hair loss affects over 50% of men by age 50. DHT miniaturizes hair follicles, but the downstream problem is weakened dermal papilla cells and reduced scalp collagen.
GHK-Cu: Follicle Restoration from Below
GHK-Cu (glycyl-L-histidyl-L-lysine copper complex) is a tripeptide that declines with age. It stimulates collagen synthesis, increases dermal papilla cell proliferation, and modulates TGF-beta in hair follicle cycling. A gene expression study found GHK-Cu modulates 4,000+ human genes, many involved in tissue repair and follicle health (Pickart et al., BioMed Res Int, 2015). Human skin studies showed a 70% increase in collagen thickness after topical GHK-Cu (Leyden et al., J Cosmet Sci, 2002).
Protocol: - Topical: GHK-Cu serum applied to the scalp daily, often combined with microneedling - Injectable: 1-2 mg/day subcutaneous for systemic collagen support - Duration: 3-6 months minimum for visible hair changes
GHK-Cu does not block DHT. It works downstream by strengthening the tissue that DHT damages. Men on finasteride or minoxidil can add it as a complementary approach. See GHK-Cu for hair growth and the GHK-Cu microneedling guide.
Longevity and Anti-Aging
Longevity peptides target telomere maintenance and mitochondrial efficiency. The evidence is thinner than for muscle or fat loss peptides, but two compounds have human or strong mechanistic data.
Epitalon: The Telomere Peptide
Epitalon is a synthetic tetrapeptide that activates telomerase, the enzyme that maintains telomere length. Telomeres shorten with each cell division; critically short telomeres trigger cellular senescence. A human study in elderly patients showed epitalon restored telomerase activity and improved immune function markers over 6 months (Khavinson et al., Bull Exp Biol Med, 2003).
Protocol: - Dose: 5-10 mg/day subcutaneous or intramuscular - Cycle: 10-20 days on, then 4-6 months off. Repeat 2-3 cycles per year.
Epitalon does not reverse aging. It may slow one measurable component of cellular aging. The rationale is preventive, not cosmetic.
MOTS-c: The Mitochondrial Optimizer
MOTS-c is encoded by mitochondrial DNA and activates AMPK, the master switch for cellular energy regulation. AMPK activation increases mitochondrial biogenesis and improves insulin sensitivity. Plasma MOTS-c correlates with exercise capacity and declines with age (Reynolds et al., Peptides, 2021). A foundational study confirmed MOTS-c improved glucose regulation through skeletal muscle AMPK activation (Lee et al., Cell Metab, 2015).
Protocol: - Dose: 5-10 mg subcutaneous, 1-3 times per week - Duration: 4-8 weeks
See the MOTS-c dosage guide for weight-adjusted protocols.
Common Mistakes Men Make with Peptides
Mistake 1: Stacking five peptides from day one. Start with one peptide or one stack (CJC-1295 + ipamorelin counts as one stack). Add a new compound every 2-3 weeks. Running everything simultaneously makes it impossible to identify which compound causes a side effect.
Mistake 2: Expecting peptides to replace TRT. If your testosterone is below 300 ng/dL with symptoms, kisspeptin and CJC-1295 will not fix it. Peptides support optimization in the borderline range. They do not substitute for hormone replacement. Get bloodwork first.
Mistake 3: Injecting ipamorelin after eating. Carbohydrates blunt GH release. Injecting ipamorelin after a meal can reduce the GH pulse by 50% or more. Inject fasted, at least 2 hours after your last meal.
Mistake 4: Skipping reconstitution math. A dosing error with semaglutide can mean taking 5 mg instead of 2.5 mg, with severe nausea as the consequence. Use the peptide dosage chart and the reconstitution calculator to verify every draw.
Safety Considerations
Get bloodwork first. Baseline labs (total testosterone, free testosterone, IGF-1, CBC, metabolic panel) before starting any protocol. A man with clinical hypogonadism needs TRT, not kisspeptin. Peptides are tools for optimization, not treatments for deficiency.
Pro-angiogenic peptides and cancer risk. BPC-157 and CJC-1295 promote blood vessel growth. If you have any cancer history, discuss peptide use with your oncologist before starting. See the peptide safety guide for a full risk breakdown.
GH secretagogues and blood sugar. Growth hormone raises fasting glucose. Men with diabetes or insulin resistance should monitor blood glucose closely and consult an endocrinologist before using CJC-1295 or ipamorelin.
Source quality matters. Research peptides are unregulated. Demand third-party certificates of analysis showing >98% purity and endotoxin testing. For safe handling, see how to store peptides.
Frequently Asked Questions
What is the best peptide for men over 40?
CJC-1295 + ipamorelin is the most versatile starting point. Inject 100-200 mcg CJC-1295 + 200-300 mcg ipamorelin before bed on an empty stomach. This combination restores GH pulsatility, improving sleep, body composition, and recovery. Expect sleep changes within 1-2 weeks and body composition shifts by week 6-8.
Can peptides replace testosterone replacement therapy?
No. Peptides like kisspeptin and CJC-1295 can support endogenous testosterone in men with borderline levels (400-550 ng/dL), but they cannot substitute for TRT when levels are clinically low (below 300 ng/dL with symptoms). Get bloodwork first.
How quickly does PT-141 work for libido?
PT-141 takes 45-60 minutes after a 1.75 mg subcutaneous injection. It works through the central nervous system, producing desire rather than just blood flow. Effects last 6-12 hours. Nausea occurs in about 40% of users and is usually mild. Limit use to once per 24 hours.
Are peptides legal for men to buy?
In the United States, most peptides are sold as research compounds. Semaglutide requires a prescription. PT-141 (as Vyleesi) is prescription-only. BPC-157 was placed in FDA Category 2 in 2023, restricting pharmacy compounding. Regulatory status varies by country.
What peptide helps with stubborn belly fat?
Semaglutide is the strongest option, with 14.9% mean body weight reduction in clinical trials. For men who cannot access GLP-1 agonists, AOD-9604 at 300 mcg/day targets lipolysis without GH-related side effects. 5-Amino-1MQ (50-100 mg oral) is an emerging alternative with preclinical data.
Can you stack multiple peptides safely?
Yes, but introduce one peptide or stack at a time, waiting 2-3 weeks before adding another. CJC-1295 + ipamorelin counts as one stack. Adding BPC-157 for an injury is a reasonable second step. Use the peptide stack calculator to plan combinations and check interactions.
Do peptides cause hair loss in men?
No common peptide on this list causes hair loss. GH secretagogues do not affect DHT levels. GHK-Cu actively supports hair follicle health by strengthening scalp collagen. If you experience shedding on a peptide protocol, evaluate other variables (stress, diet, medications) before attributing it to the peptide.
How much do peptides for men cost per month?
CJC-1295 + ipamorelin costs $80-150/month. BPC-157 adds $60-100/month. PT-141 runs $50-80/month at 2-3 uses per week. Prescription semaglutide costs $300-1,300/month depending on insurance; compounded versions run $150-400/month. Use the Peptide Cost Calculator for estimates.
The Bottom Line
The right peptide depends on the goal. CJC-1295 + ipamorelin for muscle and recovery. Semaglutide for fat loss. PT-141 for libido. GHK-Cu for hair. Epitalon and MOTS-c for the long game.
Start with one goal, one peptide or stack, and baseline bloodwork. Add compounds only after you understand how the first one affects you. The men who get the best results match the right molecule to the right problem and give it 8-12 weeks.
Plan your protocol with the peptide stack calculator and the CJC-1295 + ipamorelin calculator. For safe handling, see how to store peptides. For a complete starting guide, see getting started with peptides.
Helpful Tools
Related Articles
Peptides for Bodybuilding (2026)
Best peptides for bodybuilding: BPC-157, TB-500, MK-677, CJC-1295/Ipamorelin, HGH Fragment 176-191. Dosages and stacking protocols.
5 Best Peptides for Libido (2026)
5 best peptides for libido ranked: PT-141 (FDA-approved), kisspeptin (56% increase), melanotan II, oxytocin, gonadorelin. Dosages for men and women.
PT-141 Peptide: What It Is and How It Works
PT-141 peptide (bremelanotide) explained: MC4R mechanism in the brain, FDA approval as Vyleesi for HSDD, real benefits, RECONNECT trial data, and safety limits.
CJC-1295 Dosage: Complete Protocol Guide
CJC-1295 dosage guide: DAC and no-DAC protocols. Dosing by goal (anti-aging, fat loss, muscle, sleep), ipamorelin stacking, and injection timing.