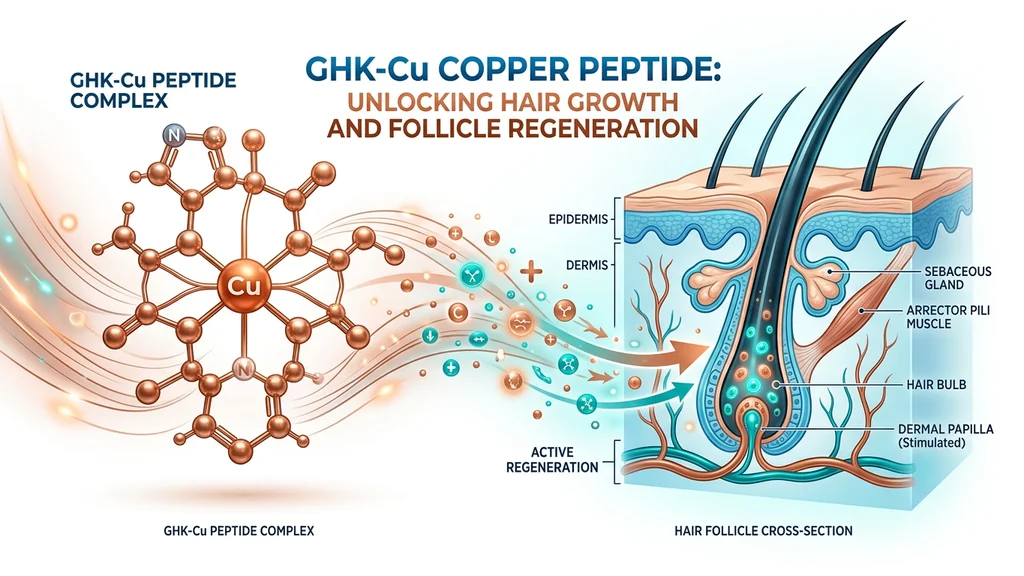
You are watching more hair collect in the shower drain each week, and the standard treatments (finasteride, minoxidil) either scare you with side effects or stopped working months ago. GHK-Cu (glycyl-L-histidyl-L-lysine copper) is a naturally occurring tripeptide that reactivates miniaturized hair follicles through Wnt/beta-catenin signaling, the master switch for hair cycling (Pickart & Margolina, 2018).
The clinical numbers: a 2025 trial using copper peptides with microneedling measured 26.5% hair regrowth across 5 monthly sessions (Kuceki et al., 2025). A 2007 Seoul National University study showed GHK-Cu stimulated follicle elongation and dermal papilla cell proliferation at concentrations as low as 10^-12 M (Pyo et al., 2007).
GHK-Cu is not FDA-approved for hair loss. No copper peptide product has regulatory approval for androgenetic alopecia. Consult a healthcare provider before starting any peptide protocol.
For the full GHK-Cu research profile and injectable dosing, see our GHK-Cu injection dosage guide. To calculate reconstitution volumes, use the Peptide Reconstitution Calculator.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
Quick Reference: GHK-Cu Hair Growth at a Glance
| Factor | Detail |
|---|---|
| What it is | Naturally occurring copper-binding tripeptide (GHK + Cu2+) |
| Primary mechanism | Wnt/beta-catenin pathway activation, triggering telogen-to-anagen transition |
| Secondary mechanisms | TGF-beta1 suppression, VEGF upregulation, dermal papilla cell survival |
| Best clinical result | 26.5% regrowth over 5 months (microneedling combo, Kuceki et al., 2025) |
| Topical-only result | 7% hair count increase at 16 weeks (Japanese trial, 0.02% concentration) |
| FDA-approved for hair? | No |
| Delivery methods | Topical serum, microneedling-assisted, subcutaneous injection |
| Time to first signs | 2 to 4 weeks (reduced shedding) |
| Time to visible density | 16 to 24 weeks |
| Key caution | Overuse causes "copper uglies" (collagen degradation from MMP overexpression) |
How GHK-Cu Promotes Hair Growth: Four Mechanisms
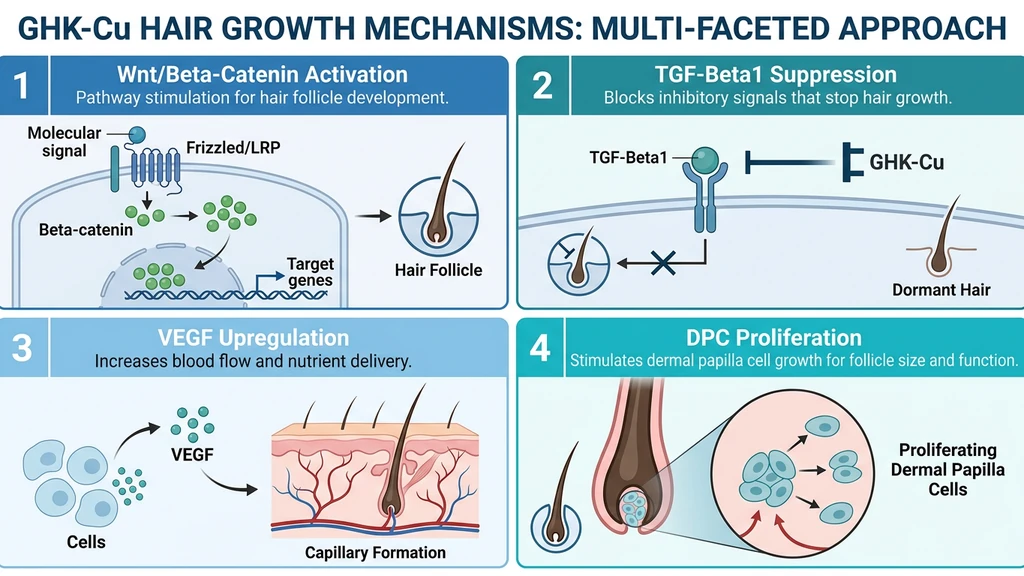
Think of a hair follicle like a furnace with four systems: an ignition switch (Wnt signaling), a thermostat that can shut it down (TGF-beta1), a fuel line (blood supply via VEGF), and a pilot light (dermal papilla cells). Pattern hair loss breaks all four. GHK-Cu repairs each one through a different molecular pathway.
That is the analogy. Here is the literal biology: GHK-Cu activates Wnt/beta-catenin signaling to restart dormant follicles, suppresses TGF-beta1 to prevent premature regression, stimulates VEGF for perifollicular blood supply, and protects dermal papilla cells from programmed death (Pickart & Margolina, 2018).
1. Wnt/Beta-Catenin Pathway Activation
The Wnt/beta-catenin pathway controls whether a follicle grows or stays dormant. When beta-catenin accumulates in dermal papilla cell nuclei, it triggers the transition from telogen (resting) to anagen (active growth). Block that signal, and follicles remain asleep (Lien et al., 2014).
In pattern hair loss, DHT drives dermal papilla cells to secrete DKK1 (Dickkopf-1), a protein that shuts down Wnt signaling. Each hair cycle produces a thinner, shorter strand until the follicle miniaturizes completely.
GHK-Cu upregulates components of the Wnt/beta-catenin pathway, promoting beta-catenin nuclear accumulation. This restores the anagen trigger that DHT-induced DKK1 suppresses (Pickart et al., 2015). A 2022 study confirmed that compounds restoring follicular beta-catenin signaling produce measurable regrowth in androgenetic alopecia models (PMC 9693075).
2. TGF-Beta1 Suppression
TGF-beta1 is one of the primary executioners in pattern hair loss. Inui et al. at Osaka University showed that androgen-stimulated dermal papilla cells from balding scalps produce TGF-beta1, which inhibits keratinocyte growth by roughly 50% (Inui et al., 2002). This cytokine forces the follicle from anagen into catagen (regression), shortening the growth window.
The Pyo et al. (2007) study measured the countereffect directly. Copper-peptide-treated dermal fibroblasts showed decreased TGF-beta1 secretion. The Bcl-2/Bax ratio increased and cleaved caspase-3 levels dropped, indicating reduced apoptosis (Pyo et al., 2007).
GHK-Cu tackles TGF-beta1 from two directions: it reduces production of the "stop growing" signal and protects the cells receiving that signal from programmed death. Finasteride reduces DHT upstream. GHK-Cu blocks TGF-beta1 downstream. The two are complementary.
3. VEGF Upregulation and Angiogenesis
Miniaturizing follicles lose their blood supply. Perifollicular capillaries regress as the follicle shrinks, starving remaining cells of oxygen and nutrients.
GHK-Cu stimulates fibroblasts to produce vascular endothelial growth factor (VEGF), the primary signal for new blood vessel formation. Minoxidil also upregulates VEGF, but through a different pathway: potassium channel opening and prolyl hydroxylase inhibition (Lachgar et al., 1998). GHK-Cu drives VEGF through direct fibroblast stimulation and copper-dependent enzymatic activity.
The copper(II) ion in GHK-Cu is a cofactor for lysyl oxidase (LOX), the enzyme responsible for collagen and elastin cross-linking in blood vessel walls. GHK-Cu delivers both the growth signal (VEGF) and the structural building material (copper for LOX) that new perifollicular vessels require (Pickart & Margolina, 2018).
4. Dermal Papilla Cell Proliferation and Anti-Apoptosis
Dermal papilla cells (DPCs) are the signaling hub of the hair follicle. They instruct the follicle to grow, cycle, and produce pigmented hair. When DPCs die or become senescent, the follicle follows.
Pyo et al. (2007) showed that copper-tripeptide complex at 10^-12 to 10^-9 M stimulated both follicle elongation and DPC proliferation in human tissue. Elevated Bcl-2/Bax ratios and reduced cleaved PARP confirmed the anti-apoptotic effect (Pyo et al., 2007).
GHK-Cu also modulates superoxide dismutase (SOD), the antioxidant enzyme that shields follicle stem cells from oxidative damage. Chronic oxidative stress in balding scalps accelerates DPC senescence. Increased SOD activity extends the functional lifespan of cells that drive follicle cycling (Pickart & Margolina, 2018).
| Mechanism | What GHK-Cu Does | Result for Hair |
|---|---|---|
| Wnt/beta-catenin | Upregulates beta-catenin, counteracts DKK1 | Triggers telogen-to-anagen transition |
| TGF-beta1 | Reduces TGF-beta1 secretion from fibroblasts | Prevents premature catagen entry |
| VEGF | Stimulates VEGF production, supplies copper for LOX | Restores perifollicular blood supply |
| DPC survival | Elevates Bcl-2/Bax ratio, reduces caspase-3 | Keeps dermal papilla cells alive and functional |
Delivery Methods: Topical vs Injectable vs Microneedling
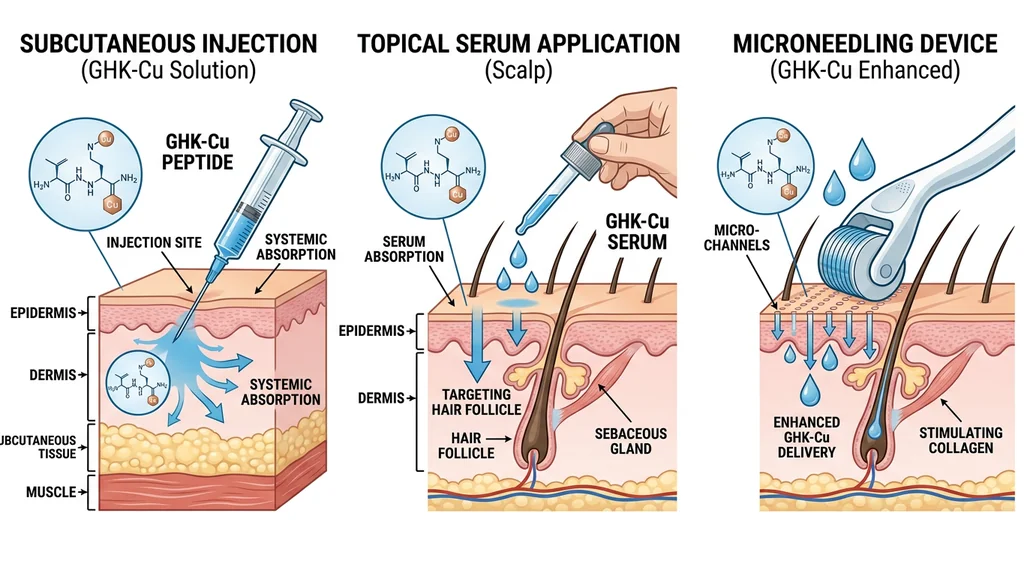
The delivery method determines how much GHK-Cu reaches the dermal papilla, which sits 3 to 4 mm below the scalp surface. Penetration to follicle depth is the rate-limiting factor for every protocol.
Topical Application (Serum or Solution)
Topical GHK-Cu serums typically contain 0.5% to 2% concentration in a hyaluronic acid or liposomal base. You apply directly to thinning areas once daily.
The limitation is penetration. GHK-Cu cannot cross intact stratum corneum effectively. A 2015 permeation study confirmed near-zero transdermal delivery through untreated skin (Li et al., 2015). The peptide reaches the epidermis and superficial dermis but struggles to reach follicle depth.
Nanoliposomal formulations improve delivery. A 2022 study co-encapsulated GHK-Cu with acetyl tetrapeptide-3 and myristoyl pentapeptide-4 in nanoliposomes. In vivo tests on C57BL/6 mice showed superior hair growth compared to free peptides, likely from enhanced dermal penetration (Tian et al., 2022).
| Parameter | Detail |
|---|---|
| Concentration | 1% to 2% GHK-Cu |
| Frequency | Once daily (evening) |
| Application | 6 to 8 drops on thinning areas, massage 2 minutes |
| Duration | Minimum 12 to 16 weeks for visible results |
| Best for | Diffuse thinning, early-stage loss, maintenance |
| Limitation | Poor penetration to follicle depth without enhancement |
A 2025 Japanese trial using 0.02% peptide lotion as standalone treatment observed a 7% increase in hair count after 16 weeks. The concentration was 50 to 100 times lower than standard GHK-Cu serums (0.02% vs 1 to 2%), which likely explains the modest outcome.
Subcutaneous Injection
Injectable GHK-Cu bypasses the skin barrier entirely. Subcutaneous injection delivers the peptide to the dermal and subdermal layers where follicles reside. Tissue concentrations reach 10 to 20 times the levels achieved by serums.
The standard protocol uses 2 to 3 mg GHK-Cu subcutaneously, five days per week, for 8 to 12 weeks. Some practitioners inject directly into the scalp (mesotherapy). Others use abdominal or deltoid sites for systemic delivery. See the GHK-Cu injection dosage guide for reconstitution and site rotation.
| Parameter | Detail |
|---|---|
| Dose | 2 to 3 mg per day |
| Route | Subcutaneous (scalp mesotherapy or abdominal) |
| Frequency | 5 days on, 2 days off |
| Cycle | 8 to 12 weeks on, 4 weeks off |
| Best for | Moderate to advanced thinning, treatment-resistant cases |
| Limitation | Requires reconstitution, injection technique, and medical guidance |
As of 2026, injectable GHK-Cu is classified as Category 2 by the FDA, restricting it from 503A compounding pharmacies. Access requires a prescription from a 503B outsourcing facility or a research-use context. See the GHK-Cu injection frequency guide for scheduling details.
Microneedling-Assisted Delivery
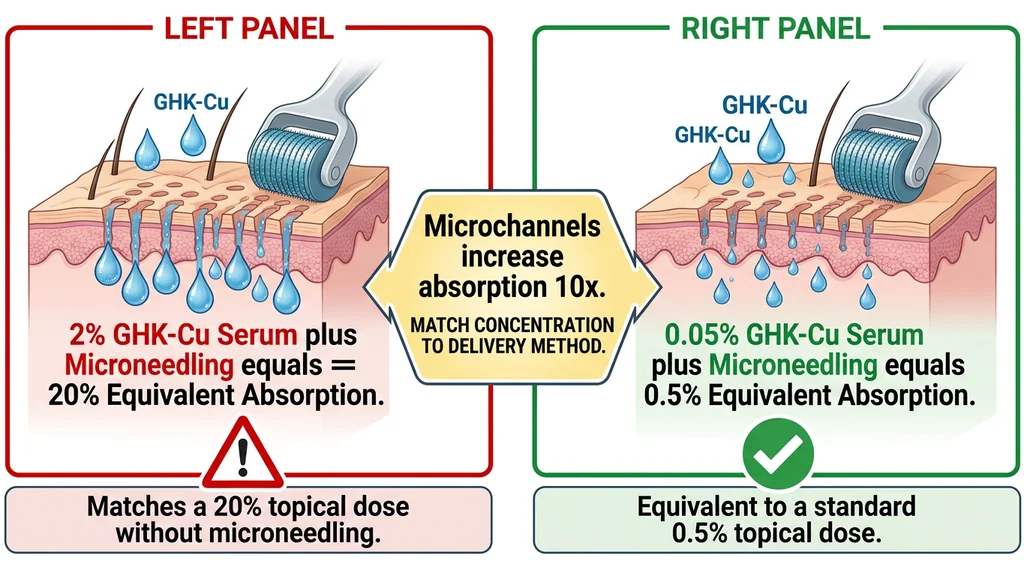
Microneedling solves the penetration problem of topical application. Temporary microchannels in the scalp increase GHK-Cu absorption by up to 10-fold.
Li et al. (2015) quantified the difference: 134 nmol of GHK peptide and 705 nmol of copper permeated through microneedle-treated skin over 9 hours. Through intact skin, permeation was near zero (Li et al., 2015).
The strongest clinical evidence for GHK-Cu hair regrowth comes from this delivery method. Kuceki et al. (2025) used 0.5 to 1.0 mm needle depth, monthly sessions, and a topical mixture of copper peptides with minoxidil 5% and dutasteride 0.25%. After 5 sessions: 26.5% median hair regrowth, 93% shedding reduction, zero adverse events (Kuceki et al., 2025).
| Parameter | Detail |
|---|---|
| Needle depth | 0.5 to 1.0 mm |
| Device | Dermapen preferred (reaches scalp through hair) |
| GHK-Cu concentration | 0.05% post-needling (10x absorption through channels) |
| Frequency | Monthly (every 4 weeks) |
| Minimum sessions | 5 sessions for measurable density change |
| Best for | All stages of androgenetic alopecia |
| Limitation | Monthly commitment, mild discomfort, professional depth preferred at 1.0 mm |
For the full procedure and needle depth selection, see our GHK-Cu microneedling guide.
What Happens When Delivery Goes Wrong: Two Danger Scenarios
Scenario 1: Full-strength serum after microneedling.
You finish a 1.0 mm dermapen session and apply your regular 2% GHK-Cu serum directly to the treated scalp. The microchannels increase absorption by 10-fold. Your skin absorbs the equivalent of 20% concentration. Within 48 hours, the treated area develops persistent redness, inflammatory papules, and increased sensitivity. You have triggered the copper uglies: MMP overexpression from copper overload that degrades collagen instead of building it. The fix: use 0.05% concentration (not 2%) after microneedling. Match the serum strength to the delivery method.
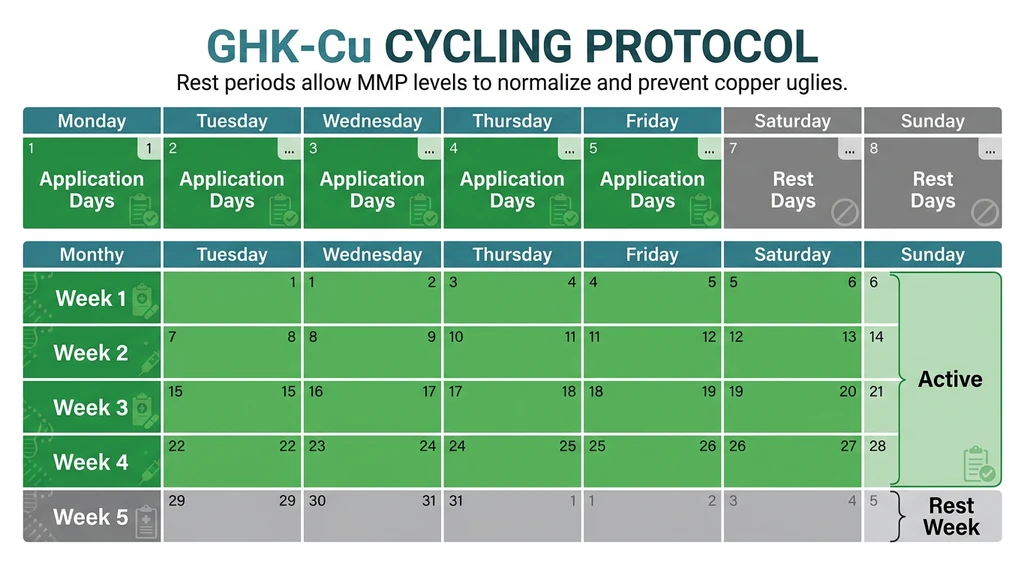
Scenario 2: Daily topical at 2% without cycling.
You apply 2% GHK-Cu serum to your scalp every day for 8 weeks straight, never taking a break. By week 5, your scalp is red and irritated. By week 7, hair shedding has increased rather than decreased. Chronic copper peptide exposure without rest periods upregulates MMPs past the remodeling threshold. The enzymes that should support healthy turnover begin destroying the extracellular matrix around your follicles. The fix: cycle 5 days on, 2 days off, or 4 weeks on, 1 week off. The rest period allows MMP levels to normalize.
GHK-Cu vs Minoxidil vs Finasteride: Head-to-Head
| Factor | GHK-Cu | Minoxidil (5%) | Finasteride (1 mg) |
|---|---|---|---|
| Mechanism | Wnt activation, TGF-beta1 suppression, VEGF, DPC survival | Potassium channel opening, vasodilation, VEGF | 5-alpha reductase inhibition, reduces scalp DHT ~60% |
| FDA-approved for hair | No | Yes (topical) | Yes (oral) |
| Route | Topical, injectable, microneedling | Topical or oral | Oral |
| Time to results | 12 to 16 weeks (topical), 8 to 12 weeks (injectable) | 12 to 24 weeks | 12 to 24 weeks |
| Standalone efficacy | 7% hair count increase (topical); 26.5% regrowth (microneedling combo) | 10 to 15% regrowth (meta-analysis average) | 30 to 40% reduction in progression |
| Side effects | Mild scalp irritation; copper uglies with overuse | Scalp irritation, dryness, initial shedding | Decreased libido (1 to 2%), erectile dysfunction (1%) |
|---|---|---|---|
| Alopecia types | Androgenetic, diffuse thinning, post-inflammatory | Androgenetic primarily | Androgenetic only (male) |
| OTC availability | Yes (topical serums) | Yes (topical) | Prescription only |
Finasteride remains the strongest standalone treatment for male androgenetic alopecia because it targets the root cause: DHT. No amount of GHK-Cu replicates a 60% reduction in scalp DHT.
Minoxidil and GHK-Cu share VEGF upregulation but through different pathways (minoxidil via potassium channel/PHD inhibition, GHK-Cu via fibroblast stimulation). Using both provides additive angiogenic signaling. The Kuceki et al. study combined copper peptides with minoxidil for this reason (Kuceki et al., 2025).
GHK-Cu fills gaps that neither drug addresses: TGF-beta1 suppression, Wnt pathway support, collagen cross-linking for follicle structural integrity, and DPC anti-apoptosis. Its side effect profile is milder than both alternatives. The evidence supports GHK-Cu as a complement to finasteride or minoxidil, targeting pathways they miss (Pickart & Margolina, 2018).
Evidence Summary: What the Studies Show
Human clinical trials:
Kuceki et al. (2025): 7 patients with androgenetic alopecia received 5 monthly microneedling sessions with copper peptides, minoxidil 5%, and dutasteride 0.25%. Median hair regrowth was 26.5% (p < 0.001). SALT score dropped from 40% to 7.5%. The 5-session protocol outperformed a previous 3-session protocol (26.5% vs 10%, p = 0.0025). Zero adverse events (Kuceki et al., 2025).
Limitation: small sample (n=7), combination protocol. Individual contributions of copper peptides vs minoxidil vs dutasteride vs microneedling cannot be isolated.
A 2025 Japanese trial tested 0.02% peptide lotion as standalone topical treatment: 7% increase in hair count after 16 weeks. The concentration was far below standard GHK-Cu serums (0.02% vs 1 to 2%).
In vitro and ex vivo studies:
Pyo et al. (2007) remains the foundational study. AHK-Cu (a copper-binding tripeptide closely related to GHK-Cu) at 10^-12 to 10^-9 M stimulated human hair follicle elongation ex vivo and DPC proliferation in vitro. TGF-beta1 secretion decreased. Bcl-2/Bax ratio increased. Caspase-3 and PARP cleavage decreased (Pyo et al., 2007).
Animal models:
Nanoliposome-encapsulated GHK-Cu showed accelerated hair growth in C57BL/6 mice with visibly earlier anagen onset compared to free peptide controls (Tian et al., 2022).
Gene expression data:
Pickart, Vasquez-Soltero, and Margolina (2015) used Broad Institute Connectivity Map data to show that GHK modulates over 4,000 human genes. Among these, GHK upregulated 47 DNA repair genes and modulated pathways relevant to follicle stem cell maintenance (Pickart et al., 2015).
The gap in the evidence:
No large-scale randomized controlled trial has tested GHK-Cu as a standalone treatment for androgenetic alopecia. The Kuceki study used a combination protocol. The Pyo study was in vitro. The gene expression data is computational. The evidence is mechanistically consistent and promising, but has not reached the level required for FDA approval or clinical guideline inclusion.
GHK-Cu Hair Growth Protocols by Severity
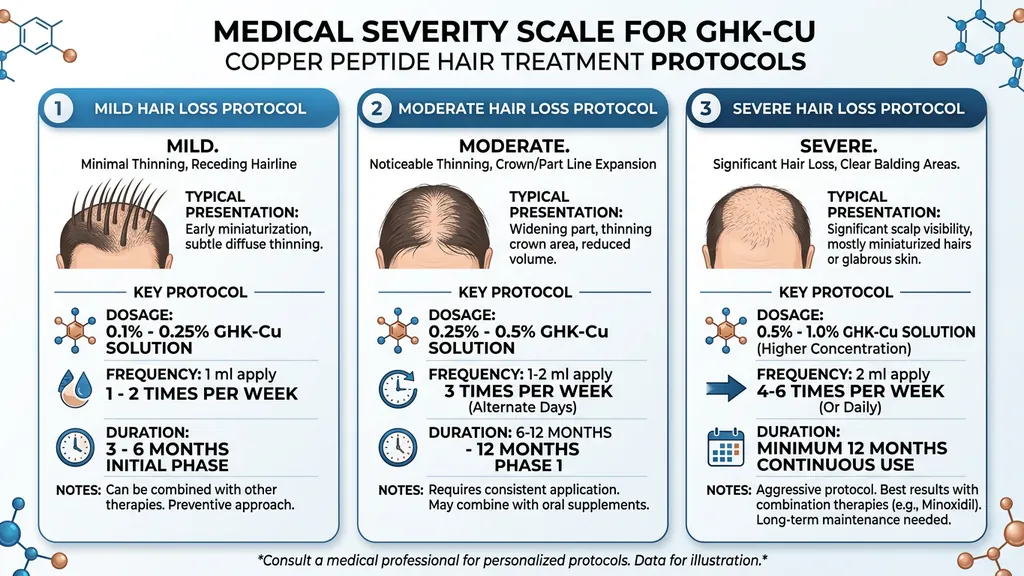
Protocol selection depends on severity of loss, willingness to use injections or microneedling, and whether you already take finasteride or minoxidil. None of these are FDA-approved treatment regimens.
Early-Stage Thinning (Norwood 2-3 / Ludwig 1)
Most follicles are still active at this stage. The goal is to extend anagen duration and reverse early miniaturization.
Step-by-step protocol:
- 1.Clean the scalp. Wash with a gentle sulfate-free shampoo. Pat dry.
- 2.Apply GHK-Cu serum (1% to 2%). Dispense 6 to 8 drops onto thinning areas.
- 3.Massage for 2 minutes. Use fingertip pressure in small circles to improve absorption.
- 4.Leave on overnight. Apply in the evening. Do not rinse.
- 5.Cycle. 5 days on, 2 days off. Continue for 16 to 24 weeks minimum before assessing results.
- 6.Optional monthly boost. Add one microneedling session at 0.5 mm depth with 0.05% GHK-Cu serum post-needling.
Expected timeline:
| Timeframe | What to Expect |
|---|---|
| Weeks 4 to 8 | Reduced shedding (first sign of response) |
| Weeks 8 to 12 | Fine vellus hairs visible in thinning zones |
| Weeks 16 to 24 | Measurable density improvement if responding |
This protocol suits people who prefer a non-invasive, low-commitment approach. Topical GHK-Cu alone is unlikely to produce dramatic regrowth in advanced cases, but for early thinning it can slow progression and support follicle health.
Moderate Thinning (Norwood 3-4 / Ludwig 2)
Significant miniaturization with visible scalp. Topical GHK-Cu alone is unlikely to produce sufficient results. Enhanced delivery is needed.
Protocol A (Microneedling combo, based on Kuceki et al.):
- 1.Microneedling session. Dermapen at 0.5 to 1.0 mm depth across thinning areas, monthly.
- 2.Apply 0.05% GHK-Cu serum immediately after needling.
- 3.Wait 12 to 24 hours, then apply minoxidil 5%.
- 4.Between sessions: daily topical GHK-Cu 1% serum (5 days on, 2 off).
- 5.Minimum commitment: 5 monthly sessions.
Protocol B (Injectable + topical):
- 1.Inject GHK-Cu 2 mg subcutaneously, 5 days per week.
- 2.Apply topical GHK-Cu 1% on non-injection days.
- 3.Cycle: 8 to 12 weeks on, 4 weeks off.
- 4.Combine with finasteride 1 mg daily if no contraindications (physician-supervised).
Expected timeline (Protocol A):
| Timeframe | What to Expect |
|---|---|
| Month 1 to 2 | Reduced shedding, improved scalp condition |
| Month 3 to 4 | Visible vellus hair growth, early density improvement |
| Month 5 to 6 | 15 to 25% hair count increase (based on Kuceki et al. data) |
For reconstitution and site rotation, see the GHK-Cu injection dosage guide. For microneedling procedures, see the GHK-Cu microneedling guide.
Advanced Loss (Norwood 5+ / Ludwig 3)
Extensive follicle miniaturization and dormancy. Many follicles may be beyond recovery. GHK-Cu still contributes, but calibrate expectations.
Maximum intervention protocol:
- 1.Finasteride 1 mg daily or dutasteride 0.5 mg daily (prescription, addresses DHT upstream).
- 2.Monthly microneedling at 1.0 mm with 0.05% GHK-Cu + minoxidil (Kuceki protocol).
- 3.GHK-Cu 2 to 3 mg subcutaneous injection, 5 days per week, 12-week cycles.
- 4.Daily topical minoxidil 5% on non-needling days.
- 5.Optional: GHK-Cu nasal spray 200 mcg twice daily as a systemic supplement.
The achievable regrowth ceiling is lower with advanced loss. Some follicles have been dormant too long for reactivation. The goal shifts to maximizing salvageable follicles and preventing further loss. GHK-Cu's DPC survival and anti-apoptotic effects preserve the remaining functional follicle population (Pyo et al., 2007).
When to consider transplantation: Areas with complete follicle loss will not respond to any topical, injectable, or microneedling protocol. Hair transplantation is the appropriate intervention for those zones. GHK-Cu protocols can support transplanted follicle survival post-procedure, though clinical data on this application remains limited.
Results Timeline: What to Expect Week by Week
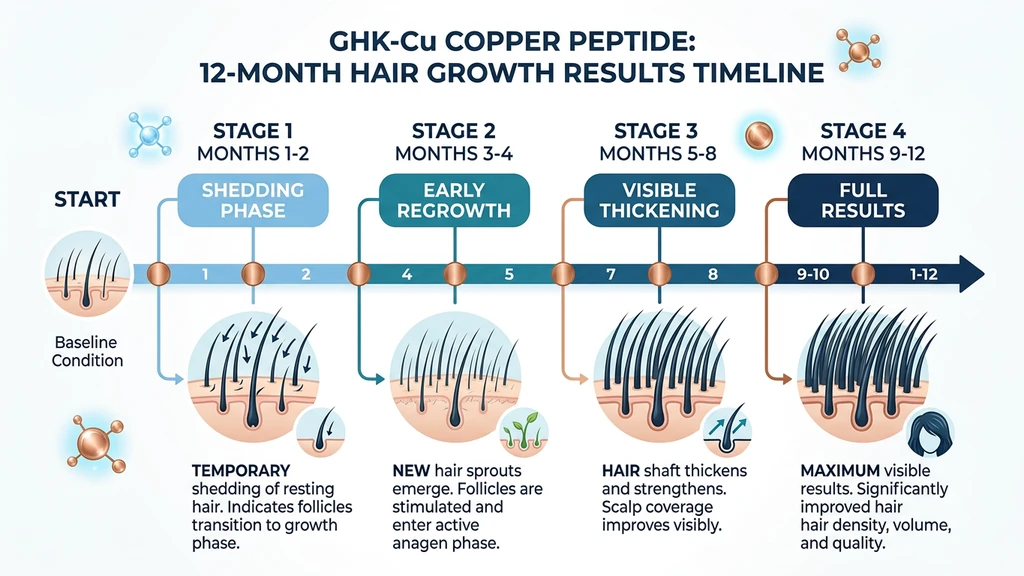
Hair follicles operate on biological timescales. No treatment produces overnight results. GHK-Cu shifts the follicle environment over weeks to months, and the visible changes follow a predictable sequence.
| Phase | Timeframe | What Happens |
|---|---|---|
| Foundation | Weeks 1 to 4 | Gene expression modulation begins. Reduced shedding is the first signal. Fewer hairs on pillow, in shower drain, on brush. Scalp condition improves (less dryness, reduced flaking) from anti-inflammatory effects. |
| Early response | Weeks 4 to 8 | TGF-beta1 suppression and VEGF upregulation lengthen anagen phases. Fine vellus hairs (thin, light-colored) become visible in thinning areas, particularly along the hairline and temples. |
| Growth acceleration | Weeks 8 to 16 | Vellus hairs begin converting to terminal hairs (thicker, pigmented). This is Wnt/beta-catenin signaling driving follicle maturation. Hair density measurements show quantifiable improvement. |
| Visible density | Weeks 16 to 24 | Cumulative effects from multiple follicle cycles produce noticeable improvement. Kuceki et al. measured 26.5% regrowth at 5 months. Topical-only users see more modest gains (7% at 16 weeks). |
| Maintenance | Month 6+ | Growth continues as long as the protocol continues. Stopping GHK-Cu returns the follicle environment to pre-treatment state over several months. Reduced-frequency maintenance can sustain results. |
Signs to reassess your protocol: If shedding has not decreased by week 8 and no vellus hairs are visible by week 16, consider escalating. Switch from topical-only to microneedling-assisted delivery. Add finasteride if you have not already. Some non-responders to topical GHK-Cu respond to injectable delivery because of the 10 to 20x bioavailability difference.
Common Mistakes with GHK-Cu for Hair
Mistake 1: Using 2% serum directly after microneedling.
Open microchannels increase absorption 10-fold. A 2% serum through needled skin delivers the equivalent of 20% on intact skin. The consequence: MMP overexpression, persistent inflammation, paradoxical hair shedding. Use 0.05% after microneedling, full-strength only on intact skin.
Mistake 2: Applying GHK-Cu daily without cycling.
Continuous copper peptide exposure for 6+ weeks without rest periods upregulates MMPs beyond the healthy remodeling threshold. Users report worsening redness and increased shedding by week 5 to 6. Cycle 5 days on, 2 days off, or 4 weeks on, 1 week off.
Mistake 3: Applying vitamin C serum at the same time.
L-ascorbic acid (vitamin C) oxidizes the copper(II) ion in GHK-Cu, neutralizing both actives. You lose the copper peptide benefit and the antioxidant benefit in one application. Separate them by 12 hours or use on alternate days.
Mistake 4: Expecting results in 4 weeks and quitting.
The follicle cycling timeline is biological, and biology cannot be rushed. Visible density change requires 16 to 24 weeks. Reduced shedding (weeks 2 to 4) is the first signal that the protocol is working. Quitting at week 4 because you do not see new hair means abandoning the protocol before it could possibly produce visible growth.
Safety, Side Effects, and the Copper Uglies
GHK-Cu has a favorable safety profile compared to minoxidil and finasteride. No hormonal effects. No cardiovascular concerns. No systemic copper toxicity at standard doses (Pickart & Margolina, 2018).
Topical side effects: - Mild scalp redness or irritation (5 to 10% of users), typically resolves within days - Temporary shedding increase during the first 2 weeks (adjustment phase) - Contact dermatitis in rare cases, usually from other ingredients in the serum formulation
Injectable side effects: - Injection site redness or swelling (resolves within hours) - Mild headache in the first week of use (uncommon) - See the GHK-Cu injection dosage guide for full safety data
The copper uglies explained:
This is the most important side effect to understand. It occurs when GHK-Cu is overused, typically from daily high-concentration topical application without cycling. Chronic copper peptide exposure upregulates matrix metalloproteinases (MMPs), enzymes that break down collagen and extracellular matrix. In controlled doses, MMPs support healthy tissue remodeling. With chronic overexposure, they cause tissue degradation.
Symptoms: persistent redness, new breakouts, increased sensitivity, skin that worsens rather than improves over time. The paradox is that overusing a pro-collagen peptide destroys collagen through MMP overexpression.
Prevention: Cycle your use. Topical: 5 days on, 2 days off, or 4 weeks on, 1 week off. Post-microneedling: the monthly session schedule naturally provides recovery time. Do not apply serum above 1% daily without cycling. For a full troubleshooting guide, see our copper peptides irritation guide.
Pregnancy and nursing: No safety data exists. Avoid GHK-Cu during pregnancy and breastfeeding.
Frequently Asked Questions
Does GHK-Cu regrow hair or only slow loss?
Both. The Kuceki et al. (2025) microneedling study measured 26.5% new hair regrowth over 5 months using copper peptides, minoxidil, and dutasteride. Topical GHK-Cu alone produced 7% increase in hair count at 16 weeks in a Japanese trial. GHK-Cu activates Wnt/beta-catenin (triggering new growth) and suppresses TGF-beta1 (slowing loss). The degree of regrowth depends on how many follicles remain salvageable and which delivery method you use.
How long before GHK-Cu shows results for hair?
Reduced shedding appears within 2 to 4 weeks. Fine vellus hairs in thinning areas become visible at 6 to 12 weeks. Measurable density improvement requires 16 to 24 weeks. The Kuceki et al. clinical trial measured 26.5% regrowth at 5 months. Injectable and microneedling-assisted delivery produce earlier visible results than topical-only protocols due to 10 to 20x higher bioavailability at follicle depth.
Can I combine GHK-Cu with minoxidil and finasteride?
Yes. All three work through different pathways. Finasteride reduces DHT (root cause). Minoxidil opens potassium channels and increases VEGF. GHK-Cu adds Wnt activation, TGF-beta1 suppression, and DPC survival. The Kuceki et al. (2025) study combined copper peptides with minoxidil and dutasteride, confirming the combination is safe and synergistic. One caution: do not apply minoxidil on freshly microneedled skin. Wait 12 to 24 hours.
Is topical or injectable GHK-Cu better for hair growth?
Injectable GHK-Cu reaches follicle-depth tissue at 10 to 20 times the concentration of topical serums, making it more effective for moderate-to-advanced loss. Topical application is limited by the stratum corneum barrier, with near-zero penetration through intact skin (Li et al., 2015). Microneedling-assisted delivery bridges the gap. For early-stage thinning, topical may suffice. For anything beyond mild loss, enhanced delivery is needed.
What concentration of GHK-Cu serum should I use on my scalp?
For daily application on intact skin: 1% to 2%. For application after microneedling: 0.05% (500 ppm), because open microchannels increase absorption up to 10-fold. A 0.05% serum through microchannels behaves like 0.5% on intact skin. Using full-strength serum after needling risks the copper uglies: persistent redness, breakouts, and collagen degradation from MMP overexpression. Match concentration to delivery method.
What are the copper uglies and how do I avoid them?
The copper uglies occur when chronic GHK-Cu overuse upregulates matrix metalloproteinases (MMPs) past the healthy remodeling threshold. Symptoms include persistent redness, breakouts, and worsening skin quality. Prevention: cycle 5 days on, 2 days off for topical use. Never apply concentrations above 1% daily without breaks. After microneedling, use 0.05% concentration only.
Does GHK-Cu work for female pattern hair loss?
GHK-Cu targets pathways relevant to both male and female pattern hair loss: Wnt/beta-catenin activation, TGF-beta1 suppression, VEGF upregulation, and DPC survival. The Kuceki et al. (2025) trial included both sexes. For women who cannot take finasteride (contraindicated in pregnancy), GHK-Cu combined with minoxidil and microneedling offers a non-hormonal alternative targeting four follicle pathways simultaneously.
Can I apply GHK-Cu and vitamin C serum together?
No. L-ascorbic acid oxidizes the copper(II) ion in GHK-Cu, neutralizing both actives. You lose the copper peptide benefit and the vitamin C antioxidant benefit in one step. Separate them by 12 hours minimum. Apply GHK-Cu in the evening and vitamin C in the morning, or use them on alternate days.
The Bottom Line
GHK-Cu promotes hair growth through four mechanisms: Wnt/beta-catenin activation, TGF-beta1 suppression, VEGF-driven angiogenesis, and dermal papilla cell survival. The strongest clinical evidence shows 26.5% regrowth over 5 months with microneedling-assisted delivery (Kuceki et al., 2025).
Delivery method determines outcome. Topical serums on intact skin produce modest results (7% at 16 weeks). Microneedling increases absorption 10-fold. Injectable protocols reach 10 to 20x the tissue concentration of topical application. Match your delivery method to your severity: topical for early-stage, microneedling for moderate, injectable plus anti-androgens for advanced.
Cycle your protocol (5 days on, 2 off) to avoid the copper uglies. Commit to 16 to 24 weeks minimum. Measure progress with standardized monthly photos. For reconstitution help, use the Peptide Reconstitution Calculator. For injectable protocols, see the GHK-Cu injection dosage guide. For microneedling steps, see the GHK-Cu microneedling guide. For the full peptide profile, visit the GHK-Cu page.
Helpful Tools
Related Articles
Where to Inject GHK-Cu: Sites by Goal
Where to inject GHK-Cu for skin, hair, wounds, and anti-aging. Subcutaneous site map by goal, rotation patterns, needle depth, and angle guidance.
GHK-Cu Microneedling: Depths & Results
GHK-Cu microneedling protocol with needle depths by goal, step-by-step instructions, the copper uglies warning, and results timeline.
How to Reconstitute GHK-Cu: Guide
How to reconstitute GHK-Cu step by step for 50mg and 100mg vials. Concentration table, bacteriostatic water volumes, syringe units, and storage instructions.
Peptides for Healing: What the Evidence Shows
Peptides for healing by tissue: tendon, bone, wound, gut, post-surgery. Which claims rest on human trials, which rest on rat studies, and what is unsafe.