You ordered both BPC-157 and TB-500, and now you are searching for what the combination might do to your body before loading the first syringe. The BPC-157 and TB-500 stack (the "Wolverine stack") is generally well-tolerated based on available evidence. Reported side effects include mild headaches, fatigue, bloating, and injection site reactions during the first 1-2 weeks. Most side effects are transient and resolve without intervention. The primary safety concerns are theoretical: both peptides promote angiogenesis, raising questions about use in individuals with undiagnosed cancers, and TB-500 has rare reports of hypersensitivity reactions including anaphylaxis. No human clinical trials have studied this specific combination.
| Quick Reference | Details |
|---|---|
| Common side effects | Headaches, fatigue, mild bloating, injection site soreness |
| Onset | Week 1-2 of protocol |
| Resolution | Most resolve by week 3-4 |
| Serious concerns | Pro-angiogenic effects (both peptides), TB-500 hypersensitivity (rare) |
| Cancer screening | Recommended before starting (both promote blood vessel growth) |
| FDA status | Neither approved for human use; BPC-157 on category 2 risk list |
| Typical stack dose | BPC-157 250-500 mcg + TB-500 2-5 mg, 2x/week |
BPC-157 is not FDA-approved for any indication. No completed human clinical trial exists for this combination. Consult a healthcare provider before use.
The "Wolverine stack" name reflects the combination's reputation for accelerated tissue repair. That healing power comes with specific safety considerations worth understanding before your first injection. For dosing protocols, see our BPC-157 dosage calculator.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
BPC-157 Side Effects When Used Alone
BPC-157 has a remarkably clean safety profile in preclinical research. No lethal dose (LD1) has been achieved in animal studies, and a 2025 human pilot found no adverse events at 20 mg intravenously (Safety of IV BPC157, Altern Ther Health Med, 2025). A systematic review of the emerging clinical evidence confirmed this favorable profile (Pickering, Biomedicines, 2025).
User reports paint a consistent picture. The most common side effects fall into predictable categories, and nearly all resolve without intervention.
Common Side Effects (Reported by >10% of Users)
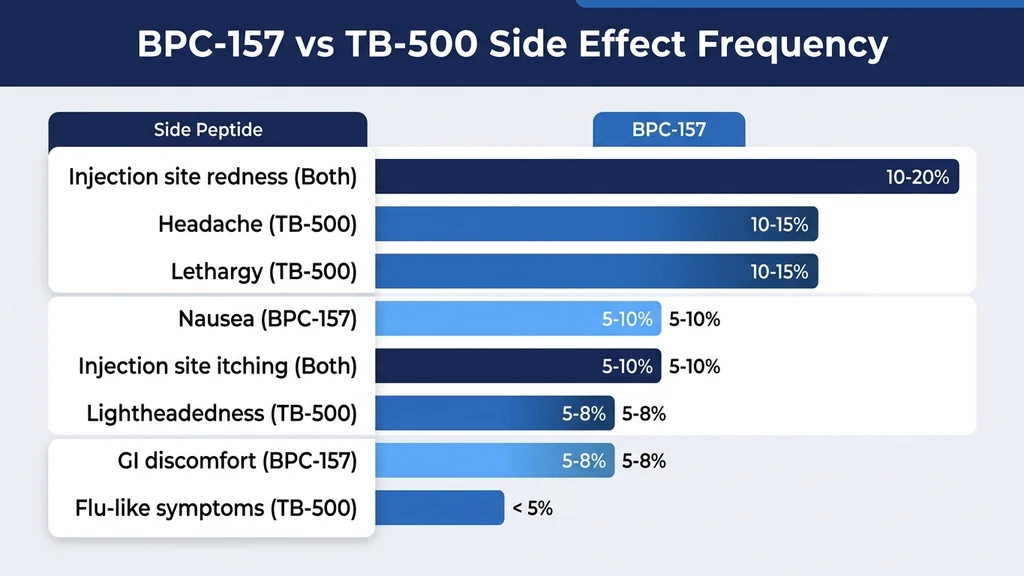
Nausea and mild GI discomfort. This occurs more often with oral BPC-157 than injectable forms, since the peptide contacts the gastrointestinal lining directly. Most users describe it as a brief wave of queasiness within 30-60 minutes of dosing. It typically fades by day 3. For a dedicated guide, see BPC-157 capsule side effects.
Injection site reactions. Redness, slight swelling, and soreness at the injection point affect roughly 10-15% of subcutaneous users. Proper injection technique and site rotation minimize these reactions. See our guide on how to inject BPC-157 for detailed instructions.
Mild fatigue during week 1. The body is allocating resources toward tissue repair. This resembles the tiredness you feel after a deep-tissue massage. It passes as your system adjusts to the peptide.
Uncommon Side Effects (1-10% of Users)
Headaches. BPC-157 increases nitric oxide production and dilates blood vessels through the Src-Caveolin-1-eNOS pathway (Hsieh et al., Sci Rep, 2020). This vasodilation can trigger mild headaches, especially during the first week. Read our detailed breakdown of BPC-157 headaches.
Dizziness and lightheadedness. Related to blood pressure modulation. BPC-157 can lower blood pressure transiently in normotensive individuals. Standing up slowly after injection helps.
Appetite changes. Some users report increased hunger, others decreased appetite. The effect is mild and inconsistent across reports.
Insomnia (with evening dosing). BPC-157 modulates dopamine D2 receptors and serotonin pathways (Sikiric et al., J Physiol Paris, 1999). Evening injections can shift neurotransmitter balance toward wakefulness. The fix: inject before 10 AM.
Rare Side Effects (<1% or Theoretical)
Blood pressure fluctuations and allergic reactions appear in fewer than 1% of user reports. BPC-157 modulates the NO system bidirectionally, meaning it can raise blood pressure in hypotensive states and lower it in hypertensive states (Sikiric et al., Eur J Pharmacol, 1997). True allergic reactions to the peptide itself are extremely rare. Reactions to the carrier solution (bacteriostatic water) are more common.
TB-500 Side Effects When Used Alone
TB-500 (a synthetic fragment of Thymosin Beta-4) has its own safety data. A Phase I clinical trial administered 42 to 1,260 mg of Thymosin Beta-4 over 14 days with no dose-limiting toxicity (Sosne et al., Ann N Y Acad Sci, 2016). The side effect profile differs from BPC-157 in specific ways.
Common TB-500 Side Effects
Fatigue and lethargy. More pronounced than BPC-157 fatigue, TB-500 tiredness often lasts the full first two weeks. Users describe it as feeling "run down" despite adequate sleep. The peptide is directing substantial resources toward tissue remodeling.
Water retention and bloating. TB-500 causes mild fluid retention in many users. Expect 1-3 pounds of temporary water weight during the loading phase. This is the most distinctive TB-500 side effect and the one BPC-157 does not share.
Injection site discomfort. Similar to BPC-157 but sometimes more noticeable because TB-500 injection volumes tend to be larger (reconstituted in 1-2 mL versus 0.5 mL for BPC-157).
Uncommon TB-500 Side Effects
Headaches. TB-500 also promotes vasodilation, though through different pathways than BPC-157. The headache profile is similar: mild, dull, and concentrated in the first week.
Mild nausea. Less frequent than with BPC-157, since TB-500 is rarely taken orally. Subcutaneous injection bypasses the GI tract entirely.
Temporary dizziness. Blood pressure changes during the adjustment phase can cause brief lightheadedness, particularly when standing quickly.
Rare but Serious TB-500 Side Effects
Hypersensitivity reactions, including anaphylaxis. Case reports document rare allergic reactions to TB-500, ranging from skin rash to anaphylaxis. This is the most serious known risk associated with TB-500 specifically. Anyone with a history of severe allergies should have epinephrine available during the first injection. Administer the first dose in a setting where anaphylaxis can be managed.
Heart palpitations. A small number of users report brief episodes of rapid or irregular heartbeat. The mechanism is unclear but may relate to TB-500's effects on cardiac tissue remodeling. Persistent palpitations warrant immediate discontinuation and medical evaluation.
What Changes When You Stack Both Peptides
The central question: does combining BPC-157 and TB-500 create new risks beyond what each peptide carries alone? No published study has tested this exact combination.
Think of it like combining two medications that both lower blood pressure through different pathways. The individual effects are known. The combined effect is predicted to be additive in some areas, neutral in others. The concern is about unexpected synergies.
Additive Effects to Watch
Compounded vasodilation. Both BPC-157 and TB-500 modulate the nitric oxide system and promote blood vessel dilation. BPC-157 works through the Src-Cav-1-eNOS pathway (Hsieh et al., 2020). TB-500 promotes vasodilation through different mechanisms related to actin sequestration and endothelial cell migration. Together, blood vessel dilation may be more pronounced than with either alone, meaning a higher chance of headaches and dizziness during week 1.
Increased fatigue during loading phase. Your body is running two repair programs simultaneously. The energy demand is real. Users stacking both peptides report more noticeable fatigue in the first 7-10 days compared to either peptide solo.
Greater water retention. TB-500 is the primary driver of water retention, but BPC-157's vascular effects may amplify it slightly. Expect 2-4 pounds of water weight during the loading phase when stacking, versus 1-3 pounds with TB-500 alone.
Week-by-Week Side Effect Timeline
This timeline reflects the typical experience reported by users running a standard BPC-157 + TB-500 protocol.
| Week | Expected Side Effects | Severity | Action |
|---|---|---|---|
| 1-2 | Fatigue, headaches, mild bloating, injection site soreness | Mild to moderate | Normal adaptation; continue protocol |
| 3-4 | Most side effects resolving; possible residual water retention | Mild | Continue; headaches should be gone |
| 5-8 | Minimal to none; water retention normalizing | Negligible | Maintenance phase |
| 9-12 | None expected | None | Monitor; consider cycling off |
Most users who tolerate weeks 1-2 without serious reactions complete their full protocol without further issues. The first 10 days are the adjustment window.
Does the Stack Cause More Side Effects Than Either Peptide Alone?
Limited evidence suggests the combination does not produce dramatically worse side effects than individual use. Most users report the same types of reactions they would expect from each peptide separately. The loading phase can feel more intense because two peptides are active simultaneously.
The key distinction: stacking does not appear to create novel side effects that neither peptide produces alone. The risks are additive rather than synergistic. If you tolerate BPC-157 and TB-500 individually, you will likely tolerate the stack.
Serious Safety Considerations for the Stack
Three categories of concern deserve careful attention before starting the BPC-157 and TB-500 combination. These are not common side effects. They are structural risks inherent to the peptides' mechanisms of action.
Cancer and Angiogenesis Concerns
Both BPC-157 and TB-500 promote angiogenesis: the formation of new blood vessels. BPC-157 upregulates VEGF (vascular endothelial growth factor) and activates the VEGFR2 signaling cascade (Sikiric et al., Pharmaceuticals, 2025). TB-500 promotes endothelial cell migration and new vessel formation through its interaction with actin polymerization.
Tumors depend on blood vessel growth to sustain themselves. The theoretical concern: if you have an undiagnosed cancer, pro-angiogenic peptides could accelerate tumor progression. A 2025 narrative review specifically highlighted this as the primary safety question for long-term BPC-157 use (Pickering, Biomedicines, 2025).
No evidence suggests either peptide causes cancer. The concern is limited to potentially promoting the growth of existing, undiagnosed tumors. A comprehensive health screening before starting is a reasonable precaution. This includes age-appropriate cancer screenings (colonoscopy, mammography, PSA testing, skin checks) and baseline bloodwork.
Cardiovascular Considerations
Both peptides affect blood pressure regulation through overlapping but distinct pathways. BPC-157 modulates the NO system, capable of both lowering and raising blood pressure depending on the baseline state (Sikiric et al., 1997). TB-500 promotes vasodilation through endothelial cell effects.
Users on blood pressure medications (ACE inhibitors, ARBs, calcium channel blockers, beta-blockers) should consult their physician before starting either peptide. The additive vasodilatory effect of the stack could compound the blood pressure reduction from medication, leading to symptomatic hypotension.
Monitor your blood pressure daily during the first two weeks. A systolic drop of more than 20 mmHg from baseline or any reading below 90/60 warrants discontinuation and medical evaluation.
Immune System Effects
TB-500 modulates immune function through its role in T-cell maturation (it is derived from Thymosin Beta-4, a thymic peptide). BPC-157 affects inflammatory cytokine expression and immune cell activity at the tissue level (Sikiric et al., Gut Liver, 2020).
The theoretical concern applies to autoimmune conditions. If your immune system is already dysregulated, introducing two immune-modulating peptides simultaneously could shift the balance unpredictably. Users with rheumatoid arthritis, lupus, multiple sclerosis, Hashimoto's thyroiditis, or other autoimmune conditions should discuss this stack with their rheumatologist or immunologist before starting.
Who Should Not Use the BPC-157 TB-500 Stack

Certain populations should avoid this combination entirely. These contraindications apply to both individual peptides and become more relevant when stacking.
Active cancer or cancer history. Both peptides promote angiogenesis. Until research clarifies the actual risk, individuals with active malignancies or a recent cancer history should avoid pro-angiogenic peptides.
Pregnancy or breastfeeding. No reproductive safety data exists for either peptide. The risk to fetal development is unknown and not worth taking.
Under 18 years old. Neither peptide has been studied in adolescents. Growth and development could be affected by compounds that modulate tissue repair and blood vessel formation.
Active infections. Angiogenesis can theoretically help infections spread by providing new blood vessel pathways. Wait until acute infections fully resolve before starting.
Uncontrolled blood pressure. The additive vasodilatory effects of both peptides make this stack inappropriate for anyone whose blood pressure is not well-managed. Get BP under control first.
Anticoagulant therapy. Both peptides affect vascular function. Users on warfarin, heparin, or direct oral anticoagulants should consult their prescriber. The interaction has not been studied, but theoretical overlap exists.
Both peptides are prohibited by WADA. Competitive athletes subject to drug testing cannot use this stack.
How to Minimize Side Effects from the Wolverine Stack
Four strategies reduce the likelihood and severity of side effects when combining BPC-157 and TB-500.
Start with One Peptide First
Begin BPC-157 alone at 250 mcg daily for 5-7 days. Note any reactions. If you tolerate it well, add TB-500 at the lowest recommended dose (typically 2 mg twice weekly). This sequential introduction serves two purposes: it lets you identify which peptide causes any reaction, and it reduces the shock of introducing two bioactive compounds simultaneously.
If you develop headaches or fatigue on BPC-157 alone, you can address those before adding TB-500. If side effects appear only after adding TB-500, you know the source immediately.
Dosing Strategies for Reduced Side Effects
Start low. BPC-157 at 250 mcg (not 500 mcg) and TB-500 at 2 mg (not 5 mg) for the first two weeks.
Inject BPC-157 in the morning. Peak neurotransmitter and vasodilatory effects occur 2-6 hours post-injection. Morning dosing means these peaks happen during daytime hours.
Rotate injection sites. Alternate between abdominal quadrants, thighs, and deltoids. No site should be used more than twice per week.
Stay hydrated. Dehydration amplifies vasodilation headaches and worsens TB-500 water retention. Aim for 2.5-3 liters of water daily during the loading phase.
Maintain electrolyte balance. Sodium, potassium, and magnesium support vascular tone. Magnesium glycinate (200-400 mg before bed) may specifically help with vasodilation headaches.
When to Stop the Stack
Discontinue immediately and seek medical attention if you experience:
- Allergic reaction symptoms: rash, hives, throat tightness, difficulty breathing, swelling of face or tongue
- Chest pain or persistent heart palpitations
- Severe headache (8/10 or higher) that does not respond to hydration and acetaminophen
- Any neurological symptom: visual changes, confusion, numbness, weakness on one side
Discontinue and reassess (but medical emergency is less likely) if you experience:
- Headaches persisting beyond 2 weeks despite morning dosing and hydration
- Fatigue that worsens rather than improves after the first 10 days
- Blood pressure readings consistently below 90/60 or above 160/100
- Any symptom that is getting worse rather than better over time
Injection vs Oral Stack: Side Effect Differences
The route of administration changes the side effect profile significantly. For the oral capsule option, see our guide on BPC-157 TB-500 capsules.
| Side Effect | Injectable Stack | Oral Stack |
|---|---|---|
| Headaches | More common (faster systemic absorption) | Less common (slower absorption curve) |
| GI discomfort | Rare (bypasses gut) | More common (direct gut contact) |
| Diarrhea | Uncommon | Possible with oral BPC-157 |
| Injection site reactions | Yes | None |
| Water retention | Standard | Similar |
| Fatigue | Standard | Similar |
| Onset of side effects | Within hours | Within 1-2 days |
| Bioavailability | Higher (BPC-157 ~100%, TB-500 ~90%) | Lower (BPC-157 ~50-70%, TB-500 variable) |
Injectable forms produce faster-onset, more noticeable side effects because peak blood levels are reached within minutes. Oral forms produce a slower, more gradual absorption curve that spreads the effect over hours. For users sensitive to vasodilation headaches, oral capsules may be the better starting point.
What the Research Shows About Stack Safety
No single study has examined the BPC-157 + TB-500 combination. The safety case is built from individual peptide data.
BPC-157 safety evidence. Over 100 preclinical studies. No LD1 achieved in toxicity studies at any dose tested. A Phase II trial for ulcerative colitis (code: PL14736) showed no significant adverse events. A 2025 human pilot administered 20 mg IV with no reported side effects (Safety of IV BPC157, 2025). The cytoprotection review by Sikiric et al. confirmed no toxicity across decades of animal research (Sikiric et al., Gut Liver, 2020).
TB-500 safety evidence. Phase I trial data from Thymosin Beta-4 studies showed no dose-limiting toxicity across a wide dose range (42-1,260 mg over 14 days) (Sosne et al., 2016). Dermal healing trials in humans confirmed tolerability. The rare anaphylaxis reports come from post-market case reports, not controlled trials.
The gap. Individual safety does not guarantee combination safety. The pharmacological profiles of BPC-157 and TB-500 overlap in their pro-angiogenic and vasodilatory effects, creating the potential for additive responses in those systems. The overall risk profile, based on available evidence, appears low. "Low risk" is not "no risk," and no physician can cite a randomized controlled trial to support this specific combination.
For deeper side effect coverage of each individual peptide, see BPC-157 side effects and our dedicated does BPC-157 cause headaches and can BPC-157 cause diarrhea guides.
Frequently Asked Questions
Is the BPC-157 TB-500 stack safe?
No human clinical trial has tested this specific combination. Individual peptide data suggests a favorable safety profile: BPC-157 showed no adverse events at 20 mg IV in a 2025 pilot, and TB-500 (Thymosin Beta-4) showed no toxicity across 42-1,260 mg in Phase I trials. Most users report only mild, transient side effects during weeks 1-2. The primary theoretical concern is additive pro-angiogenic effects in individuals with undiagnosed cancers.
Can the Wolverine stack cause cancer?
No evidence suggests BPC-157 or TB-500 causes cancer. The concern is that both peptides promote angiogenesis (new blood vessel formation), which could theoretically support existing tumor growth. A 2025 narrative review in Biomedicines raised this as the primary long-term safety question (Pickering, PMC12446177). Cancer screening before starting the stack is a reasonable precaution, particularly for users over 40.
How long do side effects from BPC-157 and TB-500 last?
Most side effects peak during weeks 1-2 and resolve by week 3-4. Headaches typically fade within 5-7 days. Fatigue improves after 10-14 days. Water retention from TB-500 normalizes over 2-3 weeks. If any side effect worsens rather than improves after the first 2 weeks, discontinue the stack and consult a physician.
Should I stop the BPC-157 TB-500 stack if I get headaches?
Mild headaches (3-4/10 on a pain scale) during the first week are a normal response to vasodilation and do not require stopping. Drink 500 mL of water before each dose and consider starting at lower doses (BPC-157 at 250 mcg, TB-500 at 2 mg). Stop only if headaches are severe (8/10 or higher), accompanied by visual changes, or persist beyond 2 weeks. See our BPC-157 headaches guide for detailed management.
Are oral BPC-157 TB-500 capsules safer than injections?
Oral capsules produce fewer vasodilation-related side effects (headaches, dizziness) because absorption is slower and peak blood levels are lower. Oral forms cause more GI side effects (nausea, diarrhea) due to direct gut contact. Neither route is categorically safer. Choose injectable for targeted healing with faster onset. Choose oral if vasodilation side effects concern you. See our capsule guide for details.
Can I take the Wolverine stack with blood pressure medication?
Consult your prescribing physician first. Both BPC-157 and TB-500 affect blood pressure through vasodilation and NO system modulation. Combining them with antihypertensive medications (ACE inhibitors, ARBs, calcium channel blockers) could cause additive blood pressure reduction. Monitor BP daily during the first 2 weeks. A systolic drop exceeding 20 mmHg from baseline warrants medical review.
What is the safest way to start the BPC-157 TB-500 stack?
Start BPC-157 alone at 250 mcg daily for 5-7 days. If tolerated, add TB-500 at 2 mg twice weekly. This sequential approach identifies which peptide causes any reaction. Inject BPC-157 in the morning. Stay hydrated with 2.5-3 liters of water daily. Get baseline bloodwork and age-appropriate cancer screenings before beginning. Use our BPC-157 + TB-500 dosage guide for the full protocol.
Does the Wolverine stack interact with other medications?
No formal drug interaction studies exist for this combination. Theoretical concerns include interactions with anticoagulants (both peptides affect vascular function), blood pressure medications (additive vasodilation), and immunosuppressants (TB-500 modulates immune function). BPC-157 has GABAergic and serotonergic interactions that could theoretically affect sleep medications and antidepressants. Disclose all peptide use to your physician.
The Bottom Line
The BPC-157 and TB-500 stack carries a manageable side effect profile for most users. Headaches, fatigue, and mild bloating during weeks 1-2 represent the typical experience. These resolve as your body adapts to both peptides. The serious considerations center on angiogenesis (get screened before starting), cardiovascular effects (monitor blood pressure), and the rare TB-500 hypersensitivity risk.
Start one peptide at a time. Begin with low doses. Inject BPC-157 in the morning. Stay hydrated. These four steps prevent or reduce the majority of reported side effects. If anything worsens after the first two weeks instead of improving, stop and consult a physician.
Use our BPC-157 dosage calculator to plan your protocol. Check the peptide interaction checker before adding other compounds. For reconstitution guidance, see the peptide reconstitution calculator. For a comparison of BPC-157 and TB-500 individually, see our BPC-157 vs TB-500 guide.
Helpful Tools
Related Articles
Can Tirzepatide Cause Joint Pain? Clinical Data
Can tirzepatide cause joint pain? SURMOUNT arthralgia rates match placebo. Review 5 indirect causes, uric acid risks, and 8 relief tactics.
Peptide Therapy Side Effects: Complete Guide (2026)
Peptide therapy side effects by category: GLP-1, GH-releasing, healing, and immune. Severity matrix, incidence rates, and management strategies.
TB-500 Side Effects: What Research Shows
TB-500 side effects: headache (10-15%), lethargy, nausea, and injection site reactions. Cancer risk evidence, contraindications, and monitoring.
BPC-157 TB-500 Dosage: Combined Protocol
BPC-157 TB-500 dosage: 250-500 mcg BPC-157 + 2-2.5 mg TB-500 daily. Weight-adjusted charts, injury-type matrix, blend vial math, and cycle timing.