> YMYL Disclaimer: BPC-157 is not FDA-approved for any medical use. No completed human clinical trial has confirmed its safety or efficacy in headache management or any other indication. This article is for educational purposes only. Consult a licensed physician before beginning any peptide protocol.
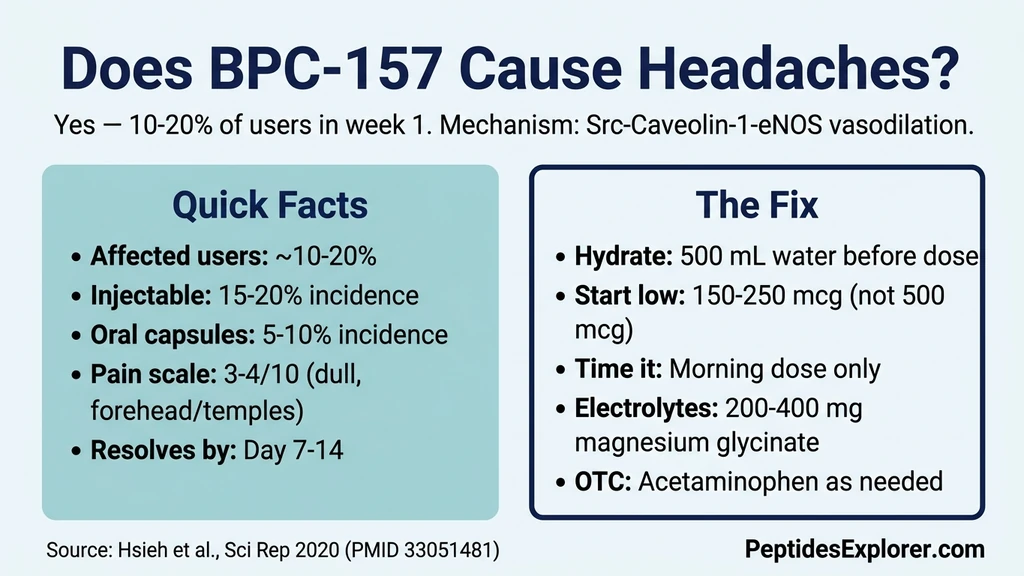
You injected BPC-157 this morning and now have a dull ache spreading across your forehead. Yes, BPC-157 can cause mild headaches in an estimated 10-20% of users, primarily during the first 3-7 days. The mechanism is vasodilation: BPC-157 activates the Src-Caveolin-1-eNOS pathway, increasing nitric oxide production and widening blood vessels (Hsieh et al., Sci Rep, 2020). This same blood vessel expansion that promotes healing also triggers headaches in susceptible individuals.
| Quick Reference | Details |
|---|---|
| Does BPC-157 cause headaches? | Yes, in approximately 10-20% of users |
| Typical severity | Mild to moderate (3-4/10 pain scale) |
| Character | Dull, diffuse, forehead or temples |
| Onset | Days 1-3 of use |
| Peak | Days 3-5 |
| Resolution | Days 5-7 in most users; nearly all by day 14 |
| Mechanism | Nitric oxide-mediated vasodilation (Src-Cav-1-eNOS pathway) |
| Injectable vs oral | Injectable causes more headaches (faster peak levels) |
| Key fix | Hydration (500 mL water before dose) + start at 250 mcg |
The headache is actually a signal that BPC-157 is engaging the vascular system. That same vasodilation is what delivers nutrients to injured tissue and drives the healing response. For dosing protocols, see our BPC-157 dosage calculator. For other transient GI side effects, see our guide on whether BPC-157 causes diarrhea.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
Why BPC-157 Causes Headaches: The Vasodilation Mechanism
The connection between BPC-157 and headaches runs through a specific molecular pathway. Understanding it explains why the headache happens, why it passes, and why it actually indicates the peptide is biologically active.
Nitric Oxide and the Src-Caveolin-1-eNOS Pathway
BPC-157 activates endothelial nitric oxide synthase (eNOS), the enzyme that produces nitric oxide (NO) in blood vessel walls. It does this through two identified pathways: the classical VEGFR2-PI3K-Akt-eNOS cascade and the Src-Caveolin-1-eNOS pathway (Hsieh et al., Sci Rep, 2020).
Increased NO production dilates blood vessels. When cerebral vessels (the arteries supplying your brain) dilate, the surrounding tissue stretches. Pain receptors in the vessel walls fire. You perceive a headache.
This is the same mechanism behind nitroglycerin headaches. Patients taking nitroglycerin for angina commonly report headaches because the drug floods the system with NO, dilating vessels throughout the body including the brain. BPC-157's effect is milder, but the pathway is identical.
Blood Pressure Changes During Adaptation
BPC-157 does not simply dilate blood vessels. It modulates the entire NO system bidirectionally. In hypertensive rats, BPC-157 lowered blood pressure by counteracting L-NAME (an NO inhibitor). In hypotensive rats, it raised blood pressure by counteracting L-arginine (an NO precursor) (Sikirić et al., Eur J Pharmacol, 1997).
During the first week of use, your cardiovascular system is recalibrating to BPC-157's modulatory presence. Blood pressure may fluctuate by 5-15 mmHg in either direction. These transient fluctuations contribute to headaches independently of the direct vasodilation effect. Once the NO system reaches a new equilibrium, both the BP fluctuations and headaches resolve.
For more on BPC-157's cardiovascular effects, see does BPC-157 cause high blood pressure.
Why Headaches Mean BPC-157 Is Biologically Active
The vasodilation causing your headache is the same mechanism that promotes tissue healing. BPC-157 increases blood flow to injured areas through NO-mediated vessel dilation and VEGF-driven angiogenesis (new blood vessel formation) (Sikirić et al., Pharmaceuticals, 2025).
More blood flow means more oxygen, more growth factors, and more immune cells reaching the damaged tissue. The headache is a systemic side effect of this targeted healing response. It does not mean something is wrong. It means the peptide is interacting with your vascular system as documented in the research.
That said, not all headaches confirm BPC-157 is "working." Some users experience no headache and still achieve full therapeutic benefit. The absence of a headache does not indicate an inactive product.
How Common Are BPC-157 Headaches?
No clinical trial has specifically measured headache incidence from BPC-157. The estimates below come from user reports, clinical practice observations, and community data.
| Population | Estimated Headache Incidence | Notes |
|---|---|---|
| All BPC-157 users | 10-20% | First week, any administration route |
| Injectable users | 15-20% | Faster systemic absorption = higher peak |
| Oral users | 5-10% | Slower absorption = lower peak levels |
| Users starting at 500 mcg | Higher end of range | More pronounced vasodilation |
| Users starting at 250 mcg | Lower end of range | Gradual vascular adaptation |
| Users with migraine history | Higher than average | Pre-existing vascular sensitivity |
The typical BPC-157 headache scores 3-4 on a 10-point pain scale. Users describe it as dull, non-throbbing, located across the forehead or temples. It is not a migraine. It does not include aura, light sensitivity, or nausea in most cases.
Most users who experience it describe it as "noticeable but not bad enough to stop." That assessment aligns with the pharmacological expectation: mild vasodilation produces mild discomfort.
Injectable vs Oral: Which Causes More Headaches?
Injectable BPC-157 causes headaches more frequently than oral forms. The reason is pharmacokinetic: how fast the peptide reaches peak blood levels.
Subcutaneous injection delivers BPC-157 directly into tissue with rapid absorption into the bloodstream. Peak blood levels arrive within 15-30 minutes. This fast peak means a rapid increase in NO production and acute vasodilation. Cerebral vessels dilate quickly. Headache onset follows within 1-2 hours of injection.
Oral administration delivers BPC-157 through the GI tract with slower, more gradual absorption. First-pass metabolism in the liver reduces peak blood levels. The NO increase is spread over hours rather than minutes. The vasodilation curve is flatter. Headaches are less common and less intense.
Nasal spray falls between the two. Mucosal absorption is fast (comparable to injection for onset) but delivers smaller doses. Headache risk is intermediate.
If headaches are your primary concern with BPC-157, oral capsules offer a lower-headache alternative. The trade-off: lower systemic bioavailability (estimated 50-70% for oral versus near-100% for injection). For detailed route comparison, see our BPC-157 oral vs injection guide.
How Long Do BPC-157 Headaches Last?
The timeline follows a consistent pattern tied to vascular adaptation.
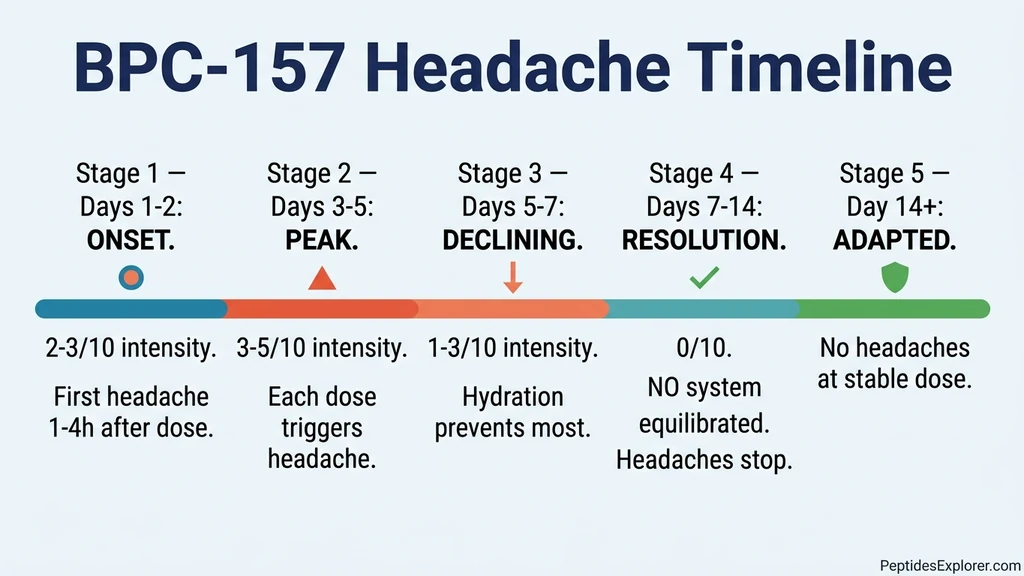
Day 1-2: Onset. The headache first appears, usually within 1-4 hours of the first or second dose. Injectable users notice it sooner. Oral users may not feel it until day 2. Intensity is mild (2-3/10).
Day 3-5: Peak. The adjustment period when headaches are most noticeable. Intensity may reach 4-5/10 for some users. Acetaminophen provides relief. Each individual dose triggers a headache, but the headache starts arriving later after injection and resolving faster as the body adapts.
Day 5-7: Declining. Headache frequency and intensity drop. Many users notice the headache only if they skip hydration before dosing. The vascular system is recalibrating to BPC-157's NO modulatory effects.
Day 7-14: Resolution. Nearly all users report complete headache resolution by the end of week 2. The NO system has reached its new equilibrium. BPC-157 continues exerting its therapeutic effects without triggering the vascular discomfort.
Beyond 14 days. Persistent headaches after two weeks at a stable dose are unlikely caused by BPC-157. Consider other causes: dehydration, screen time, sleep quality, caffeine changes, or stress. If headaches persist, consult a physician.
| Phase | Days | Intensity | What Happens |
|---|---|---|---|
| Onset | 1-2 | 2-3/10 | First headaches within 1-4 hours of dosing |
| Peak | 3-5 | 3-5/10 | Each dose triggers headache; adaptation begins |
| Declining | 5-7 | 1-3/10 | Headache frequency drops; hydration reduces risk |
| Resolution | 7-14 | 0/10 | NO system equilibrium; full tolerance established |
| Post-adaptation | >14 | 0/10 | No headaches expected at stable dose |
How to Prevent or Manage BPC-157 Headaches
Five strategies address BPC-157 headaches. The first two resolve the issue for most users.
Pre-Dose Hydration
Dehydration amplifies vasodilation headaches. When blood volume is low, vessels dilate more aggressively to maintain perfusion. Adding BPC-157's NO boost on top of dehydration-related vasodilation produces a stronger headache.
Drink 500 mL (about 16 oz) of water 30 minutes before your BPC-157 dose. Maintain total daily intake of 2.5-3 liters. This single intervention prevents or significantly reduces headaches in the majority of affected users. Think of it as pre-loading your vascular system with volume so the vessels do not need to dilate as much.
Start Low, Increase Gradually
Begin at 150-250 mcg instead of jumping to 500 mcg. The lower starting dose produces less acute vasodilation, giving your cerebral vessels time to adapt gradually.
Titration schedule: - Days 1-3: 150-250 mcg - Days 4-6: 250-350 mcg - Days 7-10: 350-500 mcg (target dose)
Each step increases NO production by a small increment rather than one large spike. Users who follow this graduated approach report significantly fewer headaches than those who start at full dose. The total time to reach therapeutic dosing increases by about one week, a worthwhile trade-off.
Morning Dosing
Inject or take BPC-157 in the morning, before 10 AM. The vasodilation peak occurs 2-6 hours post-dose. Morning dosing means the peak hits during active daylight hours when you are upright, hydrated, and engaged in activity. Blood distributes more evenly when standing and moving.
Evening dosing concentrates the vasodilation peak during sedentary evening hours and can interfere with sleep onset. A headache at 3 PM while working is manageable. A headache at 10 PM while trying to sleep compounds into insomnia. For more on timing and sleep effects, see our BPC-157 insomnia guide.
Electrolyte Support
Sodium, potassium, and magnesium all influence vascular tone. Low magnesium in particular is associated with increased headache susceptibility because magnesium helps regulate vessel diameter.
Magnesium glycinate (200-400 mg before bed) may specifically counteract vasodilation headaches. Magnesium acts as a natural calcium channel blocker, moderating the degree of vessel dilation. Glycinate is the preferred form because it has the best absorption and fewest GI side effects.
Electrolyte drinks during the first week provide sodium and potassium that support blood volume. Higher blood volume means less compensatory vasodilation. Any commercial electrolyte mix works. Target 500-1,000 mg sodium and 200-400 mg potassium daily above your dietary baseline.
OTC Pain Relief When Needed
Acetaminophen (paracetamol) is the preferred choice. It reduces headache pain without interfering with BPC-157's mechanism of action. Standard adult dose: 500-1,000 mg as needed, maximum 3,000 mg per 24 hours.
NSAIDs (ibuprofen, naproxen, aspirin) are safe for short-term use with BPC-157. In fact, BPC-157 counteracts NSAID-induced GI toxicity in animal studies (Sikirić et al., Curr Pharm Des, 2012). If you are taking BPC-157 specifically for GI healing, NSAIDs are counterproductive to your goal even though BPC-157 may protect against their damage. For non-GI indications, short-term NSAID use for headache management is reasonable.
Do not take headache medication preemptively before every BPC-157 dose. Medication-overuse headache develops when pain relievers are taken more than 10-15 days per month. Use OTC pain relief only when the headache is bothersome, not as prophylaxis.
When to Be Concerned About BPC-157 Headaches
Most BPC-157 headaches are benign vasodilation responses. Certain patterns warrant immediate medical attention.
Stop BPC-157 and seek emergency care if you experience:
- Sudden, severe headache (10/10, "worst headache of my life") within minutes of injection
- Headache with visual disturbances: blurred vision, blind spots, flashing lights, double vision
- Headache with confusion, difficulty speaking, or memory problems
- Headache with numbness or weakness on one side of the body
- Headache with stiff neck and fever (meningitis signs)
- Headache with seizure
These patterns suggest a vascular emergency (stroke, cerebral hemorrhage, aneurysm) that may be coincidental to BPC-157 use or, in extremely rare theoretical cases, related to acute vasodilation in vulnerable vessels.
Stop BPC-157 and consult a physician (non-emergency) if:
- Headaches persist beyond 2 weeks at stable dose despite hydration and dose reduction
- Headache intensity increases over time rather than decreasing
- You develop new migraine-like features (aura, light sensitivity, nausea) that you have never had before
- Headaches are accompanied by persistent elevated blood pressure (>140/90 on multiple readings)
BPC-157 and Blood Pressure: The Full Picture
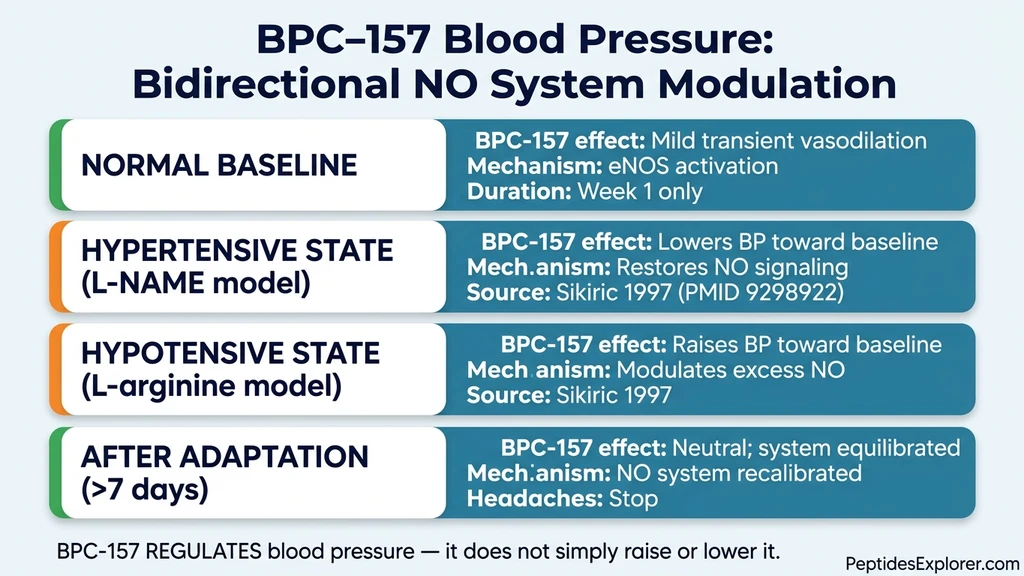
Headaches from BPC-157 exist within the broader context of its cardiovascular effects. The peptide does not simply dilate blood vessels. It regulates them.
BPC-157 counteracts L-NAME-induced hypertension (where NO production is blocked) by restoring NO signaling. It also counteracts L-arginine-induced hypotension (where excess NO causes dangerous drops) by modulating the system back toward baseline (Sikirić et al., Eur J Pharmacol, 1997). A comprehensive review of BPC-157's NO system interactions confirmed this bidirectional regulatory capacity (Sikirić et al., Curr Pharm Des, 2013).
This bidirectional effect explains why most users tolerate BPC-157 after the first week. The initial vasodilation and blood pressure fluctuations represent the system adjusting to a new modulatory input. Once equilibrium is reached, the headaches stop because the vessels are no longer acutely dilating in response to each dose.
| Blood Pressure State | BPC-157 Effect | Mechanism |
|---|---|---|
| Normal baseline | Mild transient vasodilation | eNOS activation |
| Hypertensive (L-NAME model) | Lowers BP toward baseline | Restores NO signaling |
| Hypotensive (L-arginine model) | Raises BP toward baseline | Modulates excess NO |
| After adaptation (>7 days) | Neutral; system equilibrated | NO system recalibrated |
For users concerned about long-term cardiovascular effects, the vascular research on BPC-157 is extensive and consistently shows protective rather than harmful effects on blood vessels (Seiwerth et al., J Physiol Pharmacol, 2021). The peptide promotes healthy angiogenesis and supports vascular integrity through multiple pathways (Sikirić et al., Pharmaceuticals, 2025). For the detailed discussion of BPC-157's blood pressure effects, see our does BPC-157 cause high blood pressure guide.
What the Research Confirms About BPC-157 Headaches
No human trial has measured BPC-157 headache incidence specifically. The evidence below connects the documented pharmacology to the reported side effect.
Vasodilation mechanism (Hsieh et al., 2020). BPC-157 modulates vasomotor tone through Src-Caveolin-1-eNOS signaling. The study demonstrated that BPC-157 activates eNOS through this pathway, increasing NO production and relaxing blood vessel smooth muscle. This is the primary molecular explanation for BPC-157 headaches (PubMed).
Blood pressure modulation (Sikirić et al., 1997). BPC-157 interacts with L-NAME and L-arginine in opposite directions, demonstrating bidirectional control of the NO system. Blood pressure effects are modulatory, not simply vasodilatory (PubMed).
NO system comprehensive review (Sikirić et al., 2013). Detailed analysis of BPC-157's relationship with nitric oxide signaling across multiple organ systems. Confirmed the peptide's regulatory role in vascular function (PubMed).
Safety profile (Sikirić et al., 2024). Pleiotropic review confirming BPC-157's multi-system effects with no toxicity at any tested dose. No lethal dose achieved in animal models (PMC).
Human safety pilot (2025). Administration of 20 mg BPC-157 intravenously in humans produced no adverse events, providing the first direct human safety data at doses far exceeding typical subcutaneous use (PubMed).
Limitation. All mechanism studies were conducted in animals. No human trial has specifically measured headache incidence, severity, or duration from BPC-157 administration. The connection between the demonstrated vasodilation mechanism and reported headaches is pharmacologically sound but clinically unconfirmed.
Related side effect guides that share the same NO pathway mechanism: does BPC-157 cause high blood pressure, BPC-157 TB-500 side effects (where combined vasodilation may intensify headaches), and BPC-157 capsule side effects (oral-specific profile including GI effects). For the complete protocol guide including timing and injection technique that minimizes headaches, see how to take BPC-157.
Frequently Asked Questions
Are BPC-157 headaches dangerous?
BPC-157 headaches are not dangerous in the vast majority of cases. They score 3-4/10 on a pain scale, are caused by nitric oxide-mediated vasodilation, and resolve within 5-7 days. Seek emergency care only for sudden severe headaches (10/10), headaches with visual disturbances, or headaches accompanied by neurological symptoms like confusion, numbness, or weakness on one side.
Does getting a headache from BPC-157 mean it is working?
The headache confirms BPC-157 is engaging the vascular system through NO-mediated vasodilation. This same mechanism drives the healing response by increasing blood flow to injured tissue. A headache is evidence of biological activity, not direct proof of therapeutic efficacy. Many users achieve full benefits without headaches. Absence of headache does not indicate an inactive product.
Will BPC-157 headaches go away on their own?
Yes. The vascular system adapts to BPC-157's NO modulatory effects within 5-14 days. Most users report significant improvement by day 5-7 and complete resolution by day 14. The NO system reaches a new equilibrium where each dose no longer causes acute vasodilation. No intervention is needed beyond staying hydrated and starting at a lower dose.
Should I take ibuprofen for BPC-157 headaches?
Acetaminophen is preferred because it does not affect the gastrointestinal tract. Ibuprofen is safe for short-term use with BPC-157 if you are not taking the peptide for gut healing. BPC-157 actually counteracts NSAID-induced GI toxicity in animal studies. Avoid daily NSAID use beyond 10-15 days to prevent medication-overuse headache.
Do oral BPC-157 capsules cause fewer headaches than injections?
Yes. Oral BPC-157 causes headaches in an estimated 5-10% of users versus 15-20% for injectable forms. The difference is pharmacokinetic: oral absorption is slower, producing lower peak blood levels and less acute vasodilation. Oral forms cause more GI side effects instead (nausea, diarrhea). Choose your trade-off based on your primary concern.
What dose of BPC-157 is least likely to cause headaches?
Start at 150-250 mcg daily. This produces less acute vasodilation than the standard 500 mcg dose. Increase by 100 mcg every 3 days until you reach your target. Users who follow this graduated protocol report fewer and milder headaches than those starting at full dose. Pre-dose hydration (500 mL water) at any dose level further reduces headache incidence.
Can BPC-157 trigger migraines?
BPC-157 could theoretically trigger migraines in individuals with a migraine history, since vasodilation is a known migraine trigger. The NO pathway activated by BPC-157 overlaps with pathways implicated in migraine pathophysiology. If you have a documented migraine disorder, start at the lowest dose (150 mcg) and discuss BPC-157 use with your neurologist before beginning.
How much water should I drink to prevent BPC-157 headaches?
Drink 500 mL (16 oz) of water 30 minutes before each BPC-157 dose. Maintain 2.5-3 liters of total daily water intake during the first two weeks. Pre-dose hydration increases blood volume, reducing the degree of compensatory vasodilation that triggers headaches. Add an electrolyte supplement containing 200-400 mg magnesium glycinate for additional vascular support.
The Bottom Line
BPC-157 causes headaches in approximately 10-20% of users during the first week. The mechanism is nitric oxide-mediated vasodilation through the Src-Caveolin-1-eNOS pathway, the same vascular response that drives tissue healing. The headache is a side effect of the therapeutic mechanism, not a sign of toxicity.
The fix is practical. Drink 500 mL of water before each dose. Start at 250 mcg instead of 500. Inject in the morning. These three steps prevent or minimize headaches for most users. The vascular system adapts within 5-14 days, and headaches resolve without further intervention.
If headaches persist beyond two weeks, worsen over time, or are accompanied by neurological symptoms, stop BPC-157 and consult a physician. These patterns are rare but require medical evaluation before resuming any peptide protocol.
Use our BPC-157 dosage calculator to plan a graduated dosing protocol that minimizes vasodilation headaches. For reconstitution guidance, see the peptide reconstitution calculator. For the complete side effect profile, read our BPC-157 side effects guide. If you are experiencing BPC-157 insomnia alongside headaches, both side effects share the same solution: morning dosing.
Helpful Tools
Related Articles
Can Tirzepatide Cause Joint Pain? Clinical Data
Can tirzepatide cause joint pain? SURMOUNT arthralgia rates match placebo. Review 5 indirect causes, uric acid risks, and 8 relief tactics.
BPC-157 TB-500 Side Effects: Stack Safety Data
BPC-157 TB-500 stack side effects: headaches, fatigue weeks 1-2, anaphylaxis risk, cancer screening tips. Week-by-week timeline inside.
Peptide Therapy Side Effects: Complete Guide (2026)
Peptide therapy side effects by category: GLP-1, GH-releasing, healing, and immune. Severity matrix, incidence rates, and management strategies.
Can BPC-157 Cause Diarrhea? Research Review
Can BPC-157 cause diarrhea? Yes, 5-15% of users on days 1-5. Gut-healing paradox, oral vs injectable, dose-response, and management.