You injected BPC-157 at 8 PM to heal a nagging shoulder. By midnight you are staring at the ceiling, mind racing. No clinical trial has linked BPC-157 to insomnia, but its documented effects on dopamine D2 and serotonin pathways provide a plausible mechanism for sleep disruption (Sikirić et al., J Physiol Paris, 1999). Community reports put the prevalence at roughly 10 to 15 percent, almost always tied to evening injection timing. The fix is switching the dose to before 10 AM.
| Quick Reference | Details |
|---|---|
| Clinical evidence of insomnia | None (no human trials measuring sleep) |
| Anecdotal prevalence | 10 to 15 percent of users report some sleep disruption |
| Severity | Mild: difficulty falling asleep, not staying asleep |
| Mechanism | Dopamine D2 receptor and serotonin pathway modulation |
| Onset | Within 1 to 3 days of starting, dose dependent |
| Resolution | Usually within 1 to 2 weeks of continued use |
| Key fix | Switch injections to morning (before 10 AM) |
| Standard dose | 250 to 500 mcg/day subcutaneously |
For exact draw volumes, use the BPC-157 dosage calculator. For full safety context, see the BPC-157 side effects review and the peptide safety guide.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
How BPC-157 Could Affect Your Sleep
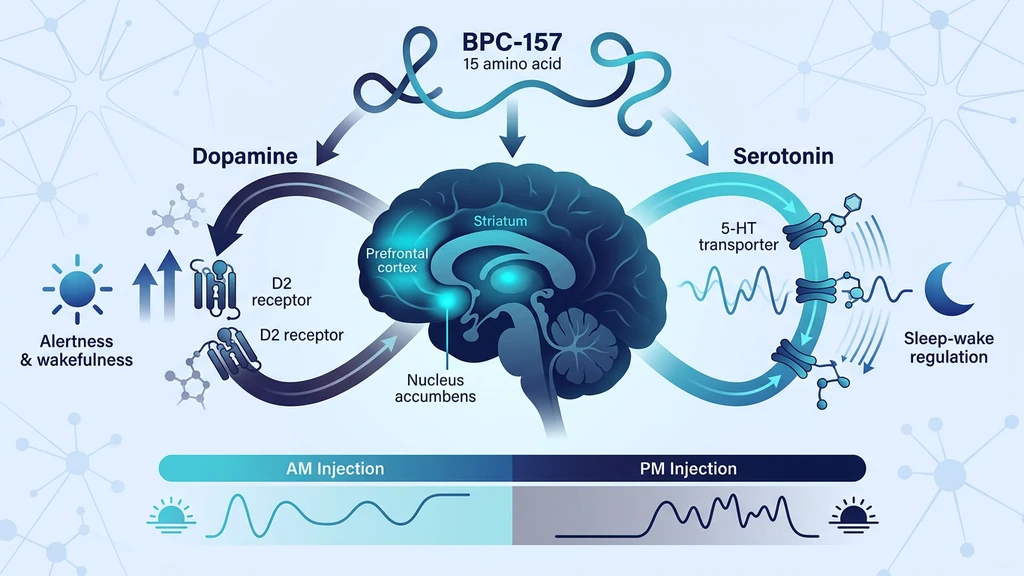
Think of your brain's sleep system like a dimmer switch. Serotonin turns the lights down at night, signaling your body to wind down. Dopamine keeps the lights bright, promoting wakefulness and alertness. BPC-157 reaches into the control panel and adjusts both dials simultaneously.
Sikirić et al. demonstrated that BPC-157 modulates dopamine D2 receptors and interacts with the serotonergic system in rats (Sikirić et al., J Physiol Paris, 1999). A later study confirmed these effects extend to both dopamine and serotonin turnover across multiple brain regions (Sikirić et al., Curr Pharm Des, 2010). When dopaminergic activity increases in the evening hours, falling asleep becomes harder.
There is a third pathway. BPC-157 interacts with the nitric oxide (NO) system, which regulates vascular tone and neural signaling (Sikirić et al., J Pharmacol Sci, 2014). Increased NO activity can heighten alertness. BPC-157 also modulates GABAergic pathways, the same system that benzodiazepines target to induce sleep (Sikirić et al., 2010). These overlapping mechanisms explain why some users feel wired after an evening dose.
What Evening Injection Looks Like in Practice
A 38-year-old man injects 250 mcg of BPC-157 subcutaneously near his injured knee at 7 PM. He follows his normal bedtime routine. At 11 PM, he lies down but cannot quiet his mind. Sleep comes at 1:30 AM instead of his usual 11:30. His Oura ring shows 45 minutes of deep sleep versus his baseline of 90 minutes. He assumes the peptide is the cause and considers stopping.
The fix is simple. He switches his injection to 7 AM. Within two days, sleep returns to normal. Deep sleep rebounds to 85 minutes. The BPC-157 continues healing his knee without disrupting his nights. The peptide itself was not the problem. The timing was.
A second scenario: a woman using 500 mcg daily for gut healing reports improved sleep after starting BPC-157. Her chronic abdominal pain had been waking her 2-3 times per night. With BPC-157 reducing inflammation and pain, she sleeps through the night for the first time in months. This paradoxical improvement occurs because pain reduction outweighs any stimulatory effect on neurotransmitters.
When Does BPC-157 Sleep Disruption Start and Stop?
Sleep effects from BPC-157 follow a predictable pattern tied to neurotransmitter adaptation.
Onset: Days 1-3
Sleep disruption, when it occurs, appears within the first 1-3 days of starting BPC-157. The dopaminergic and serotonergic systems respond quickly to the peptide's modulatory effects. Users who inject in the evening notice it sooner than morning injectors.
Peak: Days 3-7
The first week is when sleep disruption is most noticeable. Your brain has not yet adapted to the altered neurotransmitter balance. Users report difficulty falling asleep (sleep onset latency increases by 20-40 minutes), lighter sleep, and earlier waking. Total sleep may drop from 7-8 hours to 5.5-6.5 hours.
Resolution: Weeks 1-2
Neurotransmitter receptors recalibrate. The dopaminergic system reaches a new equilibrium. Most users report sleep normalizing by the end of week 2 without any changes to their protocol. Those who switch to morning injections typically resolve the issue within 2-3 days.
When to Seek Medical Advice
Persistent insomnia beyond 2-3 weeks despite morning injection timing. Severe sleep disruption (fewer than 4 hours per night). New anxiety or racing thoughts that accompany the insomnia. These patterns may indicate a sensitivity to BPC-157's neurotransmitter effects or an unrelated sleep disorder that requires evaluation.
How to Minimize Sleep Disruption from BPC-157
Four strategies address BPC-157-related sleep issues. The first one resolves the problem for most users.
Inject in the Morning
Shift your BPC-157 injection to before 10 AM. The peptide's peak neurotransmitter effects occur within 2-6 hours of injection. A morning dose means peak dopaminergic activity aligns with your natural wakefulness period. By evening, the acute stimulatory effect has diminished. This single change eliminates sleep disruption in the majority of affected users.
Start at 250 mcg Before Increasing
If you plan to use 500 mcg daily, start at 250 mcg for the first 5-7 days. This gives your neurotransmitter systems time to adjust gradually. Jumping straight to 500 mcg is more likely to produce noticeable sleep effects. The dose-response relationship with sleep disruption appears roughly linear: higher doses correlate with more pronounced effects.
Protect Your Sleep Hygiene
Standard sleep hygiene becomes more important on BPC-157. Keep your bedroom at 65-68F (18-20C). Avoid screens for 30 minutes before bed. No caffeine after noon if you notice sensitivity. These measures counterbalance the mild stimulatory effect. Magnesium glycinate (200-400 mg before bed) supports GABAergic activity and may offset BPC-157's modulation of that pathway.
Split the Dose If Needed
Instead of 500 mcg once daily, try 250 mcg in the morning and 250 mcg at noon. Splitting the dose reduces peak neurotransmitter fluctuation. Each injection produces a smaller dopaminergic spike. This approach maintains the same total daily dose while smoothing the pharmacological curve. Never inject the second dose after 2 PM.
What Does the Research Actually Show?
Neurotransmitter Modulation (Sikirić et al., 1999) BPC-157 modulates dopamine D2 receptors, serotonin transporters, and related pathways in rat brains. The study demonstrated that BPC-157 counteracts both the hyperactivity caused by amphetamine and the catalepsy caused by haloperidol, indicating it acts as a modulator rather than a simple agonist or antagonist (PubMed).
Dopamine-Serotonin System Interactions (Sikirić et al., 2010) Extended research confirmed BPC-157 affects dopamine, serotonin, and their metabolites across multiple brain regions including the striatum, nucleus accumbens, and prefrontal cortex. The peptide also interacts with GABAergic and NO systems (PubMed).
NO System and Vascular Effects (Sikirić et al., 2014) BPC-157 interacts with the nitric oxide system, influencing both blood vessel function and neural signaling. Increased NO activity can promote wakefulness and alertness in the short term (PubMed).
Critical limitation: all of these studies were conducted in rats. No human clinical trial has measured BPC-157's effects on sleep architecture, polysomnography, or subjective sleep quality. The connection between BPC-157 and insomnia remains mechanistically plausible but clinically unproven.
BPC-157 Insomnia vs. Other Causes
Before attributing insomnia to BPC-157, rule out these common confounders. Users starting a peptide protocol often make multiple lifestyle changes simultaneously, and the peptide may not be the culprit.
Injection site pain or discomfort. Subcutaneous injection can cause local soreness, redness, or itching that disrupts sleep. If you are injecting near an injury site, inflammation at the injection point may worsen at night.
Anxiety about the protocol. Starting a new peptide can trigger hypervigilance. You monitor every sensation, research side effects before bed, and lie awake wondering if each twitch is normal. This psychological component is independent of BPC-157's pharmacology.
Bacteriostatic water sensitivity. Some users react to benzyl alcohol (the preservative in bacteriostatic water) with mild stimulation or skin reactions. If insomnia coincides with injection site redness, try a different BAC water source.
Pre-existing sleep issues. Roughly 30% of adults have some form of insomnia (Roth, 2007). Attributing longstanding sleep problems to a new peptide creates a false association. Track your sleep for one week before starting BPC-157 to establish a baseline.
Common Mistakes That Make BPC-157 Insomnia Worse
Five errors keep showing up in user reports of persistent sleep disruption. Each has a concrete fix.
1. Injecting after dinner. Peak dopaminergic activation hits 2 to 6 hours after the dose. A 7 PM injection lands stimulation right at your bedtime. Move the dose to before 10 AM and the peak passes during the workday.
2. Jumping straight to 500 mcg. A first-time user who starts at 500 mcg sees twice the dopaminergic load of a 250 mcg start. The first week of any protocol is when neurotransmitter systems are least adapted. Hold at 250 mcg for at least 5 to 7 days before titrating up. The BPC-157 dosage by body weight guide covers escalation pacing.
3. Stacking with caffeine late in the day. Caffeine after 2 PM compounds with BPC-157's mild stimulatory effect. A 200 mg afternoon coffee that you tolerated before starting BPC-157 can now push sleep onset latency past midnight.
4. Ignoring bacteriostatic water as a variable. Benzyl alcohol in bacteriostatic water causes mild reactions in a small subset of users. If insomnia tracks with the start of a new vial, swap the BAC water source before blaming BPC-157.
5. Continuing past week 3 without adjustment. Most users adapt in 14 days. If you are still losing sleep at week 3 on morning dosing, the protocol is not for you. Stop and reassess. The peptide interaction checker flags conflicts with current medications that may explain persistence.
Important Warnings
BPC-157 has not been approved for human use by any regulatory agency. All human dosing data comes from anecdotal reports, not clinical trials. The safety profile in humans is not established.
Do not combine BPC-157 with prescription sleep medications (zolpidem, eszopiclone, benzodiazepines) without medical supervision. BPC-157's GABAergic interactions could theoretically alter the effects of these drugs. The interaction has not been studied.
If you take antidepressants that affect serotonin (SSRIs, SNRIs), be aware that BPC-157's serotonergic effects may interact with your medication. Consult your prescriber before starting BPC-157.
Users with a history of bipolar disorder or mania should exercise particular caution. Dopaminergic stimulation can trigger manic episodes in susceptible individuals. Insomnia is often an early warning sign of mania.
For proper injection technique that minimizes discomfort and anxiety-related sleep disruption, see our how to inject BPC-157 guide. For information on where to buy peptides, consult our sourcing guide.
Related Side Effects
Does Semaglutide Cause Fatigue? The opposite problem. Semaglutide causes tiredness in 11% of users through caloric deficit and GLP-1 receptor activation. If you stack BPC-157 with semaglutide, the stimulatory and sedating effects may partially cancel each other.
Does Semaglutide Cause Nausea? GI discomfort from other peptides can independently disrupt sleep. Nausea at bedtime keeps you awake regardless of BPC-157's neurotransmitter effects.
Does BPC-157 Cause High Blood Pressure? BPC-157's interaction with the nitric oxide system can also affect cardiovascular markers. If you experience both sleep disruption and elevated blood pressure, the NO pathway may be involved.
Does BPC-157 Cause Liver Damage? Concerns about BPC-157 organ effects extend beyond sleep. The liver data is actually reassuring: animal studies show hepatoprotective effects rather than damage.
BPC-157 and Alcohol Alcohol disrupts sleep architecture independently of BPC-157. If you drink while on a BPC-157 protocol, the combined sleep effects may compound.
BPC-157 Dosage for 200lb Male Dose-dependent insomnia is more common at 500 mcg. Starting at 250 mcg reduces the risk. Dosing protocols for every body weight.
How to Take BPC-157 Morning timing is the single most effective fix for sleep issues. Full administration routes and dosing windows.
Peptide Safety Guide Side effect management across every peptide class: injection technique, storage, and when to seek medical care.
Frequently Asked Questions
Does BPC-157 cause insomnia?
No clinical trial has linked BPC-157 to insomnia. The peptide modulates dopamine D2 receptors and serotonin pathways, both of which regulate sleep architecture (Sikirić et al., 1999). Roughly 10 to 15 percent of users report mild sleep disruption, mostly with evening injections. Switching to morning dosing before 10 AM resolves the issue in most cases. See how to take BPC-157 for timing details.
When should I inject BPC-157 to avoid sleep problems?
Inject before 10 AM. Peak neurotransmitter effects occur within 2 to 6 hours of injection, so a morning dose aligns dopaminergic activity with natural wakefulness. Evening injections after 5 PM carry the highest risk of sleep disruption. If you run 500 mcg daily, split into 250 mcg at 7 AM and 250 mcg at noon. The BPC-157 dosage calculator confirms your draw volume.
How long does BPC-157 insomnia last?
Sleep disruption from BPC-157 typically resolves within 1 to 2 weeks as neurotransmitter receptors adapt. The first 3 to 7 days are the most affected, with sleep onset latency increasing by 20 to 40 minutes. Switching to morning injection timing accelerates resolution to 2 to 3 days. Persistent insomnia beyond 3 weeks warrants a physician visit. Review BPC-157 side effects for the full safety profile.
Can BPC-157 improve sleep?
Paradoxically, yes. Users taking BPC-157 for pain-related conditions (gut inflammation, joint injuries, tendon damage) sometimes report better sleep. Chronic pain causes frequent nighttime awakenings. When BPC-157 reduces the underlying pain, uninterrupted sleep returns. Roughly 15 to 20 percent of community reports describe this benefit. For evidence on healing claims, see the BPC-157 benefits overview.
What dose of BPC-157 is least likely to cause sleep issues?
Start at 250 mcg per day injected in the morning. This sits at the lower end of the standard 250 to 500 mcg daily range. The dose response with sleep disruption is roughly linear. Users at 500 mcg report more sleep effects than those at 250 mcg. After 5 to 7 days at 250 mcg with no sleep issues, increase to 500 mcg. See the BPC-157 dosage by body weight chart for personalized ranges.
Does BPC-157 interact with sleep medications?
BPC-157 modulates GABA pathways in rat models (Sikirić et al., 2010), the same system targeted by zolpidem, eszopiclone, and benzodiazepines. No human interaction study exists. Do not combine BPC-157 with prescription sleep medications without physician supervision. SSRI and SNRI users should also discuss it with their prescriber because of serotonergic overlap. The peptide interaction checker flags common conflicts.
Can BPC-157 cause anxiety along with insomnia?
A small fraction of users (under 5 percent) report mild anxiety alongside sleep disruption in the first week of dosing. The mechanism overlaps with the dopaminergic stimulation that drives insomnia. Both effects respond to morning dosing and dose reduction to 250 mcg. Persistent anxiety beyond 14 days warrants stopping the protocol. See BPC-157 side effects for full symptom mapping.
Is BPC-157 oral capsules less likely to disrupt sleep?
Possibly. Oral BPC-157 bypasses systemic circulation to a degree, with most of the peptide acting locally on gut tissue. Plasma concentrations stay lower than with subcutaneous injection, which may reduce central nervous system effects on dopamine and serotonin. Community reports suggest sleep disruption is less common with oral dosing, though no controlled comparison exists.
The Bottom Line
BPC-157 does not cause clinical insomnia based on available evidence. No human trial has measured its effects on sleep. The mechanism is plausible: dopamine D2 receptor modulation and serotonergic interactions can shift the neurotransmitter balance toward wakefulness. Community data suggests 10-15% of users notice mild sleep disruption, almost always tied to evening injection timing.
The fix is straightforward. Inject before 10 AM. Start at 250 mcg. Give your body 1-2 weeks to adapt. These three steps prevent or resolve sleep issues for the vast majority of users. If insomnia persists beyond 3 weeks despite morning timing, consult a physician.
Use our BPC-157 dosage calculator to plan your protocol. For proper reconstitution technique, see the peptide reconstitution calculator. Learn how to store peptides correctly to maintain potency throughout your cycle.
Helpful Tools
Related Articles
Does Tirzepatide Cause Insomnia?
Does tirzepatide cause insomnia? Trials say no, but 5 indirect pathways explain lost sleep. GI, blood sugar, and caloric deficit fixes.
BPC-157 Capsule Side Effects: Oral User Guide
BPC-157 capsule side effects: nausea in 20-30% of users, diarrhea days 1-5, fewer headaches than injectable. Acetate vs arginate compared.
Does BPC-157 Cause Liver Damage?
BPC-157 shows liver-protective effects in animal studies, not liver damage. Review the evidence on hepatotoxicity, ALT/AST levels, and safe dosing protocols.
Does BPC-157 Cause High BP?
BPC-157 may modulate blood pressure through the nitric oxide system. Review rat study data, NO pathway mechanisms, and safety considerations.