You opened a bottle of BPC-157 capsules, swallowed one on an empty stomach, and 40 minutes later felt a wave of nausea. Oral BPC-157 capsules cause mild gastrointestinal side effects in roughly 20-30% of users during the first 3-5 days. Nausea, bloating, and loose stools are the most common complaints. These effects stem from direct peptide contact with the GI mucosa and typically resolve within one week (Sikiric et al., Gut Liver, 2020). No serious adverse events have appeared in animal toxicity studies at doses far exceeding standard human protocols.
| Quick Reference | Details |
|---|---|
| Most common side effect | Nausea (especially above 500 mcg/day) |
| Onset | First 1-3 days of use |
| Duration | Resolves within 5-7 days for most users |
| GI effects frequency | ~20-30% of oral users report some GI discomfort |
| Headache frequency | ~5-10% with capsules vs 15-20% with injectable |
| Serious adverse events | None documented in preclinical toxicity studies |
| Key mitigation | Start at 250 mcg/day, take with food |
| Formulation difference | Arginate may cause fewer GI effects than acetate |
BPC-157 is not FDA-approved for any indication. No completed human clinical trial exists for oral capsules. Consult a healthcare provider before using any peptide.
For dosing guidance, use our BPC-157 dosage calculator. For a comparison with injectable, see our oral vs injection guide.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
Common Side Effects of Oral BPC-157 Capsules

Capsule-form BPC-157 produces a distinct side effect profile compared to injections. The peptide passes through the stomach and small intestine before reaching systemic circulation, which means GI tissue bears the initial load.
Nausea ranks as the most frequently reported complaint. Users describe it as mild queasiness that peaks 30-60 minutes after taking a capsule, particularly at doses above 500 mcg. Taking capsules with a small meal reduces this significantly.
Diarrhea and loose stools appear in the first 3-5 days, then resolve without intervention. BPC-157 interacts with intestinal tight junctions and mucosal blood flow, which can temporarily alter bowel motility (Chang et al., Curr Pharm Des, 2020). For a deeper look at this specific symptom, see our guide on BPC-157 and diarrhea.
Bloating and abdominal discomfort tend to accompany the diarrhea phase. The peptide stimulates local blood flow to the GI mucosa, producing a feeling of fullness or mild cramping in the first few days.
Appetite changes go both directions. Some users report increased hunger; others notice a temporary decrease. Both patterns stabilize by the end of week one.
Mild headaches occur less frequently with capsules than with injectable BPC-157. When injected subcutaneously, BPC-157 reaches systemic circulation faster and at higher peak concentrations, producing stronger vasodilation through the nitric oxide system (Hsieh et al., Sci Rep, 2020). Oral absorption is slower and more gradual, which blunts this effect.
Fatigue during the first week is reported by a smaller subset of users. This may relate to the body's inflammatory recalibration as BPC-157 modulates cytokine activity in the gut lining.
Why Capsule Side Effects Differ from Injection Side Effects
Think of it like the difference between swallowing an aspirin and getting an aspirin IV drip. The pill contacts your stomach lining directly and gets partially broken down by stomach acid before the remaining fraction enters your bloodstream. The IV drip bypasses the gut entirely and hits systemic circulation at full strength.
Oral BPC-157 follows the same principle. The peptide (Body Protection Compound-157, a stable gastric pentadecapeptide) contacts the GI mucosa directly, triggering local effects before any systemic absorption occurs. First-pass hepatic metabolism then reduces bioavailability to roughly 3% for acetate forms (He et al., Front Pharmacol, 2022). This means the gut sees a high local concentration while the rest of the body sees a relatively low one.
The paradox is worth noting: BPC-157 is studied precisely for its cytoprotective effects on the GI tract (Sikiric et al., Gut Liver, 2020). It accelerates ulcer healing, stabilizes intestinal permeability, and reduces mucosal inflammation. Yet the initial contact between a concentrated peptide bolus and sensitive stomach tissue can cause transient irritation. The healing follows the discomfort, not the other way around.
Injectable BPC-157 produces a different profile: more headaches (from faster NO-mediated vasodilation), more injection-site reactions, but fewer GI complaints.
How Long Do Capsule Side Effects Last?
Side effects from oral BPC-157 follow a predictable timeline.
Days 1-3: Peak intensity. Nausea, bloating, and loose stools are most pronounced. Your GI tract is encountering the peptide for the first time. Local mucosal blood flow increases. Tight junction remodeling begins.
Days 4-7: Diminishing. The gut adapts. Nausea fades first, usually by day 4. Bloating and stool changes follow by day 5-7. Users who started at 250 mcg typically feel normal by the end of this window.
Week 2 onward: Resolved. GI side effects are absent for the vast majority of users who reach this point. The mucosal tissue has adapted to the peptide's presence. Any residual effects beyond week 2 at standard doses (250-500 mcg/day) warrant reassessment of dose or formulation.
Dose plays a direct role in this timeline. Users starting at 500 mcg or higher experience longer and more intense GI symptoms than those beginning at 250 mcg. The adaptation curve stretches by 2-3 days at higher starting doses.
Capsule Side Effects vs Injectable Side Effects
The administration route changes which side effects dominate. This comparison table covers the most reported effects across both forms.
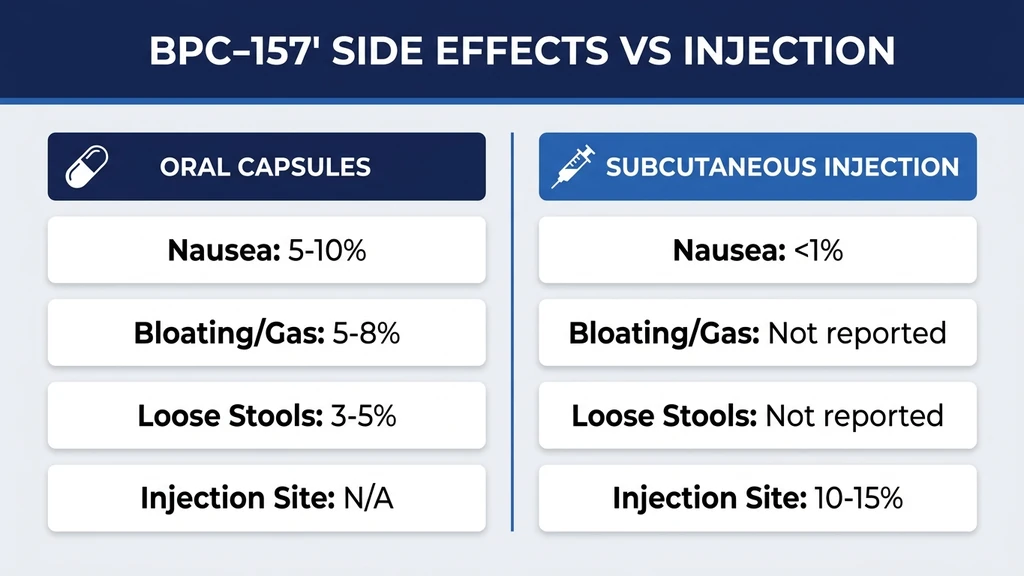
| Side Effect | Oral Capsules | Injectable (SubQ) |
|---|---|---|
| Nausea | Common (20-30%) | Uncommon (<10%) |
| Diarrhea | Common in first week | Rare |
| Bloating | Common in first week | Rare |
| Headache | Uncommon (~5-10%) | More common (~15-20%) |
| Injection-site pain | Not applicable | Common (~25%) |
| Injection-site redness | Not applicable | Common (~15-20%) |
| Dizziness | Rare | Uncommon (~10%) |
| Fatigue | Uncommon (~10%) | Uncommon (~10%) |
| Appetite changes | Occasional | Rare |
Oral users trade injection-site discomfort for GI symptoms. Injectable users trade GI comfort for site reactions and more frequent headaches.
The pharmacokinetic data explains why. He et al. (2022) showed that oral BPC-157 in rats produced peak plasma concentrations 60-90 minutes after administration, compared to 15-30 minutes for subcutaneous injection (He et al., Front Pharmacol, 2022). The slower rise with oral dosing reduces the acute vasodilatory spike that causes headaches, but the prolonged GI transit time increases local mucosal exposure.
For capsule-specific headache information, see does BPC-157 cause headaches. For GI-specific details, see can BPC-157 cause diarrhea.
Acetate vs Arginate Capsules: Do Side Effects Differ?
Two BPC-157 capsule formulations exist in the market, and the difference matters for side effects.
BPC-157 acetate is the standard research-grade form. It has low oral bioavailability (approximately 3% in animal models) because gastric acid degrades the peptide before significant absorption occurs (He et al., Front Pharmacol, 2022). More peptide is destroyed in the stomach, which means more degradation products contact the GI lining. This may contribute to the higher rate of nausea and bloating with acetate capsules.
BPC-157 arginate uses an arginine salt that stabilizes the peptide at stomach pH levels. Patent data (WO2014142764A1) claims oral bioavailability near 90% for the arginate form. If accurate, this means less peptide degradation in the stomach, less GI contact with breakdown products, and potentially fewer local side effects. The trade-off: higher systemic absorption could increase the likelihood of headaches and dizziness, bringing the side effect profile closer to injectable BPC-157.
| Feature | BPC-157 Acetate | BPC-157 Arginate |
|---|---|---|
| Oral bioavailability | ~3% (animal data) | Up to ~90% (patent claim) |
| Gastric acid stability | Low | High |
| GI side effects | More common | Potentially fewer |
| Systemic side effects | Less common | Potentially more |
| Research backing | Extensive (most studies use acetate) | Limited (patent data, fewer studies) |
| Price | Lower | Higher |
One important caveat: the 90% bioavailability claim for arginate comes from patent filings, not peer-reviewed pharmacokinetic studies. Independent verification is limited. Most published BPC-157 research uses the acetate form, so safety data is strongest for acetate.
Who Faces Higher Risk for Capsule Side Effects?
Not every user experiences GI complaints. Certain factors increase the likelihood and severity of oral BPC-157 side effects.
Pre-Existing GI Conditions
Users with IBS, IBD, GERD, or chronic gastritis have more sensitive GI mucosa. The initial irritation phase of oral BPC-157 can amplify existing symptoms before the peptide's protective effects take hold.
This creates a paradox. Many people take oral BPC-157 specifically for GI healing. Animal studies show BPC-157 accelerates ulcer closure and reduces intestinal inflammation (Sikiric et al., Curr Neuropharmacol, 2017). But the first 3-5 days may feel worse before improvement begins. Users with active GI conditions should start at 250 mcg with food and expect a brief adjustment period.
Medication Interactions
NSAIDs: BPC-157 counteracts NSAID-induced GI toxicity in animal models (Sikiric et al., Curr Pharm Des, 2012). Users taking ibuprofen or naproxen may actually experience fewer GI side effects from the combination than from NSAIDs alone. This is a potential positive interaction, not a contraindication.
Blood pressure medications: BPC-157 modulates the nitric oxide system and can affect vascular tone. Users on antihypertensives should monitor blood pressure during the first week. Dizziness may be more pronounced.
Anticoagulants: BPC-157 affects platelet function and angiogenesis in animal studies. While no adverse interaction has been documented, users on warfarin or direct oral anticoagulants should inform their physician before starting BPC-157 capsules.
Dosage-Related Risk Factors
Dose is the strongest predictor of side effect severity.
Above 500 mcg/day: GI side effects increase sharply. Users at 750 mcg or 1,000 mcg report nausea rates roughly double those at 250 mcg. No evidence shows doses above 500 mcg per day produce proportionally better outcomes.
Empty stomach dosing: Taking BPC-157 capsules without food concentrates the peptide against bare mucosa. Some protocols recommend empty-stomach dosing for better absorption, but the side effect trade-off is real. A small meal reduces nausea without meaningfully reducing absorption.
Time of day: Morning dosing on an empty stomach produces the strongest GI response. Users sensitive to nausea should take capsules with breakfast.
How to Minimize Capsule Side Effects
Five strategies reduce or eliminate GI discomfort from oral BPC-157.
Start Low, Increase Gradually
Begin at 250 mcg once daily for the first 5-7 days. This half-dose introduction lets your GI tract adjust to the peptide before increasing the load. After one week with no significant side effects, increase to 250 mcg twice daily (morning and early afternoon). If you tolerate that well for another week, you can move to 500 mcg twice daily if your protocol requires it.
This ramp-up takes 2-3 weeks to reach full dose. The patience pays off: users who start at full dose (500 mcg twice daily) report 2-3x more GI complaints than those who ramp up gradually.
Take Capsules with Food
A small meal buffers the peptide against the stomach lining. You do not need a full meal. A piece of toast, a few crackers, or half a banana provides enough buffer to reduce nausea by an estimated 50-70% based on community reports.
The trade-off: food may slightly reduce absorption. For acetate-form BPC-157, which already has low oral bioavailability (~3%), this reduction is negligible. For arginate forms with higher bioavailability, the impact is uncertain. If you are using BPC-157 specifically for GI healing, the local effect on the stomach and intestinal lining occurs regardless of systemic absorption.
Morning Dosing to Avoid Insomnia
BPC-157 modulates dopamine D2 receptors and serotonin pathways, which can affect sleep if taken in the evening (Sikiric et al., J Physiol Paris, 1999). Take capsules before 10 AM for the first dose and before 2 PM for a second dose. This timing aligns peak neurotransmitter activity with your natural wakefulness period.
Stay Hydrated
Drink at least 8 ounces of water when taking a BPC-157 capsule. Adequate hydration helps dissolve the capsule shell faster, distributes the peptide across a larger mucosal surface area, and reduces the concentration hitting any single spot. Dehydration concentrates the peptide and increases local irritation.
When to Stop or Switch to Injectable
Three situations warrant discontinuing oral BPC-157 or switching routes:
- 1.GI symptoms persist beyond 2 weeks at the lowest dose (250 mcg/day) with food.
- 2.Severe nausea or vomiting occurs that prevents normal eating.
- 3.Signs of allergic reaction appear: hives, throat swelling, difficulty breathing.
Switching to subcutaneous injection eliminates GI side effects entirely since the peptide never contacts the digestive tract. Learn how to inject BPC-157 if you decide to change routes. For information on taking BPC-157 orally, see our dedicated guide.
What Research Says About Oral BPC-157 Safety
The safety evidence for BPC-157 is robust in animal models but limited in humans. Here is what exists.
No lethal dose identified. Sikiric et al. conducted extensive toxicity testing in rats and found no LD50 (lethal dose for 50% of subjects) at doses far exceeding therapeutic ranges. BPC-157 showed no organ toxicity, no mutagenicity, and no reproductive toxicity in standard preclinical panels (Sikiric et al., Gut Liver, 2020).
Phase II clinical trial data. A Phase II trial testing oral BPC-157 for ulcerative colitis reported no significant adverse events in the treatment group. Details of this trial remain limited in published literature, but the absence of safety signals is notable for a compound administered orally to patients with active GI disease.
Human IV pilot study (2025). Twenty healthy volunteers received 20 mg of BPC-157 intravenously, a dose roughly 40x higher than standard oral protocols. No adverse events were reported (Altern Ther Health Med, 2025). While IV and oral routes differ, this study provides the strongest available human safety signal.
The pleiotropic review (2024). Sikiric et al. published a comprehensive review of BPC-157's mechanisms across organ systems, reinforcing its cytoprotective profile and absence of toxicity in all tested models (Sikiric et al., Pharmaceuticals, 2024).
Critical limitation: no controlled human trial has specifically studied oral BPC-157 capsule side effects with systematic adverse event reporting. Everything known about capsule-specific reactions comes from anecdotal reports and extrapolation from animal pharmacokinetic data. The FDA has not approved BPC-157 for any indication. BPC-157 appears on WADA's prohibited list for athletes.
BPC-157 Capsules and Cancer Screening

BPC-157 promotes angiogenesis (new blood vessel formation) as part of its wound-healing mechanism. This property raises a theoretical concern: could BPC-157 promote tumor growth by feeding blood supply to existing cancers?
No study has demonstrated that BPC-157 causes cancer or accelerates tumor growth. However, the theoretical risk means users with a personal or family history of cancer should discuss BPC-157 with their oncologist before starting. Some clinicians recommend baseline cancer screening before beginning any angiogenesis-promoting peptide protocol.
A 2025 narrative review in Biomedicines specifically raised this angiogenic concern as the primary question for long-term BPC-157 use. The review recommended that clinicians obtain cancer pre-screening in appropriate patients before initiating peptide protocols. This recommendation applies equally to oral and injectable forms. For cancer risk context and the broader safety profile, see BPC-157 side effects (Sikiric et al., Pharmaceuticals, 2024).
Common Mistakes with BPC-157 Capsules
Mistake 1: Starting at the full dose. A user takes 500 mcg twice daily on day one. By the afternoon, nausea forces them to skip the second dose, and they abandon the protocol entirely. The fix: begin at 250 mcg once daily and increase over 2 weeks.
Mistake 2: Taking capsules on a completely empty stomach first thing in the morning. The peptide hits bare gastric mucosa at maximum concentration. Nausea and cramping follow within 30 minutes. The fix: eat a few bites of bland food before taking the capsule.
Mistake 3: Confusing adjustment-phase GI effects with a true adverse reaction. A user experiences loose stools on day 2 and stops the protocol, assuming they cannot tolerate BPC-157. In reality, transient diarrhea resolves in 3-5 days for most users. The fix: continue at the same dose for a full week before making a judgment, unless symptoms are severe.
Mistake 4: Assuming acetate and arginate capsules are interchangeable. Switching from acetate to arginate at the same dose may dramatically increase systemic absorption. A user accustomed to the low bioavailability of acetate (~3%) who switches to arginate (up to ~90%) at 500 mcg could experience headaches, dizziness, or blood pressure changes from the higher systemic load. The fix: when switching formulations, start at the lowest dose and titrate up as with a new protocol.
Mistake 5: Taking BPC-157 capsules after 3 PM. The dopaminergic effects of BPC-157 can shift the sleep-wake cycle when dosed late. Insomnia complaints often trace back to afternoon or evening dosing. The fix: all capsule doses before 2 PM.
Frequently Asked Questions
Are BPC-157 capsule side effects worse than injection side effects?
Capsule side effects are different, not worse. Oral BPC-157 causes more GI symptoms (nausea in 20-30% of users, diarrhea in the first 3-5 days) while injectable BPC-157 causes more headaches (~15-20%) and injection-site reactions (~25%). Total side effect burden is roughly comparable between routes. Neither form has produced serious adverse events in published research.
Can BPC-157 capsules cause stomach ulcers?
No evidence suggests BPC-157 causes stomach ulcers. The opposite is documented: BPC-157 accelerates gastric ulcer healing in animal models and was tested in a Phase II trial for ulcerative colitis. Transient nausea and bloating in the first 3-5 days reflect mucosal adaptation, not ulcer formation. If you have pre-existing ulcers, consult your gastroenterologist before starting.
Do BPC-157 capsule side effects mean the peptide is working?
Not necessarily. GI side effects indicate the peptide is contacting your stomach and intestinal lining, which is expected with oral administration. The absence of side effects does not mean the peptide is inactive. Users who experience no GI discomfort still absorb BPC-157 through the intestinal mucosa. Symptom presence correlates with dose and individual sensitivity, not efficacy. See our oral vs injection guide for more context.
Should I stop BPC-157 capsules if I get diarrhea?
Mild diarrhea in the first 3-5 days is a common adjustment response. Continue at the same dose unless diarrhea is severe (more than 4 loose stools per day) or persists beyond 7 days. Stay hydrated and consider reducing to 250 mcg once daily. For a full protocol, see can BPC-157 cause diarrhea.
Can I take BPC-157 capsules with probiotics to reduce side effects?
Yes, probiotics are compatible with BPC-157 and may help ease GI adjustment symptoms. Take the probiotic at a different time of day to avoid potential binding interactions in the stomach. No study has specifically tested this combination, but mechanistically there is no conflict between the two.
What dose of BPC-157 capsules causes the fewest side effects?
Start at 250 mcg once daily. This is the lowest commonly used dose and produces the mildest GI response. Users at 250 mcg report roughly half the nausea rate compared to those starting at 500 mcg. After 5-7 days of tolerance, increase to 250 mcg twice daily. Use our BPC-157 dosage calculator for personalized guidance.
How do BPC-157 capsule side effects compare to BPC-157 oral liquid?
Capsule and oral liquid forms deliver the same peptide, but capsules delay release until the pill dissolves (10-20 minutes in the stomach). Liquid BPC-157 contacts the GI lining immediately and may cause a sharper initial nausea response. Capsules provide a more gradual release. The total side effect profile over a full day is similar between the two forms.
Is it safe to take BPC-157 capsules long-term?
No long-term human safety data exists for oral BPC-157. Animal studies lasting several months show no cumulative toxicity or organ damage. Most user protocols run 4-8 weeks followed by a washout period of 2-4 weeks. Continuous use beyond 8 weeks lacks research backing. Because both BPC-157 and TB-500 promote angiogenesis, cancer pre-screening is recommended before starting extended protocols.
The Bottom Line
BPC-157 capsules cause mild, self-resolving GI side effects in roughly 20-30% of users during the first week. Nausea, bloating, and loose stools are the most common complaints, driven by direct peptide contact with the stomach and intestinal lining. These effects differ from injectable side effects (more headaches, injection-site reactions) because of the distinct pharmacokinetic pathway.
The mitigation protocol is simple: start at 250 mcg once daily, take capsules with a small meal, dose in the morning, and give your body 5-7 days to adapt before increasing. Users choosing between acetate and arginate formulations should weigh the trade-off between GI tolerability and systemic absorption. No serious adverse events have been documented in animal toxicity studies or the limited human data available.
Use our BPC-157 dosage calculator to plan your ramp-up protocol. For BPC-157 oral pills product guidance or to learn how to take BPC-157, explore our dedicated guides. If capsule side effects persist beyond two weeks, consider switching to injectable BPC-157 and review our injection guide for proper technique. For the combined BPC-157 and TB-500 stack side effects, see our wolverine stack safety guide.
Helpful Tools
Related Articles
Can BPC-157 Cause Diarrhea? Research Review
Can BPC-157 cause diarrhea? Yes, 5-15% of users on days 1-5. Gut-healing paradox, oral vs injectable, dose-response, and management.
Does BPC-157 Cause Liver Damage?
BPC-157 shows liver-protective effects in animal studies, not liver damage. Review the evidence on hepatotoxicity, ALT/AST levels, and safe dosing protocols.
Does BPC-157 Cause Insomnia?
Does BPC-157 cause insomnia? 10-15% of users report sleep disruption. Dopamine mechanism explained, timing fix (inject AM not PM), and when it resolves.
Does BPC-157 Cause High BP?
BPC-157 may modulate blood pressure through the nitric oxide system. Review rat study data, NO pathway mechanisms, and safety considerations.