
You are staring at a bottle of BPC-157 capsules, wondering if swallowing a peptide can possibly work when most peptides get shredded by stomach acid before they do anything useful. BPC-157 is different. BPC-157 is derived from a protein already present in human gastric juice, making it one of the only peptides that survives stomach acid intact and reaches the gut lining in active form. Oral doses of 250 to 500 mcg deliver the peptide directly to the gastrointestinal tract, where it promotes mucosal healing through VEGF upregulation and nitric oxide modulation (Sikiric et al., J Physiol Paris, 1999).
| Factor | Oral (Pills/Capsules) | Subcutaneous Injection | Nasal Spray |
|---|---|---|---|
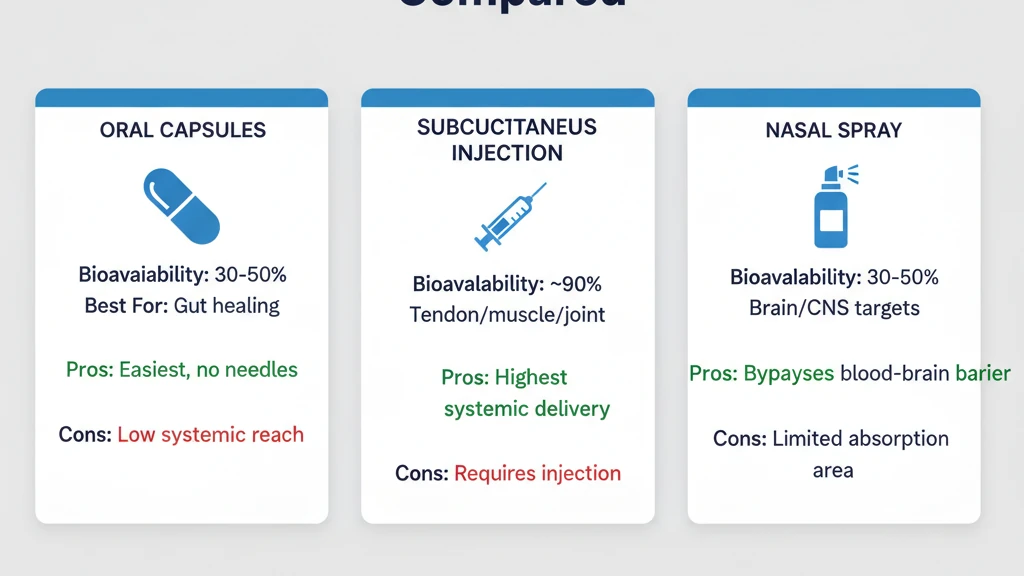
| Best for | Gut healing: IBS, leaky gut, ulcers, NSAID damage | Tendon, muscle, joint injuries, systemic repair | Brain/CNS, TBI recovery, cognitive support |
| Typical dose | 250 to 500 mcg, 1 to 2 times daily | 250 to 500 mcg per day | 200 to 500 mcg per session |
| Bioavailability (systemic) | Low to moderate (30 to 50%) | High (~90%) | Moderate (~30 to 50%) |
| Gut tissue concentration | Highest (direct contact) | Low (arrives via bloodstream) | Negligible |
| Convenience | Easiest: swallow a capsule | Requires syringe, sterile technique | Spray bottle, no needles |
| Monthly cost estimate | $50 to $120 | $40 to $100 | $40 to $80 |
| Best use case | GI tract conditions, needle-free convenience | Localized musculoskeletal injury | Neurological targets, brain delivery |
That low systemic bioavailability number scares people away from oral BPC-157. It shouldn't. For gut conditions, systemic bioavailability is irrelevant. The peptide does its work while passing through the stomach and intestines, bathing damaged tissue in direct contact. For a torn Achilles tendon, you want subcutaneous injection. For a damaged gut lining, you want the peptide in the gut. Oral puts it there.
Use the BPC-157 dosage calculator to dial in your exact dose. For the full protocol covering all three routes, see how to take BPC-157.
BPC-157 is not FDA-approved for any medical use. All dosing information reflects preclinical research and clinical observation. Consult a licensed healthcare provider before using any peptide.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
How Oral BPC-157 Survives Stomach Acid
Most peptides dissolve in gastric acid within minutes. Insulin, growth hormone, thymosin beta-4: swallow any of them and the hydrochloric acid in your stomach cleaves their peptide bonds before they reach the intestines. This is why nearly all therapeutic peptides require injection.
BPC-157 breaks this rule. The peptide is a 15-amino-acid fragment isolated from Body Protection Compound, a protein naturally secreted in human gastric juice. Think of it like a fish that evolved in saltwater. Drop a freshwater fish into the ocean and it dies. Drop a saltwater fish into the ocean and it thrives. BPC-157 evolved in one of the harshest chemical environments in the body: a pool of hydrochloric acid with a pH between 1.5 and 3.5.
The literal fact: BPC-157 remains stable and biologically active after prolonged exposure to gastric acid in vitro, a property confirmed across multiple studies (Sikiric et al., Curr Pharm Des, 2018). It does not require enteric coating to survive the stomach. This gastric stability is the reason oral BPC-157 is viable when oral delivery of other peptides is not.
What Oral BPC-157 Is Best For
Oral BPC-157 excels when the target tissue is the gastrointestinal tract itself. The peptide makes direct contact with damaged mucosa as it moves through the stomach and intestines, delivering higher local concentrations than injection ever could.
Gut Healing Conditions Where Oral Wins
NSAID-induced gastric damage. Ibuprofen, naproxen, and aspirin erode the stomach lining over time. BPC-157 administered orally counteracted gastric lesions caused by NSAIDs in multiple rat studies, accelerating mucosal repair and reducing ulcer size (Sikiric et al., Life Sci, 1994). The peptide contacts the damaged tissue directly as it passes through the stomach.
Inflammatory bowel conditions (IBS, Crohn's, ulcerative colitis). Oral BPC-157 reduced inflammation markers and improved tissue healing in rat models of colitis (Sikiric et al., J Physiol Paris, 1999). The peptide reaches the colon intact, where it upregulates VEGF and promotes new blood vessel formation in damaged intestinal walls. For more on peptide approaches to gut conditions, see peptides for gut health.
Leaky gut (intestinal permeability). A compromised intestinal barrier allows bacteria and undigested food particles to enter the bloodstream. BPC-157 promotes tight junction protein expression and mucosal integrity in animal models. Oral delivery coats the entire intestinal surface, addressing damage along the full length of the GI tract rather than relying on systemic circulation to deliver the peptide from a distant injection site.
Gastric and duodenal ulcers. BPC-157 accelerated healing of both gastric and duodenal ulcers in rats when administered orally, performing comparably to standard anti-ulcer drugs in some models (Sikiric et al., J Physiol Paris, 1999).
What Oral BPC-157 Is NOT Good For
Localized tendon and ligament injuries. A torn rotator cuff, Achilles tendinopathy, or knee ligament sprain needs the peptide at the injury site. Oral BPC-157 delivers only 30 to 50% bioavailability systemically, and even less reaches a specific peripheral tissue. For tendon injuries, inject subcutaneously near the injury at 250 to 500 mcg per day.
Muscle tears and joint injuries. Same principle. The damaged tissue is far from the GI tract. Injectable BPC-157 at 90% bioavailability delivers roughly 2 to 3 times more peptide to a distant injury site than the same oral dose. For musculoskeletal targets, see BPC-157 vs TB-500 for stacking options.
Brain and CNS targets. Oral BPC-157 delivers negligible amounts to the brain. The blood-brain barrier blocks most peptides that enter systemic circulation. For neurological goals, the nasal spray route bypasses the BBB via the olfactory pathway.
Oral BPC-157 Dosing Protocol
No human clinical trial has established an optimal oral BPC-157 dose. Current dosing derives from animal studies scaled using FDA body surface area conversion, compounding pharmacy practice, and clinical observation. The standard range is 250 to 500 mcg per dose, taken once or twice daily.
| Goal | Dose per Session | Frequency | Timing | Cycle Length |
|---|---|---|---|---|
| Mild gut maintenance | 250 mcg | Once daily | Morning, empty stomach | 4 to 6 weeks |
| Active IBS or leaky gut | 500 mcg | Twice daily | Morning + evening, empty stomach | 6 to 8 weeks |
| NSAID damage repair | 500 mcg | Twice daily | Morning + evening, empty stomach | 4 to 8 weeks |
| Gastric/duodenal ulcer support | 500 mcg | Twice daily | 30 min before meals | 6 to 8 weeks |
| Combined oral + injectable | 250 to 500 mcg oral + 250 to 500 mcg injected | Once daily each route | Oral on empty stomach; inject near injury | 4 to 8 weeks |
Take oral BPC-157 on an empty stomach. Food in the stomach dilutes the peptide and may reduce direct mucosal contact time. Wait at least 30 minutes before eating after dosing.
Start at 250 mcg once daily for the first 3 to 5 days. If tolerated without GI discomfort, increase to 500 mcg or add a second daily dose. The BPC-157 dosage calculator can help verify your protocol.
Animal studies used oral doses of 10 mcg/kg in rats for gastric protection (Sikiric et al., Life Sci, 1994). FDA body surface area conversion to humans yields approximately 1.6 mcg/kg, or roughly 100 to 130 mcg for a 70 to 80 kg adult. The 250 to 500 mcg clinical range provides a margin above this minimum to account for variable absorption.
Capsules vs. Liquid Sublingual: Which Oral Form Works Better
Two oral forms dominate the market: enteric-coated capsules and liquid sublingual drops. They deliver BPC-157 through different mechanisms, and the choice depends on your target.
Enteric-Coated Capsules
Enteric coating resists stomach acid and dissolves in the alkaline environment of the small intestine (pH 6 to 7.4). The capsule releases its BPC-157 payload in the duodenum and jejunum rather than the stomach.
This matters if your condition is intestinal rather than gastric. For IBS, leaky gut, or Crohn's affecting the small or large intestine, enteric-coated capsules deliver more peptide to the target tissue. For stomach ulcers or NSAID-induced gastric damage, enteric coating actually works against you by skipping the stomach entirely.
Capsules are the most convenient oral form. No taste, no preparation, no refrigeration during the day. Shelf life of properly stored capsules exceeds reconstituted liquid by months.
Liquid Sublingual Drops
Sublingual delivery places liquid BPC-157 under the tongue, where the peptide absorbs through the thin mucosa into the bloodstream. This route partially bypasses the GI tract and avoids first-pass liver metabolism.
For systemic effects (not gut-specific), sublingual may deliver slightly higher bioavailability than swallowed capsules because the peptide enters the bloodstream directly. However, the sublingual mucosa has limited surface area. Holding the liquid under the tongue for 60 to 90 seconds is essential. Swallowing too early converts it to standard oral dosing.
Sublingual BPC-157 tastes bitter. Some products add flavoring, which may affect peptide stability. Check that the formulation uses bacteriostatic water or a validated carrier, not a proprietary flavored base with unknown preservatives.
Which to Choose
For stomach conditions (gastric ulcers, NSAID damage): standard capsules without enteric coating, or liquid swallowed directly. You want the peptide in the stomach.
For intestinal conditions (IBS, leaky gut, Crohn's): enteric-coated capsules. You want the peptide to survive the stomach and release in the intestines.
For systemic effects without injection: sublingual liquid. You want the peptide in the bloodstream, not the gut.
For the broadest gut coverage: standard capsule without enteric coating. The peptide contacts the stomach lining first, then continues through the intestines. This is the most common choice for general GI support.
Quality, Sourcing, and Stability Concerns
The oral BPC-157 market has a quality problem. Capsules and sublingual products are easier to manufacture than injectable-grade lyophilized powder, which means more companies enter the space with lower standards. A poorly made BPC-157 capsule may contain degraded peptide, incorrect doses, or filler that interferes with absorption.
What to Look For in a BPC-157 Oral Product
Third-party certificate of analysis (COA). The COA should confirm peptide purity above 98% via HPLC testing and verify the exact milligram content per capsule. Request the COA before purchasing. A company that cannot produce one is selling an untested product. For general sourcing guidance, see where to buy peptides in 2026.
Proper storage instructions. BPC-157 degrades with heat and light exposure. Capsules should be stored in a cool, dark environment. Liquid sublingual products require refrigeration after opening. Any product shipped without temperature control during summer months may arrive partially degraded.
No proprietary blends. Some companies list "BPC-157 complex" or "gastric peptide blend" without disclosing the exact BPC-157 content. You cannot dose accurately without knowing the exact micrograms per capsule.
Stability Over Time
Lyophilized (freeze-dried) BPC-157 powder is the most stable form. Stored at room temperature in a sealed vial, it maintains potency for 12 to 24 months. Once reconstituted into liquid, shelf life drops to 28 days refrigerated.
Pre-made capsules fall between these extremes. The peptide is typically mixed with a carrier powder and sealed in a gelatin or vegetarian capsule. Exposure to moisture inside the capsule can initiate degradation. Quality manufacturers use desiccant packets and moisture-barrier packaging.
Pre-made sublingual liquids degrade fastest. Peptide in solution is less stable than peptide in dry form. Refrigerate immediately after opening and use within the timeframe on the label. If the liquid develops cloudiness or an unusual odor, discard it.
What Happens When You Choose the Wrong Route
Scenario 1: Oral BPC-157 for a knee injury. A user takes 500 mcg of oral BPC-157 daily for 6 weeks to heal a patellar tendon injury. Systemic bioavailability is roughly 30 to 50%, meaning 150 to 250 mcg reaches circulation. Of that, a fraction arrives at the knee. After 6 weeks, the tendon shows minimal improvement. The same 500 mcg injected subcutaneously near the knee would have delivered approximately 450 mcg to systemic circulation, with a higher concentration reaching the patellar tendon due to local depot effect. The fix: inject near the injury for musculoskeletal targets. Reserve oral for the gut.
Scenario 2: Enteric-coated capsules for a stomach ulcer. A user buys enteric-coated BPC-157 capsules to heal a gastric ulcer. The enteric coating is designed to resist stomach acid and dissolve in the intestines. The capsule passes through the stomach intact, releasing BPC-157 in the duodenum. The stomach ulcer receives no direct peptide contact. Six weeks of dosing produces minimal improvement. The fix: use non-enteric capsules or liquid BPC-157 swallowed directly for gastric (stomach) conditions. Save enteric-coated capsules for intestinal targets below the stomach.
Scenario 3: Swallowing sublingual drops immediately. A user places sublingual BPC-157 under the tongue but swallows within 10 seconds because of the bitter taste. The peptide enters the stomach as a diluted oral dose rather than absorbing through the sublingual mucosa. Systemic bioavailability drops to standard oral levels (30 to 50%) instead of the higher sublingual absorption. The fix: hold under the tongue for 60 to 90 seconds minimum. The bitterness fades after 20 seconds.
Combining Oral and Injectable BPC-157
Oral and injectable BPC-157 are not competing routes. They target different tissues. Running both simultaneously is a valid strategy when you have both gut and musculoskeletal issues to address.
A common combined protocol: 250 to 500 mcg oral on an empty stomach for gut healing, plus 250 to 500 mcg injected subcutaneously near an injury for tissue repair. Both doses are taken once daily. The total daily BPC-157 intake of 500 to 1000 mcg falls within the ranges studied in preclinical research. No published study reports adverse interactions between oral and injectable BPC-157, because the active compound is identical regardless of route.
The combined approach suits users recovering from gut damage caused by chronic NSAID use for a musculoskeletal injury. The oral dose heals the stomach lining the NSAIDs eroded. The injectable dose heals the tendon or joint that prompted the NSAIDs in the first place. For stacking with other healing peptides, see BPC-157 benefits and BPC-157 vs TB-500.
Frequently Asked Questions
Do BPC-157 pills actually work?
Yes, for gut-specific conditions. BPC-157 is gastric acid stable, meaning it survives the stomach and reaches intestinal tissue intact. Oral BPC-157 accelerated healing of gastric ulcers and reduced colitis markers in rat models (Sikiric et al., J Physiol Paris, 1999). For gut healing, oral delivery provides higher local tissue concentration than injection. For musculoskeletal injuries, injectable is more effective.
What is the correct BPC-157 oral dosage?
The standard range is 250 to 500 mcg per dose, taken once or twice daily on an empty stomach. For active gut conditions like IBS or ulcers, 500 mcg twice daily is common. Start at 250 mcg once daily for 3 to 5 days, then increase. Wait 30 minutes before eating after dosing. No human clinical trial has established a definitive oral dose.
Is BPC-157 oral as effective as injection?
It depends on the target. For gut healing (IBS, leaky gut, ulcers, NSAID damage), oral is more effective because the peptide contacts the damaged tissue directly. For tendon, muscle, and joint injuries, injection is superior, delivering roughly 90% bioavailability versus 30 to 50% orally. Each route serves a different purpose.
Should I take BPC-157 capsules or sublingual liquid?
For gut conditions, capsules deliver the peptide directly to the GI tract. For systemic effects without injection, sublingual liquid absorbs through the mucosa under the tongue, partially bypassing the gut. For stomach ulcers, use non-enteric capsules. For intestinal conditions, use enteric-coated capsules. For systemic goals, sublingual held for 60 to 90 seconds.
Can I take BPC-157 pills and inject at the same time?
Yes. Oral and injectable BPC-157 target different tissues with no known interaction. A common protocol is 250 to 500 mcg oral for gut healing plus 250 to 500 mcg injected near a musculoskeletal injury, both once daily. Total daily intake of 500 to 1000 mcg falls within preclinical study ranges.
How long does oral BPC-157 take to work for gut healing?
Most users report initial symptom improvement within 1 to 3 weeks. Measurable healing of gastric or intestinal tissue typically requires 4 to 8 weeks. In rat models, oral BPC-157 showed significant gastric ulcer size reduction within 14 days (Sikiric et al., Life Sci, 1994). Plan for a minimum 4-week commitment before evaluating results.
Does BPC-157 need to be taken on an empty stomach?
Yes. Food dilutes the peptide in gastric fluid and reduces direct mucosal contact time. Take BPC-157 capsules or liquid at least 30 minutes before eating. Morning dosing before breakfast is the most common approach. If taking twice daily, the second dose works well 2 to 3 hours after dinner, before bed.
Are BPC-157 oral pills safe?
BPC-157 has shown no lethal dose in any published animal study across any route. The first human safety trial found no adverse effects from 10 mg and 20 mg intravenous BPC-157 infusions (Staresinic et al., 2025). Common oral side effects are mild: occasional nausea, loose stools, or GI discomfort in the first few days. BPC-157 is not FDA-approved for any medical use.
The Bottom Line
Oral BPC-157 pills and capsules work for one specific category of conditions: gut healing. The peptide's unique gastric acid stability means it survives the stomach and coats the entire GI tract in active form, delivering higher local concentrations to damaged mucosa than any injectable dose could match.
For IBS, leaky gut, NSAID-induced gastric damage, and ulcers, oral BPC-157 at 250 to 500 mcg twice daily on an empty stomach is the preferred route. For tendon, muscle, and joint injuries, subcutaneous injection remains superior. For brain and CNS targets, nasal spray bypasses the blood-brain barrier. Each route serves a different tissue. Choosing the right one for your condition is the difference between a successful protocol and a wasted one. Use the BPC-157 dosage calculator to verify your protocol, and the peptide cost calculator to compare monthly expenses across delivery methods.
Related guides: - How to Take BPC-157 - complete protocol covering injection, oral, nasal, dose, cycle, and stacking - How to Inject BPC-157 - step-by-step injection technique and site selection - BPC-157 Nasal Spray Guide - preparation, dosage, and brain delivery - BPC-157 Benefits - full overview of research-backed effects - Peptides for Gut Health - comparison of gut-targeting peptides - BPC-157 vs TB-500 - choosing and stacking healing peptides - BPC-157 Profile - mechanism of action and research summary
Related Articles
Peptides for Gut Health: 5 Best
BPC-157, KPV, LL-37, collagen peptides, and larazotide for gut healing. Condition-specific protocols for IBS, leaky gut, Crohn's, and bloating.
How Long Does BPC-157 Take to Work?
BPC-157 timelines: gut healing 1-2 weeks, pain relief 1-2 weeks, tendon repair 4-8 weeks, bone healing 6-12 weeks. Factors that speed results.
BPC-157 Oral vs Injection: Which Route to Pick
BPC-157 oral vs injection: 80-95% injectable bioavailability vs 3-90% oral. PK data, condition matrix, combo protocol, and cost breakdown.
BPC-157 TB-500 Capsules: Oral Blend Guide
BPC-157 TB-500 capsules: oral bioavailability data, dosage protocols, side effects, and buyer checklist. TB-500 oral evidence gap explained.