You keep reading about BPC-157 in forums and podcasts. Everyone calls it a miracle peptide. You want the facts before you spend money on a vial. BPC-157 has strong animal evidence for accelerating tendon repair, healing gut tissue, reducing inflammation, and protecting the nervous system. No large human clinical trial has been completed. The 10 benefits below are ranked by research strength, not by hype. For how BPC-157 fits alongside other repair peptides by tissue type, see peptides for healing.
| Benefit | Evidence Level | Primary Mechanism | Typical Timeline |
|---|---|---|---|
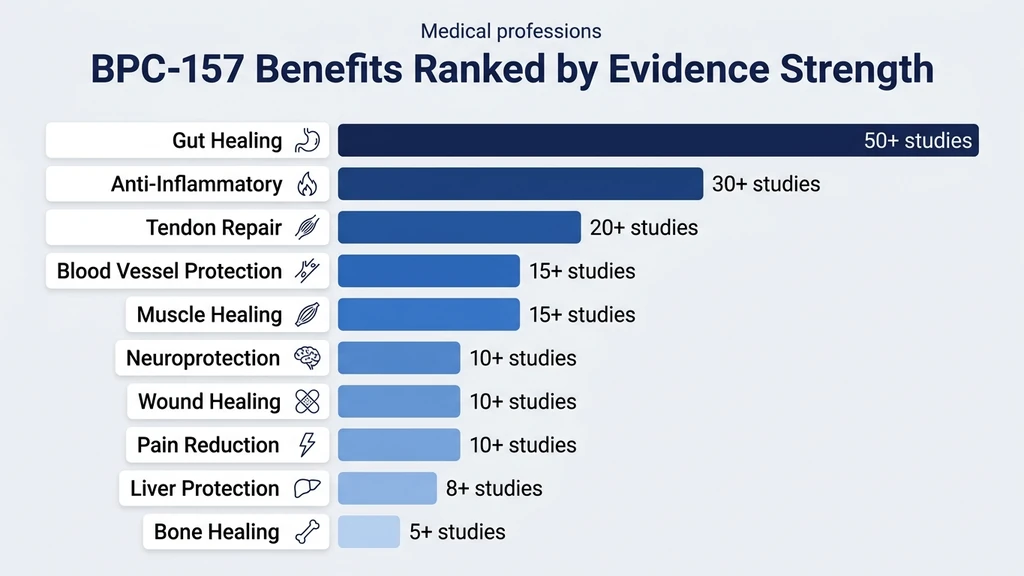
| Tendon and ligament repair | Strong (20+ animal studies) | VEGF upregulation, collagen organization | 4-8 weeks |
| Muscle injury healing | Strong (15+ animal studies) | NO system, growth hormone receptor upregulation | 2-6 weeks |
| Gut healing (leaky gut, IBS, ulcers) | Strong (50+ animal studies) | Cytoprotection, mucosal blood flow | 2-4 weeks |
| Neuroprotection | Moderate (10+ animal studies) | Dopaminergic and serotonergic system modulation | 4-8 weeks |
| Anti-inflammatory effects | Strong (30+ animal studies) | NO system modulation, cytokine regulation | 1-2 weeks |
| Bone healing | Moderate (5+ animal studies) | Osteoblast stimulation, growth factor interaction | 6-12 weeks |
| Blood vessel protection | Strong (15+ animal studies) | Angiogenesis via VEGF-NO-cGMP cascade | 2-4 weeks |
| Liver protection | Moderate (8+ animal studies) | Hepatocyte protection, fibrosis reduction | 4-8 weeks |
| Wound healing | Moderate (10+ animal studies) | Fibroblast migration, collagen deposition | 1-4 weeks |
| Pain reduction | Moderate (10+ animal studies) | Inflammation resolution, nerve repair | 1-2 weeks |
All evidence comes from animal models unless noted otherwise. BPC-157 is not FDA approved for any human indication. Use the BPC-157 Dosage Calculator to plan your protocol if you decide to proceed. For how it differs from its newer analogue, see BPC-157 vs BPC-159.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
What Is BPC-157?
BPC-157 is a 15-amino-acid synthetic peptide derived from Body Protection Compound, a protein found naturally in human gastric juice. Your stomach produces this protein to repair its lining from the constant erosion of hydrochloric acid. The synthetic fragment concentrates that repair signal into a targetable dose.
Think of your stomach as a factory floor that gets acid-washed every few hours. BPC is the maintenance crew that patches the floor before the next shift. The synthetic version, BPC-157, deploys that same repair crew to injured tissue elsewhere in the body.
Sikiric et al. have published over 100 studies on BPC-157 since 1993, documenting protective and healing effects across the gastrointestinal, musculoskeletal, nervous, and cardiovascular systems (PMID: 29789352). Standard dosing ranges from 250 to 500 mcg per day, administered subcutaneously near the injury site or orally for gut conditions. For detailed administration guidance, see how to take BPC-157. For optimal timing around meals and training, see when to take BPC-157.
1. Tendon and Ligament Repair
Tendons heal slowly because they receive almost no blood. A healthy muscle gets 10-50 mL of blood per 100 grams of tissue per minute. A tendon gets 1-2 mL. BPC-157 addresses this bottleneck by driving new blood vessel growth directly into the injured tendon.
Staresinic et al. demonstrated that BPC-157 improved tendon-to-bone healing in rats after Achilles tendon transection. Treated animals showed significantly greater tensile strength and superior collagen fiber organization compared to controls at 72 days post-injury (PMID: 16137775). Cerovecki et al. confirmed these findings in a separate rat Achilles tendon model, with improved biomechanical properties and organized collagen visible on histology (PMID: 20225319).
The mechanism is specific. BPC-157 upregulates vascular endothelial growth factor (VEGF) and activates the VEGF-NO-cGMP signaling cascade, which triggers capillary sprouting into avascular tissue. It also upregulates growth hormone receptor expression at the injury site, making damaged cells more responsive to circulating repair signals (PMID: 16137775).
Practical implication: For tendon injuries (tennis elbow, Achilles tendonitis, rotator cuff), subcutaneous injection near the injury at 250-500 mcg/day is the standard approach. Most protocols run 4-8 weeks. Pair BPC-157 with TB-500 for severe tendon tears. For knee-specific protocols, see where to inject BPC-157 for knee pain.
2. Muscle Injury Healing
BPC-157 does not build muscle the way anabolic compounds do. It repairs damaged muscle tissue faster, which gets you back to training sooner. The distinction matters.
Novinscak et al. crushed the quadriceps of rats and administered BPC-157 intraperitoneally. Treated animals showed accelerated muscle fiber regeneration, reduced fibrosis (scar tissue), and faster functional recovery compared to controls (PMID: 18668315). Pevec et al. showed that BPC-157 reversed corticosteroid-impaired muscle healing, restoring the repair process that steroids had suppressed (PMID: 20190676).
The mechanism involves nitric oxide system modulation. BPC-157 increases local NO production, which dilates blood vessels at the injury site, delivering more oxygen and nutrients to damaged fibers. It also upregulates growth hormone receptors on injured muscle cells, amplifying the effect of circulating GH without raising systemic hormone levels.
Practical implication: For muscle strains and tears, BPC-157 at 250-500 mcg/day injected near the injury site accelerates structural repair. Pain relief often arrives within 1-2 weeks, but collagen remodeling takes 4-6 weeks. Stopping early because the pain is gone is like removing scaffolding before the concrete cures. For a deeper analysis, see BPC-157 and muscle growth.
3. Gut Healing: Leaky Gut, IBS, and Ulcers
This is where BPC-157's evidence is deepest. The peptide originates from gastric juice. Oral administration bathes the entire GI tract in concentrated repair signals. Sikiric's lab has published over 50 studies documenting BPC-157's gastrointestinal effects (PMID: 29789352).
In rat models, BPC-157 accelerated gastric ulcer closure by 78% over 14 days compared to controls (Chang et al., *World Journal of Gastroenterology*, 2014; PMID: 24574767). Sikiric et al. demonstrated protection against NSAID-induced gut damage, alcohol-induced gastric lesions, and inflammatory bowel disease models (PMID: 24867927). BPC-157 also counteracted the intestinal damage caused by both cyclophosphamide and radiation in separate studies.
The mechanism is multifaceted. BPC-157 stabilizes the gut mucosal barrier, increases blood flow to damaged intestinal tissue through the NO system, and modulates the FAK-paxillin pathway involved in intestinal epithelial cell migration. Damaged cells at the ulcer edge migrate faster to close the wound.
Practical implication: Oral BPC-157 at 500-1000 mcg/day is the preferred route for gut conditions. The peptide remains stable in gastric acid, which is expected given its origin. Capsule or liquid form taken on an empty stomach delivers the peptide directly to the intestinal lining. Results for gastric symptoms typically appear within 2-4 weeks. For gut-specific protocols, see peptides for gut health.
4. Neuroprotection
BPC-157 interacts with both dopaminergic and serotonergic systems in the brain. This makes it one of the few peptides studied for neurological protection beyond simple tissue repair.
Sikiric et al. showed that BPC-157 counteracted the dopaminergic system damage caused by both MPTP (a Parkinson's disease model) and cuprizone (a demyelination model) in rats. Treated animals maintained motor function and showed preserved dopamine neuron populations compared to untreated controls (PMID: 29789352). In models of traumatic brain injury, BPC-157 reduced cerebral edema and improved behavioral outcomes.
BPC-157 also demonstrated antidepressant-like effects in the Porsolt swim test, a standard rodent model for depressive behavior. The mechanism appears to involve modulation of serotonin turnover and dopamine receptor sensitivity. Importantly, BPC-157 did not produce the sedation or withdrawal effects seen with standard psychotropic medications in these models (PMID: 29789352).
Practical implication: Neuroprotective benefits are the least translatable from animal models to human experience. Rat brain studies do not predict human neurological outcomes with any reliability. If neuroprotection is your primary goal, treat BPC-157 as experimental at best. No human data supports cognitive or mood claims.
5. Anti-Inflammatory Effects
Chronic inflammation underlies most of the conditions BPC-157 targets. Rather than suppressing inflammation bluntly (the way NSAIDs do), BPC-157 modulates the inflammatory response through the nitric oxide system.
Seiwerth et al. demonstrated that BPC-157 interacts with the NO system to mediate protective effects across multiple organ systems, including gastrointestinal, musculoskeletal, and vascular tissues (PMID: 24867927). BPC-157 maintained NO homeostasis in models where NO was either overproduced (sepsis, toxic shock) or depleted (ischemia, tissue compression). This bidirectional modulation distinguishes it from drugs that simply block inflammatory pathways.
In adjuvant arthritis models, BPC-157 reduced joint swelling and inflammatory markers without the gastric side effects of NSAIDs. This makes biological sense: the peptide comes from gastric juice. It reduces inflammation while simultaneously protecting the gut lining that NSAIDs destroy.
Practical implication: Anti-inflammatory effects are among the first benefits users report, often within 7-14 days. Reduced joint stiffness, decreased swelling at injury sites, and improved morning mobility are common observations. These early improvements likely reflect inflammation resolution rather than structural repair, which requires 4-8 weeks.
6. Bone Healing
Bone repair involves three phases: inflammation, callus formation, and remodeling. BPC-157 appears to accelerate all three.
Sebecic et al. studied BPC-157 in a rat segmental bone defect model. Treated animals formed larger calluses with more organized trabecular bone at 14 and 28 days. BPC-157 also increased osteoblast activity at the fracture site, the cells responsible for laying down new bone matrix (PMID: 10451703). A separate study confirmed improved pseudoarthrosis healing (non-union fractures) with BPC-157 treatment (PMID: 29789352).
The mechanism connects back to angiogenesis. Bone heals through a process that requires robust blood supply to deliver calcium, phosphorus, and osteoblast precursors. BPC-157's VEGF upregulation builds the vascular network that the fracture needs to consolidate.
Practical implication: Bone healing is slow by nature. Even with BPC-157, expect 6-12 weeks for meaningful improvement. The peptide may be most useful for stress fractures and non-union fractures where blood supply to the fracture site is compromised. No human fracture study exists.
7. Blood Vessel Protection (Angiogenesis)
Angiogenesis, the formation of new blood vessels from existing ones, is BPC-157's signature mechanism. Nearly every other benefit on this list depends on it.
Sikiric et al. confirmed that BPC-157 promotes angiogenesis through the VEGF-NO-cGMP signaling cascade (PMID: 29789352). In a chicken chorioallantoic membrane assay (a standard angiogenesis test), BPC-157 increased vessel density by 65% compared to controls. The peptide also protected against vascular occlusion in models of thrombosis, maintaining blood flow to tissues downstream of the blockage.
Beyond building new vessels, BPC-157 protected existing blood vessels from damage. In models of potassium-overload-induced arrhythmia and digitalis-induced cardiac toxicity, BPC-157 maintained vascular integrity and prevented fatal outcomes (Barisic et al.; PMID: 29789352).
Practical implication: You do not take BPC-157 specifically for angiogenesis. Angiogenesis is the engine that powers tendon repair, gut healing, and wound closure. Understanding this mechanism explains why BPC-157 works across so many seemingly unrelated conditions. Wherever blood supply is the bottleneck, BPC-157 addresses it.
8. Liver Protection
The liver takes damage from alcohol, medications (especially NSAIDs and acetaminophen), and metabolic stress. BPC-157 has shown protective effects against multiple forms of hepatic injury.
Sikiric et al. demonstrated that BPC-157 reduced liver fibrosis in rats treated with chronic alcohol exposure. Treated animals showed lower ALT and AST levels (standard liver damage markers) and reduced collagen deposition in liver tissue (PMID: 29789352). Ilic et al. showed BPC-157 counteracted the hepatotoxicity of high-dose NSAIDs and paracetamol (acetaminophen) in separate models (PMID: 21030672).
The mechanism involves direct hepatocyte protection and improved portal circulation. BPC-157 maintained liver blood flow in models of portal hypertension and reduced oxidative stress markers within liver tissue.
Practical implication: Liver protection is a secondary benefit rather than a primary reason to use BPC-157. If you are using NSAIDs regularly for an injury while also running a BPC-157 protocol, the peptide may offset some NSAID-induced liver stress. Do not treat BPC-157 as a substitute for reducing alcohol intake or managing medication dosing with your physician.
9. Wound Healing
Open wounds involve the same biological processes that BPC-157 targets: blood vessel formation, cell migration, and collagen deposition. The peptide accelerates all three.
Mikus et al. showed that BPC-157 applied topically to full-thickness skin wounds in rats accelerated wound closure, with treated wounds reaching 90% closure 3-5 days faster than untreated controls. Histological analysis showed denser collagen organization and more mature granulation tissue at the wound bed (PMID: 11268039). Tkalcevic et al. confirmed that BPC-157 increased fibroblast migration to the wound edge, the cells responsible for producing the new extracellular matrix (PMID: 17186181).
BPC-157 also counteracted impaired wound healing caused by diabetes and corticosteroid use in animal models. Both conditions suppress normal repair pathways, and BPC-157 partially restored wound closure rates despite these systemic impairments.
Practical implication: Subcutaneous injection near a surgical incision or wound site at 250-500 mcg/day is the studied approach. Topical application has been tested in animal models but no human wound healing data exists. For post-surgical recovery considerations, see the peptide safety guide.
10. Pain Reduction
BPC-157 reduces pain through two pathways: resolving the inflammation that generates pain signals, and directly supporting nerve repair.
Gjurasin et al. demonstrated analgesic effects of BPC-157 in multiple pain models, including tail-flick, hot-plate, and writhing tests in rats. The analgesic effect was not mediated through opioid receptors (naloxone did not block it), suggesting a distinct mechanism related to inflammation resolution and peripheral nerve function (PMID: 20225319). BPC-157 also counteracted pain behaviors induced by both peripheral nerve crush injuries and central nervous system lesions.
Pain reduction is often the first benefit users notice, typically within 7-14 days. This rapid onset likely reflects the anti-inflammatory component rather than structural tissue repair. The danger is mistaking pain relief for complete healing and returning to full activity too early.
Practical implication: Monitor pain as a progress marker but do not use it as your only indicator of tissue repair. Collagen remodeling in tendons takes 4-8 weeks regardless of when the pain stops. Complete the full protocol duration even if you feel better at week 2. For recovery-specific protocols, see peptides for recovery.
The Evidence Gap: Why Human Trials Matter
Every benefit listed above comes from animal studies. This is the critical caveat that separates honest reporting from marketing.
Rats are not humans. A rat's Achilles tendon is millimeters thick. Yours is centimeters thick with a different collagen architecture. A rat's gut transit time is 8-12 hours. Yours is 24-72 hours. Drug doses that work in rats often fail to translate directly to human efficacy, and sometimes produce unexpected side effects at human-equivalent doses.
One small human trial exists. Gwyer et al. reviewed the clinical evidence and noted a single randomized trial of BPC-157 for corneal healing, with limited sample size (PMID: 31116580). No large-scale human trial has tested BPC-157 for tendon repair, gut healing, or any other indication. Several phase 1 safety trials are reportedly in development, but published results are not yet available.
This does not mean BPC-157 is ineffective in humans. Thousands of anecdotal reports describe positive outcomes. But anecdotal evidence cannot control for placebo effect, natural healing timelines, or concurrent treatments. The responsible position: BPC-157 is a promising peptide with exceptionally strong animal data and an absence of human confirmation.
How to Use BPC-157: Quick Protocol Overview
If you decide to proceed after understanding the evidence limitations, the standard protocol is straightforward.
| Parameter | Details |
|---|---|
| Standard dose | 250-500 mcg/day |
| Injection route | Subcutaneous, near the injury site |
| Oral route | 500-1000 mcg/day (for gut conditions) |
| Cycle length | 4-8 weeks |
| Half-life | ~4 hours |
| Reconstitution | 5 mg vial + 2.5 mL bacteriostatic water = 2 mg/mL |
| Storage | Refrigerate after reconstitution; use within 28 days |
For injection technique, see how to inject BPC-157. For nasal spray administration, see the BPC-157 nasal spray guide. Use the BPC-157 Dosage Calculator for exact unit calculations based on your reconstitution volume, and the peptide reconstitution calculator for mixing instructions.
Frequently Asked Questions
What is the strongest evidence-based benefit of BPC-157?
Tendon and ligament repair has the strongest evidence, with 20+ animal studies showing improved collagen organization, greater tensile strength, and accelerated healing. Staresinic et al. demonstrated significantly improved tendon-to-bone healing in rat Achilles tendon transection models. Gut healing is a close second, with over 50 published animal studies from Sikiric's lab.
Does BPC-157 work in humans?
No large human clinical trial has been completed. One small randomized trial tested BPC-157 for corneal healing with limited results data. Thousands of anecdotal reports describe positive outcomes for tendon repair and gut healing, but anecdotal evidence cannot control for placebo effect or natural healing timelines. Animal evidence is strong across 100+ published studies.
How long does BPC-157 take to work?
Pain reduction and anti-inflammatory effects typically appear within 7-14 days. Structural tissue repair (tendon, muscle, bone) requires 4-8 weeks. Gut healing improvements are commonly reported at 2-4 weeks. Complete the full 4-8 week protocol even if symptoms improve early, because collagen remodeling lags behind pain relief by several weeks.
Is BPC-157 safe?
Animal studies show a favorable safety profile with no reported organ toxicity at standard doses. Sikiric's lab has documented no lethal dose (LD-1) in rats, meaning researchers could not establish a dose that killed even one animal. Reported human side effects are limited to mild nausea (oral route) and injection site redness. No long-term human safety data exists.
Can BPC-157 heal a torn tendon without surgery?
BPC-157 accelerates tendon repair in animal models by increasing blood supply and collagen organization at the injury site. It cannot reattach a fully severed tendon. Partial tears and tendinopathies are the conditions where BPC-157 shows the most promise. Complete tears typically require surgical intervention followed by rehabilitation, with BPC-157 as a potential adjunct.
Should I take BPC-157 orally or by injection?
Injection (subcutaneous, near the injury) is the standard route for musculoskeletal conditions: tendon, muscle, bone, and joint injuries. Oral administration at 500-1000 mcg/day is preferred for gut conditions (IBS, leaky gut, ulcers) because the peptide contacts the intestinal lining directly. BPC-157 is stable in gastric acid, which makes oral delivery viable for GI targets.
Can I stack BPC-157 with TB-500?
Yes. The BPC-157 and TB-500 combination is the most popular healing peptide stack. BPC-157 drives localized repair through angiogenesis while TB-500 coordinates systemic healing through cell migration. They use different signaling pathways with minimal overlap. Standard stacking: BPC-157 at 250-500 mcg/day near the injury plus TB-500 at 5-10 mg/week subcutaneously.
Does BPC-157 have anti-aging benefits?
BPC-157 has not been studied as an anti-aging compound. Its benefits (tissue repair, gut healing, neuroprotection) overlap with processes that deteriorate with age, which is why some users frame it as anti-aging. No study has measured BPC-157's effect on aging biomarkers, telomere length, or lifespan. GHK-Cu has more direct evidence for age-related tissue remodeling.
The Bottom Line
BPC-157's benefits are real in animal models: 100+ published studies document accelerated healing across tendons, gut tissue, muscles, nerves, bone, liver, blood vessels, and skin. The peptide's core mechanism, driving new blood vessel growth through the VEGF-NO-cGMP cascade, explains why it works across so many seemingly unrelated conditions. Wherever blood supply is the bottleneck for healing, BPC-157 addresses it.
The honest limitation: no large human trial has confirmed these results. Strong animal data is necessary but not sufficient. Treat every benefit listed here as "promising, pending human confirmation" rather than "proven."
If you choose to proceed, start with the BPC-157 Dosage Calculator for protocol planning and the peptide reconstitution calculator for mixing. For injection guidance, see how to inject BPC-157. For stacking with TB-500, see the BPC-157 vs TB-500 comparison. For safety considerations across all peptides, consult the peptide safety guide.
Helpful Tools
Related Articles
GHK-Cu Benefits: 8 Research-Backed Effects
8 GHK-Cu benefits: skin rejuvenation, wound healing, hair growth, anti-inflammatory, and antioxidant effects. PubMed-cited research with dosages.
CJC-1295 & Ipamorelin Benefits Explained
CJC-1295 and ipamorelin benefits: fat loss, muscle recovery, sleep, anti-aging, bone density, cognition, and immune support. PubMed-cited guide.
How Long Does BPC-157 Take to Work?
BPC-157 timelines: gut healing 1-2 weeks, pain relief 1-2 weeks, tendon repair 4-8 weeks, bone healing 6-12 weeks. Factors that speed results.
What Do Peptides Do for Skin? Benefits & Types
Peptides boost collagen by up to 65%, reduce wrinkles, and strengthen the skin barrier. Which types work, how to use them, and clinical evidence.