You are sitting on the edge of your bed with a loaded syringe of BPC-157 and a sore knee. Your MCL aches. Your patellar tendon throbs after every run. You know the dose. You have no idea where to stick the needle.
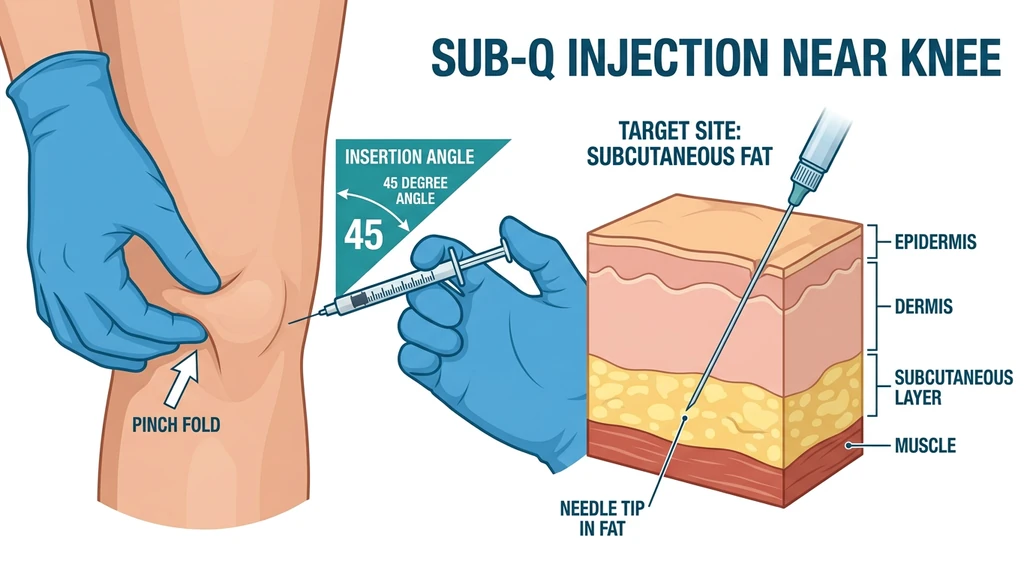
Inject subcutaneously within 1-3 cm of the injured structure. Pinch the skin near the injury, insert at 45 degrees, and deliver the peptide into the fat layer beneath the skin. A 2025 systematic review of 36 studies confirmed BPC-157 improved structural and biomechanical outcomes in ligament, tendon, muscle, and bone injuries. The one human knee study, Lee et al. (2021), found 7 of 12 patients maintained pain relief beyond 6 months after direct knee injection.
Find your injury in the table below and inject at the corresponding site.
| Knee Injury | Primary Injection Site | Secondary Site | Route |
|---|---|---|---|
| ACL tear/strain | Medial and lateral to patellar tendon | Posterior knee (popliteal fossa) | Subcutaneous |
| MCL sprain | Medial (inner) knee along joint line | Above/below medial epicondyle | Subcutaneous |
| LCL sprain | Lateral (outer) knee along joint line | Above/below lateral epicondyle | Subcutaneous |
| Patellar tendinopathy | Directly below kneecap (inferior pole) | Medial/lateral to patellar tendon | Subcutaneous |
| Meniscus tear | Medial or lateral joint line (side of tear) | Opposite joint line | Subcutaneous |
| General knee pain | Rotate all four quadrants around kneecap | Lower abdomen (systemic) | Subcutaneous |
Use the BPC-157 Dosage Calculator to determine the correct dose for your body weight and injury severity.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
Why Injection Location Matters for Knee Injuries
Think of BPC-157 like fertilizer on a garden. Scatter it across an entire acre and each plant gets a trace amount. Pour it at the base of the one plant that needs help and that plant gets a concentrated dose. The peptide works the same way: inject near the damaged ligament, and the tissue bathes in a high local concentration. Inject in your abdomen, and that same dose dilutes across your entire bloodstream before a fraction reaches the knee.
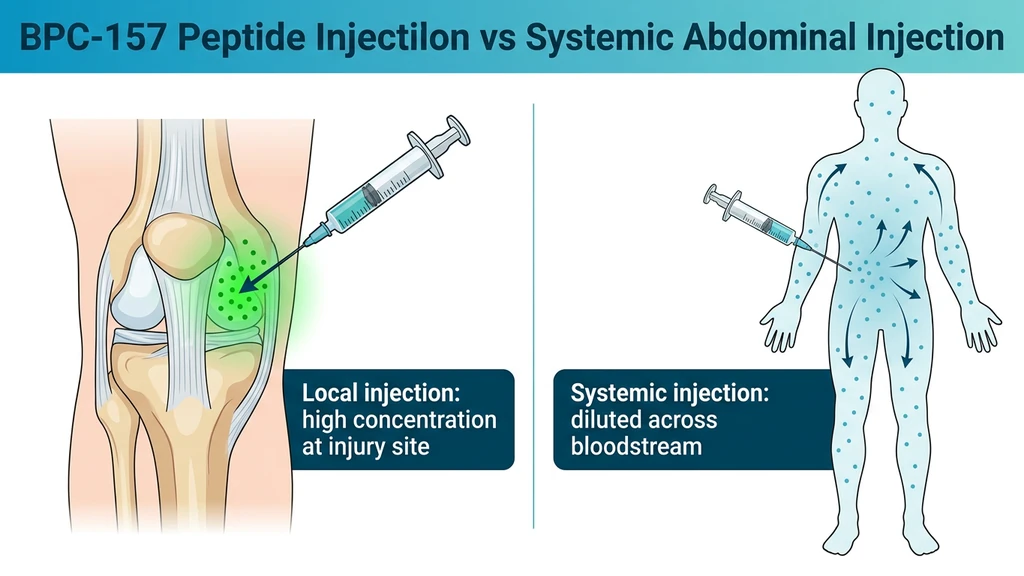
Cerovecki et al. (2010) proved this in a rat MCL transection model. BPC-157 applied locally at the injury site improved ligament healing across functional, biomechanical, macroscopic, and histological measures over 90 days. Systemic administration also worked, but local delivery produced the strongest results consistently.
Chang et al. (2011) showed BPC-157 promotes tendon fibroblast outgrowth, cell survival under oxidative stress, and cell migration through the FAK-paxillin signaling pathway. These effects are concentration-dependent: higher local levels mean more fibroblast activation at the injury.
The rule is simple. Inject as close to the injured structure as you can safely reach with a subcutaneous needle. You do not need to penetrate the joint capsule. Subcutaneous fat surrounding the knee provides adequate proximity for peptide diffusion to deeper structures.
Local vs. Systemic Injection: When to Use Each
Local subcutaneous injection near the knee is the default for any identified knee injury. Systemic injection (lower abdomen or upper thigh) supplements it; it does not replace it.
Use local knee injection when: - You have a specific, localized injury (torn ACL, MCL sprain, patellar tendinopathy, meniscus tear) - Pain concentrates in one area of the knee - You can identify the approximate location of the damaged structure
Use systemic injection when: - You have diffuse knee pain without a clear source - Multiple structures are involved (post-surgical, advanced osteoarthritis) - You are stacking BPC-157 with TB-500 for broader systemic repair - You cannot tolerate injections near the knee
Split protocol: Some users inject 60-70% of their daily dose locally near the knee and the remaining 30-40% subcutaneously in the abdomen. No published study has tested this split approach directly, but the pharmacological logic holds: maximize both local concentration and systemic delivery.
What Happens When You Inject in the Wrong Place
Two scenarios show why injection site matters as much as dose.
Scenario 1: Abdominal injection for a patellar tendon injury. You inject 500 mcg of BPC-157 subcutaneously in your abdomen. The peptide enters systemic circulation and distributes across roughly 5 liters of blood volume. By the time it reaches your patellar tendon, the local concentration is a small fraction of the injected dose. Chang et al. (2011) demonstrated that BPC-157's fibroblast activation through the FAK-paxillin pathway is dose-dependent. Lower local concentration means less tendon cell migration, less outgrowth, and slower repair. After 8 weeks, you see minimal improvement and conclude the peptide does not work. The fix: inject 1-2 cm below the kneecap, directly over the patellar tendon.
Scenario 2: Injecting into the joint space without training. You read that Lee et al. (2021) used intra-articular injection and decide to replicate it. You push the needle past the subcutaneous layer and into the joint capsule. Without proper anatomical landmarks and sterile technique, you risk introducing bacteria into a synovial space where infection (septic arthritis) can destroy cartilage within 24-48 hours. Septic arthritis requires emergency IV antibiotics and often surgical drainage. The fix: stay subcutaneous. Pinch the skin, insert at 45 degrees, stop in the fat layer. The peptide diffuses inward on its own.
Exact Injection Sites by Knee Injury Type
Each knee structure sits in a different anatomical position. The injection site should be the closest accessible subcutaneous tissue to the damaged structure.
For all sites: you are injecting into the subcutaneous fat layer. The needle tip sits in the soft tissue just beneath the skin. Not in the joint, not in the muscle, not in the tendon.
ACL Tear or Strain
The anterior cruciate ligament runs diagonally through the center of the knee, connecting the femur to the tibia. You cannot reach it directly with a subcutaneous needle. The goal is to surround the knee with BPC-157 so the peptide diffuses inward from multiple directions.
Primary sites: Inject subcutaneously on both the medial (inner) and lateral (outer) sides of the patellar tendon, about 1-2 cm below the lower edge of the kneecap. Alternate sides across injections.
Secondary site: The posterior knee (popliteal fossa, the soft area behind the knee). Inject subcutaneously with the knee slightly bent. This targets the posterior attachment of the ACL.
Rotation pattern: Day 1 medial, Day 2 lateral, Day 3 posterior. Repeat.
The Lee et al. (2021) human knee study used intra-articular injection (directly into the joint space), which requires clinical supervision. Subcutaneous injection around the joint is the self-administered alternative.
MCL Sprain
The medial collateral ligament runs along the inner side of the knee from the femoral epicondyle to the tibial plateau. It is the most superficial major knee ligament, making it the easiest target for subcutaneous injection.
Primary site: Inject subcutaneously along the medial (inner) joint line. Bend your knee to 90 degrees and feel the gap between the femur and tibia on the inner side. Inject 1 cm above or below this line, alternating between injections.
Secondary site: The medial epicondyle area (the bony bump on the inner side just above the joint line). This targets the femoral attachment of the MCL.
Cerovecki et al. (2010) used the MCL transection model specifically. BPC-157 treated rats showed reduced valgus instability, higher load-to-failure values, and better collagen fiber organization at 14, 30, 45, and 90 days post-injury.
LCL Sprain
The lateral collateral ligament runs along the outer side of the knee. Mirror the MCL approach on the opposite side.
Primary site: Inject subcutaneously along the lateral (outer) joint line. The LCL is a cord-like structure you can often palpate when the knee is in a figure-four position. Inject 1 cm above or below the joint line on the outer knee.
Secondary site: Near the lateral epicondyle (bony prominence on the outer knee) and the fibular head (the small bump below and to the outside of the knee).
Rotation pattern: Alternate between the upper and lower portions of the LCL across injections.
Patellar Tendinopathy (Jumper's Knee)
The patellar tendon connects the bottom of the kneecap to the tibial tuberosity (the bump below your knee). Pain typically concentrates at the inferior pole of the patella, where the tendon attaches to the kneecap.
Primary site: With the knee relaxed and extended, pinch the skin just below the patella. Insert the needle at 45 degrees into the subcutaneous tissue overlying the tendon.
Secondary sites: Medial and lateral borders of the patellar tendon, about 1 cm to each side. Rotate across three sites.
Chang et al. (2011) demonstrated BPC-157 accelerates tendon fibroblast outgrowth and migration in a dose-dependent manner. FAK-paxillin pathway activation was strongest at higher local concentrations, supporting injection close to the tendon. Staresinic et al. (2003) confirmed BPC-157 accelerated healing of transected rat Achilles tendons and stimulated tendocyte growth in vitro.
Meniscus Tear
The menisci are C-shaped cartilage pads sitting on top of the tibial plateau. Medial tears are more common. The outer third of the meniscus has blood supply (the "red zone") and responds better to healing interventions than the inner "white zone."
Primary site: Inject along the joint line on the side of the tear. For a medial meniscus tear, inject subcutaneously along the medial joint line. For a lateral tear, inject along the lateral joint line. The joint line is easiest to find with the knee bent to 90 degrees.
Secondary site: Inject on the opposite side of the same joint line, slightly anterior or posterior, to provide peptide coverage across the meniscus.
Meniscus tears in the avascular zone remain among the hardest knee injuries to treat with any intervention. BPC-157 promotes angiogenesis through VEGF upregulation, as documented by Huang et al. (2018), which may partially address limited blood supply. Large or complex tears in the white zone typically require surgery regardless of peptide use.
General Knee Osteoarthritis or Diffuse Pain
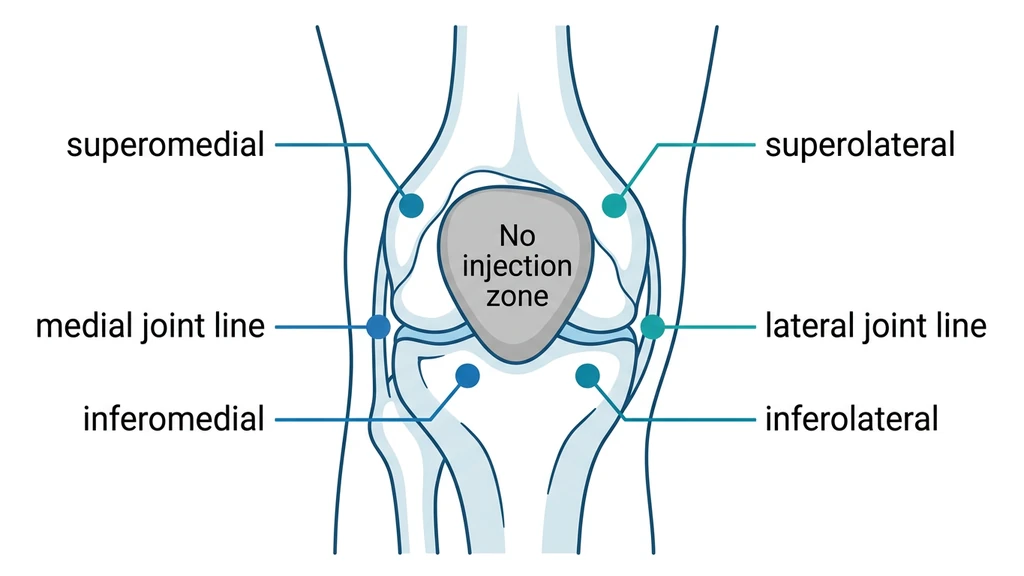
When pain is not localized to a single structure, rotate injections around all four quadrants of the knee.
| Quadrant | Location | Day |
|---|---|---|
| Superomedial | Above kneecap, inner side | Day 1 |
| Superolateral | Above kneecap, outer side | Day 2 |
| Inferomedial | Below kneecap, inner side | Day 3 |
| Inferolateral | Below kneecap, outer side | Day 4 |
Inject subcutaneously at each site, about 2-3 cm from the edge of the kneecap. This provides circumferential peptide coverage around the joint capsule.
For advanced osteoarthritis involving the entire joint, supplement local injections with a systemic abdominal injection (split the daily dose). Read the full guide on peptides for joint pain for combination strategies.
How to Find Your Injection Site by Touch
Most competitor guides tell you "inject near the MCL." They never tell you how to find the MCL with your fingers. This section gives you the tactile landmarks.
Finding the joint line. Sit with your knee bent to 90 degrees. Place your fingertips on the inner or outer side of the knee. Press gently and straighten the leg slowly. You will feel a gap close between two bones. That gap is the joint line. Mark it with a pen.
Finding the patellar tendon. Straighten your leg and tighten your quadriceps. The thick band running from the bottom of your kneecap to the bump on your shin is the patellar tendon. Relax the leg. Pinch the skin on either side of that band. Those pinchable areas are your injection sites.
Finding the popliteal fossa (posterior knee). Bend your knee to about 30 degrees. Feel the soft, fleshy area directly behind the knee between the two hamstring tendons. Avoid the exact center, where the popliteal artery runs. Inject 1-2 cm to the medial or lateral side of center.
Testing for subcutaneous depth. Pinch the skin at your chosen site. If you can lift a fold of at least 1 cm, there is enough subcutaneous tissue for a safe injection. If the skin feels tight against bone (common directly over the kneecap), move 2-3 cm laterally until you can pinch a fold.
Step-by-Step Injection Technique
For complete injection fundamentals, see the peptide injections complete guide.
Supplies
Gather everything before you start. Touching non-sterile surfaces mid-injection introduces contamination.
- Reconstituted BPC-157 vial (stored at 2-8C)
- Insulin syringe, 29-31 gauge, 0.5 inch or 8mm needle
- Alcohol swabs (70% isopropyl)
- Sharps disposal container
- Nitrile gloves (optional but recommended)
- Gauze or cotton ball for post-injection pressure
- Mirror (for posterior knee injection)
Use the Peptide Reconstitution Calculator to determine the correct amount of bacteriostatic water for your vial.
Preparation
1. Wash your hands. Soap and water, 20 seconds.
2. Wipe the vial stopper. Rub the rubber stopper with an alcohol swab. Let it air dry for 10 seconds.
3. Draw the dose. Pull back on the plunger slightly past your target mark, then push forward to the correct line to expel air bubbles.
4. Clean the injection site. Fresh alcohol swab, circular motion from center outward. Let the skin air dry for 30 seconds. Injecting through wet alcohol stings and can push bacteria into the puncture.
Injection Process
1. Position your knee. Sit with the leg relaxed. For anterior and lateral sites, keep the leg extended or slightly bent. For posterior sites, bend the knee to 30 degrees.
2. Pinch the skin. Grab a fold of skin at your injection site between your thumb and index finger. Lift it away from the underlying muscle and bone.
3. Insert the needle. Push in at a 45-degree angle. With a 29-31 gauge insulin needle, the full 8mm length places the tip in the subcutaneous fat layer.
4. Release the pinch. Let go of the skin fold once the needle is seated.
5. Inject slowly. Push the plunger over 5-10 seconds. Rapid injection increases local pressure and discomfort.
6. Wait 5 seconds. Keep the needle in place after the plunger bottoms out. This prevents peptide from tracking back through the needle path.
7. Withdraw at the same angle. Pull the needle out the way it went in. Apply gentle pressure with gauze for 10 seconds. Do not rub.
| Gauge | Diameter | Best For | Pain Level |
|---|---|---|---|
| 29G | 0.34 mm | Standard subcutaneous, most knee sites | Low |
| 30G | 0.31 mm | Thin skin areas, anterior knee | Very low |
| 31G | 0.26 mm | Minimal pain, slower draw time | Minimal |
| 27G | 0.41 mm | Viscous reconstitutions only | Moderate |
For knee injections, 29G or 30G insulin syringes are the standard choice. Avoid anything larger than 27G for subcutaneous injection.
Site Rotation Protocol
Injecting the same spot daily causes tissue irritation, scar tissue formation, and reduced absorption. Rotation is mandatory for any protocol lasting more than a few days.
Minimum rotation: Three sites around the knee. For a 4-week protocol with daily injections, use the four-quadrant system plus one or two additional sites (posterior knee, proximal patellar tendon).
Spacing: Keep injection sites at least 2 cm apart. The subcutaneous tissue around the knee provides enough surface area for 5-6 distinct sites.
Tracking: Log the date, site used, and any observations (redness, soreness, lumps). This prevents accidentally favoring one site.
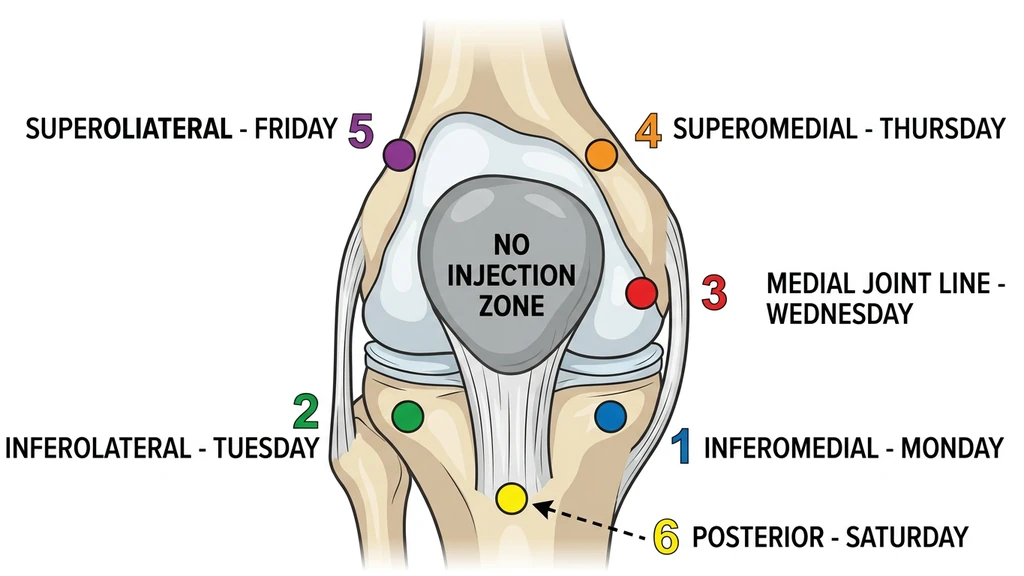
| Day | Site |
|---|---|
| Mon | Inferomedial (below kneecap, inner) |
| Tue | Inferolateral (below kneecap, outer) |
| Wed | Medial joint line |
| Thu | Superomedial (above kneecap, inner) |
| Fri | Superolateral (above kneecap, outer) |
| Sat | Posterior knee |
| Sun | Rest or systemic (abdomen) |
BPC-157 Knee Protocol: Dosage, Duration, and Stacking
Injection site is one variable. Dose, frequency, and cycle length determine the rest. For full dosage calculations based on body weight and injury severity, use the BPC-157 Dosage Calculator.
Standard Knee Protocol
Dosage: 250-500 mcg per day, injected subcutaneously near the knee. Most users and clinics report 250 mcg twice daily (morning and evening) or 500 mcg once daily. Cerovecki et al. (2010) used 10 mcg/kg and 10 ng/kg in rats, both effective. Scaled to humans, this supports the 250-500 mcg/day range.
Frequency: Once or twice daily. Splitting the dose into two injections at different sites around the knee maintains more consistent local peptide levels. Single daily injection is simpler and still effective.
Cycle length: 4-8 weeks for most knee injuries. The rat MCL study showed progressive improvement at 14, 30, 45, and 90 days. Tendon injuries generally require longer protocols than ligament sprains.
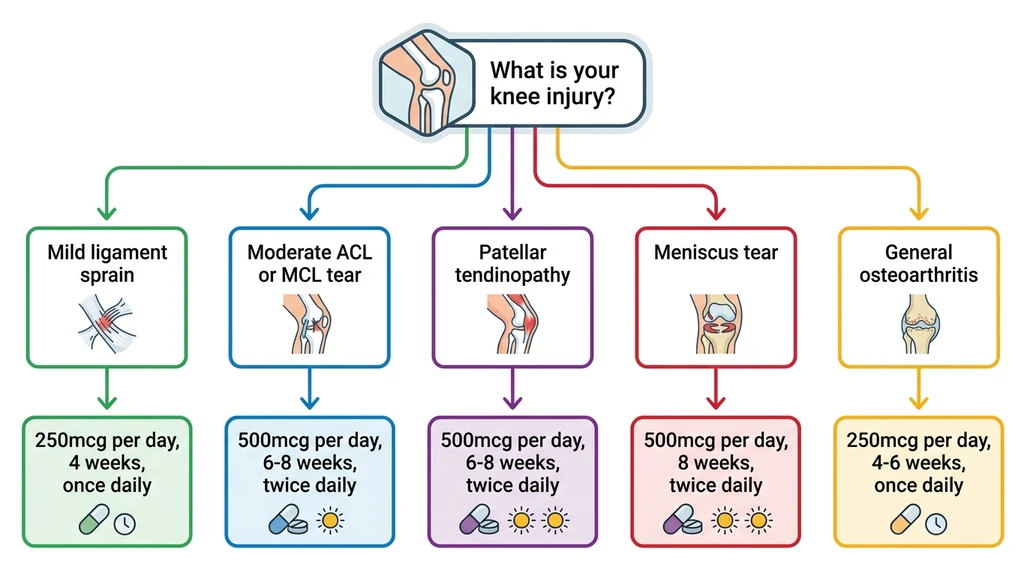
| Injury Type | Suggested Dose | Duration | Frequency |
|---|---|---|---|
| Mild ligament sprain | 250 mcg/day | 4 weeks | Once daily |
| Moderate ligament tear | 500 mcg/day | 6-8 weeks | Twice daily (split) |
| Patellar tendinopathy | 500 mcg/day | 6-8 weeks | Twice daily (split) |
| Meniscus tear | 500 mcg/day | 8 weeks | Twice daily (split) |
| Post-surgical recovery | 500 mcg/day | 4-8 weeks | Twice daily (split) |
| General knee OA | 250 mcg/day | 4-6 weeks | Once daily |
Rest between cycles: 2-4 weeks off after a full cycle before starting another. No published data establishes an optimal rest period.
Stacking BPC-157 with TB-500 for Knee Injuries
BPC-157 and TB-500 (Thymosin Beta-4) address different repair mechanisms. BPC-157 promotes angiogenesis and collagen organization. TB-500 accelerates cell migration through actin polymerization and reduces inflammation. The mechanisms are complementary.
A common knee-focused stack:
- BPC-157: 250 mcg twice daily, injected subcutaneously near the knee
- TB-500: 2-2.5 mg twice per week, injected subcutaneously (abdomen or near knee)
TB-500 works systemically due to its larger molecular size and longer half-life. Local injection is less critical for TB-500 than for BPC-157. See the full TB-500 dosage chart for loading and maintenance phases, and best peptides for tendon repair for additional combination strategies.
Supporting Your Protocol
BPC-157 accelerates biological healing processes that still depend on adequate inputs.
Do: - Maintain protein intake at 1.6-2.2 g/kg body weight. Collagen synthesis requires amino acid substrate. - Follow your physical therapy exercises. BPC-157 builds tissue; loading and movement organize it correctly. - Sleep 7-9 hours. Growth hormone release during deep sleep compounds peptide-driven repair.
Avoid: - NSAIDs (ibuprofen, naproxen) during your BPC-157 cycle. NSAIDs suppress the inflammatory signaling that BPC-157 modulates. - Heavy training on the injured knee during weeks 1-4. Controlled loading yes, max effort no. - Excessive alcohol. See the BPC-157 and alcohol guide for the full research breakdown.
Review the complete BPC-157 side effects profile before starting.
What the Research Shows: BPC-157 and Knee Structures
All BPC-157 research on knee-specific structures comes from animal models, with one exception. Understanding the evidence base prevents overestimating results.
The Only Human Knee Study
Lee et al. (2021) studied intra-articular BPC-157 injection for chronic knee pain. Of 12 BPC-157-only patients, 11 (91.6%) reported significant improvement. A 2025 systematic review reported 7 of 12 maintained improvement beyond 6 months.
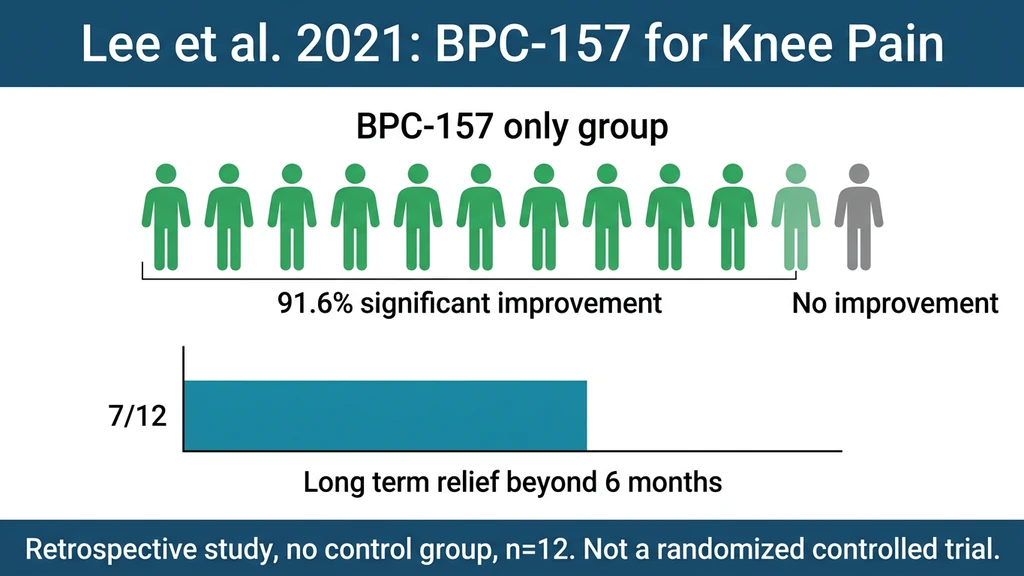
The limitations are serious. The study was retrospective with no control group. The sample was 12 patients. Knee pain types were unspecified. There was no blinding. The lead author of the 2025 narrative review titled "Regeneration or Risk?" emphasized the urgent need for randomized controlled trials.
Ligament Healing (MCL Model)
Cerovecki et al. (2010) transected the MCL in rats and treated with BPC-157 via three routes: local application, systemic intraperitoneal injection, and oral (in drinking water). All three routes improved healing.
BPC-157-treated rats showed reduced valgus instability, higher load-to-failure values, and better collagen fiber organization at 14, 30, 45, and 90 days. The 90-day follow-up is unusually long for a peptide study and showed continued benefit rather than plateau.
Tendon Repair Mechanisms
Chang et al. (2011) identified three mechanisms: BPC-157 increased fibroblast outgrowth from tendon explants in a dose-dependent manner, improved tendon cell survival under oxidative stress, and accelerated fibroblast migration through FAK-paxillin signaling.
Staresinic et al. (2003) demonstrated BPC-157 accelerated healing of transected rat Achilles tendons. Krivic et al. (2006) showed BPC-157 promoted tendon-to-bone healing and opposed corticosteroid-induced healing impairment. Huang et al. (2018) found BPC-157 enhances growth hormone receptor expression in tendon fibroblasts, providing another regeneration pathway.
Evidence Limitations
No human RCTs. Zero randomized, placebo-controlled human trials for BPC-157 and knee injuries exist as of March 2026.
Animal-to-human translation is uncertain. Rat MCL and Achilles tendon models are informative but do not guarantee equivalent results in humans.
Optimal injection route is unestablished. No head-to-head study has compared subcutaneous near the knee vs. systemic subcutaneous vs. intramuscular for the same knee injury.
Long-term safety data is absent. No long-term knee-specific safety data exists. BPC-157 is not FDA-approved for any human use. The FDA issued a warning about BPC-157 in compounded products.
The preclinical evidence is genuinely strong for musculoskeletal healing. Anyone using BPC-157 for knee injuries is operating ahead of the clinical evidence. The guide on peptides for joint pain compares BPC-157 against alternatives with stronger human data, including collagen peptides with multiple RCTs.
Common Mistakes and How to Avoid Them
Mistake 1: Injecting too far from the injury. You inject 500 mcg of BPC-157 in your abdomen for a patellar tendon problem. The peptide distributes across 5 liters of blood volume. Local concentration at the tendon drops to a fraction of what a direct knee injection delivers. After 6 weeks, you see minimal improvement. The fix: identify your injury location and inject within 2-3 cm.
Mistake 2: Skipping alcohol prep. The knee contacts clothing, gym equipment, and floor surfaces constantly. One unsterilized injection introduces skin bacteria through the puncture. A subcutaneous infection near the knee causes redness, swelling, and warmth within 48-72 hours, potentially requiring antibiotics and forcing you to stop the entire protocol. Clean every site, every time, with 70% isopropyl.
Mistake 3: Same spot every day. Daily injection at one site for 4 weeks creates a hardened nodule of scar tissue that reduces peptide absorption by the second week. The tissue becomes tender. Bruising appears. The fix: maintain at least 3 sites in rotation, ideally 5-6. Log each injection.
Mistake 4: Attempting intra-articular injection without training. The Lee et al. study used intra-articular injection under clinical supervision. Self-administered intra-articular injection risks septic arthritis (joint infection), which requires emergency IV antibiotics and possible surgical drainage within 24-48 hours of onset. Stay subcutaneous. Pinch the skin, 45-degree angle, fat layer only.
Frequently Asked Questions
Frequently Asked Questions
Can I inject BPC-157 directly into my knee joint?
Intra-articular injection (into the joint space) was used in the Lee et al. (2021) study under medical supervision. Self-administering into the joint risks septic arthritis, which can destroy cartilage within 24-48 hours. Subcutaneous injection around the knee is the recommended self-administration route. The peptide diffuses from the fat layer toward deeper structures.
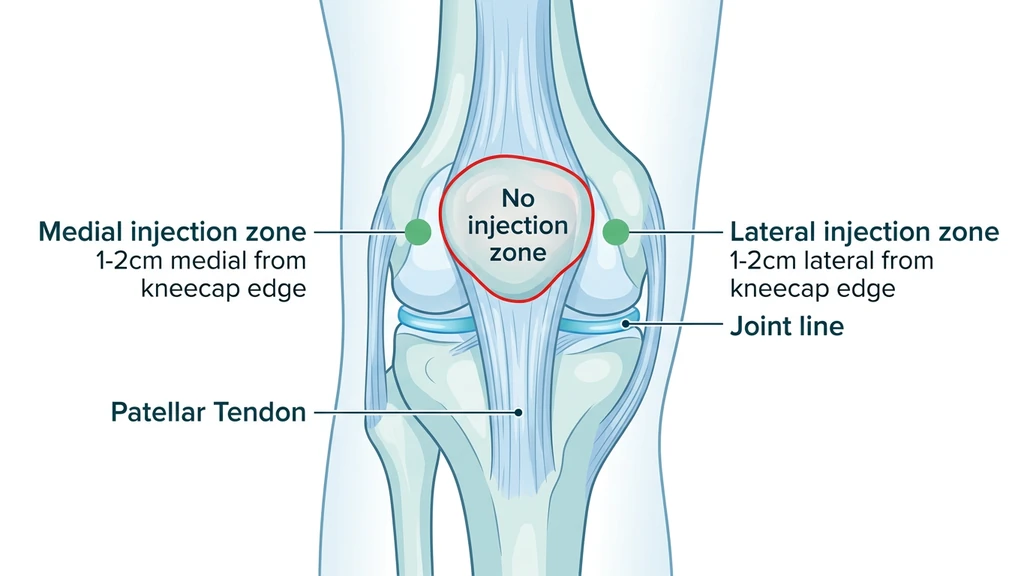
How close to the kneecap should I inject?
Inject 1-3 cm from the edge of the kneecap. The areas adjacent to the patellar tendon (medial and lateral) and the soft tissue above and below the kneecap offer the best balance of injury proximity and subcutaneous depth. Avoid injecting directly over the patella, where there is minimal subcutaneous fat over bone.
Should I inject BPC-157 in the same knee every day?
Yes. If your left knee has an MCL sprain, all injections go near the left knee. Rotate the specific site around the knee: medial joint line one day, superomedial the next, inferomedial after that. This maintains high local concentration while preventing tissue irritation at any single spot.
Is subcutaneous or intramuscular injection better for knee injuries?
Subcutaneous is the standard for self-administered BPC-157 knee protocols. It uses finer needles (29-31G vs. 22-25G for intramuscular), carries lower infection risk, and is technically simpler. The subcutaneous tissue surrounding the knee provides adequate proximity for peptide diffusion to ligaments, tendons, and the joint capsule.
How long until BPC-157 knee injections produce results?
Most users report initial pain and mobility improvement within 1-2 weeks. Structural healing takes longer. The Cerovecki et al. (2010) rat study showed continued improvement across 14, 30, 45, and 90-day checkpoints. Plan for 4-8 weeks minimum. If you see zero improvement after 4 weeks, reassess your diagnosis and protocol.
Can I take ibuprofen while using BPC-157 for my knee?
NSAIDs suppress the inflammatory signaling that BPC-157 modulates. They work against each other. Avoid ibuprofen, naproxen, and similar NSAIDs during your BPC-157 cycle. Acetaminophen (Tylenol) is a safer pain management option during the protocol, as it reduces pain without suppressing the inflammatory cascade.
What needle gauge should I use for knee injections?
Use 29G or 30G insulin syringes with 8mm (0.5 inch) needles for all subcutaneous knee sites. 31G works but draws liquid slowly. Never go larger than 27G for subcutaneous injection. Finer needles reduce pain and tissue damage while still reaching the subcutaneous fat layer around the knee.
Do I need to inject behind the knee for an ACL tear?
The posterior knee (popliteal fossa) is a secondary site for ACL injuries, targeting the posterior ligament attachment. Inject 1-2 cm to the side of center to avoid the popliteal artery. Rotate between medial, lateral, and posterior sites across days for multi-directional peptide coverage around the deep ACL.
The Bottom Line
Inject BPC-157 subcutaneously within 1-3 cm of the injured knee structure. Match the site to the injury: medial joint line for MCL, lateral for LCL, below the kneecap for patellar tendon, multi-quadrant rotation for ACL or diffuse pain. Use 29-31G insulin needles at 45 degrees. Rotate across at least 3 sites.
The evidence base is preclinical with one small human study. Cerovecki et al. (2010) and Chang et al. (2011) support local delivery for ligament and tendon repair. Set expectations accordingly: BPC-157 is a promising tool for knee rehabilitation, not a proven therapy. Combine it with physical therapy, 1.6-2.2 g/kg protein, and 7-9 hours of sleep.
Calculate your exact dose with the BPC-157 Dosage Calculator. Prepare your vial with the Peptide Reconstitution Calculator. For a complete injection walkthrough covering needle selection, sterile technique, and pain minimization, read how to inject BPC-157. Review safety data at BPC-157 side effects. Compare alternatives at peptides for joint pain and best peptides for tendon repair.
References
- 1.Vasireddi N et al. (2025). Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review. *Orthop J Sports Med.* PMC
- 2.Lee JY et al. (2021). Intra-Articular Injection of BPC 157 for Multiple Types of Knee Pain. *Altern Ther Health Med.* 27(S1):8-13. PubMed
- 3.Cerovecki T et al. (2010). Pentadecapeptide BPC 157 (PL 14736) improves ligament healing in the rat. *J Orthop Res.* 28(9):1155-1161. PubMed
- 4.Chang CH et al. (2011). The promoting effect of pentadecapeptide BPC 157 on tendon healing involves tendon outgrowth, cell survival, and cell migration. *J Appl Physiol.* 110(3):774-780. PubMed
- 5.Staresinic M et al. (2003). Gastric pentadecapeptide BPC 157 accelerates healing of transected rat Achilles tendon and in vitro stimulates tendocytes growth. *J Orthop Res.* 21(6):976-983. PubMed
- 6.Krivic A et al. (2006). Achilles detachment in rat and stable gastric pentadecapeptide BPC 157: Promoted tendon-to-bone healing and opposed corticosteroid aggravation. *J Orthop Res.* 24(5):982-989. PubMed
- 7.Huang T et al. (2018). Pentadecapeptide BPC 157 Enhances the Growth Hormone Receptor Expression in Tendon Fibroblasts. *Molecules.* 23(7):1733. PMC
- 8.Gwyer D et al. (2025). Regeneration or Risk? A Narrative Review of BPC-157 for Musculoskeletal Healing. *Biomedicines.* PMC
Related Articles
Where to Inject BPC-157: Site Guide
Where to inject BPC-157 for shoulder, back, hip, gut, elbow, and Achilles injuries. Anatomical sites, local vs systemic delivery, and rotation.
How to Take BPC-157: Dosage and Timing
How to take BPC-157: inject 250-500 mcg subcutaneously near the injury once daily for 4-8 weeks. Reconstitution, dosing, and cycle length.
GLP-1 Injection Sites: The 3 Approved Spots
GLP-1 injection sites: abdomen, front thigh, back of upper arm. What the Ozempic, Wegovy, Mounjaro and Zepbound labels say, plus a rotation plan that works.
Peptides for Healing: What the Evidence Shows
Peptides for healing by tissue: tendon, bone, wound, gut, post-surgery. Which claims rest on human trials, which rest on rat studies, and what is unsafe.