
You started retatrutide two days ago and have already made three urgent trips to the bathroom. Diarrhea affects 16-34% of retatrutide users depending on dose, making it the second most common GI side effect after nausea. In the Phase 3 TRIUMPH-4 trial, 33% of participants on the 12 mg dose reported diarrhea compared to 13.4% on placebo (Wang et al., Syst Rev Meta-Analysis, 2025). The good news: it is dose-dependent, peaks during escalation, and typically resolves within 8-12 weeks.
| Quick Reference | Details |
|---|---|
| Incidence at 12 mg | 33% (vs 13.4% placebo) |
| Incidence at 4 mg | ~16% |
| Rank among side effects | #2 (after nausea) |
| Mechanism | GLP-1 + glucagon receptor activation |
| Onset | Days 1-5 after each dose increase |
| Duration | 3-5 days at stable dose; 8-12 weeks total |
| Key fix | Slow 4-week dose escalation + low-fat meals |
| Discontinuation rate | 6-16% due to GI AEs in trials |
For dosing protocols that minimize GI distress, see our retatrutide dosage calculator. For the full safety picture, read our retatrutide side effects overview.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
How Common Is Diarrhea on Retatrutide?
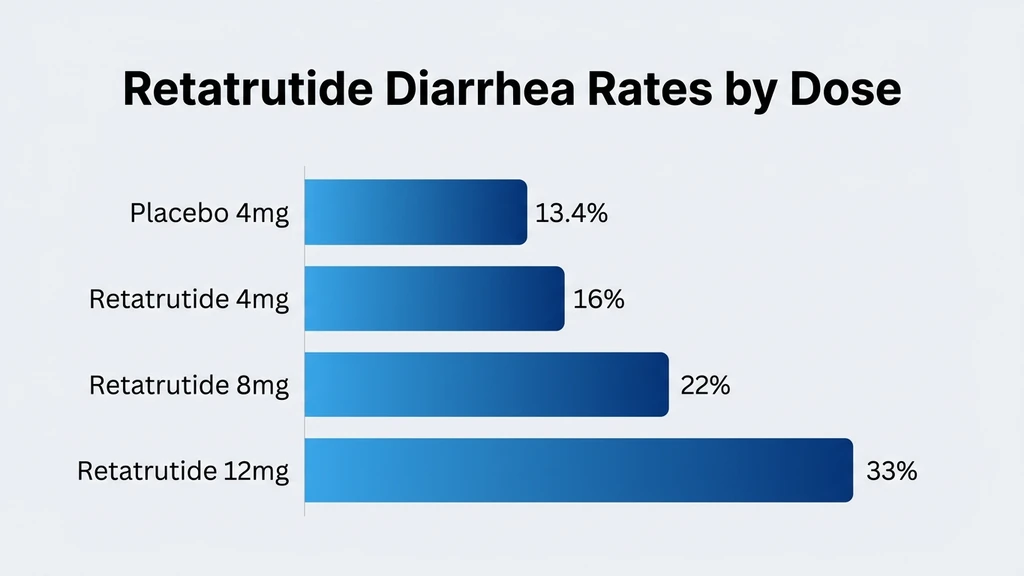
Retatrutide's diarrhea rates climb in lockstep with dose. The Phase 2 NEJM trial mapped this relationship across four dose tiers, and the Phase 3 TRIUMPH-4 data confirmed it at scale (Jastreboff et al., NEJM, 2023).
The pattern is clear: every step up the dose ladder brings a fresh wave of GI symptoms. Placebo groups experienced diarrhea at 10-13%, establishing the baseline noise. Retatrutide pushed that number to 16% at 4 mg, 22% at 8 mg, and 33-34% at 12 mg.
| Dose | Diarrhea Rate | Placebo Rate | Relative Increase |
|---|---|---|---|
| 4 mg | ~16% | 13.4% | 1.2x |
| 8 mg | ~22% | 13.4% | 1.6x |
| 9 mg (fast escalation) | ~28% | 13.4% | 2.1x |
| 12 mg | 33-34% | 13.4% | 2.5x |
Escalation speed matters as much as final dose. Rosenstock et al. found that fast escalation to 8 mg produced GI adverse events in 50% of participants, compared to roughly 35% with gradual titration (Rosenstock et al., Lancet, 2023). The same destination reached slowly causes less turbulence.
Why Does Retatrutide Cause Diarrhea?
Retatrutide is a triple agonist: it activates GLP-1, GIP, and glucagon receptors simultaneously. Each receptor contributes differently to the GI disruption. Understanding which one does what helps explain why retatrutide's diarrhea profile differs from simpler drugs like semaglutide.
GLP-1 Receptor Activation and Gastric Motility
GLP-1 receptor activation slows gastric emptying. Food sits in your stomach longer than normal. Think of it like a kitchen drain that has been partially blocked: water still flows, but the backup creates pressure above the blockage.
When the stomach eventually releases its contents into the small intestine, the bolus arrives larger and less processed than usual. The intestinal lining responds with increased fluid secretion, accelerating transit through the colon. The result is loose stools and urgency. This mechanism is shared across all GLP-1 drugs, from semaglutide to tirzepatide to retatrutide (PMC12992036).
Glucagon Receptor's Role in GI Disruption
The glucagon receptor component is unique to retatrutide. Neither semaglutide nor tirzepatide activates this pathway. Glucagon receptor agonism triggers pro-emetic signaling in the area postrema of the brainstem and increases intestinal motility through direct smooth muscle stimulation (PMC12992036).
This is why retatrutide produces higher GI rates than its dual-agonist predecessor tirzepatide. The glucagon receptor adds a second accelerator to intestinal transit on top of the GLP-1 brake-then-release cycle. Two mechanisms pushing stool through the colon faster means more diarrhea at equivalent weight loss.
GIP Agonism: Does It Help or Hurt?
GIP receptor activation was originally hypothesized to buffer GI side effects. Tirzepatide's lower nausea rates compared to semaglutide supported this theory. In retatrutide, the GIP signal still provides some buffering effect. But the addition of glucagon receptor agonism overwhelms the GIP benefit.
The net result: retatrutide's triple mechanism produces more GI disruption than either GLP-1 alone (semaglutide) or GLP-1 plus GIP (tirzepatide). The glucagon component tilts the balance toward discomfort, at least during the escalation phase.
Retatrutide Diarrhea vs Tirzepatide vs Semaglutide
Head-to-head trials comparing all three drugs do not exist yet. The comparison below draws from each drug's respective Phase 3 data. Different trial designs and populations make direct comparison imperfect, but the trend is consistent (PMC12654588).
| Drug | Mechanism | Max Diarrhea Rate | Max Nausea Rate | Max Weight Loss |
|---|---|---|---|---|
| Semaglutide 2.4 mg | GLP-1 only | ~30% | ~44% | ~15% |
| Tirzepatide 15 mg | GLP-1 + GIP | ~23% | ~33% | ~22% |
| Retatrutide 12 mg | GLP-1 + GIP + Glucagon | ~34% | ~48% | ~24% |
Tirzepatide's GIP co-agonism appears to protect against diarrhea relative to semaglutide, even at higher weight loss. Retatrutide's glucagon receptor then reverses that protection. More weight loss comes at a GI cost.
For a full head-to-head breakdown, see our retatrutide vs tirzepatide comparison. If you are weighing options, semaglutide produces less diarrhea but also less weight loss.
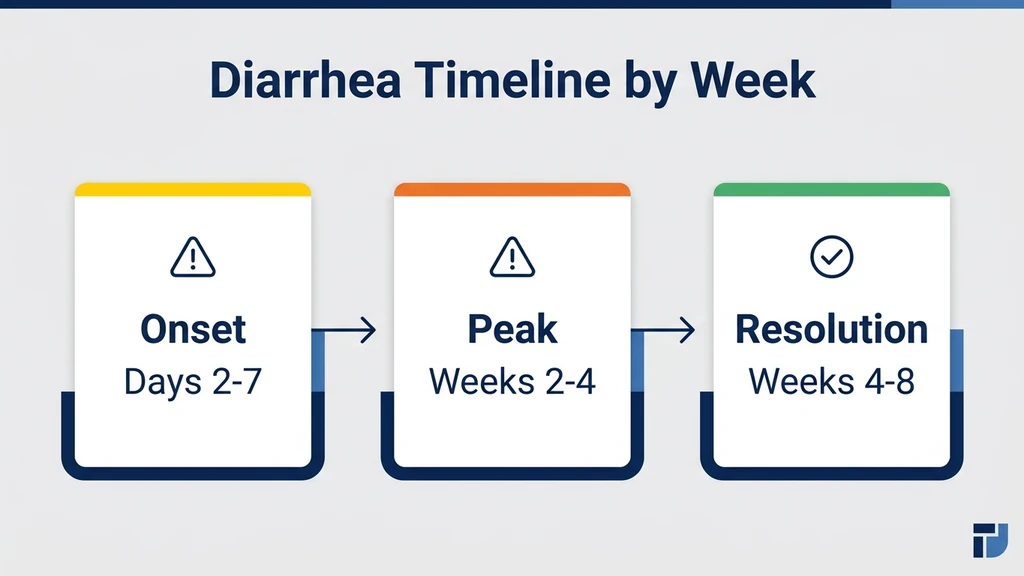
When Does Retatrutide Diarrhea Start and Stop?
Diarrhea follows a predictable cycle tied to dose escalation. Each increase resets the clock, but each successive wave tends to be milder than the last as your GI tract adapts.
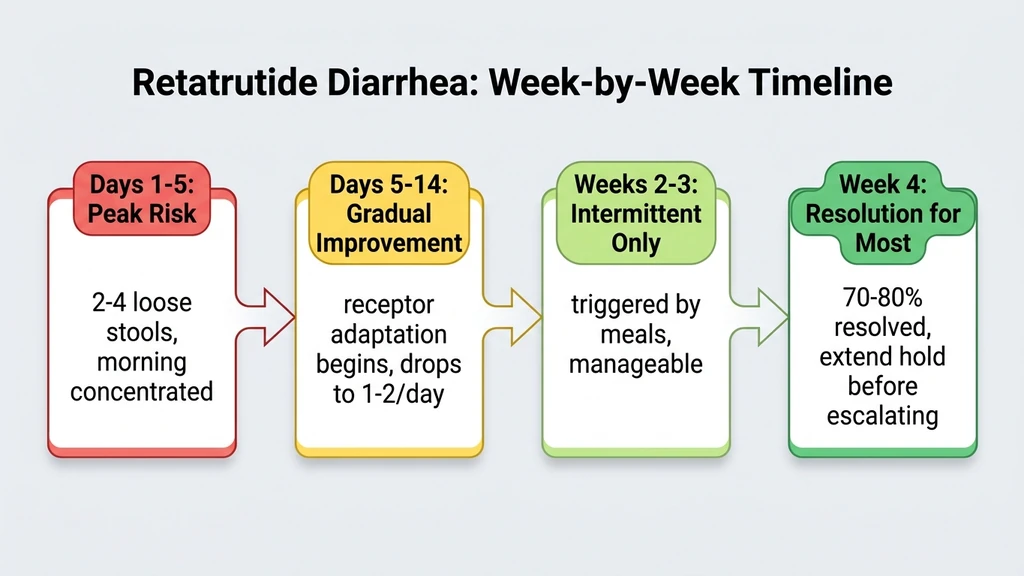
Days 1-5 After Each Dose Increase
The first five days after a dose escalation are the highest-risk window. Your GLP-1 and glucagon receptors face a sudden increase in activation. Intestinal motility spikes. Most users report 2-4 loose stools per day during this peak, concentrated in the morning and after meals.
The severity depends on how large the dose jump was. Going from 4 mg to 8 mg in one step is harder on the gut than two smaller increases with a 4-week interval between them.
Days 5-14: Gradual Improvement
Receptor desensitization begins. Your intestinal smooth muscle adapts to the new level of GLP-1 and glucagon signaling. By day 10-14 at a stable dose, most users report stool consistency returning to near-normal. Frequency drops from 3-4 loose stools to 1-2 per day.
Weeks 3-4: Resolution at Stable Dose
By weeks 3-4 at the same dose, diarrhea resolves for most users. This is why the 4-week minimum escalation interval matters. Rushing to the next dose before GI adaptation completes means stacking one wave of diarrhea on top of another. The Phase 2 data showed slow titration cut GI adverse events by approximately 50% (Rosenstock et al., Lancet, 2023).
Weeks 8-12: Long-Term Adaptation
By the time you reach your target maintenance dose and remain there for 4-8 weeks, diarrhea becomes infrequent. Roughly 85% of users who experienced diarrhea during escalation report resolution by week 12 of stable dosing. The remaining 15% may have persistent loose stools that warrant medical evaluation.
7 Evidence-Based Ways to Manage Retatrutide Diarrhea
These strategies come from clinical trial protocols, GLP-1 management guidelines, and pharmacist-level recommendations for GI symptom control (US Pharmacist, GI AEs of GLP-1 RAs).
1. Follow Slow Dose Escalation (4-Week Minimum)
Stay at each dose for a full 4 weeks before increasing. This is the single most effective prevention strategy. The Phase 2 data proves it: fast escalation to 8 mg doubled GI adverse event rates compared to gradual titration.
Your retatrutide dosage guide should include built-in 4-week holds. If diarrhea has not resolved by week 4, extend the hold to 6 weeks before moving up. There is no clinical penalty for slower escalation.
2. Eat Low-Fat, Small Meals
Fat is the hardest macronutrient for your GI tract to process during GLP-1 therapy. A single high-fat meal can trigger diarrhea within 1-2 hours. Switch to 5-6 small meals per day with less than 15g of fat per meal.
Focus on lean protein (chicken breast, white fish, egg whites), complex carbohydrates (rice, oatmeal, sweet potato), and cooked vegetables. Raw vegetables and salads can worsen symptoms during the first 2 weeks of a new dose.
3. Stay Aggressively Hydrated
Diarrhea depletes fluids faster than you realize. Aim for 2.5-3 liters of water daily during active episodes. Plain water is not enough: you need electrolytes. Add an oral rehydration solution or electrolyte mix to at least 1 liter per day.
Signs of dehydration to watch: dark urine, dizziness when standing, dry mouth, reduced urine output. If you cannot keep fluids down due to concurrent nausea, seek medical attention. Dehydration is the primary safety concern with GLP-1-induced diarrhea.
4. Use OTC Anti-Diarrheals (Loperamide) as Rescue
Loperamide (Imodium) 2 mg can be taken after the first loose stool, followed by 2 mg after each subsequent loose stool up to 8 mg per day. It slows intestinal motility and increases water reabsorption in the colon.
Do not use loperamide preventively or daily. Reserve it for rescue use during acute episodes, particularly if you need to leave the house or attend work. Chronic use can mask worsening symptoms that need medical evaluation.
5. Time Your Injection at Night
Injecting retatrutide at bedtime shifts the peak GI effects to your sleeping hours. Most users report that nighttime injection reduces daytime diarrhea episodes by allowing the initial receptor activation surge to pass overnight.
This is especially helpful during the first week of a new dose. Learn more about injection timing in our how to take retatrutide guide.
6. Maintain Electrolyte Balance
Diarrhea strips sodium, potassium, and magnesium from your body. Low potassium causes muscle cramps. Low magnesium causes fatigue and headaches. Low sodium causes dizziness and nausea, which compounds the retatrutide side effect burden.
Supplement with 400 mg magnesium glycinate daily. Add potassium-rich foods: bananas, avocado, coconut water. If diarrhea persists beyond 5 days, ask your provider to check a basic metabolic panel.
7. Rotate Injection Sites
While injection site does not directly cause diarrhea, abdominal injection sites can increase local GI awareness and discomfort. During active diarrhea episodes, inject in the thigh or upper arm instead.
Rotating sites also reduces lipodystrophy risk over long-term use. Keep a rotation log: left abdomen, right abdomen, left thigh, right thigh, alternating weekly.
When to See a Doctor About Retatrutide Diarrhea
Most retatrutide diarrhea resolves with time and the management strategies above. Certain red flags require prompt medical evaluation.
Seek immediate medical attention if you experience: bloody or black stools, severe abdominal pain, signs of significant dehydration (no urine output for 8+ hours, rapid heart rate, confusion), fever above 101F (38.3C), or diarrhea lasting more than 7 consecutive days without improvement.
Consider contacting your prescriber if: diarrhea persists beyond 4 weeks at a stable dose, you are losing more than 3% of body weight per week, you cannot maintain adequate nutrition or hydration, or OTC management fails to provide relief.
In clinical trials, 6-16% of participants discontinued retatrutide due to gastrointestinal adverse events (Jastreboff et al., NEJM, 2023). Discontinuation is a valid choice when symptoms exceed the benefit. Your prescriber may recommend a dose reduction rather than stopping entirely.
Related Side Effects
Retatrutide Nausea Nausea is the #1 side effect, affecting 25-48% of users. It shares the same GLP-1 and glucagon receptor mechanisms as diarrhea. Managing one often helps the other.
Retatrutide Hair Loss Rapid weight loss from retatrutide can trigger telogen effluvium (temporary hair shedding). The 24% body weight loss seen in trials puts retatrutide users at higher risk than users of lower-efficacy GLP-1 drugs.
Retatrutide Side Effects Overview Complete guide covering all documented adverse events from Phase 2 and Phase 3 clinical trials, including cardiovascular, hepatic, and endocrine safety data.
Does Tirzepatide Cause Diarrhea? Tirzepatide's dual GLP-1/GIP mechanism produces lower diarrhea rates (~23%) than retatrutide's triple agonist approach. If GI tolerance is your priority, tirzepatide may be a better fit.
Retatrutide vs Tirzepatide Full comparison of efficacy, side effects, cost, and availability between these two next-generation weight loss drugs.
Frequently Asked Questions
What percentage of people get diarrhea on retatrutide?
In Phase 3 TRIUMPH-4 trials, 33% of participants at the 12 mg dose experienced diarrhea compared to 13.4% on placebo. Rates are dose-dependent: approximately 16% at 4 mg and 22% at 8 mg. Slow escalation over 4-week intervals reduces severity by roughly 50%.
Does retatrutide diarrhea go away?
Yes. Most episodes resolve within 3-5 days at a stable dose. Diarrhea recurs with each dose escalation but diminishes significantly by weeks 8-12 of treatment. Approximately 85% of affected users report resolution once they reach and maintain their target dose for 4-8 weeks.
Is retatrutide diarrhea worse than semaglutide?
Retatrutide's triple-agonist mechanism (GLP-1 + GIP + glucagon) produces diarrhea in approximately 34% of users at 12 mg, compared to roughly 30% for semaglutide at 2.4 mg. The glucagon receptor component unique to retatrutide increases intestinal motility beyond what GLP-1 alone causes.
How do I stop diarrhea from retatrutide?
The most effective strategy is slow dose escalation with 4-week holds. Eat 5-6 small, low-fat meals daily. Take loperamide (Imodium) 2 mg as rescue for acute episodes, up to 8 mg per day. Inject at bedtime. Maintain aggressive hydration with electrolytes: 2.5-3 liters daily during active episodes.
Can I take Imodium with retatrutide?
Yes. Loperamide (Imodium) is safe to use as a rescue anti-diarrheal during retatrutide therapy. Clinical trials permitted OTC anti-diarrheal use. Take 2 mg after the first loose stool, then 2 mg after each subsequent episode, not exceeding 8 mg in 24 hours. Reserve it for acute episodes rather than daily prevention.
Does the diarrhea get worse at higher retatrutide doses?
Yes. Diarrhea rates increase with dose: 16% at 4 mg, 22% at 8 mg, and 33-34% at 12 mg. Each dose escalation triggers a new 3-5 day wave of loose stools. Slow titration with 4-week holds between increases allows GI adaptation and significantly reduces the severity of each wave.
Should I stop retatrutide if I have diarrhea?
Not immediately. Diarrhea is expected during dose escalation and resolves for most users. Contact your prescriber if diarrhea persists beyond 4 weeks at a stable dose, is accompanied by blood, causes dehydration, or prevents adequate nutrition. In trials, 6-16% of participants discontinued due to GI adverse events.
Why does retatrutide cause more diarrhea than tirzepatide?
Retatrutide activates the glucagon receptor, which tirzepatide does not. Glucagon receptor agonism stimulates intestinal smooth muscle directly and triggers pro-emetic signaling in the brainstem. This third mechanism adds a layer of GI disruption on top of the GLP-1-mediated delayed gastric emptying that both drugs share.
The Bottom Line
Retatrutide causes diarrhea in 16-34% of users, depending on dose. The triple-agonist mechanism (GLP-1 + GIP + glucagon) produces higher GI rates than semaglutide or tirzepatide alone, with the glucagon receptor being the primary driver of the difference. Diarrhea peaks during the first 5 days of each dose escalation and resolves within 3-4 weeks at stable dosing.
Slow titration is the most powerful tool you have. A 4-week minimum hold at each dose cuts GI adverse event rates by roughly half. Combine that with low-fat meals, aggressive hydration, and bedtime injection timing. Keep loperamide on hand for rescue use during acute episodes.
Use our retatrutide dosage calculator to plan a gradual escalation schedule. For the complete side effect picture, read our retatrutide side effects overview. If diarrhea persists beyond 4 weeks at a stable dose, consult your prescriber about dose adjustment or alternative therapies.
Related Articles
Retatrutide Nausea: Rates, Timeline & Management
Retatrutide nausea affects 25-48% of users. Rates by dose, GLP-1 + glucagon mechanism, week-by-week timeline, and 8 management strategies.
Can Semaglutide Cause Diarrhea?
Diarrhea affects 8-30% of semaglutide users depending on dose. Learn the GLP-1 mechanism, STEP trial incidence data, timeline, and 6 management strategies.
Retatrutide Hair Loss: Prevention & Fix
Does retatrutide cause hair loss? Telogen effluvium from rapid weight loss (up to 24%) is the likely cause. Prevention protocol and GHK-Cu options.
Does Tirzepatide Cause Diarrhea?
Diarrhea affects 12-17% of tirzepatide users. Learn why GLP-1/GIP activation triggers it, when it resolves, danger signs, and 6 strategies that work.