
You injected your first dose of retatrutide yesterday and woke up feeling like you stepped off a boat. Nausea is the #1 side effect of retatrutide, affecting 25-48% of users depending on dose. In the Phase 3 TRIUMPH-4 trial, 43% of participants at the treatment dose reported nausea compared to roughly 10% on placebo (Wang et al., Syst Rev Meta-Analysis, 2025). The good news: it peaks during dose escalation, resolves within 3-4 weeks at each stable dose, and slow titration cuts severity by approximately 50%.
| Quick Reference | Details |
|---|---|
| Incidence (Phase 3) | 43% at treatment dose |
| Incidence range by dose | 25-48% |
| Placebo rate | ~10% |
| Rank among side effects | #1 most common |
| Mechanism | GLP-1 delayed gastric emptying + glucagon pro-emetic signaling |
| Peak timing | Days 1-3 after each dose increase |
| Resolution | Weeks 3-4 at each stable dose |
| Total nausea burden | 6-12 weeks across full escalation |
| Key fix | 4-week minimum dose escalation + bedtime injection |
For a dosing schedule that minimizes nausea, see our retatrutide dosage calculator. For the full safety profile, read our retatrutide side effects overview.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
How Common Is Nausea on Retatrutide?
Nausea rates scale with dose. The Phase 2 NEJM trial provided the first dose-by-dose breakdown, and Phase 3 TRIUMPH-4 confirmed the pattern at larger scale (Jastreboff et al., NEJM, 2023).
| Dose | Nausea Rate | Placebo Rate | Escalation Speed |
|---|---|---|---|
| 1 mg | ~9% | ~10% | N/A (starting dose) |
| 4 mg | ~25% | ~10% | Slow escalation |
| 8 mg (slow) | ~35% | ~10% | 4-week intervals |
| 8 mg (fast) | ~50% | ~10% | 2-week intervals |
| 12 mg | ~48% | ~10% | After slow escalation |
Rosenstock et al. showed the impact of escalation speed most clearly: fast escalation to 8 mg produced nausea in approximately 50% of participants, nearly double the rate of slow titration at the same dose (Rosenstock et al., Lancet, 2023). The destination matters, but how quickly you get there matters just as much.
Wang et al.'s meta-analysis pooled data across all retatrutide trials and confirmed that nausea was significantly increased at every dose level above 1 mg (PMC12026077). The pooled incidence across all active doses was 38%.
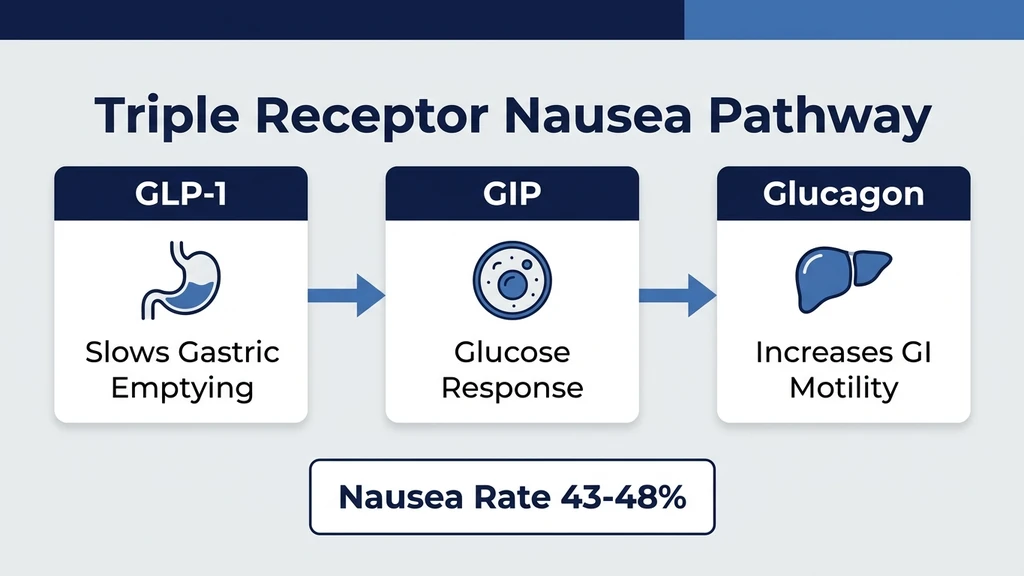
Why Does Retatrutide Cause Nausea?
Retatrutide's nausea comes from two distinct pathways firing simultaneously. GLP-1 receptor activation slows your stomach. Glucagon receptor activation triggers your brain's vomiting center. Together, they produce more nausea than either mechanism alone.
GLP-1 Receptor: Delayed Gastric Emptying
GLP-1 receptor activation is the primary nausea driver across the entire drug class. When GLP-1 receptors in the stomach are activated, gastric emptying slows dramatically. Food that would normally leave your stomach in 2-3 hours lingers for 4-6 hours.
Think of it like a sink filling faster than it drains. The sensation of fullness, pressure, and queasiness builds as the stomach stretches. This is why nausea is worst after meals and why eating large portions on retatrutide feels physically uncomfortable. The feeling is mechanical as much as chemical.
Glucagon Receptor: Central Pro-Emetic Signaling
The glucagon receptor component is unique to retatrutide. Neither semaglutide nor tirzepatide activates this pathway. Glucagon receptor agonism sends direct pro-emetic signals to the area postrema in the brainstem, the region responsible for triggering the vomiting reflex (PMC12992036).
This central signaling is independent of stomach fullness. Users report nausea even on an empty stomach during dose escalation, a pattern less common with GLP-1-only drugs. The brainstem activation explains why retatrutide nausea can feel different from semaglutide nausea: more like motion sickness and less like overeating.
Does GIP Agonism Offset Nausea? (The Evidence Says No)
When tirzepatide (GLP-1 + GIP dual agonist) launched with lower nausea rates than semaglutide, researchers hypothesized that GIP co-agonism buffers GI side effects. Retatrutide tests this hypothesis. It has GIP agonism, but its nausea rates are the highest in the class.
The conclusion: GIP provides some protective effect, but the glucagon receptor overwhelms it. The net nausea burden is GLP-1 slowing + glucagon signaling, partially offset by GIP buffering. The math does not favor the patient. Triple agonism produces triple-class weight loss but with the highest GI side effect rates.
Nausea Timeline: Week by Week During Dose Escalation
Nausea follows a predictable wave pattern tied to each dose increase. Understanding this timeline helps you plan around the worst days and know when relief is coming.
Days 1-3 After Each Dose Increase: The Peak
The first 72 hours after a dose escalation are the hardest. GLP-1 and glucagon receptors face a sudden increase in activation. Nausea ranges from mild queasiness to persistent waves that interfere with daily activities. Some users experience vomiting during this window, reported in 12-20% of participants at higher doses.
Food aversion is common. The sight or smell of certain foods, particularly fatty or strongly flavored items, can trigger nausea episodes. Keep your environment bland and your meals simple during these three days.
Days 4-10: Gradual Improvement
Receptor adaptation begins. The nausea does not disappear but becomes more predictable. Most users report that the constant baseline queasiness fades, replaced by triggered episodes after meals or in response to specific smells. By day 7, many can eat small meals without immediate nausea.
Weeks 2-3: Significant Relief
By weeks 2-3 at a stable dose, nausea becomes intermittent rather than constant. Most users report fewer than 2-3 episodes per week, triggered by larger meals or eating too quickly. Daily function returns to near-normal. Sleep is no longer disrupted by nighttime queasiness.
Week 4: Resolution for Most Users
By week 4, 70-80% of users at a given dose report that nausea has resolved or is minimal. This is precisely why the 4-week hold matters before escalating. Jumping to the next dose before week 4 stacks a new nausea wave on top of an incompletely resolved one.
The full escalation from starting dose to 12 mg involves 2-3 dose increases, each triggering its own wave. Total nausea burden across the entire escalation is typically 6-12 weeks. After reaching maintenance dose, ongoing nausea is uncommon.
Retatrutide Nausea vs Tirzepatide vs Semaglutide
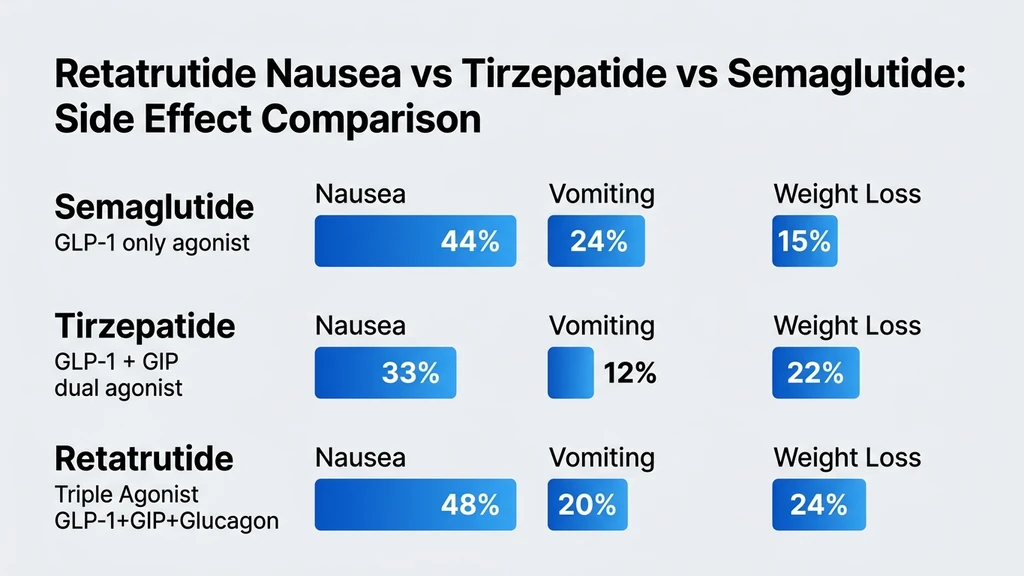
Head-to-head nausea trials do not exist. This comparison draws from each drug's Phase 3 programs. Different trial designs and populations limit direct comparability, but the pattern is consistent across meta-analyses (PMC12654588).
| Drug | Mechanism | Max Nausea Rate | Vomiting Rate | Max Weight Loss |
|---|---|---|---|---|
| Semaglutide 2.4 mg | GLP-1 only | ~44% | ~24% | ~15% |
| Tirzepatide 15 mg | GLP-1 + GIP | ~33% | ~12% | ~22% |
| Retatrutide 12 mg | GLP-1 + GIP + Glucagon | ~48% | ~20% | ~24% |
Tirzepatide produces the best nausea-to-weight-loss ratio: 22% weight loss with only 33% nausea. Semaglutide has high nausea despite moderate weight loss, likely because it lacks GIP's buffering effect. Retatrutide has the highest nausea and the highest weight loss. The glucagon receptor is the differentiator.
For a complete comparison, see retatrutide vs tirzepatide. For semaglutide-specific nausea data, read does semaglutide cause nausea.
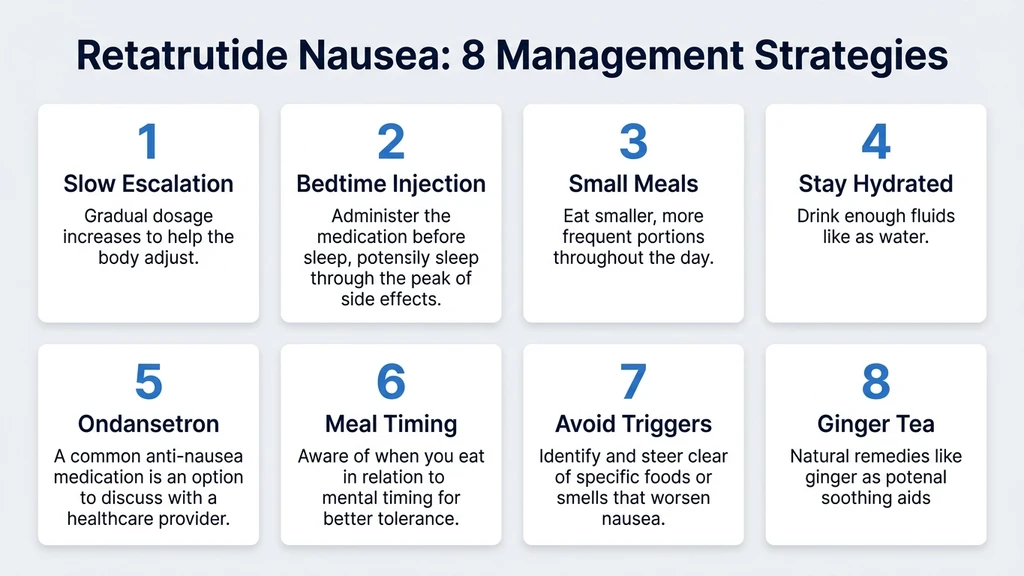
8 Evidence-Based Strategies to Manage Retatrutide Nausea
These strategies combine clinical trial protocol recommendations with pharmacist-level practical guidance (PMC12992036; US Pharmacist).
1. Follow 4-Week Minimum Dose Escalation
This is the most effective nausea prevention strategy. Rosenstock et al. demonstrated that slow titration (4-week intervals between increases) cut nausea rates roughly in half compared to fast escalation (Rosenstock et al., Lancet, 2023).
Stay at each dose for a full 4 weeks. If nausea has not resolved by week 4, extend the hold to 6 weeks. The retatrutide dosage guide provides a full escalation schedule. There is no clinical penalty for slower titration.
2. Inject at Bedtime
Injecting retatrutide at bedtime shifts the peak nausea window (hours 6-18 post-injection) to your sleeping hours. You sleep through the worst of it. By the time you wake, the acute wave has passed and the remaining nausea is manageable.
Several clinical trial sites recommended evening injection as standard protocol. Learn specific injection timing in our how to take retatrutide guide.
3. Eat Small, Low-Fat Meals (5-6 Per Day)
Your stomach empties slowly on retatrutide. Large meals overwhelm it. Switch from three standard meals to 5-6 small meals of 200-300 calories each. Fat is the slowest macronutrient to empty from the stomach, so keep fat under 10-15 grams per meal during active nausea episodes.
Good options: plain rice with grilled chicken, oatmeal with banana, scrambled eggs on toast, plain yogurt with berries. Avoid fried foods, heavy sauces, and large portions of red meat during the escalation phase.
4. Stay Hydrated (Electrolytes + Ginger Water)
Dehydration worsens nausea. Aim for 2-3 liters of fluid daily. Sip continuously rather than drinking large volumes at once, which can trigger nausea in a stomach with delayed emptying.
Ginger water (steep fresh ginger slices in room-temperature water) has mild antiemetic properties supported by clinical evidence across pregnancy and chemotherapy nausea studies. Keep a bottle at your desk. Electrolyte beverages prevent the mineral depletion that compounds nausea.
5. Use Ondansetron (Zofran) as Rescue Antiemetic
Ondansetron (Zofran) 4-8 mg orally dissolving tablet is the most effective rescue antiemetic for GLP-1-induced nausea. Clinical trials for retatrutide permitted its use. It blocks serotonin 5-HT3 receptors in the chemoreceptor trigger zone, directly counteracting the nausea signal.
This requires a prescription. Ask your prescriber for a small supply (10-20 tablets) to keep on hand during dose escalation. Reserve it for days when nausea prevents eating or functioning. Metoclopramide (Reglan) is an alternative that also accelerates gastric emptying.
6. Take Your Injection With or Just Before a Meal
Some users find that having food in the stomach at injection time reduces the initial nausea spike. A small, bland meal 30 minutes before injection provides a buffer. This is not universally effective, but worth testing during your first dose escalation.
If evening injection with dinner is your plan, eat a small meal (200-300 calories, low-fat) before injecting. The food should be easy to digest: crackers with lean protein, soup, or plain pasta.
7. Avoid Trigger Foods (High Fat, Spicy, Acidic)
During the first 2 weeks at each new dose, eliminate the foods most likely to trigger nausea episodes. High-fat foods (fried chicken, pizza, butter-heavy dishes) sit in the stomach longest. Spicy foods irritate already-sensitized gastric lining. Acidic foods (tomatoes, citrus, vinegar) increase gastric acid production.
Reintroduce these foods gradually after week 3 at each dose level. Most users can return to a normal diet (with smaller portions) once nausea resolves.
8. Ginger Supplements and Peppermint Tea
Ginger extract capsules (250 mg, 4 times daily) provide standardized antiemetic dosing. Clinical evidence supports ginger for nausea across multiple contexts. Peppermint tea or peppermint oil capsules relax the lower esophageal sphincter and can reduce the sensation of fullness and pressure.
These are complementary strategies, not replacements for dose management and ondansetron. Use them as a baseline daily protocol during escalation, adding pharmaceutical rescue on the worst days.
When to See a Doctor About Retatrutide Nausea
Most nausea resolves with time and the strategies above. Certain signs require medical evaluation.
Seek immediate attention if: You cannot keep any fluids down for more than 24 hours. You vomit blood or see blood in your stool. You experience severe abdominal pain (not just queasiness). You show signs of dehydration: dark urine, rapid heart rate, dizziness, confusion. You lose more than 3% of body weight in a single week.
Contact your prescriber if: Nausea persists beyond 4 weeks at a stable dose. You cannot maintain adequate nutrition. You miss more than 3 days of work due to nausea. Your quality of life is significantly impaired.
In clinical trials, 6-16% of participants discontinued retatrutide due to adverse events, with GI symptoms being the primary driver (Jastreboff et al., NEJM, 2023). Discontinuation or dose reduction is a reasonable option when nausea exceeds the benefit of weight loss.
Related Side Effects
Retatrutide Diarrhea The #2 GI side effect, affecting 16-34% of users. Diarrhea and nausea share the same GLP-1 and glucagon receptor mechanisms. Managing one often helps the other.
Retatrutide Hair Loss Rapid weight loss from retatrutide can trigger telogen effluvium. Persistent nausea that reduces food intake can worsen nutritional deficiencies that accelerate hair shedding.
Retatrutide Side Effects Overview Complete guide covering all documented adverse events from Phase 2 and Phase 3 clinical trials.
Does Semaglutide Cause Nausea? Semaglutide nausea runs at ~44% but lacks the glucagon receptor component. Compare the profiles if you are choosing between GLP-1 drugs.
Retatrutide vs Tirzepatide Tirzepatide produces significantly less nausea (~33%) while achieving 22% weight loss. Full head-to-head comparison of efficacy and tolerability.
Frequently Asked Questions
What percentage of people get nausea on retatrutide?
Between 25% and 48% depending on dose. Phase 3 TRIUMPH-4 reported 43% nausea at the treatment dose versus roughly 10% on placebo. At the 4 mg starting dose, nausea affects approximately 25% of users. Fast dose escalation increases rates to nearly 50% at 8 mg.
How long does retatrutide nausea last?
Nausea peaks during the first 3 days after each dose increase and resolves by weeks 3-4 at a stable dose for 70-80% of users. The total nausea burden across the full escalation from starting dose to 12 mg is typically 6-12 weeks. After reaching maintenance dose, ongoing nausea is uncommon.
Is retatrutide nausea worse than Ozempic?
Retatrutide's nausea rates (~48% at 12 mg) slightly exceed semaglutide's (~44% at 2.4 mg). The difference is the glucagon receptor: retatrutide activates it, semaglutide does not. Retatrutide nausea can feel more like motion sickness due to central brainstem signaling, while semaglutide nausea is more stomach-based.
Can I take anti-nausea medication with retatrutide?
Yes. Clinical trials permitted ondansetron (Zofran) 4-8 mg and metoclopramide (Reglan) as rescue antiemetics. Ondansetron is the most commonly prescribed option. Ask your prescriber for a small supply to keep on hand during dose escalation. Over-the-counter ginger capsules (250 mg, 4 times daily) also help.
Does retatrutide nausea get worse at higher doses?
Yes. Nausea rates climb with each dose tier: ~25% at 4 mg, ~35% at 8 mg (slow escalation), and ~48% at 12 mg. Each dose increase triggers a new 1-3 day peak. Slow 4-week titration reduces the severity at each step by roughly 50% compared to fast escalation.
When should I inject retatrutide to avoid nausea?
Inject at bedtime. Peak nausea occurs 6-18 hours after injection. A bedtime dose shifts the worst window to your sleeping hours. By morning, the acute wave has passed. Combine this with a small, low-fat meal 30 minutes before injection for additional buffering.
What foods reduce retatrutide nausea?
Bland, low-fat, small meals are best. Focus on plain rice, grilled chicken, oatmeal, bananas, crackers, and broth-based soups. Eat 5-6 meals of 200-300 calories instead of 3 large meals. Avoid fried foods, heavy sauces, spicy dishes, and acidic foods (tomatoes, citrus) during the first 2 weeks at each dose.
Should I stop retatrutide because of nausea?
Not immediately. Nausea is expected during dose escalation and resolves for most users by week 4 at a stable dose. Contact your prescriber if nausea prevents eating for more than 48 hours, persists beyond 4 weeks, or significantly impairs your quality of life. Dose reduction is often more appropriate than full discontinuation.
The Bottom Line
Nausea is the #1 side effect of retatrutide, affecting 25-48% of users across doses. The triple-agonist mechanism is responsible: GLP-1 slows gastric emptying while the glucagon receptor sends pro-emetic signals to the brainstem. The combination produces higher nausea rates than semaglutide or tirzepatide alone.
The most powerful tool is patience. Slow titration with 4-week holds at each dose cuts nausea severity by half. Bedtime injection shifts the peak to sleeping hours. Small, low-fat meals every 3-4 hours prevent the stomach overload that triggers episodes. Keep ondansetron on hand for the hardest days.
Use our retatrutide dosage calculator to build a gradual escalation schedule. For GI management across all retatrutide side effects, read our retatrutide side effects overview. If nausea persists beyond 4 weeks at a stable dose, discuss dose adjustment with your prescriber.
Related Articles
Retatrutide Diarrhea: Rates, Causes & Management
Retatrutide diarrhea affects 16-34% of users by dose. Clinical trial rates, triple-agonist GI mechanism, comparison to semaglutide, and 7 evidence-based fixes.
Retatrutide Hair Loss: Prevention & Fix
Does retatrutide cause hair loss? Telogen effluvium from rapid weight loss (up to 24%) is the likely cause. Prevention protocol and GHK-Cu options.
Does Semaglutide Cause Hair Loss?
Semaglutide-related hair loss affects 3-5% of users. Learn why it happens, when it peaks, and 5 evidence-based strategies to minimize thinning.
Does Semaglutide Cause Nausea?
Nausea affects 40-45% of semaglutide users, especially during dose titration. Learn the mechanism, timeline, and 5 proven strategies to reduce it.