You just moved from 5 mg to 7.5 mg of tirzepatide. Your provider sent new instructions. But you are staring at the syringe and the math no longer lands on a clean number. At 5 mg, you drew to a round mark. At 7.5 mg, every concentration produces a fractional draw that sits between lines on the barrel.
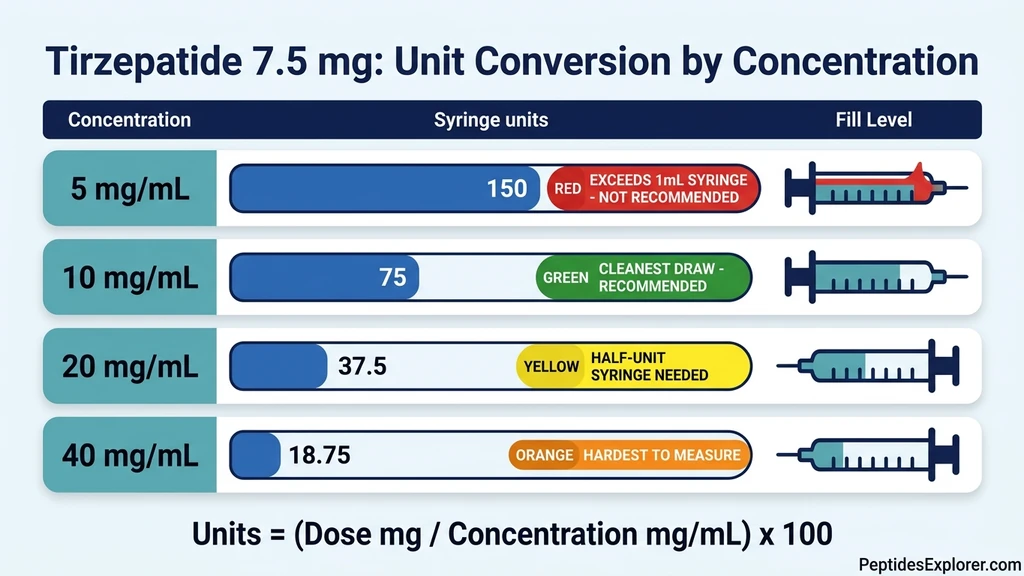
Here is your answer: at 10 mg/mL, 7.5 mg of tirzepatide = 75 units. At 20 mg/mL, it is 37.5 units. At 40 mg/mL, it is 18.75 units. None of these are round. That is what makes 7.5 mg the most error-prone dose on the entire titration schedule.
This guide covers the exact conversion at every concentration, explains why this specific dose trips people up, shows you how to read the half-unit marks your syringe may or may not have, and walks through the step-by-step calculation so you never guess. If you want the answer instantly, use the Tirzepatide Dosage Calculator.
Get your custom peptide protocol:
- Tailored to your body and goals
- Precise dosing and cycle length
- Safe stacking combinations
- Backed by peer-reviewed studies
- Ready in under 2 minutes
Quick Reference: 7.5 mg in Units at Every Concentration
Find your vial concentration in the left column. Draw to the number in the right column.
| Your Vial Says | Units to Draw | Volume (mL) | Recommended Syringe |
|---|---|---|---|
| 5 mg/mL | 150 units* | 1.50 mL | Exceeds 1 mL syringe |
| 10 mg/mL | 75 units | 0.75 mL | 1 mL (100-unit) |
| 20 mg/mL | 37.5 units | 0.375 mL | 0.5 mL (50-unit) |
| 40 mg/mL | 18.75 units | 0.1875 mL | 0.3 mL half-unit |
*Exceeds a standard 100-unit syringe. You need a higher concentration vial or must split into two draws.*
If you do not know your concentration, stop. Flip the vial and read the label. It will say something like "Tirzepatide 10 mg/mL." If it says "200 mg / 10 mL," divide: 200 / 10 = 20 mg/mL. If you cannot tell, call your pharmacy before you inject.
Look at the table. Not a single value is a whole number except 75 units at 10 mg/mL. Three of the four common concentrations require you to hit a half-unit or quarter-unit mark. This is why 7.5 mg generates more dosing errors than any other step in the titration. For the complete dose-by-dose chart covering every milligram from 2.5 to 15, see the tirzepatide dosage chart in units.
Why 7.5 mg Is the Most Error-Prone Dose
If you breezed through your first two months on tirzepatide, 7.5 mg is where the ride gets bumpy. The titration ladder goes 2.5, 5, 7.5, 10, 12.5, 15 mg. At 10 mg/mL (what most compounding pharmacies ship), the first two rungs land on tidy numbers: 25 units, then 50 units. You line up the plunger, it clicks on a printed mark, done.
Then your provider bumps you to 7.5 mg and the math stops cooperating. At 10 mg/mL you need 75 units, which at least lands on a tick mark on a 1 mL syringe. Workable. But pharmacies do not always send the same concentration. If your refill arrives at 20 mg/mL, the draw is 37.5 units. At 40 mg/mL, it is 18.75 units. Good luck finding either of those printed on any syringe in your medicine cabinet.
Here is why this particular dose trips so many people up. The standard Mounjaro and Zepbound titration jumps straight from 5 mg to 10 mg after 4 weeks at each level. A lot of providers insert a 7.5 mg step to soften the blow, because doubling the dose in one shot tends to bring on a wave of nausea. SURPASS-1 data backs this up: nausea hit 12-18% of patients at 5 mg and climbed to 16-24% at 10 mg (Frias et al., N Engl J Med, 2021). The half-step smooths that transition, but it also drops you into the hardest syringe read on the entire schedule.
Three things pile up at once: - The draw lands on a fraction at most concentrations. No clean lines to aim for. - Many people are picking up a 1 mL syringe for the first time after 8+ weeks on a 0.5 mL. The barrel feels different in your hand, the tick spacing changes, and visual landmarks you trusted are gone. - You feel confident. The first two doses went fine, so you stop double-checking. That comfort is exactly where the mistakes creep in.
See how many units is 2.5 mg of tirzepatide for how the math works at the simpler starting dose.
The Calculation Formula (Works for Every Dose)
You only need one formula. Write it on a sticky note and keep it near your supplies until it becomes second nature.
Units = (Dose in mg / Concentration in mg/mL) x 100
Let me walk you through it with 7.5 mg at 10 mg/mL, step by step:
- 1.Divide your dose by your concentration: 7.5 mg / 10 mg/mL = 0.75 mL. That tells you 7.5 mg of drug is sitting in 0.75 mL of liquid inside that vial.
- 2.Multiply by 100 to get syringe units: 0.75 mL x 100 = 75 units. Why 100? Because a U-100 insulin syringe treats 1 mL as 100 units. So 0.75 mL = 75 units. That is where you draw to.
Same formula at 20 mg/mL:
- 1.7.5 mg / 20 mg/mL = 0.375 mL
- 2.0.375 x 100 = 37.5 units
And at 40 mg/mL:
- 1.7.5 mg / 40 mg/mL = 0.1875 mL
- 2.0.1875 x 100 = 18.75 units
There is a handy pattern here: every time the concentration doubles, the number of units you draw gets cut in half. From 10 mg/mL (75 units) to 20 mg/mL (37.5 units), halved. From 20 to 40, halved again. The amount of tirzepatide entering your body never changes. You are always injecting 7.5 mg. Only the volume of liquid shifts.
This is why concentration swaps are so dangerous. If your pharmacy sends a 20 mg/mL refill and you keep drawing 75 units out of habit, you just injected 15 mg. Double your target. That is the absolute ceiling of approved tirzepatide dosing, delivered in one shot with no titration. For the reverse calculation (you know the units and need the milligrams), see how many mg is 20 units of tirzepatide. Or skip the math entirely: the Peptide Unit Converter does it in seconds.
Syringe Reading Guide for Fractional Draws
At 7.5 mg, your syringe draw lands on a fraction at most concentrations. Reading that fraction correctly requires understanding what the lines on the barrel actually mean. The spacing changes with syringe size.
75 Units on a 1 mL Syringe (10 mg/mL)
A 1 mL syringe holds 100 units. Each small tick mark represents 2 units. Printed numbers appear at 10, 20, 30, 40, 50, 60, 70, 80, 90, and 100 on most brands.
Your target is 75 units. That sits exactly halfway between the printed 70 and 80, and it lands directly on a tick mark (because 75 is an odd multiple of the 2-unit graduation). Look for the line that is 2.5 small ticks above the 70. That is 75.
This is the cleanest read for 7.5 mg at any concentration. If your pharmacy sends 10 mg/mL vials, you will find 75 units straightforward on a 1 mL syringe. A 0.5 mL (50-unit) syringe cannot hold 75 units, so do not attempt it.
37.5 Units on a 0.5 mL Syringe (20 mg/mL)
A 0.5 mL syringe holds 50 units. Each small tick mark represents 1 unit. Printed numbers appear every 5 or 10 units.
Your target is 37.5 units. That falls exactly between the 37 and 38 unit lines. On a standard syringe, this is the gap between two tick marks with no line to aim for. You are estimating a half-unit.
Two options to hit 37.5 precisely:
Option 1: Use a half-unit syringe. These syringes (sometimes labeled "Lo-Dose") have tick marks every 0.5 units instead of every 1 unit. The 37.5 mark appears as a printed line. No estimation needed. This is the safest approach.
Option 2: Aim for the visual midpoint. If you only have a standard 0.5 mL syringe, draw the plunger so the top of the rubber stopper sits exactly centered between the 37 and 38 lines. This is imprecise. A half-unit error at 20 mg/mL changes your dose by 0.1 mg. Tolerable, but avoidable with the right syringe.
18.75 Units on a 0.3 mL Syringe (40 mg/mL)
A 0.3 mL syringe holds 30 units. Each small tick mark on a standard version represents 1 unit. On a half-unit version, each tick is 0.5 units.
Your target is 18.75 units. On a standard 0.3 mL syringe, 18.75 falls three-quarters of the way between the 18 and 19 lines. On a half-unit syringe, it falls halfway between 18.5 and 19. Neither offers a clean landing.
This is the hardest draw on the entire titration schedule. A quarter-unit estimation error at 40 mg/mL means you are off by 0.1 mg per 0.25 units. Miss by a full unit and you shift your dose by 0.4 mg. Over multiple weeks of consistent rounding in one direction, the cumulative deviation matters.
Practical recommendation: If you are prescribed 7.5 mg and your pharmacy provides 40 mg/mL vials, request a half-unit 0.3 mL syringe and aim for the midpoint between the 18.5 and 19.0 lines. Alternatively, ask your pharmacy if they can supply a 20 mg/mL vial instead. At 20 mg/mL, the draw becomes 37.5 units, which is easier to read on a half-unit 0.5 mL syringe.
Concentration-Specific Calculations: Worked Examples
Each concentration requires a different thought process. Below is the complete calculation for 7.5 mg at all four concentrations, including the syringe choice and visual target.
7.5 mg at 5 mg/mL
Calculation: 7.5 / 5 = 1.5 mL. 1.5 x 100 = 150 units.
Problem: A standard insulin syringe maxes out at 100 units (1 mL). You cannot fit 150 units in a single draw.
Solutions: - Best: Call your pharmacy and request a 10 or 20 mg/mL vial. This eliminates the problem entirely. - Backup: Draw 100 units, inject, then draw another 50 units from the same vial and inject again. This works but doubles the needle sticks and introduces more opportunity for air bubbles and measurement error. If you must split the draw, verify both volumes before injecting either one.
At 5 mg/mL, any dose above 5 mg exceeds syringe capacity. If your provider plans to titrate you past 5 mg, a higher concentration vial is not a convenience. It is a necessity. For help with vial preparation, see the Peptide Reconstitution Calculator.
7.5 mg at 10 mg/mL
Calculation: 7.5 / 10 = 0.75 mL. 0.75 x 100 = 75 units.
Syringe: 1 mL (100-unit). A 0.5 mL syringe only holds 50 units, so it cannot accommodate this draw. This is the first dose in the titration where you must switch up from the 0.5 mL syringe you used at 2.5 and 5 mg.
Visual target: Three-quarters of the way up the barrel. On most 1 mL syringes, 75 falls directly on a tick mark between the printed 70 and 80. Count 2.5 small lines above the 70 (each line = 2 units, so 2.5 lines = 5 units above 70 = 75).
Common error: Confusing the syringe you were using at 5 mg. If you drew 50 units on a 0.5 mL syringe at 5 mg, your muscle memory says "draw to the top." At 7.5 mg, drawing to the top of a 0.5 mL syringe gives you only 50 units, which equals 5 mg. You just underdosed by one-third. Switch to the 1 mL syringe.
7.5 mg at 20 mg/mL
Calculation: 7.5 / 20 = 0.375 mL. 0.375 x 100 = 37.5 units.
Syringe: 0.5 mL (50-unit) with half-unit markings if available. A standard 0.5 mL syringe works but requires you to estimate the midpoint between the 37 and 38 unit lines.
Visual target: On a half-unit syringe, draw to the 37.5 line. On a standard syringe, draw to the midpoint between 37 and 38.
Precision check: A half-unit error here (drawing 38 instead of 37.5) adds 0.01 mL, which at 20 mg/mL equals 0.2 mg. That means 7.7 mg instead of 7.5 mg. Over a single injection, the error is small. But if you consistently round up, you accumulate extra drug exposure week after week.
7.5 mg at 40 mg/mL
Calculation: 7.5 / 40 = 0.1875 mL. 0.1875 x 100 = 18.75 units.
Syringe: 0.3 mL (30-unit) half-unit syringe. A standard 0.3 mL syringe requires you to estimate three-quarters of the distance between the 18 and 19 unit lines. A half-unit version narrows it to estimating the midpoint between 18.5 and 19.0.
Precision check: Each unit on a 40 mg/mL vial represents 0.4 mg. A 1-unit error (drawing 19 instead of 18.75) adds 0.1 mg to your dose. A 2-unit error (drawing 20 or 21) adds 0.5 to 0.9 mg. At this concentration, small reading mistakes produce measurable changes.
Recommendation: 40 mg/mL is the highest concentration most compounding pharmacies offer. If precision at 18.75 units feels unreliable, ask your provider or pharmacy if 20 mg/mL is available. The 37.5-unit draw at 20 mg/mL is substantially easier to read.
What Happens When You Get the 7.5 mg Draw Wrong
The 7.5 mg dose sits at the midpoint of the titration schedule. Errors in both directions produce real consequences.
Scenario 1: You switched from 10 mg/mL to 20 mg/mL and did not recalculate.
You have been drawing 75 units from a 10 mg/mL vial. Your pharmacy sends a refill at 20 mg/mL. You do not read the label. You draw 75 units.
75 units at 20 mg/mL = 15 mg. That is double your intended dose and the absolute maximum approved tirzepatide dose. In the SURPASS trials, patients reached 15 mg only after a 20-week escalation. Jumping from 7.5 to 15 in a single week causes severe GI distress: vomiting, diarrhea, and abdominal pain that can last 48 to 72 hours. In patients taking sulfonylureas or insulin, a sudden 15 mg dose increases the risk of hypoglycemia (Mounjaro prescribing information, Eli Lilly, 2022).
The fix: Read your vial label every time you open a new one. Write the concentration on the box with a marker if it helps.
Scenario 2: You used a 0.5 mL syringe out of habit.
At 5 mg, you drew 50 units on a 0.5 mL syringe. It was easy: full to the top. At 7.5 mg, you need 75 units. That exceeds the 50-unit capacity of your syringe. You draw to the top and figure it is "close enough."
You just injected 50 units = 5 mg. That is two-thirds of your prescribed dose. You underdosed by 2.5 mg. Your weight loss stalls and you assume the medication stopped working. In reality, you never titrated.
The fix: At 10 mg/mL, the 7.5 mg dose requires a 1 mL syringe. Mark the switch point on your calendar when you move from 5 to 7.5 mg.
Scenario 3: You rounded 18.75 to 20 units on a 40 mg/mL vial.
Your target is 18.75 units. You draw to 20 because it is the nearest visible mark. 20 units at 40 mg/mL = 8 mg. You overdosed by 0.5 mg. Over a single injection, 0.5 mg is tolerable. But if you round up at every dose for 4 weeks, you receive 8 mg per week instead of 7.5 mg, which is 32 mg total exposure instead of 30 mg over the month. The extra 2 mg shifts your effective titration ahead of schedule and may increase the rate of GI side effects.
The fix: Use a half-unit 0.3 mL syringe. Aim for the midpoint between 18.5 and 19.0 rather than rounding to the nearest whole number.
Step by Step: Drawing and Injecting 7.5 mg of Tirzepatide
This walkthrough uses a 10 mg/mL vial and a 1 mL (100-unit) insulin syringe. Your target is 75 units.
1. Wash your hands. Soap and water, 20 seconds. Dry completely.
2. Check your vial. Read the label. Confirm the concentration is 10 mg/mL. Look at the liquid. It should be clear and colorless. If it is cloudy, discolored, or has particles, do not use it. Verify it has not expired and has been stored properly in the fridge.
3. Wipe the vial stopper. Swab the rubber top with an alcohol pad. Let it air dry for 10 seconds.
4. Prime the syringe with air. Pull the plunger back to the 75-unit mark. You are pulling air into the syringe. This air goes into the vial to equalize pressure, which makes drawing liquid easier.
5. Insert the needle and inject air. Push the needle straight through the center of the rubber stopper. Press the plunger all the way down to push the air into the vial.
6. Flip the vial upside down. With the needle still inserted, invert the vial so it hangs above the syringe. The liquid should cover the needle tip.
7. Pull the plunger to 75 units. Slowly draw the liquid to the 75-unit line. On a 1 mL syringe, 75 units is three-quarters of the way up the barrel, between the printed 70 and 80. Pull slightly past 75, then push back to exactly 75. This clears small air bubbles.
8. Check for bubbles. Look at the liquid in the barrel. If you see air bubbles, tap the syringe with your fingernail. The bubbles rise to the needle end. Push the plunger gently to squirt them into the vial, then pull back to 75 units. Repeat until bubble-free.
9. Remove the needle from the vial. Pull straight out.
10. Choose your injection site. Abdomen (at least 2 inches from your navel), front of thigh, or back of upper arm. Rotate sites each week. For a detailed injection tutorial, see how to inject tirzepatide.
11. Pinch and inject. Pinch a fold of skin, insert the needle at a 90-degree angle (or 45 degrees if you have less subcutaneous fat), and press the plunger slowly and steadily. Count to 5 after the plunger is fully depressed before withdrawing.
Switching Syringes at the 7.5 mg Step
The 7.5 mg dose is the inflection point where most patients at 10 mg/mL must change syringe sizes. This switch itself introduces error.
At 2.5 mg (25 units) and 5 mg (50 units), a 0.5 mL syringe works perfectly. Each tick mark on a 0.5 mL syringe represents 1 unit. The lines are wide, readable, and familiar after 8+ weeks of use.
At 7.5 mg (75 units), you exceed the 0.5 mL syringe capacity. You must move to a 1 mL syringe. On a 1 mL syringe, each tick mark represents 2 units instead of 1. The lines are closer together. The barrel is wider. The visual landmarks you relied on for two months no longer apply.
What to do before your first 7.5 mg injection:
- 1.Buy the 1 mL syringes before you need them. Do not discover the problem on injection day.
- 2.Practice reading the new syringe dry. Pull the plunger to 75 units with no vial attached. Look at where 75 sits relative to the barrel. Now pull to 50 (your old dose). See the difference. Then pull to 100 (your next dose at 10 mg). Build the visual map before you draw live medication.
- 3.Double-check the first live draw. After pulling to 75 units, hold the syringe at eye level. Confirm the top of the rubber plunger stopper aligns with the 75-unit line. If it sits above or below, adjust.
At 20 mg/mL, the 7.5 mg dose is 37.5 units, which fits inside a 0.5 mL syringe. You do not need to switch sizes. But you do need a half-unit syringe for accuracy. The considerations change with concentration, so always match your syringe to your specific draw volume.
Common Mistakes at the 7.5 mg Dose
I see the same four mistakes come up repeatedly in patient forums and provider Q&A threads. Most of them boil down to muscle memory overriding basic math.
Mistake 1: Grabbing the same 0.5 mL syringe you used last month.
At 5 mg you drew 50 units on a 0.5 mL syringe. It went right to the top, easy. Now you need 75 units for 7.5 mg. That physically will not fit. If you draw to the top anyway, you get 50 units (5 mg), a full third less than prescribed. Your weight loss stalls and you blame the medication. The fix is simple: move to a 1 mL syringe for any draw above 50 units.
Mistake 2: Calling 74 close enough to 75 on a 1 mL syringe.
Here is something most people do not realize about 1 mL syringes: each tiny tick mark is 2 units, not 1. So the marks near your target go 70, 72, 74, 76, 78, 80. The number 75 falls between 74 and 76. On most brands, there is no line there at all. You are eyeballing a midpoint. Drawing to 74 shortchanges you by 0.2 mg. Drawing to 76 gives you 0.2 mg extra. Neither will hurt you, but know that you are estimating. If precision matters to you, a half-unit syringe eliminates the guesswork.
Mistake 3: Trusting a stranger's unit number from Reddit.
Someone posts "I draw 37 units for my 7.5 mg dose." Their vial is 20 mg/mL. Yours is 10 mg/mL. If you draw 37 units from your vial, you inject 3.7 mg. That is barely half your prescribed dose. The unit number only means something paired with a concentration. Always run the formula against your own vial label: (7.5 / your concentration) x 100.
Mistake 4: Not rechecking when a new vial arrives.
Your first pharmacy shipped 10 mg/mL. The refill comes from a different pharmacy at 20 mg/mL. The vials look similar. You draw 75 units without reading the label. Actual dose: 15 mg, double your target, the maximum approved tirzepatide dose delivered with zero titration. This is the single most common dosing error I see discussed in tirzepatide communities. Treat every new vial like the first one you ever opened: read the label, run the math, then draw.
Frequently Asked Questions
How many units is 7.5 mg of tirzepatide at 10 mg/mL?
75 units. The math: 7.5 / 10 = 0.75 mL, and 0.75 x 100 = 75 units on a U-100 insulin syringe. Use a 1 mL (100-unit) syringe. A 0.5 mL syringe cannot hold this volume.
How many units is 7.5 mg of tirzepatide at 20 mg/mL?
37.5 units. The liquid is twice as concentrated as 10 mg/mL, so you need half the volume: 7.5 / 20 = 0.375 mL = 37.5 units. Use a half-unit 0.5 mL syringe and draw to the 37.5 mark. On a standard syringe, aim for the midpoint between the 37 and 38 lines.
How many units is 7.5 mg of tirzepatide at 40 mg/mL?
18.75 units. The calculation: 7.5 / 40 = 0.1875 mL = 18.75 units. Use a half-unit 0.3 mL syringe and aim between the 18.5 and 19.0 marks. Each unit at this concentration equals 0.4 mg, so precision matters.
Why is 7.5 mg not a standard Mounjaro pen dose?
Mounjaro auto-injector pens come in 2.5, 5, 7.5, 10, 12.5, and 15 mg. The 7.5 mg pen does exist. But compounded tirzepatide comes in multi-dose vials, not pre-filled pens, so you must calculate and draw the dose yourself. The 7.5 mg step is part of the FDA-approved titration schedule.
Can I skip 7.5 mg and go straight from 5 mg to 10 mg?
Some providers prescribe this jump, but it doubles your dose in one step. In the SURPASS trials, nausea rates increased at each dose level (Frias et al., N Engl J Med, 2021). The 7.5 mg step reduces the severity of GI side effects by splitting the increase. Follow your provider's instructions, not an online suggestion.
What syringe should I use for 7.5 mg of tirzepatide?
At 10 mg/mL (75 units): 1 mL syringe. At 20 mg/mL (37.5 units): 0.5 mL half-unit syringe. At 40 mg/mL (18.75 units): 0.3 mL half-unit syringe. The rule is always the same: use the smallest syringe that fits your entire dose. Smaller barrel means finer markings and better accuracy.
How many mL is 7.5 mg of tirzepatide?
It depends on concentration. At 5 mg/mL: 1.5 mL. At 10 mg/mL: 0.75 mL. At 20 mg/mL: 0.375 mL. At 40 mg/mL: 0.1875 mL. Divide 7.5 by your vial's concentration to get milliliters. Multiply by 100 to convert to syringe units.
I was drawing 50 units for 5 mg. How much more do I draw for 7.5 mg?
At the same concentration (10 mg/mL), add 25 units. Your new draw is 75 units. But you will need a 1 mL syringe because 75 exceeds the 50-unit capacity of the 0.5 mL syringe you likely used for 5 mg. Do not try to overfill the smaller syringe.
The Bottom Line
At 10 mg/mL, 7.5 mg of tirzepatide is 75 units. At 20 mg/mL, it is 37.5 units. At 40 mg/mL, it is 18.75 units. The formula: (7.5 / concentration) x 100.
This dose produces fractional draws at every concentration except 10 mg/mL on a 1 mL syringe. Use the smallest syringe that fits your draw, and use half-unit syringes for concentrations above 10 mg/mL. Read your vial label before every injection. Recalculate when anything changes.
Want to skip the math? The Tirzepatide Dosage Calculator converts any dose at any concentration instantly. For the full titration table covering 2.5 to 15 mg, see the tirzepatide dosage chart in units. For help preparing your vials, use the Peptide Reconstitution Calculator.
Related Articles: - How Many Units Is 2.5 mg of Tirzepatide — starting dose conversion - How Many mg Is 20 Units of Tirzepatide — reverse conversion from units to milligrams - How to Inject Tirzepatide — step-by-step injection technique - How to Reconstitute Tirzepatide — vial preparation before your first draw - Tirzepatide Maintenance Dose After Weight Loss — what comes after the titration - Is Compound Tirzepatide Safe? — safety considerations for compounded tirzepatide
Related Articles
How Many mg Is 20 Units Tirzepatide?
20 units of tirzepatide = 1 mg at 5 mg/mL, 2 mg at 10 mg/mL, or 4 mg at 20 mg/mL. Full conversion table for every concentration.
How Many Units Is 2.5 mg Tirzepatide?
2.5 mg of tirzepatide is 25 units at 10 mg/mL, 12.5 units at 20 mg/mL, or 50 units at 5 mg/mL. Conversion table with syringe instructions.
How Many Units Is 12.5 mg of Tirzepatide?
How many units is 12.5 mg of tirzepatide? 125 units at 10 mg/mL, 62.5 at 20 mg/mL, 31.25 at 40 mg/mL. Conversion chart and syringe guide.
Tirzepatide Dosage Chart in Units (2026)
Tirzepatide dosage chart converting mg to units for 5, 10, 20, and 40 mg/mL concentrations. Covers 2.5 to 15 mg doses with syringe markings and common mistakes.